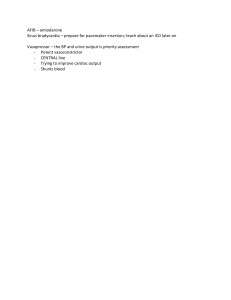
Research Article ORL DOI: 10.1159/000514458 Received: November 24, 2020 Accepted: January 11, 2021 Published online:■■■ Sphenoid Sinus: Pneumatization and Septation Patterns in a Hispanic Population José Luis Treviño-Gonzalez a Félix Maldonado-Chapa a Joel Adrián Becerra-Jimenez b Germán Armando Soto-Galindo a Josefina Alejandra Morales-del Angel a aDepartment of Otolaryngology-Head and Neck Surgery, Faculty of Medicine and University Hospital “Dr. José Eleuterio González”, Monterrey, Mexico; bDepartment of Radiology, Faculty of Medicine and University Hospital “Dr. José Eleuterio González”, Monterrey, Mexico Abstract Introduction: Pneumatization of the sphenoid sinus (SS) varies widely among different ethnic groups. Information regarding the prevalence and significance of SS variants among Hispanic groups is limited. This study aims to describe and analyze pneumatization and septation patterns of the SS in a Hispanic population. Methods: A total of 160 paranasal sinus computed tomographies were reviewed by a head and neck-specialized radiologist and 2 otolaryngologists. Results: The postsellar and sellar types were the most frequent patterns of pneumatization observed, with a prevalence of 52.5 and 40%, respectively. Accessory septations were present in 59.4% of the patients. Septa were inserting over the internal carotid artery (ICA) in 43.8% and over the optic nerve in 17.5% of the population. No significant association (p > 0.05) was observed when comparing the different accessory septation patterns among the types of the SS. The frequency of septa inserting on the ICA was significantly higher in postsellar types (p < 0.001). Pneumatization of the anterior clinoid process, pterygoid processes, and greater karger@karger.com www.karger.com/orl © 2021 S. Karger AG, Basel wing was present in 20, 17.5, and 45.9% of the sinuses, respectively. Onodi cells were encountered in 40% of the sinuses. There were no significant differences in any of the pneumatization and septation variables when compared by gender and age (p > 0.05). Discussion/Conclusion: Differences regarding anatomical variants and septations of the SS were observed in our study when compared with findings reported in other ethnic groups. Preoperative assessment of the anatomical variants of the SS in Mexican patients is imperative to select the most optimal surgical approach and prevent iatrogenic injuries to related neurovascular structures. © 2021 S. Karger AG, Basel Introduction The sphenoid sinuses (SSs) represent one of the most variable structures in the body. Their pneumatization process starts between the third and the fourth year of life, ending around the age of 16 years. Pneumatization of the sphenoid bone frequently is asymmetrical and might extend to an anterior clinoid process (ACP), posterior clinoid process, greater wings of the sphenoid bone (GWS), Correspondence to: José Luis Treviño-Gonzalez, jose.trevinog @ uanl.mx Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM Keywords Computed tomography · Sinus surgery · Skull base b c d pterygoid process (PP), and dorsum sellae (DS) [1]. This complex anatomy is further complicated by the different complete or incomplete septation patterns that could be present [2]. Computed tomography (CT) is the gold standard for evaluating the anatomy and pathology of the paranasal sinuses [3]. The anatomy of the SS has been acquiring growing importance during the past decades due to its relevance for different transsphenoidal endoscopic surgical approaches not only for pituitary lesions but also for lesions arising in the perisellar region, clivus, petroclival region, and cavernous sinuses [4]. In these cases, it is of utmost importance to assess preoperatively anatomical variants of pneumatization by CT scan as an extensive pneumatization might result in bulging of significant neurovascular structures, such as the internal carotid artery (ICA) or optic nerve (ON), into the aired space. Their exposure within the SS might result in iatrogenic damage to these structures, resulting in significant hemorrhage or permanent blindness [5]. Moreover, traumatic disinsertion of the main or an accessory septum from the bony canal of these neurovascular structures could cause the same complications [1]. 