Ultrasound of the Groin: Techniques, Pathology, and Pitfalls
advertisement

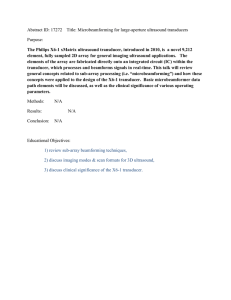
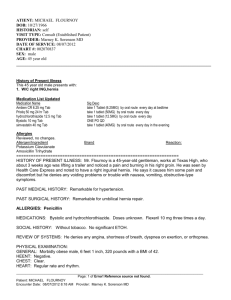
M u s c u l o s k e l e t a l I m a g i n g • R ev i ew Jacobson et al. Ultrasound of the Groin FOCUS ON: Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Musculoskeletal Imaging Review Jon A. Jacobson1 Viviane Khoury 2 Catherine J. Brandon1 Jacobson JA, Khoury V, Brandon CJ Ultrasound of the Groin: Techniques, Pathology, and Pitfalls OBJECTIVE. In a patient with symptoms referable to the groin, there can be a number of causes to consider and at times the cause of the symptoms is multifactorial. Although ultrasound can be effective in the evaluation of the groin, the depth and complexity of the anatomy can be problematic. A protocol-driven approach for ultrasound evaluation of the groin will help to ensure an accurate and comprehensive evaluation. This article summarizes the ultrasound technique and protocol for evaluation of the groin to include evaluation of the hip joint, anterior hip musculature, the iliopsoas bursa, the inguinal lymph nodes, the pubic sym­phys­ eal region, and the inguinal region for hernias. Common pathologic conditions and pitfalls related to ultrasound evaluation of the groin will be reviewed. CONCLUSION. There are many potential pathologic conditions in a patient with groin symptoms. Because symptoms may be multifactorial and history may be ambiguous or misleading, a protocol-driven evaluation with ultrasound is recommended. The hip joint is evaluated for effusion, synovitis, and labral abnormalities. The muscles and tendons, including the common aponeurosis at the pubic symphysis, are evaluated for tendinosis and tears. Dynamic evaluation should be considered to assess for snapping hip syndrome. Iliopsoas bursal distention and lymph node enlargement are other considerations. Last, inguinal region hernias must be evaluated during the Valsalva maneuver and documented in two orthogonal planes to avoid several important diagnostic pitfalls. U Keywords: groin, hernia, hip, joint, ultrasound DOI:10.2214/AJR.15.14523 Received February 2, 2015; accepted after revision April 15, 2015. 1 Department of Radiology, University of Michigan, 1500 E Medical Center Dr, TC-2910L, Ann Arbor, MI 48109-0326. Address correspondence to J. A. Jacobson (jjacobsn@umich.edu). 2 Department of Radiology, University of Pennsylvania, Philadelphia, PA. Supplemental Data Available online at www.ajronline.org. AJR 2015; 205:513–523 0361–803X/15/2053–513 © American Roentgen Ray Society AJR:205, September 2015 ltrasound has been used to effectively evaluate pathology of the musculoskeletal system [1–3]. When an abnormality involves the distal extremity, ultrasound can accurately show anatomy and pathology in detail with the benefit of directly correlating imaging and physical examination findings [4]. Dynamic evaluation of structures with muscle contraction, joint movement, or position change of the patient may also add significant information that may not be obtainable with static MRI [5]. In contrast to evaluation of the distal extremities, evaluation of the groin and hip can be more problematic. The added depth of the area being imaged results in lower resolution, and there is more complex anatomy. It is often difficult to directly correlate imaging findings with patient symptoms and the clinical presentation may be ambiguous. To ensure a comprehensive evaluation, one should follow a specific protocol when performing an ultrasound examination (Table 1). The groin can be defined as the area at the junction of the lower abdomen and the in- ner thigh; therefore, ultrasound of the groin should include evaluation of the hip joint, anterior hip musculature, iliopsoas bursa, inguinal lymph nodes, pubic symphyseal region, and inguinal region for hernias. Dynamic evaluation is also an integral aspect of a groin ultrasound examination. This article reviews a protocol-driven approach to the ultrasound evaluation of the groin, showing common pathologic conditions and discussing diagnostic pitfalls. Ultrasound Equipment Clinically available ultrasound units, both portable and cart-based, with variable frequency transducers can be used to evaluate the groin and hip. For an examination of a thin individual, a linear transducer of greater than 10 MHz is effective. For larger patients, a curvilinear transducer of less than 10 MHz is often needed to evaluate the hip. It is a misconception to presume that a curvilinear transducer must be used, but often it is necessary. The objective is to use the highest frequency transducer possible to achieve the 513 Jacobson et al. Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved highest resolution given the constraints of a patient’s body habitus. Hip Joint Scanning Details For ultrasound examination of the hip joint, the transducer is placed in the sagittal oblique plane long axis to the femoral neck. The characteristic bone landmarks of the femoral head and neck should be identified (Fig. 1A). The femoral neck should be perpendicular to the sound beam to eliminate anisotropy of the overlying joint capsule. The hyperechoic fibrocartilage labrum is also identified at the acetabulum. The transducer is then rotated 90° to evaluate the anterior hip in its short axis (Fig. 1B). Anatomy The hip joint is evaluated for joint-related abnormalities, such as a joint effusion, intraarticular bodies, and synovial disorders. When evaluating for a joint effusion, one should target the area over the anterior femoral