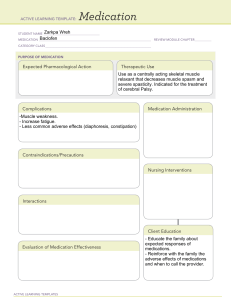
Pharmacology Exam #1 Study Guide Rights of medication administration • • • • • • Right drug Right dose Right route Right time Right patient Right documentation Pharmaceutics: understand how different forms of the medication affect its dissolution and absorption into the body • • • • • Oral drugs that are liquids (elixirs, syrups) are already dissolved and are usually absorbed more quickly than solid dosage forms. Enteric-coated tablets have a coating that prevent them from being broken down in the acidic pH of the stomach and do not get absorbed until reaching a higher pH in the intestines. Particle size within a tablet or capsule can make different dosage form of the same drug dissolve and be absorbed at different rates → different times to onset of action o Example: micronized glyburide reaches a maximum concentration peak faster than non-micronized formulation Extended-release tablets and capsules release in GI tract over a prolonged period → prolongs drug absorption and duration of action o This is opposite for immediate-release dosage forms Parenteral dosage forms that are injected IV have 100% absorption and occurs immediately upon injection. Remember which medications should not be crushed • • Extended release oral dosage forms → could cause accelerated release of drug from the dosage form and possible toxicity Enteric-coated tablets → causes disruption of the tablet coating designed to protect the stomach lining from the local effects of the drug and/or protect the drug from being prematurely disrupted by stomach acid. In pharmacokinetics review the following concepts: absorption, distribution, metabolism, and excretion. Remember main organs in charge of metabolism and excretion as well • Absorption: o Bioavailability: extent of drug absorption ▪ First pass effect: the initial metabolism in liver of a drug from GI tract before entering systemic circulation • • Liver metabolizes drug into inactive metabolites • high first pass effect → low bioavailability o Routes of absorption: enteral, parenteral, topical ▪ Enteral: absorbed into systemic circulation through mucosa of the stomach and/or small intestines (oral, sublingual, buccal, rectal) • Can be altered with short bowel syndrome (portions of small intestines removed) or from bariatric weight-loss surgery • Suppository form of rectal drugs are considered enteral • Sublingual and buccal routes: absorbed rapidly into bloodstream and delivered to site of action; these drugs bypass the liver • Dosage form will usually be higher than parenteral form because of first pass effect ▪ Parenteral: fastest route a drug can be absorbed; bypasses the first-pass effect • Intravenous (fastest delivery into blood): • Intramuscular: absorbed faster than subcutaneous injections o Depot drugs → a form of long-acting IM dosage forms designed to slow absorption over a period of several days to a few months • Subcutaneous • Intradermal • Intraarterial, intrathecal, intraarticular → must be given by a physician ▪ Topical: delivers a uniform amount of drug over a longer period, but the effects of the drug are usually slower in their onset and more prolong in duration of action. This can be a problem if a patient begins to experience adverse effects from drug and a considerable amount of the drug has already been absorbed. • Avoid first-pass effect (except for rectal) • can be applied to skin, eyes, ears, nose, lungs, rectum, or vagina • Transdermal patches deliver a constant amount of drug for a certain amount of time. This route is convenient for patients who cannot tolerate oral administration Distribution: transport of a drug by the bloodstream to its site of action. Distributed first to those areas with extensive blood supply (heart, liver, kidneys, brain). Muscle, skin, and fat are areas of slower distribution. o drug molecules that are not bound to plasma proteins can freely distribute to extravascular tissue o Albumin is the most common blood protein and carries the majority of proteinbound drug molecules ▪ • • Unbound portion is active (considered “free”) and the bound portion is inactive ▪ Conditions that cause albumin level (such as extensive burns and malnourished states) to be low result in a large portion of “free” drugs which can raise risk for toxicity ▪ Taking 2 medication that are highly protein bound → competition for binding site on albumin which causes more unbound drug ▪ Hydrophilic drugs will have a smaller volume of distribution and high blood concentration ▪ Lipophilic