2 ORL DOI: 10.1159/000514458 A highly variable prevalence of the different pneumatization and septation patterns have been reported among several ethnic groups [3, 6]. However, growing but limited data exist on the Hispanic population in which to support on. The scope of advanced endoscopic skull base and paranasal sinus surgery has been consistently expanding, and this fact stresses the importance of studying the SS anatomy and the implications of the presence or absence of anatomical variants in the surgery´s complexity and related risks. This study aims to describe the pneumatization patterns of the SS and its septations and establish a relationship between these variants with the insertion of a septum over the ICA or ON in a Hispanic adult population. Materials and Methods This retrospective and descriptive study was conducted in the University Hospital “José Eleuterio González,” a tertiary referral center in Monterrey, México, according to the principles of the Declaration of Helsinki and was approved by the local Research and Ethics Committee, registered with the key OT16-00004. Paranasal sinus CTs of the last 160 patients complying with the inclu- Treviño-Gonzalez et al. Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM Fig. 1. Sphenoidal sinus types: conchal (a), presellar (b), sellar (c), and postsellar (d). a * * Fig. 2. a Accessory septum inserting on the ICA (asterisk). b Main septum inserting on a b sion and exclusion criteria were reviewed. The study population was Mexicans aged 18 years and older. The exclusion criteria were evidence of acute or chronic rhinosinusitis involving the SS, skull base fractures, sinus tumors, skull base tumors, craniofacial deformities, and history of surgery of the paranasal sinuses or skull base. All CT scans were obtained from the radiology department and contained axial slices of 1.25 mm and sagittal and coronal reconstructions from the vertex of the cranium to the level of the hyoid bone in a high-definition bone window. These were obtained with a General Electric Medical Systems Light Speed VCT, with a tube voltage of 120 Kv, 18 effective mAs, and a field of view of 14.2 × 27.8 cm. CT scans were reviewed by 3 investigators to reach a consensus, a radiologist with training in head and neck imaging and 2 otolaryngologists. In case of discrepancies among investigators, another head and neck specialized radiologist was consulted to reach a mutual consensus. Along with sex and age, the following variables in the CT scans were investigated: • SS pneumatization: It is defined as conchal (posterior wall of the sinus ends anterior to the sellae), presellar (pneumatization ends anterior to the sellae, forming the posterior wall of the sinus), sellar (pneumatization ends between the anterior and posterior border of the sellae), and postsellar (pneumatization extending beyond the posterior limit of the sellae) (Fig. 1). This variable was best evaluated in the sagittal plane. • SS dominance: It is classified as none, right, or left, according to the sinus with higher volume. • SS accessory septation: It is classified as none, 1 incomplete, 1 complete, 2 complete, and 3 or more complete septa. Septa were evaluated using the axial and coronal planes. • Septation insertion (main or accessory septa) over the bony canal of the ICA (Fig. 2a) or ON (Fig. 2b). For the ON, this was best evaluated in a coronal plane, whereas the ICA was evaluated in the axial and coronal planes. • Pneumatization of the ACP: This was evaluated in the coronal and axial planes (Fig. 3a). • Pneumatization of the DS: It is evaluated in the sagittal and axial planes (Fig. 3b, c). • Pneumatization of the GWS: It is defined as pneumatization extending laterally to a vertical plane crossing the foramen rotundum, creating a lateral recess, best evaluated in the coronal plane. • Pneumatization of PP: It is defined as pneumatization extending inferiorly to a horizontal line crossing the vidian canal, evaluated in the coronal plane. • Pneumatization of ipsilateral GWS and PP (full lateral recess) (Fig. 3d). • Presence of Onodi cells (OC): This variable was evaluated in the sagittal, axial, and coronal planes (Fig. 4). Dependence between variables was investigated using the χ2 test. A value of p < 0.05 was considered statistically significant. Statistical evaluations were performed using the Statistical Package for Social Sciences (SPSS) version 20.0. Sphenoid Sinus: Pneumatization and Septation Patterns ORL DOI: 10.1159/000514458 Results We analyzed a total of 160 paranasal sinus CTs. There