neck. Normally, a hyperechoic layer measuring up to 7 mm is present, representing the iliofemoral ligament and joint capsule with its reflection [6] (Fig. 1A). If not imaged perpendicular, this hyperechoic layer may appear artifactually hypoechoic from anisotropy and may potentially simulate joint fluid. Regardless, the layer should measure less than 7 mm if normal [7]. An additional pitfall relates to leg positioning: Internal rotation of the hip may cause the anterior joint capsule to become convex anteriorly and to potentially measure greater than 7 mm. Joint Effusion A joint effusion will appear as anechoic distention of the joint capsule preferentially around the femoral neck [6]. In the native hip, evaluation of the anterior recess provides an adequate evaluation for a joint effusion. It is a misconception to believe that fluid may be present only posteriorly; some degree of fluid is always present anterior to the femoral neck in the native hip with a joint effusion [8]. However, in the setting of a hip arthroplasty, a joint effusion may be loculated, which warrants a more thorough evaluation of the lateral and posterior femoral neck. As an additional pitfall after arthroplasty, ultrasound can be inaccurate in the diagnosis of a small joint effusion [9]. An extensive evaluation of all areas of the hip is warranted when evaluating for complications related to a hip arthroplasty, such as particle disease and pseudotumor formation [10]. 514 TABLE 1: Ultrasound Scanning Protocol of the Groin Anatomic Region and Structures Pathology Hip joint Anterior recess Effusion, infection, synovial hypertrophy Labrum Labral tear, paralabral cyst Femur Femoroacetabular impingement Anterior hip musculature Iliopsoas complex Snapping hip syndrome Rectus femoris Tendinosis including calcific tendinosis Sartorius Tendon tear Iliopsoas bursa Distention, synovial hypertrophy, infection Inguinal lymph nodes Superficial and deep inguinal lymph nodes Hyperplasia, inflammation, primary neoplasia, metastases Pubic symphyseal region Rectus abdominis Common aponeurosis injury Pubic symphysis Adductor tendon tear or tendinosis Adductor tendons Fracture Inguinal region hernias Internal ring and inguinal canal Indirect inguinal hernia Hesselbach triangle Direct inguinal hernia Femoral canal Femoral hernia Synovial Hypertrophy If a joint effusion is complex, the fluid may appear hypoechoic rather than anechoic and synovial hypertrophy should be considered. For assistance in the differentiation of a joint effusion from synovial hypertrophy, a lack of compressibility and internal flow on color or power Doppler imaging would indicate synovial hypertrophy; however, this distinction may be difficult, and ultrasound-guided aspiration may be indicated. Because findings on ultrasound cannot be used to exclude infection, joint aspiration, lavage and reaspiration, and synovial biopsy should be considered in patients with any distention of the joint capsule if there is concern for septic joint [11–13]. In addition to infection, other possible causes of synovial hypertrophy include systemic inflammatory arthritis, pigmented villonodular synovitis (Fig. 2), synovial chondromatosis, and amyloid deposition [14]. Labrum Although the posterior aspect of the labrum is difficult to visualize on ultrasound, the anterior aspect, which is the most common site for labral tears, can be easily evaluated [15]. A hypoechoic or heterogeneous labrum indicates degeneration, whereas a more defined anechoic cleft indicates a labral tear [16]. In the evaluation for a labral tear with ultrasound, sensitivity, specificity, and accuracy have been shown to be 82%, 60%, and 75%, respectively [16]; therefore, MRI, preferably MR arthrography, is indicated if there is concern for labral abnormalities [16]. One cause for a labral tear is cam-type femoroacetabular impingement (FAI), in which an abnormal osseous contour of the proximal femur or abnormal femoral head-neck offset can impinge on the acetabulum causing hyaline cartilage and labral injuries [17]. Although ultrasound can show an anterosuperior bony prominence and cam deformity of the proximal femur associated with FAI, alpha angles cannot be reliably measured and ultrasound is not recommended for FAI screening [18]. Related to a labral tear, a paralabral cyst may also be identified on ultrasound as a lobular anechoic or hypoechoic fluid collection in contact with the labral tear [19] (Fig. 3). As a potential pitfall, a paralabral cyst may be hypoechoic and difficult to delineate, although the lobular appearance and associated labral tear suggest the appropriate diagnosis. Anterior Hip Musculature Scanning Details For evaluation of the anterior hip musculature, ultrasound scanning can begin over the AJR:205, September 2015 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Ultrasound of the Groin femoral head and neck in the sagittal oblique plane using bone landmarks for orientation (Fig. 1A). The transducer can then be turned transverse to the body and centered over the femoral head where the psoas major tendon and iliopsoas complex can be identified (Fig. 1B). The transducer can then be moved cephalad to the level of the ilium at the anterior inferior iliac spine (AIIS) to visualize the individual components of the iliopsoas complex (Fig. 1C). The transducer can be moved lateral at the level of the AIIS so that the rectus femoris can be identified. More cephalad, the sartorius origin can be identified at the anterior superior iliac spine. The anterior hip musculature can then be assessed