ANAT SC 3003
Page 1
Anat Sc 3003 Applied Clinical Anatomy
Semester 2, Week 9
HMS S127
Groups 2a-f: 14:00-15:30pm. Groups 1a-f: 15:30-15:00pm
Anatomy Session: Head & Neck 2: Ears and Nose
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and communicated to you by or on behalf of Adelaide University pursuant to Part VB of the
Copyright Act 1968 (the Act). The material in this communication may be subject to copyright under the Act. Any further reproduction
or communication of this material by you may be the subject of copyright protection under the Act.
Do not remove this notice.
Work in your groups to answer the questions related to the following clinical scenarios:
Clinical Scenario A
A 5 year old boy is brought in to see his general practitioner (GP) by his parents. His parents report that he has
been complaining of ear pain and pulling at his right ear for the past 2 days. He has had multiple similar
episodes in both ears in the past year, and his parents are particularly concerned because his school teacher
has noticed that he sometimes has difficulty hearing. The GP examines the boy’s ear with an otoscope, and
diagnoses a middle ear infection.
1. Name the anatomical structure that usually provides “ventilation” (when required) between the middle ear and the
nasopharynx.
eustacian tube
2. Explain the appearance of the tympanic membrane. Why does the boy’s ear hurt?
appears inflamed, not translucent as usual. usually it's concave towards the inner ear, this one
appears to be bulging towards the middle ear. nociceptors are being stimulated. innervation:
Tympanic branch off of CN IX
3. Explain why hearing would be affected in this ear.
tympanic membrane is fixed in one spot due to build of fulids if it's unable to move,
it's unable to transmit and amplify vibrations from the outter ear into the inner ear.
ANAT SC 3003
Page 2
Because of his recurrent ear infections, the GP refers the boy to a specialist. The specialist performs an
assessment, and recommends adenoidectomy (surgical removal of the adenoid) and insertion of grommets.
** adenoids = nasopharyngeal tonsils
it's lymphatic tissue (like the tonsils)
** Grommets are inserted inferior to
the umbo **
4. How could an enlarged adenoid be related to recurrent middle ear infections? (Hint: there are two theories)
1. infection which can spread from the nasopharynx to the middle ear via eustacian tube
2. eustacian tube may be blocked --> mucus cannot escape and fluid build up in middle ear
18 months later, the grommets have extruded (come out of the tympanic membrane) and the tympanic
membranes have healed. Unfortunately, the boy has another episode of ear pain, and in addition to a red,
bulging tympanic membrane, his GP notices redness and swelling of the skin posterior to the pinna.
5. Where has the middle ear infection spread to?
infection has spread to the air cells of mastoid process of the temporal bone causing osteomyelitis.
ANAT SC 3003
Page 3
Clinical Scenario B
A 50 year old woman presents to the Emergency Department with a persistent nosebleed (epistaxis). Her regular
medications include warfarin (an anticoagulant medication), which she takes as she has an artificial heart valve.
She says that the bleeding was initially coming out of her right nostril, but she is now also spitting blood out of
her mouth. At home, she tried pressing externally on both sides of her nose (on the bony part just below the
eyes) for 20 minutes, but the bleeding did not slow down or stop.
1. Where in the nasal cavity is the bleeding most likely to have originated from (be specific), and why?
kisselbachs area; anastomosis of 5 different arteries = lots of weak spots. Area is close
to surface and vulnerable to injury.
2. Why didn’t the bleeding stop when she applied external pressure to her nose? Where should she have applied the
pressure for a better effect?
pressure on the anterior cartliagenous part may have been more effective to tamponade the vessels
A doctor in the Emergency Department examines her nose, and cauterizes the bleeding area on the right side of
her nasal septum. The bleeding stops, and she is sent home. Unfortunately, she returns to the Emergency
Department the next day with another nosebleed, this time from the left nostril. The bleeding area on the left
side of the nasal septum is cauterized. Six months later, the woman presents to her general practitioner
complaining that her nose “whistles” when she breathes. She is found to have an anterior septal perforation
(hole in the anterior nasal septum).
3. Explain the relationship between the cautery performed on both sides of the septum and the development of the
septal perforation.
Kisselbachs area is located anteriorly where there is no bone (vomer). cauterizing on either side may have burnt
a hole in the septum. The delayed onset of whistling may have been due to the healing process (ie. inflammation,
scab formation, healing)
4. Explain why her nose “whistles”.
air flowing through the small perforation (hole) = whistling sounds
ANAT SC 3003
Page 4
Clinical Scenario C:
A 30 year old man presents to his GP with a constantly blocked nose. He also reports a feeling of pressure in
his forehead, above both eyes, and over his cheeks. He works as a gardener, and sometimes has bouts of
sneezing, an itchy roof of mouth, and a runny nose. During these bouts, his nose feels even more blocked. He
has also noted that he cannot smell the roses very much anymore. On examining his nose, the GP observes
that he has bilateral nasal polyps. He undergoes a CT scan of the paranasal sinuses, and is referred to a
specialist. The specialist informs the man that he has chronic sinusitis with nasal polyps, as well as allergic
rhinitis.
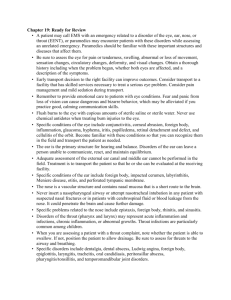
Nasal polyp in the right nasal cavity
CT of paranasal sinuses – coronal plane
1. Nasal polyps can result from inflammation and oedema of paranasal sinus mucosa. In this case, the polyps seem to
be coming from the anterior part of the middle meatus. Which paranasal sinuses are the polyps likely to have
originated from?
maxillary sinuses (ethmoid occasionally) --> they drain/ lead into the middle meatus
2. Explain why the man’s nose feels blocked (all the time).
the polyps are narrowing the nasal cavity, blocking the middle meatus, air is unable to passage through.
3. Why is his nasal obstruction worse when he is experiencing hay fever symptoms?
natural allergic response = inflammation, which, in turn, may increase mucus secrestions to remove stimulus
4. Where in the nose is olfactory epithelium located? Why is the man’s sense of smell poor?
upper 1/3 of the nasal canal.
The man is prescribed several medications, and undergoes surgery to remove the polyps and open the ostia of
the sinuses. On the 2nd day after the operation, he has a small amount of thin, clear fluid come out of his nose.
This seems to happen every time he points his nose towards the ground.
5. What sort of fluid might this be? (Hint: it is not nasal mucus)
CSF
6. Which structures must have been damaged for this fluid to leak into the nasal cavity?
ethmoid bone
 0
0