were 89 (55.6%) male and 71 (44.4%) female cases. The mean age was 45.67 ± 17.46 (18–88) years. The mean age for the male group was 46.91 ± 18.47 (18–87) years, whereas for the female group, it was 44.11 ± 16.10 (20–88) years. There were no significant differences in age among groups (p > 0.05). The prevalence of type pneumatization of the SS, dominance, accessory septations, insertion of septation over ICA and ON, pneumatization of ACP, DS, GWS, and PP by the sinus is shown in Table 1. We found pneumatization of any the ACP in 27.5% of the population, 25% of the DS, 26.7% of the PP, and 57.5% of GWS. Pneumatization and septation patterns of the SS were analyzed according to sex and are also shown in Table 1. There were no significant differences between the pneumatization of different parts of the sphenoid bone according to sex stratification. In the same manner, there were no significant differences when the same patterns were analyzed according to age by stratifying patients in decades of life (p > 0.05). The prevalence of the accessory septa configurations according to the type of SS pneumatization is depicted in Table 2. We observed a significant increase in the frequency of no accessory septations in presellar compared to sellar and postsellar configurations (p = 0.03). 3 Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM the ON (asterisk). ICA, internal carotid artery; ON, optic nerve. * * a b Fig. 3. Pneumatization of the right ACP (asterisk) (a), sagittal view showing pneumatization of the DS (asterisk) (b), axial * c The prevalence of septation insertion (main or accessory) over the ON and ICA according to SS pneumatization is shown in Table 3. We found that the postsellar pneumatization was associated with a significant ­increase in the insertion of bony septations on the ICA (p < 0.001). We determined the prevalence of distinct patterns of lateral pneumatization (PP, GWS, or both) according to SS pneumatization to correlate anterior-posterior to lateral pneumatization (Table 4). We observed a significant association for all the different lateral pneumatization patterns to the anterior-posterior pneumatization (p < 0.05), finding a higher frequency of lateral pneumatization in sellar and postsellar configurations. The prevalence of at least 1 OC in our population was 53.8%. The frequency right OC for different SS configurations was 0 (0%) for conchal, 3 (27.3%) for presellar, 29 (45.3%) for sellar, and 33 (39.3%) for postsellar (p = 0.543). Left OC were present in 0 (0%), 7 (63.6%), 24 (37.5%), 32 (38.1%), respectively (p = 0.319). Similarly, bilateral OC were observed in 0 (0%) of the conchal, in 2 (18.2%) of presellar, in 18 (28.1%) of sellar, and in 22 (26.2%) of postsellar SS pneumatization (p = 0.839). 4 ORL DOI: 10.1159/000514458 * d * * Fig. 4. Bilateral Onodi cells (asterisks). Discussion/Conclusion Radiologic assessment and recognition of aberrant patterns of pneumatization of the paranasal sinuses are of major importance before performing endoscopic sinus surgery. The presence of anatomical variants within paranasal sinuses might facilitate or difficult access to the parasellar region and influence the risk of iatrogenic inTreviño-Gonzalez et al. Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM view showing pneumatization of the dorsum sellae (asterisk) (c), and pneumatization of full bilateral lateral recesses (asterisks) (d). ACP, anterior clinoid process; DS, dorsum sellae. * Table 1. Pneumatization and septation patterns according to sex SS pneumatization Conchal Presellar Sellar Postsellar SS dominancy Right Left None Accessory septations None Incomplete septum One complete septum Two complete septa ≥3 complete septa Septa insertion on ON Septa insertion on ICA Pneumatization of ACP Right Left Bilateral Pneumatization of DS Lateral pneumatization of SS Right PP Left PP Bilateral PP Right GWS Left GWS Bilateral GWS Full right lateral recess Full left lateral recess Full bilateral lateral recess Onodi cell Right Left Bilateral Total (n = 160) (%) Male (n = 89) (%) Female (n = 71) (%) p value 1 (0.6) 11 (6.9) 64 (40) 84 (52.5) 1 (1.1) 8 (9) 33 (37.1) 47 (52.8) 0 (0) 3 (4.2) 31 (43.7) 37 (52.1) 0.37 0.237 0.398 0.93 54 (33.8) 73 (45.6) 33 (20.6) 30 (33.7) 42 (47.2) 17 (19.1) 24 (33.8) 31 (43.7) 16 (22.5) 0.99 0.656 0.594 65 (40.6) 30 (18.8) 38 (23.8) 24 (15) 3 (1.9) 28 (17.5) 70 (43.8) 31 (34.8) 20 (22.5) 25 (28.1) 12 (13.5) 1 (1.1) 