in both the long and short axes. fibers, and the medial iliacus becomes interposed between the psoas major tendon and superior pubic ramus [23]. As the patient returns the leg to a straight position, there is a normal reversal in the rotational gliding of the psoas major around the medial iliacus muscle fibers. In patients with the abnormal condition, the medial component of the iliacus muscle becomes temporarily entrapped between the psoas major tendon and superior pubic ramus [20]. As the iliacus muscle abruptly moves lateral, the psoas major tendon also abruptly moves posterior and makes contact with the superior pubic ramus [20]. This contact results in an abnormal snap, which is perceived by the patient and felt through the transducer. Iliopsoas Complex The iliopsoas complex is composed of several structures. In the transverse plane at the AIIS, the psoas major tendon is visible with its muscle component located medial [20] (Fig. 1C). The psoas major tendon may be bifid with partial and complete splits [20]. Anterolateral to the psoas major tendon are the medial and lateral muscle fibers of the iliacus with an interposed fascial layer [20]. Inferior to the AIIS, the ilioinfratrochanteric muscle component is present lateral to the iliacus; the rectus femoris is located directly lateral and the sartorius anterior to the ilioinfratrochanteric muscle [20]. An additional muscle component, composed of the inferior fibers of the iliacus, is more difficult to visualize on ultrasound [20]. More distally, an accessory tendon from the medial iliacus fibers unites with the psoas major tendon to form the iliopsoas tendon several centimeters proximal to the lesser trochanter. The lateral aspect of the iliacus attaches to the proximal femoral diaphysis as a direct muscle attachment [21]. Ultrasound evaluation of the distal aspect of the iliopsoas complex is improved with positioning the hip in flexion, abduction, and external rotation [22]. Rectus Femoris and Sartorius For evaluation of the rectus femoris, assessment of both the direct (or straight) and indirect (or reflected) heads is required [24]. With the transducer’s short axis to the rectus femoris over the AIIS, the direct head is visible (Fig. 1C). When the transducer is moved lateral and slightly inferior while the sound beam is being directed perpendicular to the lateral acetabular cortex to eliminate anisotropy, the indirect head is visible. The transducer can then be turned 90° to evaluate the separate heads in the long axis. Possible pathologic findings includes tendinosis and a tendon tear. This area is also a potential site for calcium hydroxyapatite crystal deposition as calcific tendinosis (Fig. 4). Ultrasound-guided lavage and aspiration have been successfully used for percutaneous treatment [25]. Similarly, the sartorius is evaluated in the short and long axes for muscle and tendon abnormalities. Snapping Hip Syndrome To evaluate for snapping iliopsoas, the transducer is placed short axis to the psoas major tendon of the iliopsoas complex at the level of the ilium superior to the AIIS and is positioned in the oblique axial plane parallel to the inguinal ligament. The patient is then asked to flex, abduct, and externally rotate the hip. During this maneuver, the psoas major tendon normally rotates anterolateral relative to and around the medial iliacus muscle AJR:205, September 2015 Iliopsoas Bursa The iliopsoas bursa is a normal structure located medial and often deep to the iliopsoas complex where the iliopsoas passes over the ilium. Communication between the iliopsoas bursa and the hip joint is present in approximately 15% of individuals, although this number increases in the presence of inflammatory arthritis and after arthroplasty [26]. When distended, the iliopsoas bursa is identified medial and deep to the iliopsoas complex and may extend proximal along the psoas musculature in the abdomen to potentially simulate a psoas abscess. In this situation, identification of hip joint communication is essential to confirm iliopsoas bursal distention, which is most often related to a chronic hip joint process. This communica- tion with the hip joint is seen medial to the psoas major tendon at the level of the femoral head with the transducer positioned transverse to the body (Fig. 1B). Inguinal Lymph Nodes Superficial inguinal lymph nodes are located superficial to the femoral vessels in the femoral triangle and are bordered by the inguinal ligament, sartorius, and adductor longus [27]. The deep inguinal lymph nodes are located deeper and medial to the femoral vessels [27]. It is common to identify multiple inguinal lymph nodes bilaterally in asymptomatic individuals [27]. The average short-axis measurement of an inguinal lymph node in asymptomatic individuals is 5.4 mm (range = 2.1–13.6 mm) with a value of 8.8 mm at 2 SDs above the mean [27]. Because size criteria are simple guidelines, the ultrasound characteristics are important to determine whether a lymph node is abnormal regardless of its size. For example, a metastasis may cause focal asymmetric enlargement without meeting the size criterion for enlargement. A normal lymph node has an oval shape with a hyperechoic hilum, uniform thickness of the hypoechoic cortex, and a hilar pattern of blood flow on color and power Doppler imaging [28]. The normal hilum is echogenic because of the reflective interfaces among fat, sinusoids, and connective tissues [28]. With hyperplastic lymph nodes, the normal features of oval shape, echogenic hilum, uniform cortical thickness, and