drugs will have a larger volume of distribution and low blood concentration Metabolism=Biotransformation: biochemical alteration of a drug into an active metabolite or more soluble compound o Prodrug: conversion of inactive metabolite to its active form (must go through liver) o Liver is most responsible for metabolism o Hepatic metabolism involves activity of cytochrome P450 enzymes (3A4, 2C9, 2C19, 2D6) ▪ They target lipid-soluble drugs, which are typically difficult to eliminate ▪ P-450 system is one of the most important systems that influences drugdrug interactions o Enzyme inhibitors: inhibit drug metabolizing enzymes ▪ Decreases in drug metabolism can result in accumulation of the drug o Enzyme inducer: stimulate production of enzyme ▪ Can cause decrease drug effects Excretion: elimination of drugs from the body o Kidney is primary organ for excretion ▪ Renal excretion is accomplished through glomerular filtration, active tubular reabsorption, and active tubular section o Biliary excretion: excretion of drugs by the intestines o Bowel excretion Understand loading dose • An initial higher dose of a drug that may be given at the beginning to achieve therapeutic levels Understand what half-life is and how it affects drug administration • Half-life: time required for ½ (50%) of a given drug to be removed from the body o a measure of the rate at which the drug is eliminated from the body o clinically useful for determining steady state (state in which the amount of drug removed via elimination is equal to the amount of drug absorbed with each dose) o longer half-life → the longer the drug stays in the body Review Peak, trough, therapeutic window, therapeutic range, and toxicity table • • • Peak level: highest blood level concentration Trough level: lowest blood level of a drug In therapeutic monitoring, peak and trough values are measured to verify adequate drug exposure, maximize therapeutic effects, and minimize drug toxicity What is an agonist, antagonist, and what is their effect usually? • • Agonist: a substance that binds to a receptor and causes a response Antagonist: a drug that binds to a receptor and prevents a response Teratogenic effect, carcinogenic effect • • Teratogenic → capable of crossing placenta; fetal demise Carcinogenic → cancer causing What are the different drug categories in pregnancy? Which is the safest? Which is the ones that is most contraindicated? • • • • • Category A: no risk t human fetus (SAFEST) Category B: no risk to animal fetus; info. For human is unavailable Category C: adverse effect reported in animal fetus; info. For humans in unavailable Category D: possible fetal risk in human; however, consideration of potential benefit vs. risk may warrant use of these drugs in pregnant women Category X: fetal abnormalities reported (MOST CONTRAINDICATED) What is a black box warning and the subcategories? Which one is worse? • a type of warning that appears in a drug prescribing info. and is required by the FDA to alert prescribers of serious adverse events that have occurred with the given drug o Class I → most serious o Class II → less severe o Class III → least severe What are scheduled drugs and what does it mean? • Scheduling of controlled substance Review medication errors and how to prevent them. • • • • • • Errors can occur during any step of medication process → procuring, prescribing, transcribing, dispensing, administering, monitoring Issues contributing to medical errors → organizational issues, educational system issues, sociological factors, use of abbreviations Near miss: event or situation hat did produce patient injury only because of chance o patient was still exposed but with no harm Close call: an event or situation or error that took place but was identified and captured PRIOR to reaching the patient Strategies to minimize medication errors → Awareness (“speak up”, computerized prescriber order entry (CPOE), bar codes and scanning devices, automated dispensing machines, effective communication Preventing medication errors: o Multiple systems of checks and balances should be implemented o Prescribers must write legible orders that contain correct info. or should be entered electronically o Authoritative resources, such as pharmacists or current drug references or literature, must be consulted o Check 3 times before giving the drug o Right of medication administration used consistently o Two patient identifies o Do not administer if you did not draw up or prepare yourself o minimize verbal or telephone orders ▪ repeat order ▪ spell drug name ▪ speak slowly and clearly o list indication next to each order o Never assume anything that’s not specified in a drug order o Do not hesitate to question a medication order for any reason when in doubt o Do not try to decipher written orders o Do not use unapproved abbreviations o Never use a “trailing zero” with medication orders o Always use a “leading zero” for decimal dosages o Take time to learn special administration techniques of certain dosage forms o Always verify new medication administration records o Read labels o Use generic names to avoid sound alike trade names o Minimize interruptions o Mandatory second nurse verification for high-risk medications and/or patient population o Know where to find info. on medications o Check patient allergies and identifiers o Always listen to and honor any concerns expressed by patients regarding medications Review power Atlas of drug administration and major points discussed in class. How to administer SubQ, Intradermal and IM drugs (Including z track technique and airlock) review needles used, amount of medication and angle to use for each. Understand which ones you draw back and why? • • SubQ o o o o o 45- or 90-degree angle (depending on size of patient) Doses are usually 0.5-1mL 25- to 27-gauge ½- to 5/8-inch needle To ensure correct needle length, grasp the skinfold and choose a needle that is approx. half the length of the skinfold from top to bottom ID o 0.01 – 0.1 mL o Tuberculin or 1-mL syringe with a 25- or 27-gauge needle that is 3/8 or 5/8 in. long o 15-degree angle • • IM o 90-degree angle o Generally, require a longer needle to reach the muscle tissue, but shorter needles may be needed for older patients, children, and adults who are malnourished o Aqueous medication can be given with a 20- to 25- gauge needle o Oil based or viscous medication are given with a 1- to 21- gauge needle o Avg. needle length: 5/8 – 1in. for children; 1-1 ½ in. for adults o 3mL is max. amount used in a single injection ▪ 2mL is recommended if the patient is an older adult or is thin o Use the z-track method o Use draw back method → pull back on plunger for 5-10 seconds to check for blood return Z-track method: o Pull sin laterally and hold it while giving the injection o Release skin immediately after withdrawing needle to seal off the injection site. o Forms a Z-shaped track in the tissue that prevents the medication from leaking through the more sensitive subQ tissue from muscle site of injection o Used for injections of irritating substances like iron dextran and hydroxyzine; for all IM injections • Air-Lock Technique o After withdrawing desired amount of medication into the syringe, withdraw an additional 0.2mL of air. The small air bubble that follows the medication during the injection may help prevent the medication from leaking through the needle track into the subQ tissues. How to mix insulins (which one do you draw first and which one second) • • Draw up clear insulin first (rapid/fast acting) Then draw up cloudy insulin (intermediate) Opioid analgesics discussed in class, mechanism of action (MOA), indications, side effects, reversal and nursing implications (Remember what to assess before and after and what to monitor for), what to do if RR is less than 10 and medication used to reverse it • • MOA: each classification has own mechanism of action o The mu, kappa, and delta receptors are most responsive to drug activity (mu is the most important) Agonists: bind to an opioid pain receptor in the brain; cause an analgesic response (reduction of pain sensation) o Morphine: prototype ▪ Accumulation is more likely in renal failure patients ▪ Side effects: decreased blood pressure, respiratory depression, urinary retention, and constipation ▪ MS Contin is a sustained release form of morphine o Hydromorphine (Dilaudid): 7-8x stronger than morphine o Meperidine (Demerol) ▪ Rarely used and not recommended for long-term pain treatment ▪ Must be used with caution in older adults, patients who require longterm analgesia, or in patients that have kidney failure o Fentanyl (Duragesic): 80-100x stronger than morphine ▪ Fentanyl patches → intended for management of chronic or cancer pain in opioid-tolerant patient whose pain is not adequately controlled by other types of medication; should not be used for acute pain situations • Applying heat accelerates the diffusion of the drug being absorbed into the body o Codeine: HIGHLY addictive; can mix with Tylenol to decrease risk for addiction ▪ Less effective