14 (15.7) 40 (44.9) 34 (47.9) 10 (14.1) 13 (18.3) 12 (16.9) 2 (2.8) 14 (19.7) 30 (42.3) 0.095 0.177 0.149 0.547 0.433 0.51 0.733 32 (20) 32 (20) 20 (12.5) 40 (25) 20 (22.5) 20 (22.5) 13 (14.6) 23 (25.8) 12 (16.9) 12 (16.9) 7 (9.85) 17 (23.9) 0.381 0.381 0.367 0.783 28 (17.5) 28 (17.5) 13 (8.1) 68 (42.5) 79 (49.4) 55 (34.4) 27 (16.9) 28 (17.5) 13 (8.1) 14 (17.5) 19 (21.3) 7 (7.7) 35 (39.3) 43 (48.3) 28 (31.5) 14 (15.7) 19 (21.3) 7 (7.7) 14 (19.7) 9 (12.7) 6 (8.4) 33 (46.5) 36 (50.7) 27 (38) 13 (18.3) 9 (12.7) 6 (8.4) 0.51 0.151 0.893 0.363 0.764 0.385 0.665 0.151 0.893 65 (40.6) 63 (39.4) 42 (26.3) 35 (39.3) 34 (38.2) 22 (24.7) 30 (42.3) 29 (40.8) 20 (28.2) 0.708 0.734 0.622 jury to related neurovascular structures [7]. The Assessment of Pneumatization of Paranasal Sinuses (APPS) is a recently introduced and validated metric which evaluates the presence of anatomical variants among all the paranasal sinuses [8]. This instrument contains 2 different items regarding the SS: ACP pneumatization and pneumatization lateral to a line crossing through the foramen rotundum and vidian canal. The APSS has also been demonstrated to correlate strongly with the total sinus vol- ume, thus can be used as a reliable measure of the overall prevalence of different anatomical configurations in large populations [9, 10]. The prevalence of the anatomical variants of the SS cannot be generalized as incredibly significant differences have been observed among different ethnic groups [3]. These observations along with the lack of data in our population motivated the development of our study. Sphenoid Sinus: Pneumatization and Septation Patterns ORL DOI: 10.1159/000514458 5 Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM SS, sphenoidal sinus; ON, optic nerve; ICA, internal carotid artery; ACP, anterior clinoid process; DS, dorsum sellae; PP, pterygoid process; GWS, greater wing of the sphenoid. Chi-squared test was used to assess dependency between variables (p < 0.05 was considered statistically significant). Table 2. Number of accessory septations according to type of SS Accessory septation Conchal, n (%) Presellar, n (%) Sellar, n (%) Postsellar, n (%) p value None One incomplete septum One complete septum Two complete septa ≥3 complete septa 0 (0) 1 (100) 0 (0) 0 (0) 0 (0) 9 (81.8) 2 (18.2) 0 (0) 0 (0) 0 (0) 25 (39) 12 (18.8) 14 (21.9) 13 (20.3) 0 (0) 31 (36.9) 15 (17.9) 24 (28.6) 11 (13) 3 (3.6) 0.03* 0.223 0.176 0.287 0.429 SS, sphenoidal sinus. *Statistically significant according to χ2 test (p < 0.05). Table 3. Frequency of septa insertion over ON and ICA according to the type ofSS Insertion of septa Conchal, n (%) Presellar, n (%) Sellar, n (%) Postsellar, n (%) p value ICA ON 0 (0) 0 (0) 0 (0) 0 (0) 17 (26.6) 11 (17.2) 53 (63.1) 17 (20.2) <0.001* 0.394 ICA, internal carotid artery; ON, optic nerve; SS, sphenoidal sinus. *Statistically significant according to χ2 test (p < 0.05). Table 4. Lateral pneumatization according to type of SS Lateral pneumatization degree Conchal, n (%) Presellar, n (%) Sellar, n (%) Postsellar, n (%) p value Right PP Left PP Bilateral PP Right GWS Left GWS Bilateral GWS Full right lateral recess Full left lateral recess Full bilateral lateral recess 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 1 (9.1) 0 (0) 0 (0) 1 (9.1) 0 (0) 0 (0) 1 (9.1) 0 (0) 0 (0) 5 (7.8) 3 (4.7) 1 (1.6) 18 (28.1) 22 (34.4) 15 (23.4) 5 (7.8) 3 (4.7) 1 (1.6) 22 (26.2) 25 (29.8) 12 (14.3) 49 (58.3) 57 (67.9) 40 (47.6) 22 (26.2) 25 (29.8) 12 (14.3) 0.025* <0.001* 0.029* <0.001* <0.001* 0.001* 0.025* <0.001* 0.029* SS Type Pneumatization Hammer and Radberg first classified SS pneumatization into conchal, sellar, presellar, and postsellar [3]. This classification emphasizes posterior pneumatization in relation to the sellae and predicts the surgical corridor used for transsphenoidal surgeries [11]. Sellar and postsellar types of SS facilitate endoscopic procedures as the 6 ORL DOI: 10.1159/000514458 SS presents thinner walls and less bone drilling is required to access the sellae. This might also represent a risk as increased pneumatization is also associated with bulging of neurovascular structures or dehiscence of their bony canals. Endoscopic transsphenoidal procedures are less suitable for presellar and conchal types as perforation through a thicker SS is required [12]. In our Treviño-Gonzalez et al. Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM PP, pterygoid process; GWS, greater wing of the sphenoid; SS, sphenoidal sinus. * Statistically significant according to χ2 test (p < 0.05). Table 5. Prevalence of sphenoidal types and other anatomical variants among different populations in several CT-based studies Study Population Conchal, Presellar, Sellar, Postsellar, AS, % % % % % ACP, % DS, % Present study Gibelli et al. [1] Jaworek et al. [2] Lu et al. [4] Gibelli et al. [7] Hiremath et al. [11] Tawfik et al. [12] Anusha et al. [13] Dal Secchi et al. [14] Tomovic et al. [15] Rahmati et al. [16] Asal et al. [24] Siricki et al. [25] Arslan et al. [26] Hewaidi et al. [27] Kazkayasi et al. [28] Ilków et al. [29] Refaat et al. [30] Mexican Italian Croatian Chinese Italian Indian Egyptian Malaysian Brazilian American Iranian Turkish Turkish Turkish Libyan Turkish Polish Turkish 0.6 6.9 40.0 6.0 0.0 0.0 3.2 0.3 0.0 1.8 0.0 28.5 8.0 1.2 0.0 6.7 2.0 7.3 1.9 65.5 77.3 98.8 96.8 93.0 98.0 47.6 14.6 0.0 28.2 39.4 PP, % 52.5 59.4 78.1 78.0 27.5 25.0.0 26.7 14.7 62.7 20.3 32.9 0.0 11.6 46.3 39.0 43.5 69.8 17.9 12.0 13.0 33.1 43.7 29.3 6.0 15.3 17.2 38.9 43.3 86.0 32.4 27.6 12.0 GWS, OC, % % 57.5 53.8 9.3 31.8 1.0 47.0 18.0 14.3 39.6 29.3 16.0 29.0 39.7 26.5 23.0 20.0 10.0 22.9 population, higher pneumatized SS were more frequent; 52.5 and 40% were postsellar and sellar, respectively. This result is different from that observed in Italian, Egyptian, and Malaysian populations in whom sellar configurations have been shown to be more frequent with a prevalence of 74, 96.8, and 93%, respectively [7, 12, 13]. In 2 of these studies, postsellar pneumatization was not observed in any patient [12, 13]. Dal Secchi et al. [14] reviewed CT scans of 90 Brazilian patients; however, sellar and postsellar were reported and conjoined into 1 category, with a prevalence of 98%. Our findings seem to concur with studies performed in Indians, a Hispanic subgroup in a US population, and Iranians, in whom postsellar pneumatization has been observed as the most predominant subtype [11, 15, 16]. All the mentioned investigations are CT-based studies. Several other investigations performed in cadavers with less sample size have also been undertaken, and results are also variable among different ethnicities [17, 18]; however, this method might not be as accurate as the CT. The conchal type is constantly rare among studies and usually represents an incomplete pneumatization process [13]. We only observed 1 case of conchal SS in a masculine patient aged 48 years (Table 5). SS Septation Accessory septations have also been widely studied among different populations, with contrasting observations. The rate of accessory septa has been observed to range from 14.6% up to 78.1% among studies performed in distinct populations [1,2, 12, 13]. When present, 2 septa was the most frequent variant in 2 studies. We observed accessory septations in 59.4% of our population (Table 5). When present, more frequently, they were complete, traversing the full SS. Fewer studies looking for the insertion of septations over the ICA or ON have been performed, and in the same manner, several differences have been noted among studied populations. When considering the rate of septations over the ICA and ON in separate populations, authors have reported prevalence ranging from 20.8 to 89% for the ICA [1, 19, 20] and 7.7% for the ON [1]. By individual sinuses, 2 studies from Turkey and 1 from Egypt reported a prevalence of insertion over the ICA of 26.7, 8, 12.9%, respectively. These same research teams reported a prevalence of insertion over the ON of 19.6, 8, and 5.9% [21–23]. We observed higher rates of these parameters in our population, finding a prevalence of 43.8% insertion over the ICA and 17.5% insertion over ON in the evaluated patients. Sphenoid Sinus: Pneumatization and Septation Patterns ORL DOI: 10.1159/000514458 7 Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM In some studies, no particular data were reported and spaces were left in blank. CT, computed tomography; AS, accessory septa; ACP, anterior clinoid process pneumatization; DS, dorsum sellae pneumatization; PP, pterygoid process pneumatization; GWS, greater wing of the sphenoid pneumatization; OC, Onodi cell. ACP Pneumatization We observed the pneumatization of at least 1 ACP in 27.5% of the population. Bilateral pneumatization was observed in 12.5% of the patients. This prevalence falls among the range reported in the