hilar blood flow pattern persist, although the lymph node may be enlarged [28]. A neoplastic lymph node—either from metastases or primary disease such as lymphoma—is characterized by a round or asymmetric shape, nonuniform cortical thickness, loss of the normal echogenic hilum, and a peripheral or mixed pattern of blood flow [28, 29]. Pubic Symphyseal Region The pubic symphyseal region has many anatomic structures that may be the source of groin symptoms, especially in the athlete [30]. One method for ultrasound evaluation is to begin scanning the rectus abdominis muscle in short axis inferior to the umbilicus and then to turn the transducer 90° so that the muscle is viewed in the long axis. The transducer is moved inferior to the pubis, where a common aponeurosis is formed between the insertion of each rectus abdominis and the origin of each adductor longus tendon [30]. 515 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Jacobson et al. The transducer can then be moved more inferior and oblique toward the knee to maintain the long axis with the adductor musculature; external rotation of the hip assists in this evaluation. The transducer can then be repositioned over the symphysis pubis in the transverse plane on the body to evaluate for a joint abnormality. Alternatively, the pubic symphyseal region can be examined beginning over the adductor muscles and can then be moved proximal to visualize the common aponeurosis and the symphysis pubis. One of the most common abnormalities in the symphysis pubis region in athletes involves the common aponeurosis between the rectus abdominis and the adductor musculature [30, 31] (Fig. 5). Although the cause of and the term “sports hernia” is often debated, abnormality of the common aponeurosis has been described as the predominant imaging feature in patients with athletic pubalgia symptoms [31]. At the common aponeurosis, hypoechoic swelling and anechoic clefts may be seen with cortical irregularity [32]. Less commonly, isolated tears of the adductor compartment may be present: A full-thickness tear is characterized by tendon retraction and interposed heterogeneous but predominantly hypoechoic hemorrhage in the acute and subacute setting [31]. Other proposed causes for athletic pubalgia, or sports hernia, include a medial bulge in the posterior wall of the inguinal canal, obturator nerve entrapment, osteitis pubis, tendon tear, and inguinal hernias [31, 33]. Abnormalities of the pubic symphysis, which include hypoechoic capsular distention, anechoic joint fluid, synovial hypertrophy, and cortical irregularity, may also be detected with ultrasound [32]. The superior pubic ramus should also be evaluated for cortical step-off or callus to indicate fracture. A cortical irregularity of the symphysis pubis may be physiologic, related to the unfused growth plates, and may persist in patients until their mid-20s [32]. Inguinal Region Hernias Inguinal region hernias should be considered as a primary or potentially contributing cause for groin symptoms, which include indirect inguinal, direct inguinal, and femoral hernias. With regard to the imaging diagnosis of hernias, one meta-analysis showed a sensitivity of 92.7–100% and specificity of 22.2–100% using ultrasound [34]. The authors stressed that the imaging findings should be correlated with physical examina- 516 tion findings to improve accuracy in the setting of an unclear clinical diagnosis [34]. Ultrasound for the diagnosis of a nonpalpable or clinically occult hernia has proven more difficult [35], with a sensitivity and specificity of 86% and 77%, respectively [36], and another study showing a sensitivity of 33% and specificity of 0% [37]. These results likely reflect the difficulty in performing an ultrasound examination for inguinal hernias and further indicate the need for a clear understanding of sonographic anatomy and the use of a comprehensive protocol. Anatomy There are three essential soft-tissue landmarks for orientation: the lateral margin of the rectus abdominis, the inferior epigastric artery, and the inguinal ligament (Fig. 6A) [38]. These three boundaries outline Hesselbach triangle (i.e., the location of a direct inguinal hernia) (Fig. 6). Just superior to the origin of and lateral to the inferior epigastric artery is the location of the deep or internal inguinal ring (i.e., the origin of an indirect inguinal hernia) (Fig. 6). The region distal to the inguinal ligament and medial to the femoral vasculature is the femoral canal (i.e., the origin of a femoral hernia) (Fig. 6). Valsalva Maneuver An adequate Valsalva maneuver (defined as forced expiratory effort against a closed glottis) is essential during ultrasound examination for hernias. One method to increase intraabdominal pressure is to have the patient “puff the cheeks out” while blowing on the back of the hand. To ensure an adequate Valsalva maneuver, the femoral vein distal to the inguinal ligament should distend. Of note, some hernias are not visible during routine Valsalva maneuvers and may require scanning with the patient standing. Scanning Details To begin ultrasound evaluation for inguinal hernias, the transducer is placed short axis to one of the rectus abdominis muscles inferior to the umbilicus [38]. As the transducer is moved inferior, the inferior epigastric artery is identified deep to the rectus abdominis and is followed moving laterally. Color Doppler imaging may assist in the identification of the inferior epigastric artery, which is then followed inferiorly to its origin at the external iliac artery. If