as an analgesic and is only agonist to possess a ceiling effect (meaning increasing the dose will not increase the response) ▪ Causes GI upset ▪ Can be used for relief of cough • • • • • Antagonist: binds to pain receptor but does not reduce pain; reverses effect of these drugs on pain receptors o Naloxene (Narcan) ▪ For overdoses of opioids ▪ Injectable form ▪ Has a short half-life (1hr) so may need to be re-dosed ▪ Should be given when a patient experiences severe respiratory depression Agonists-Antagonists: bind to pain receptor and cause a weaker neurologic response than a full agonist (partial agonist; mixed-agonist) o Butorphanol (Stadol): prototype Indications: o Main use: alleviate moderate to severe pain o Often given with adjuvant analgesic drugs to assist primary drugs with pain relief o Also used for: cough center suppression; treatment of diarrhea; balanced anesthesia Adverse Effects: o CNS depression (most serious adverse effect) ▪ Leads to respiratory depression o GI tract effects: nausea, vomiting, and constipation o Urinary retention o Diaphoresis and flushing o Miosis- pupil constriction o Itching Nursing Implications: o Perform thorough pain assessment- pain intensity and character, location, onset, description, precipitating and relieving factors, type, remedies, and other pain treatments o Medicate patients before the pain becomes severe o oral forms should be taken with food to minimize gastric upset o ensure safety measure- keep sliding rails up to prevent injuries o withhold dose and contact physician if there is a decline in patients condition or if the vital signs are abnormal ▪ Especially if respiratory rate is LESS THAN 10-12 breaths/min (may need Narcan) o Instruct patients to follow directions for administration carefully and to keep a record of their pain experience and response to treatments o Patients should be instructed to change positions slowly to prevent orthostatic hypotension o Assess bowel sounds before administration because it will worsen constipation is patient is already constipated What is acetaminophen (Tylenol), mechanism of action, indications, side effects, main organ of concern, reversal agent, maximum daily dose, nursing implications (ie teaching and monitoring) • Acetaminophen (Tylenol): nonopioid analgesic o analgesic and antipyretic effects o little to no inflammatory effects o available OTC and combination products with opioids ▪ hydrocodone & acetaminophen → Vicodin ▪ oxycodone & acetaminophen → Percocet o MOA: blocks pain impulses peripherally by inhibiting prostaglandin synthesis Centrally ▪ similar to salicylates ▪ also lowers fever by acting on hypothalamus o Indications: ▪ Mild to moderate pain ▪ Fever ▪ Alternative to those who cannot take aspirin because of its analgesic and antipyretic effects • Use of aspirin not for children because of Reye’s syndrome o Maximum daily dosage is 3000mg/day ▪ 2000mg/day for elder adults with liver disease o Main organ of concern is Liver o Side Effects: ▪ Hepatotoxicity is the most serious adverse effect; associated with excessive dose ▪ Possible effects: skin disorders, nausea, and vomiting o Reversal Agent: acetylcysteine (Mucomyst) ▪ Works by preventing the hepatotoxic metabolites from forming ▪ Most effective when given within 10hrs of an overdose What are NSAIDs? Review main NSAIDs discussed in class in bold, mechanism of action, indications, main side effects and organs of concern, nursing implications and teaching to the patients, from the NSAIDs which ones work more on COX 2 and what is the benefit, and the main problem, signs of toxicity? • NSAIDs: large chemically diverse group of drugs with the following properties: analgesic, anti-inflammatory, antipyretic, aspirin-platelet formation o They are also used for the relief of: ▪ ▪ ▪ ▪ ▪ ▪ o o o o Mild to moderate headaches Myalgia Neuralgia Arthralgia Alleviation of postoperative pain Relief of pain associated with arthritic disorder → rheumatoid arthritis, juvenile arthritis, ankylosing, spondylitis, and osteoarthritis ▪ Treatment of gout and hyperuricemia MOA: inhibition of the leukotriene pathway, the prostaglandin pathway, or both ▪ Blocking the chemical activity of cyclooxygenase (COX) • COX-1: has a role in maintaining GI mucosa, platelet aggregation, promotes synthesis of prostaglandins that primarily have beneficial effects on the body • COX-2: promotes synthesis of prostaglandins that are involved in inflammatory process Adverse Effects: ▪ Gastrointestinal • Dyspepsia, heartburn, epigastric