literature in other ethnic populations of 6–47.2% (Table 5) [12, 13, 16, 21, 24–28]. Two studies have shown an association between pneumatization of ACP with protrusion of the ON into the aired space [12, 25] and 1 of them with dehiscence of the bony canal of the ON [12]. Pneumatization of the ACP creates an optic-carotid recess, a small space in the superolateral portion of the SS limited superiorly by the ON and by the ICA inferiorly. Bulging and dehiscence of the ON into the aired space of the SS predispose it to iatrogenic injury and subsequent vision loss [3]. DS Pneumatization Pneumatization of the DS is related to postsellar SS types. Only a few studies have evaluated the pneumatization of this structure and discussed its clinical implications. Reported rates of pneumatization are between 10 and 32.9% [4, 7, 29] compared to 25% in our evaluated population (Table 5). This comparison highlights the importance of precise descriptions of the several anatomical variants among different ethnicities to obtain more data about their origin, distribution, and possible associations. 8 ORL DOI: 10.1159/000514458 PP and GWS Pneumatization PP pneumatization has been defined as pneumatization extending inferior to a horizontal plane crossing the vidian canals [27] or pneumatization lateral to a tangential plane crossing the foramen rotundum and the vidian canal [25]. The former definition was used in the present study to present comparable results as it has been used by most authors. The reported prevalence of patients with pneumatized PP varies among Egyptian, Italian, Libyan, and Turkish populations from 9.3 to 38.9% (Table 5) [7, 12, 16, 27]. We observed pneumatization of the PP in 26.7% of the population. A total of 8.1% of the reviewed CT scans had bilateral pneumatization. This pattern of pneumatization provides access to the central skull base for the repair of cerebrospinal fluid leaks as well as for biopsies of skull base lesions [27]. Pneumatization of the GWS of the sphenoid is defined as pneumatization extending laterally to a vertical plane crossing the foramen rotundum [3]. The lateral recess has been classically defined as pneumatization of the GWS. Under this definition, prevalence among different ethnic groups varies from 20 to 47% (Table 5) [12, 14, 27, 30]. In another study, by Tomovic et al. [15], the lateral recess was defined as pneumatization not only of the GWS but also of the ipsilateral PP. He observed a lateral recess in 72.4% of the population and found a significantly higher prevalence in African Americans (84.6%) than Hispanics (58.2%). We observed pneumatization of the GWS in 57.5% of the population. A total of 34.4% of the patients had bilateral pneumatization. A full lateral recess, with pneumatization of the GWS and ipsilateral PP, was observed in 17.2% of the reviewed sinuses and 8.1% of the patients had a full bilateral recess. Although this pattern of pneumatization provides wide access to the middle cranial fossa for transsphenoidal endoscopic surgery, it is associated with protrusion of the maxillary nerve [31]. Moreover, this recess might communicate with the Stenberg canal and cause a spontaneous cerebrospinal fluid leakage or meningoencephalocele [12]. Onodi Cells We decided to analyze the prevalence of OC because of its relevance for SS surgery. The sphenoethmoidal cells are posterior ethmoidal air cells that extend superolateral into the SS. They are closely related to the ON and ICA. Possible injuries can occur during ethmoidectomy when intending to enter de SS by passing through the OC. Bony walls separating these neurovascular structures from the OC are as thin as 0.03 mm [3]. Treviño-Gonzalez et al. Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM Gibelli et al. [1] observed that a higher SS volume was significantly related to the presence of accessory septa and the insertion of septa over the ICA. While we did not measure volume, we sought to determine this association by using SS type. There was no significant association between the category of accessory septa and each SS type. As Gibelli et al. [1], we found a significant association between a higher volume and insertion of septa on the ICA bony canal. These data, taken together, suggest that a septum inserted over the ICA might be expected in large sinuses, and insertion over ON could be present in any SS volume size. Accessory septa might not be the only issue, but the