the transducer is moved slightly cephalad, this area is the location of the deep inguinal ring lateral to the inferior epigastric artery. The transducer can then be angled parallel to the inguinal canal to assess for an indirect inguinal hernia during the Valsalva maneuver. The transducer is turned 90° over the inguinal canal, and the Valsalva maneuver is repeated. This latter evaluation short axis to the inguinal canal is essential and important to avoid diagnostic pitfalls, which we discuss later. The transducer is then moved medial in the transverse plane between the inferior epigastric artery and the lateral border of the rectus abdominis to evaluate for a direct inguinal hernia in Hesselbach triangle during the Valsalva maneuver, and the transducer is also turned 90° in the sagittal plane. Finally, the transducer is positioned short axis to the femoral vasculature inferior to the inguinal ligament to assess for a femoral hernia during the Valsalva maneuver. We must emphasize the importance of documenting any hernia in two orthogonal planes: Visualization in the sagittal plane is important to avoid diagnostic pitfalls for all inguinal region hernias. Indirect Inguinal Hernia The characteristic finding of an indirect inguinal hernia is abnormal movement of intraabdominal contents (fat, bowel, or both) through the deep inguinal ring and through the inguinal canal [38–40] (Fig. 7 and Videos S1 and S2 [supplemental videos that can be viewed in the AJR electronic supplement to this article available at www.ajronline. org]). On ultrasound, this abnormality appears as tissue of variable echogenicity moving through the deep inguinal ring, which originates lateral to the inferior epigastric artery. This tissue then moves medial, parallel to the skin surface within the inguinal canal and parallel to the plane of the inguinal ligament. An extensive hernia may extend medial to and potentially through the external or superficial inguinal ring into the scrotum or labia majora and may present as a mass [41]. There is a significant pitfall if one relies on imaging long axis to the inguinal canal. If the intraabdominal contents shift inferiorly during the Valsalva maneuver, the inguinal canal region can move inferior also and can move out of view of the ultrasound imaging. This is why the short-axis view of the inguinal canal (in the sagittal oblique plane) is essential and is necessary to avoid misdiagnosis. In the short axis, the indirect inguinal hernia can be seen moving in and out of the plane adjacent to the spermatic cord (in males) and is visible even if the inguinal canal shifts inferiorly (Figs. 7B and 7C and Video S2). When AJR:205, September 2015 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Ultrasound of the Groin reporting an indirect inguinal hernia, one should measure the hernia short axis in cross section or two dimensions and also indicate the medial extent. Additional diagnostic pitfalls exist when using ultrasound to evaluate for an indirect inguinal hernia. One consideration is a spermatic cord lipoma, which may appear similar to an indirect inguinal hernia on ultrasound [42]. Movement of the abnormal tissue during the Valsalva maneuver cannot be used for this distinction because both spermatic cord lipomas and indirect inguinal hernias may display minimal movement. To distinguish between these two pathologic entities, one can evaluate the deep inguinal ring: A true indirect inguinal hernia will show abnormal tissue extending through this ring. Another diagnostic pitfall is round ligament varicosities seen in pregnant women, which should not be misinterpreted as a vascular malformation [43, 44]. An uncommon finding that can be seen in the inguinal canal in women is a cyst of the canal of Nuck due to a patent processus vaginalis [45]. Direct Inguinal Hernia The characteristic finding of a direct inguinal hernia is focal intraabdominal tissue moving anteriorly through the Hesselbach triangle [38–40] (Fig. 8 and Videos S3 and S4). On ultrasound, this tissue of variable echogenicity will move characteristically in a posterior-to-anterior direction and should be documented in two imaging planes. Relying on only transverse imaging (relative to the body) in an assessment for a direct inguinal hernia is a significant pitfall that may result in diagnostic inaccuracy. In some individuals, the normal intraabdominal contents move inferior with the Valsalva maneuver (Fig. 9 and Videos S5 and S6). Movement of this tissue under the Hesselbach triangle can simulate a direct inguinal hernia when imaged in the transverse plane; however, if the transducer is turned 90° into the sagittal plane, this pitfall can be avoided. In patients without a hernia, it becomes clear that there is no focal movement of abdominal tissue but rather just broad inferior displacement. This displacement is unlike a true direct inguinal hernia where there is focal anterior movement of the intraabdominal contents through the Hesselbach triangle. A true direct inguinal hernia should appear as focal movement of the intraabdominal contents through the Hesselbach triangle in two orthogonal planes. The AJR:205, September 2015 size of the direct hernia, which includes the cephalocaudad, mediolateral, and anteroposterior dimensions, should be described during the Valsalva maneuver. Femoral Hernia The characteristic finding of a femoral hernia is abnormal intraabdominal contents moving in an inferior direction through the femoral canal [38–40]. On ultrasound, tissue of variable echogenicity will be seen extending