distress, nausea • GI bleeding * • Mucosal lesions * o * Misoprostol (Cytotec) can be used to reduce these dangerous effects [Category X drug!!!] ▪ Renal • Reductions in creatinine clearance • Acute tubular necrosis with renal failure ▪ Cardiovascular • Noncardiogenic pulmonary edema Serious interactions can occur when given with: ▪ Anticoagulants (especially with aspirin) ▪ Corticosteroids and other ulcerogenic drugs ▪ Protein bound drugs ▪ Diuretics and ACE inhibitors Nursing Implications: ▪ Assess for GI lesion or peptic ulcer disease or bleeding disorders ▪ Do not give salicylates to children and teenagers because of Reyes Syndrome ▪ Tolerated better when given with food, milk, or an antacid to avoid irritation ▪ Explain that therapeutic effects may not be seen for 3-4 weeks ▪ ▪ Educate about the adverse effects and for them to notify prescriber if these effects become severe or if bleeding or GI pain occurs Inform patients to watch closely for the occurrence of any unusual bleeding, such as in the stool ▪ • • • Salicylates o Salicylic acid (Aspirin) (the most common one used) ▪ Inhibits platelet aggregation ▪ Antithrombotic affect → used in the treatment of MI and other thrombotic disorders ▪ Major contraindication is the use for children • Reyes Syndrome: leads to deficits that can lead to a coma and may involve liver damage ▪ Toxicity: Salicylism (Done nomogram can used to estimate the severity of intoxication and help guide treatment) • Cardiovascular: increased HR • Pulmonary: Bronchoconstriction • CNS: Tinnitus (experiencing ringing in ears), hearing loss, dimness of vision, headache, dizziness, mental confusion, lassitude, drowsiness • GI: nausea, vomiting, diarrhea, GI bleeding • Metabolic: metabolic acidosis, sweating, thirst, hyperventilation, hypoglycemia or hyperglycemia • Thrombocytopenia COX-2 inhibitor o Celecoxib (Celebrex) ▪ First and only COX-2 inhibitor ▪ Indication: osteoarthritis, rheumatoid arthritis, acute pain symptoms, ankylosing spondylitis, and primary dysmenorrhea ▪ Adverse Effects: headache, sinus irritation, diarrhea, fatigue, dizziness, lower extremity edema, and hypertension ▪ Little effect on platelet function ▪ Not to be used in patients with a known sulfa allergy ▪ Does not affect GI mucosa when compared to nonselective NSAIDs (prevents GI ulcers and GI bleeding) ▪ Doubles the risk for an MI (especially is the patient has heart disease) Propionic Acid Derivatives o Ketorolac (Toradol) ▪ Analgesic effects like morphine ▪ Can only be used for 5 days because of adverse effects on kidney and GI tract ▪ Adverse effects: renal impairment, edema, GI pain, dyspepsia, nausea o Ibuprofen (Motrin, Advil): prototype o Naproxen (Naprosyn, Aleve) ▪ Fewer drug interactions with angiotensin-converting enzyme inhibitors given for hypertension ▪ Longer half-life o Indications: rheumatoid arthritis, osteoarthritis, primary dysmenorrhea, gout, dental pain, and muscoskeletal disorders What is malignant hyperthermia and how would a patient with it present? • • A genetically linked major adverse reaction to general anesthesia Rapid rise in temperature, tachycardia, tachypnea, sweating What is a neuromuscular blocking drug (NMBD)? What does it do? Does it provide analgesia or sedation? Can the patient breath on their own after receiving this medication? What is the nursing implication of this? • NMBD: prevent nerve transmission in skeletal and smooth muscle, resulting in muscle paralysis o also paralyze the skeletal muscles required for breathing (intercostal muscles and diaphragm) o used with anesthetics during surgery (as adjunts) o do not cause sedation or pain relief o the patient cannot breathe on their own → need ventilation to prevent brain damage or death from suffocation; need ventilation before giving drug o Depolarizing: Succinylcholine (Anectine) → binds with ACh receptors at neuromuscular junction o Nondepolarizing: Mivacurium (Mivacron) → compete with ACh for cholinergic receptors at neuromuscular junction o Nursing implication: ▪ Assess past history of surgeries and response to anesthesia ▪ Asses past history, allergies, and medications ▪ Assess use of alcohol, illicit drugs, opioids, smoking ▪ Assessment is vital during preoperative, intraoperative, and postoperative → vital signs, baseline lab work, ECG, O2 saturation, ABC’s, monitor all body systems ▪ Watch for sudden elevation in body temperature, which may indicate malignant hyperthermia ▪ Provide preoperative teaching about the surgical procedure and anesthesia pain Succinylcholine