skewing of the main intersphenoidal septa might also produce asymmetric SS. We observed that 69.4% of our reviewed patients showed SS dominancy toward the left or right side. For these reasons, the main intersphenoidal septum might not be a reliable guide toward approaching the midline in the sinus. An appropriate preoperative assessment of SS septa and insertions is highly recommended to avoid removing unnecessary septa that might result in significant morbidity. We observed OC invading the SS in 53.8% of the population. A total of 26% patients had bilateral sphenoethmoidal cells. These rates are higher than 14, 18, and 23% reported in Malaysian, Egyptian, and Turkish populations, respectively (Table 5) [12, 13, 24]. Tawfik et al. [12] found a significant association between the presence of OC and ON protrusion and dehiscence. Based on these observations, it seems appropriate to evaluate preoperatively for OC before operating the SS in Mexicans. Based on our results, detailed analysis of CT scans prior to SS surgery is of paramount importance to plan the most optimal surgical approach. This study describes the anatomical variants of pneumatization and septation in a Mexican population and complements the literature that exists in other ethnic groups. Our study has limitations that should be mentioned. First, the sample is relatively small and was performed in a single center. Second, our study did not include any child. Finally, our data are insufficient to find relationship between anatomical variants of the SS and different SS- and skull base-related pathologies. Further studies in our country with larger samples describing the pneumatization patterns associated with bulging and dehiscence of neurovascular structures in the SS are needed to confirm our observations. Studies addressing anatomical variants in the presence of disease would also provide valuable data for the evaluation and approach to patients with SS-related pathology. Statement of Ethics Ethical approval was waived by the local Ethics Committee of University Hospital “Dr. José Eleuterio González” with the key OT16-00004 in view of the retrospective nature of the study, and all the procedures performed were part of the routine care. Conflict of Interest Statement The authors have no conflicts of interest to declare. Funding Sources The authors did not receive support from any organization for the submitted work. Author Contributions All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Joel Adrián Becerra-Jiménez, Germán Armando Soto-Galindo, and José Luis Treviño-González. The first draft of the manuscript was written by Félix Maldonado-Chapa and Josefina Alejandra Morales-del Ángel, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. 1 Gibelli D, Cellina M, Gibelli S, Cappella A, Oliva AG, Termine G, et al. Relationship between sphenoid sinus volume and accessory septations: a 3D assessment of risky anatomical variants for endoscopic surgery. Anat Rec. 2020;303(5):1300–4. 2 Jaworek-Troć J, Zarzecki M, Mróz I, Troć P, Chrzan R, Zawiliński J, et al. The total number of septa and antra in the sphenoid sinuses – evaluation before the FESS. Folia Med Crac. 2018;58(3):67–81. 3 Cellina M, Gibelli D, Floridi C, Toluian T, Valenti Pittino C, Martinenghi C, et al. Sphenoid sinuses: pneumatisation and anatomical variants-what the radiologist needs to know and report to avoid intraoperative complications. Surg Radiol Anat. 2020;42(9):1013–24. 4 Lu Y, Pan J, Qi S, Shi J, Zhang X, Wu K. Pneumatization of the sphenoid sinus in Chinese: the differences from Caucasian and its application in the extended transsphenoidal approach. J Anat. 2011;219(2):132–42. 5 Cho JH, Kim JK, Lee JG, Yoon JH. Sphenoid sinus pneumatization and its relation to bulging of surrounding neurovascular structures. Ann Otol Rhinol Laryngol. 2010;119(9):646–50. Sphenoid Sinus: Pneumatization and Septation Patterns 6 Anusha B, Baharudin A, Philip R, Harvinder S, Shaffie BM. Anatomical variations of the sphenoid sinus and its adjacent structures: a review of existing literature. Surg Radiol Anat. 2014;36(5):419–27. 7 Gibelli D, Cellina M, Gibelli S, Oliva AG, Termine G, Sforza C. Anatomical variants of sphenoid sinuses pneumatisation: a CT scan study on a Northern Italian population. Radiol Med. 2017;122(8):575–80. 8 Marino MJ, Weinstein JE, Riley CA, Levy JM, Emerson NA, McCoul ED. Assessment of pneumatization of the paranasal sinuses: a comprehensive and validated metric. Int Forum Allergy Rhinol. 