inferiorly, most commonly medial to the femoral vein, potentially causing compression of the femoral vein (Fig. 10 and Videos S7 and S8). The abnormal inferior movement of tissue should be seen in two orthogonal planes—both in the short axis and in the long axis. Reporting Most inguinal region hernias involve abnormal movement of isoechoic or hyperechoic intraabdominal fat. Bowel showing the characteristic circular echotexture with possible peristalsis may also be visible. The size of a hernia should be described in all dimensions rather than using ambiguous terms such as “small” or “large.” It is also important to describe what is in the hernia (fat, bowel, or both) and if the contents are reducible or irreducible. In the situation of an incarcerated hernia with ischemia, ultrasound is often ineffective given the patient’s symptoms and CT may be indicated. Summary There are many potential pathologic conditions in a patient with groin symptoms. Because symptoms may be multifactorial and history may be ambiguous or misleading, a protocol-driven evaluation with ultrasound is recommended. The hip joint is evaluated for effusion, synovitis, and labral abnormalities. The muscles and tendons, including the common aponeurosis at the pubic symphysis, are evaluated for tendinosis and tears. Dynamic evaluation should be considered to assess for snapping hip syndrome. Iliopsoas bursal distention and lymph node enlargement are other considerations. Last, inguinal region hernias must be evaluated during the Valsalva maneuver and documented in two orthogonal planes to avoid several important diagnostic pitfalls. Acknowledgment Illustrations courtesy of Danielle Dobbs, Ann Arbor, MI. References 1. Jacobson JA. Musculoskeletal sonography and MR imaging: a role for both imaging methods. Radiol Clin North Am 1999; 37:713–735 2. Klauser AS, Tagliafico A, Allen GM, et al. Clinical indications for musculoskeletal ultrasound: a Delphi-based consensus paper of the European Society of Musculoskeletal Radiology. Eur Radiol 2012; 22:1140–1148 3. Jacobson JA. Fundamentals of musculoskeletal ultrasound, 1st ed. Philadelphia, PA: Saunders Elsevier, 2007:2 4. Jamadar DA, Jacobson JA, Caoili EM, et al. Musculoskeletal sonography technique: focused versus comprehensive evaluation. AJR 2008; 190:5–9 5. Jacobson JA. Musculoskeletal ultrasound and MRI: which do I choose? Semin Musculoskelet Radiol 2005; 9:135–149 6. Robben SG, Lequin MH, Diepstraten AF, den Hollander JC, Entius CA, Meradji M. Anterior joint capsule of the normal hip and in children with transient synovitis: US study with anatomic and histologic correlation. Radiology 1999; 210:499–507 7. Koski JM, Anttila PJ, Isomaki HA. Ultrasonography of the adult hip joint. Scand J Rheumatol 1989; 18:113–117 8. Moss SG, Schweitzer ME, Jacobson JA, et al. Hip joint fluid: detection and distribution at MR imaging and US with cadaveric correlation. Radiology 1998; 208:43–48 9. Weybright PN, Jacobson JA, Murry KH, et al. Limited effectiveness of sonography in revealing hip joint effusion: preliminary results in 21 adult patients with native and postoperative hips. AJR 2003; 181:215–218 10. Ostlere S. How to image metal-on-metal prostheses and their complications. AJR 2011; 197:558–567 11. Fink B, Gebhard A, Fuerst M, Berger I, Schafer P. High diagnostic value of synovial biopsy in periprosthetic joint infection of the hip. Clin Orthop Relat Res 2013; 471:956–964 12. Kung JW, Yablon C, Huang ES, Hennessey H, Wu JS. Clinical and radiologic predictive factors of septic hip arthritis. AJR 2012; 199:868–872 13. Strouse PJ, DiPietro MA, Adler RS. Pediatric hip effusions: evaluation with power Doppler sonography. Radiology 1998; 206:731–735 14. Pai VR, van Holsbeeck M. Synovial osteochondromatosis of the hip: role of sonography. J Clin Ultrasound 1995; 23:199–203 15. Blankenbaker DG, De Smet AA, Keene JS, Fine JP. Classification and localization of acetabular labral tears. Skeletal Radiol 2007; 36:391–397 16. Jin W, Kim KI, Rhyu KH, et al. Sonographic evaluation of anterosuperior hip labral tears with magnetic resonance arthrographic and surgical correlation. J Ultrasound Med 2012; 31:439–447 17. Bedi A, Kelly BT. Femoroacetabular impinge- 517 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Jacobson et al. ment. J Bone Joint Surg Am 2013; 95:82–92 18. Buck FM, Hodler J, Zanetti M, Dora C, Pfirrmann CW. Ultrasound for the evaluation of femoroacetabular impingement of the cam type: diagnostic performance of qualitative criteria and alpha angle measurements. Eur Radiol 2011; 21:167–175 19. Mervak BM, Morag Y, Marcantonio D, Jacobson J, Brandon C, Fessell D. Paralabral cysts of the hip: sonographic evaluation with magnetic resonance arthrographic correlation. J Ultrasound Med 2012; 31:495–500 20. Guillin R, Cardinal E, Bureau NJ. Sonographic anatomy and dynamic study of the normal iliopsoas musculotendinous junction. Eur Radiol 2009; 19:995–1001 21. Polster JM, Elgabaly M, Lee H, Klika A, Drake R, Barsoum W. MRI and gross anatomy of the iliopsoas tendon complex. Skeletal Radiol 2008; 37:55–58 22. Balius R, Pedret C, Blasi M, et al. Sonographic evaluation of the distal iliopsoas tendon using a new approach. J Ultrasound Med 2014; 33:2021–2030 23. Deslandes M, Guillin R, Cardinal E, Hobden R, Bureau NJ. The snapping iliopsoas tendon: new mechanisms using dynamic sonography. AJR 2008; 190:576–581 24. Gyftopoulos S, Rosenberg ZS, Schweitzer ME, Bordalo-Rodrigues M. Normal anatomy and strains of the deep musculotendinous junction of the proximal rectus femoris: MRI features. AJR 