MOA, side effects, indications, nursing implications and black box warning • • • • • MOA: acts on cholinergic receptor sites at neuromuscular junction o at first, depolarization occurs and skeletal muscles contract o after repeated contractions, the membraine is unable to repolarize as long as the drug stays attaches to receptor o affects as muscle spasms and muscle weakness and then paralysis occurs o it is rapidly broken down by cholinesterase → duration of action is only a few minutes once IV Is stopped Adverse effects: o Bradycardia and respiratory depression o Malignant hyperthermia o If doses are high enough → the ganglia are affected which causes tachycardia, hypotension, and urinary retention Neuromuscular blockade might be prolonged in patients with hypokalemia, hypocalcemia, or low pseudocholinesterase levels Black Box Warning: should be administered in a facility with trained personal for respirations. Cardiac arrest has been reported. Nursing indications: same as NMBD Benzos (Diazepam, lorazepam)- MOA, indications, adverse effects, reversal agent, nursing implications. (Use for seizures too, especially status epilepticus) • Benzodiazepines o Classified as either → sedative-hypotic or anyiolytic o Long-acting → diazepam (Valium) o Intermediate acting → alprazolam (Xanax), lorazepam (Ativan), temazepam (Restorli) o MOA: ▪ Depress CNS activity ▪ Affect hypothalamic, thalamic, and limbic systems of the brain ▪ GABA receptors o Indications: ▪ Sedation, sedation, skeletal muscle relaxation, anxiety relief, acute seizure disorder, alcohol withdrawal, agitation relief, balanced anesthesia o Adverse effects: ▪ Drowsiness ▪ Dizziness ▪ Cognitive impairment ▪ • • Respiratory depression (with overdose or when takin with other CNS depressants- barbiturates, opioids, alcohol) ▪ Lethargy ▪ Fall hazard for elderly ▪ “hangover” effect/daytime sleepiness o Reversal agent → Flumazenil Diazepam (Valium) o For status epilepticus Lorazepam (Ativan) o Can be given by IV push/IM: useful in treatment of an acutely agitated patient o Continuous infusion for agitated patients who are undergoing mechanical ventilation o Used to treat or prevent alcohol withdrawal o Irritating to the muscle so must be diluted Salicylate toxicity: signs/symptoms • • • • • Cardiovascular: increased HR Pulmonary: bronchoconstriction Central nervous: Tinnitus, hearing loss, dimness of vision, headache, dizziness mental confusion, lassitude, drowsiness GI: nausea, vomiting, diarrhea Metabolic: metabolic acidosis, sweating, thirst, hyperventilation, hypoglycemia, or hyperglycemia Barbiturates (Phenobarbital mainly)- MOA, indications, adverse effects, nursing implications. Remember that this medication is an enzyme inducer. What does that mean? • Phenobarbital (Luminal): protoype o MOA: changing the action of GABA What are anticonvulsants or antiepileptic drugs? What is the goal of the therapy? • Antiepileptic Drugs (AED) → management for all types of epilepsy o Also known as anticonvulsants → used to prevent the convulsive seizures typically associated with epilepsy o Goals of therapy: ▪ To control or prevent seizures while maintaining a reasonable quality of life ▪ To minimize adverse effects and drug-induced toxicity o Black Box Warning: suicidal thoughts and behaviors o First-Line AED’s: ▪ Carbamazepine (Tegretol) ▪ ▪ ▪ ▪ ▪ Phenobarbital (Luminal) Phenytoin (Dilantin) Valproic acid (Depakene) Lamotrigine (Lamictal) Benzodiazepines used for acute seizure activity or status epilepticus Hydatoins family- Phenytoin (Dilantin) MOA, indications, adverse effects. Remember highly protein bound and what does this mean. Remember the therapeutic level. Remember how is this drug different to fosphenytoin which one can be given IM and what happens if phenytoin is given IM or the IV infiltrates? How should this med be mixed and what tubing? How fast to give? Sign of toxicity. Remember teaching to the patient! • • Hydantoins o Prototype: phenytoin (Dilantin) ▪ Fosphenytoin (Cerebyx) → prodrug for phenytoin • Can be given IM o MOA: to desensitize sodium channels o Phenytoin is highly protein bound! ▪ Long half-life → so stays in body longer ▪ High levels can be seen in patients with low Albumin concentrations o Primary use: treating all types of seizures o Adverse effect: CNS depression, gingival hyperplasia, skin rash, cardiac dysrhythmias, hypotension, sedation, Dilantin facies Phenytoin (Dilantin) o Effective for most seizure types, except for absence seizures o Has an anti-dysrhythmia property similar to lidocaine ▪ Off-label use for digitalis-induced dysrhythmias o IV form only with saline! ▪ Can crystalize and become an embolism use filtered tubing ▪ Slow infusion with Gaige 20g or smaller • IV MUST be given slowly, not exceeding 50mg/min ▪ if IV is in hand, can lead to purple glove • IV in ante-cubital area ▪ Monitor for Stevens-Johnson syndrome o IM has soft tissue irritants leading to necrosis o Adverse effects: hyperglycemia, hypotension, v-fib, multiple blood dyscrasias → assess for sore throat and fever! o Oral hygiene is a must!! (because of gingival hyperplasia) o Therapeutic range: 10-20 mcg/mL o Side effects: weakness & ataxia, insomnia, depression, headache, psychosis, gingival hyperplasia, hirsutism o Drowsiness occurs initially but decrease over time with use of medication Valproic acid- MOA, indications, adverse effects, therapeutic level, blood test needed to be done to monitor for adverse effects. Main organ of concern. • Valporic acid (Depakene) o not recommended for women intending to get pregnant o Family: Phenytoin like drugs/ hydations o MOA: desensitize Na channels o Indications: a wide range of seizure types- partial, absence, tonic clonic, and myoclonic ▪ Can also be used for bipolar disorder o PO routes for administration ▪ Divalproex (Depakote) → extended release form ▪ Depacon → injectable form ▪ GI irritation ▪ Do not mis liquid form with carbonated beverages ▪ Able to “sprinkle” caplet beads if difficulty taking large pill o Interactions: drug-drug → increases Dilantin and phenobarbital levels o Adverse effects: limited CNS depression, visual disturbances, ataxia, vertigo, headache ▪ Hepatoxicity, GI effects, pancreatitis o Hepatic disfunction possible in first 6 months ▪ Liver Functioning Testing at 2-month intervals • First testing for base line to know the normal range o Therapeutic level: 50-100mcg/mL Lamotrigine- MOA, indications, adverse effect (main one discussed in class). • Lamotrigine (Lactimal) o MOA: inhibiting sodium currents by binding to the inactive sodium channel o Indications: for simple and complex seizes; also used to treat bipolar disorder o Adverse effect: Stevens-Johnson syndrome ▪ Inflammation and sloughing of skin, potentially over entire body ina way that resembles a 3rd degree burn Medication used for status epilepticus- Think Benzo. See above for MOA, side effects and reversal very important! • Diazepine (Valium): prototype o MOA: similar to barbiturates but safer ▪ potentiating the action of GABA, nerve impulses traveling to in the cerebral cortex are inhibited o primary use → status epilepticus o Adverse effects: drowsiness and dizziness, respiratory depression ▪ apnea, hypotension, and somnolence o Reversal: Flumazenil (Romazicon) ▪ Used when RR and SpO2 are too low Parkinson disease, sign and symptoms and goals of pharmacological therapy. • PD: a chronic, progressive, degenerative disorder o Affects dopamine-producing neurons in the brain o Caused by an imbalance of 2 neurotransmitters: dopamine (low levels) & acetylcholine (ACh) (excessive activity) o Symptoms: (TRAP) ▪ Tremor ▪ Rigidity ▪ Akinesia ▪ Postural instability ▪ Staggering gait ▪ Drooling o Drug therapies are aimed at increasing the levels of dopamine or antagonizing the effects of ACh ▪ Drug therapies do not slow the progression of the disease but are used to slow the progression of symptoms Benztropine (Cogentin)- MOA, indications (remember avoid in elderly), side effects (Think anticholinergic) • Benzotropine (Cogentin) → Anticholinergic therapy o MOA: block the effect of ACh o Indications: for PD and extrapyramidal symptoms from antipsychotic drugs • Anticholinergic therapy treats muscle tremors and muscle rigidity associated with PD o These 2 symptoms are associated with excessive cholinergic activity o Does not relieve bradykinesia (extremely slow movements) o Adverse effects: tachycardia, confusion, disorientation, toxic psychosis, urinary retention, dry throat, constipation, nausea, and vomiting o Not a good medication for older patients, usually for younger patients with Parkinson’s o Avoid alcohol o Caution during hot weather or exercise because it may cause hyperthermia Review nursing implications for Parkinson meds. • Nursing Implications o Perform a thorough assessment, nursing history, and medication history ▪ Includes questions about the patients: • CNS → dizziness, headaches, fatigue, paralysis, syncope • GI and GU tracts • Psychological and emotional status o Assess for signs and symptoms of PD: ▪ Masklike expression ▪ Speech problems ▪ Dysphagia ▪ Rigidity of arms, legs, and neck o Assess for contraindication conditions o Provide patient education: ▪ Inform patient to not take other medication with PD drugs unless checked with physician first ▪ Teach patient about expected therapeutic and adverse effects with drug therapy o When starting dopaminergic drugs, assist patient will walking because of dizziness o Administer oral doses with food to minimize GI upset o Encourage patient to force fluids to at least 3000mL/day (unless contraindicated) o Taking levodopa with MAOI’s may result in hypertensive crisis o Patient should be taught not to discontinue antiparkinsons drugs suddenly o Entacapone may darken the patient’s urine and sweat o Therapeutic effects of COMT inhibitors may be noticed within a few days ▪ May take weeks with other drugs o Monitor for response to drug therapy ▪ Improved sense of well-being and mental status ▪ Increased appetite ▪ Increased ability to perform ADL’s, to concentrate, and to think clearly ▪ Less intense Parkinson’s manifestations → less tremor, shuffling gait, muscle rigidity, and involuntary movements SSRI’s: MOA, side effects, what to monitor • SSRI: Selective Serotonin Reuptake Inhibitors o MOA: inhibition of serotonin uptake o Adverse effects: insomnia, weight gain, sexual dysfunction, fatigue, lethargy, nausea, headache o Contraindication: concurrent MAOI therapy → can lead to serotonin syndrome o Fluoxetine (Prozac): prototypical SSRI Monoamine oxidase inhibitors: MOA, side effects, what to avoid • MAOI’s o Nonselective: phenelzine (Nardil) o Selective: selegiline o Rarely used for depression, some are used for PD o MOA: inhibit the MAO enzyme system in the CNS → dopamine, serotonin, and norepinephrine are not broken down and leads to higher level of these substance o Disadvantage: potential cause of hypertensive when taken the tyramine, which may lead to cerebral hemorrhage, stroke, coma, or death ▪ Avoid foods that contain tyramine! • Aged, mature cheeses (cheddar, bleu, swiss) • Smoked, pickled, or aged meats, fish, poultry (herring, sausage, corned beef, salami, pepperoni, pate) • Yeast extracts • Red wines • Italian broad beans (fava beans) o Use of SSRI’s and MAOI’s can lead to serotonin syndrome Know serotonin syndrome. Causes, signs and symptoms • Serotonin Syndrome: elevated levels of serotonin o May occur with the use of any psychotic drug that enhances serotonin activity o Common symptoms: ▪ Delirium ▪ Agitation ▪ Tachycardia ▪ Sweating ▪ Myoclonus (muscle spasms) ▪ Hyperreflexia ▪ Shivering ▪ Course tremors ▪ Extensor plantar muscles (sole of foot) respone o More severe symptoms: ▪ Hyperthermia ▪ Seizures ▪ Rhabdomyolysis (breakdown of muscle) ▪ Renal failure ▪ Cardia dysrhythmias ▪ Disseminated intravascular coagulation o Need 2-5 week “washout” when changing classes of antidepressants that include MAOI’s → to avoid serotonin syndrome o Avoid St. John’s wort → to avoid serotonin syndrome Neuroleptic malignant syndrome: signs/symptoms • An uncommon but serious adverse effect associated with the use of antipsychotic drugs and characterized by symptoms o Symptoms: high fever, unstable BP, myogobinemia Tricyclic antidepressants (TCA): MOA/ Side effects • • • TCA → largely been replaced by SSRI’s as first line antidepressant drugs Considered second line: o For patients who fail with SSRI’s or other newer generation antidepressants o As adjunct therapy with newer generation antidepressants Amitriptyline (Elavil) o MOA: block reuptake of neurotransmitters, causing accumulation at the nerve endings o Adverse effects: dry mouth, constipation, blurred vision, urinary retention, orthostatic hypotension and dysrhythmias ▪ Discolors urine o Original indication was depression ▪ More commonly used now to treat insomnia and neuropathic pain Lithium therapeutic levels/toxicity: how to prevent • • • • Therapeutic range: o For acute mania → 1 – 1.2mEq/L o Maintenance level → 0.6 – 1.2mEq/L Levels exceeding 1.5 – 2.5mEq/L begin to produce toxicity, including GI discomfort, tremor, confusion, somnolence, seizures, and possible death Keeping sodium level in normal range (135 – 145mEq/L) helps maintain therapeutic lithium level o Lithium is a salt, so losing too much Na can lead to lithium toxicity o Avoid overhydration and dehydration Most serious adverse effect is cardiac dysrhythmia Treatment for extrapyramidal side effects • Extrapyramidal symptoms (EPS): pseudoparkinsonism- akathisia, acute dystonia o Treated with benztropine (Cogentin) and trihexyphenidyl (Artane)