2016;6(4):429–36. 9 Marino MJ, Riley CA, Kessler RH, McCoul ED. Clinician Assessment of paranasal sinus pneumatization is correlated with total sinus volume. Int Forum Allergy Rhinol. 2016; 6(10):1088–93. 10 Marino MJ, Riley CA, Wu EL, Weinstein JE, Emerson N, McCoul ED. Variability of paranasal sinus pneumatization in the absence of sinus disease. Ochsner J. 2020;20(2):170–5. ORL DOI: 10.1159/000514458 11 Hiremath SB, Gautam AA, Sheeja K, Benjamin G. Assessment of variations in sphenoid sinus pneumatization in Indian population: a multidetector computed tomography study. Indian J Radiol Imaging. 2018 Jul–Sep;28(3):273–9. 12 Tawfik A, El-Fattah AMA, Nour AI, Tawfik AM. Neurovascular surgical keys related to sphenoid window: radiologic study of egyptian's sphenoid. World Neurosurg. 2018; 116: e840–9. 13 Anusha B, Baharudin A, Philip R, Harvinder S, Shaffie BM, Ramiza RR. Anatomical variants of surgically important landmarks in the sphenoid sinus: a radiologic study in Southeast Asian patients. Surg Radiol Anat. 2015; 37(10):1183–90. 14 Dal Secchi MM, Dolci RLL, Teixeira R, Lazarini PR. An analysis of anatomic variations of the sphenoid sinus and its relationship to the internal carotid artery. Int Arch Otorhinolaryngol. 2018;22(2):161–6. 15 Tomovic S, Esmaeili A, Chan NJ, Shukla PA, Choudhry OJ, Liu JK, et al. High-resolution computed tomography analysis of variations of the sphenoid sinus. J Neurol Surg B Skull Base. 2013;74(2):82–90. 9 Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM References 10 ORL DOI: 10.1159/000514458 21 Unal B, Bademci G, Bilgili YK, Batay F, Avci E. Risky anatomic variations of sphenoid sinus for surgery. Surg Radiol Anat. 2006;28(2): 195–201. 22 Basak S, Karaman CZ, Akdilli A, Mutlu C, Odabasi O, Erpek G. Evaluation of some important anatomical variations and dangerous areas of the paranasal sinuses by CT for safer endonasal surgery. Rhinol. 1998;36:162–7. 23 Elwany S, Elsaeid I, Thabet H. Endoscopic anatomy of the sphenoid sinus. J Laryngol Otol. 1999;113(2):122–6. 24 Asal N, Bayar Muluk N, Inal M, Şahan MH, Doğan A, Arıkan OK. Carotid canal and optic canal at sphenoid sinus. Neurosurg Rev. 2019; 42(2):519–29. 25 Sirikci A, Bayazit YA, Bayram M, Mumbuç S, Güngör K, Kanlikama M. Variations of sphenoid and related structures. Eur Radiol. 2000; 10(5):844–8. 26 Arslan H, Aydinlioğlu A, Bozkurt M, Egeli E. Anatomic variations of the paranasal sinuses: CT examination for endoscopic sinus surgery. Auris Nasus Larynx. 1999;26(1):39–48. 27 Hewaidi G, Omami G. Anatomic variation of sphenoid sinus and related structures in libyan population: CT scan study. Libyan J Med. 2008;3(3):128–33. 28 Kazkayasi M, Karadeniz Y, Arikan OK. Anatomic variations of the sphenoid sinus on computed tomography. Rhinology. 2005; 43(2):109–14. 29 Ilków W, Waligóra M, Kunc M, Kucharzew­ ski M. Pneumatization of the sphenoid sinus, dorsum sellae and posterior clinoid processes in computed tomography. Pol J Radiol. 2018; 83:366–71. 30 Refaat R, Basha MAA. The impact of sphenoid sinus pneumatization type on the protrusion and dehiscence of the adjacent neurovascular structures: A prospective MDCT imaging study. Acad Radiol. 2020;27(6):e132–9. 31 Štoković N, Trkulja V, Dumić-Čule I, Ču­ ković-Bagić I, Lauc T, Vukičević S, et al. Sphenoid sinus types, dimensions and relationship with surrounding structures. Ann Anat. 2016; 203:69–76. Treviño-Gonzalez et al. Downloaded by: J. Treviño-Gonzalez - 611371 189.140.37.206 - 4/1/2021 6:32:38 PM 16 Rahmati A, Ghafari R, AnjomShoa M. Normal variations of sphenoid sinus and the adjacent structures detected in cone beam computed tomography. J Dent. 2016;17(1):32–7. 17 Banna M, Olutola PS. Patterns of pneumatization and septation of the sphenoidal sinus. J Can Assoc Radiol. 1983;34(4):291–3. 18 Madiha AES, Raouf AA. Endoscopic anatomy of the sphenoidal air sinus. Bull Alex Fac Med. 2007;43:1021–6. 19 Abdullah BJ, Arasaratnam A, Kumar G, Gopala K. The sphenoid sinuses: computed tomographic assessment of septation, relationship to the internal carotid arteries and sidewall thickness in the Malaysian population. J HK Coll Radiol. 2001;4:185–8. 20 Fernandez-Miranda JC, Prevedello DM, Madhok R, Morera V, Barges-Coll J, Reineman K, et al. Sphenoid septations and their relationship with internal carotid arteries: anatomical and radiological study. Laryngoscope. 2009;119(10):1893–6.