2008; 190:[web]W182–W186 25. Park SM, Baek JH, Ko YB, Lee HJ, Park KJ, Ha YC. Management of acute calcific tendinitis around the hip joint. Am J Sports Med 2014; 42:2659–2665 26. Wunderbaldinger P, Bremer C, Schellenberger E, Cejna M, Turetschek K, Kainberger F. Imaging features of iliopsoas bursitis. Eur Radiol 2002; 12:409–415 27. Bontumasi N, Jacobson JA, Caoili E, Brandon C, Kim SM, Jamadar D. Inguinal lymph nodes: size, number, and other characteristics in asymptomatic patients by CT. Surg Radiol Anat 2014; 36:1051–1055 28. Esen G. Ultrasound of superficial lymph nodes. Eur J Radiol 2006; 58:345–359 29. Roberto S, Valeria B, Roberto del V, Raffaella M, Chiara FA, Leopoldo R. Analysis by high resolution ultrasound of superficial lymph nodes: anatomical, morphological and structural variations. Clin Imaging 2014; 38:96–99 30. Omar IM, Zoga AC, Kavanagh EC, et al. Athletic pubalgia and “sports hernia”: optimal MR imaging technique and findings. RadioGraphics 2008; 28:1415–1438 31. Zoga AC, Kavanagh EC, Omar IM, et al. Athletic pubalgia and the “sports hernia”: MR imaging findings. Radiology 2008; 247:797–807 32. Robinson P, Bhat V, English B. Imaging in the assessment and management of athletic pubalgia. Semin Musculoskelet Radiol 2011; 15:14–26 33. Garvey JF, Read JW, Turner A. Sportsman hernia: what can we do? Hernia 2010; 14:17–25 34. Robinson A, Light D, Nice C. Meta-analysis of sonography in the diagnosis of inguinal hernias. J Ultrasound Med 2013; 32:339–346 35. Robinson P, Hensor E, Lansdown MJ, Ambrose NS, Chapman AH. Inguinofemoral hernia: accuracy of sonography in patients with indeterminate clinical features. AJR 2006; 187:1168–1178 36. Robinson A, Light D, Kasim A, Nice C. A system- A atic review and meta-analysis of the role of radiology in the diagnosis of occult inguinal hernia. Surg Endosc 2013; 27:11–18 37. Miller J, Cho J, Michael MJ, Saouaf R, Towfigh S. Role of imaging in the diagnosis of occult hernias. JAMA Surg 2014; 149:1077–1080 38. Jamadar DA, Jacobson JA, Morag Y, et al. Sonography of inguinal region hernias. AJR 2006; 187:185–190 39. Brandon CJ, Jacobson JA, Fessell D, et al. Groin pain beyond the hip: how anatomy predisposes to injury as visualized by musculoskeletal ultrasound and MRI. AJR 2011; 197:1190–1197 40. Stavros AT, Rapp C. Dynamic ultrasound of hernias of the groin and anterior abdominal wall. Ultrasound Q 2010; 26:135–169 41. Patel B, Zivin S, Panchal N, Wilbur A, Bresler M. Sonography of female genital hernias presenting as labia majora masses. J Ultrasound Med 2014; 33:155–159 42. Rosenberg R, Williamson MR. Lipomas of the spermatic cord and testis: report of two cases. J Clin Ultrasound 1989; 17:670–674 43. Polat AV, Aydin R, Polat AK, Kececi IS, Karahan G, Taskin GO. Round ligament varicosities: a rare cause of groin swelling in pregnancy. Abdom Imaging 2013; 38:1178–1181 44. Ryu KH, Yoon JH. Ultrasonographic diagnosis of round ligament varicosities mimicking inguinal hernia: report of two cases with literature review. Ultrasonography 2014; 33:216–221 45. Ozel A, Kirdar O, Halefoglu AM, et al. Cysts of the canal of Nuck: ultrasound and magnetic resonance imaging findings. J Ultrasound 2009; 12:125–127 B Fig. 1—24-year-old woman with normal anterior hip. A, Ultrasound image with transducer in sagittal oblique plane long axis to femoral neck (N) shows femoral head (H), acetabulum (A), labrum (curved arrow), and anterior capsule (arrowhead). Note reflected capsule (straight arrow) over femoral neck. B, Ultrasound image with transducer in transverse plane over femoral head (H) shows iliopsoas muscle (IP) and tendon (arrow). S = sartorius. (Fig. 1 continues on next page) 518 AJR:205, September 2015 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Ultrasound of the Groin C Fig. 1 (continued)—24-year-old woman with normal anterior hip. C, Ultrasound image with transducer in transverse oblique plane over ilium shows psoas major muscle (Pm) and tendon (Pt) and rectus femoris direct head (RF). Note lateral (Im-L) and medial (Im-M) muscle fibers of iliacus with interposed septation (arrowhead). AIIS = anterior inferior iliac spine, V = femoral vein. Fig. 3—17-year-old girl with labral detachment and paralabral cyst. Ultrasound image with transducer in oblique sagittal plane long axis to femoral neck shows labrum (asterisk) that is detached (arrow) from acetabulum (A) and associated paralabral cyst (arrowheads). H = femoral head. Fig. 2—19-year-old woman with pigmented villonodular synovitis. Ultrasound image with transducer in oblique sagittal plane long axis to femoral neck (N) shows heterogeneous hypoechoic synovial hypertrophy (arrows) that predominantly distends anterior recess. Note bone erosion (arrowheads). H = femoral head. Fig. 4—38-year-old woman with rectus femoris calcific tendinosis. Ultrasound image in sagittal plane shows calcium hydroxyapatite deposition (arrow) within direct head of rectus femoris (arrowheads). Note close proximity of calcium hydroxyapatite to femoral head (H). AIIS = anterior inferior iliac spine. Fig. 5—40-year-old man with common aponeurosis injury. Ultrasound image with transducer in sagittal oblique plane over pubis (P) shows hypoechoic thickening of common aponeurosis (straight arrows) associated with cortical irregularity. Note adductor longus tendon (arrowheads) and rectus abdominis (curved arrow). AJR:205, September 2015 519 Jacobson et al. Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Fig. 6—Illustrations of inguinal region without and with hernias. (Drawing by Dobbs D, used with permission) A, Illustration of anterior inguinal region shows rectus abdominis (R), inferior epigastric vessels (arrowhead), and inguinal ligament (curved arrow), which outlines Hesselbach triangle (H). Note deep inguinal ring (straight arrow) at origin of inguinal canal. B, Illustration shows direct inguinal hernia at Hesselbach triangle (arrowhead); indirect inguinal hernia with bowel extending through deep ring, inguinal canal, and superficial ring (curved arrow); and femoral hernia extending through femoral canal (straight arrow). Note direction of specific hernias during Valsalva maneuver, with direct inguinal hernia moving anterior, indirect inguinal hernia moving medial and to lesser extent inferior, and femoral hernia moving inferior. A B A B Fig. 7—31-year-old man with right-sided indirect inguinal hernia. A, Ultrasound image with transducer in axial oblique plane long axis to inguinal canal during Valsalva maneuver shows fat-containing indirect inguinal hernia (white arrows) traversing internal ring (arrowheads) lateral to epigastric and external iliac vessels (V) and coursing medial parallel to skin surface within inguinal canal; left side of image is lateral. Black arrow indicates direction of movement. See Video S1, a supplemental video; it can be viewed in AJR electronic supplement to this article, available at www.ajronline.org. B and C, Ultrasound image (B) and illustration (C) in sagittal oblique plane short axis to inguinal canal during Valsalva maneuver show indirect hernia in short axis (straight arrows) adjacent to spermatic cord (curved arrow) in inguinal canal; left side of image is cephalad. Wavy arrow points to normal intraabdominal contents. See Video S2. (Drawing by Dobbs D, used with permission) C 520 AJR:205, September 2015 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Ultrasound of the Groin E AJR:205, September 2015 A B C D Fig. 8—63-year-old man with right-sided direct inguinal hernia. A, Ultrasound image in transverse plane over Hesselbach triangle shows direct inguinal hernia (white arrows) extending in posterior-to-anterior direction during Valsalva maneuver, medial to inferior epigastric and external iliac vessels (V); left side of image is lateral. Black arrow indicates direction of movement. See Video S3 in AJR electronic supplement to this article, available at www.ajronline.org. B and C, Axial MR images obtained during rest (B) and Valsalva maneuver (C) show direct inguinal hernia (white arrows, C) medial to vasculature (V) extending anterior (arrowhead, C) during Valsalva maneuver with black arrow indicating direction of hernia. Note bowel-containing left direct inguinal hernia with gas (black arrow, C). D, Ultrasound image in sagittal plane over Hesselbach triangle shows focal direct inguinal hernia (straight white arrows) and adjacent spermatic cord (curved arrow); left side of image is cephalad. Straight black arrow indicates posterior-to-anterior direction of hernia in continuity with intraabdominal contents (wavy arrow). See Video S4. E, Sagittal MR image obtained during Valsalva maneuver shows focal anterior movement (black arrow) of intraabdominal contents through Hesselbach triangle (straight white arrows). Note spermatic cord (curved arrow). (Fig. 8 continues on next page) 521 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Jacobson et al. F G Fig. 8 (continued)—63-year-old man with right-sided direct inguinal hernia. F and G, Illustrations in sagittal plane obtained during rest (F) and Valsalva maneuver (G) show focal and anterior movement of direct inguinal hernia (straight arrows, G) in continuity with intraabdominal contents (wavy arrow). Curved arrow = spermatic cord. (Drawings by Dobbs D, used with permission) A B 522 Fig. 9—42-year-old man with right-sided pseudodirect inguinal hernia. A, Ultrasound image with transducer in transverse plane over Hesselbach triangle during Valsalva maneuver shows normal intraabdominal contents (arrows), medial to inferior epigastric and external iliac vessels (V); left side of image is lateral. See Video S5 in AJR electronic supplement to this article, available at www.ajronline.org. B and C, Ultrasound image (B) and illustration (C) in sagittal plane over Hesselbach triangle during Valsalva maneuver show diffuse movement of normal intraabdominal contents without focal anterior movement, bulge, or hernia (wavy arrows); left side of image is cephalad. Curved arrow = spermatic cord. See Video S6. (Drawing by Dobbs D, used with permission) C AJR:205, September 2015 Downloaded from www.ajronline.org by 37.44.207.95 on 01/12/17 from IP address 37.44.207.95. Copyright ARRS. For personal use only; all rights reserved Ultrasound of the Groin A B Fig. 10—59-year-old woman with right-sided femoral hernia. A, Ultrasound image in transverse plane inferior to inguinal ligament with transducer over femoral canal shows focal femoral hernia (arrows) compressing femoral vein (V) during Valsalva maneuver. A = femoral artery; left side of image is lateral. See Video S7 in AJR electronic supplement to this article, available at www.ajronline.org. B, Ultrasound image in sagittal plane with transducer over femoral canal and medial to femoral vasculature shows focal femoral hernia (white arrows) during Valsalva maneuver. Black arrow indicates inferior direction of movement during Valsalva maneuver; left side of image is cephalad. See Video S8. F O R YO U R I N F O R M AT I O N A data supplement for this article can be viewed in the online version of the article at: www.ajronline.org. AJR:205, September 2015 523