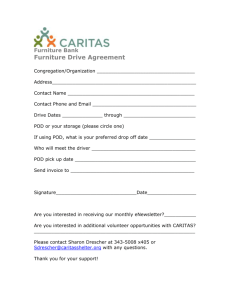
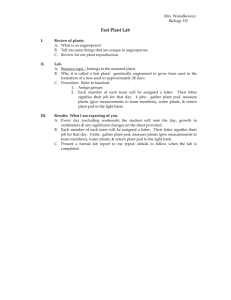
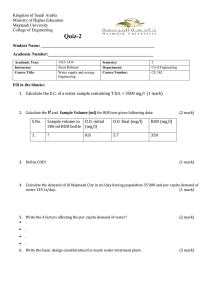
Measurement in Physical Education and Exercise Science ISSN: 1091-367X (Print) 1532-7841 (Online) Journal homepage: https://www.tandfonline.com/loi/hmpe20 A comparison of the agreement, internal consistency, and 2-day test stability of the InBody ® 720, GE iDXA, and BOD POD gold standard for assessing body composition Bruce W Bailey, Gabrielle LeCheminant, Timothy Hope, Mathew Bell & Larry A Tucker To cite this article: Bruce W Bailey, Gabrielle LeCheminant, Timothy Hope, Mathew Bell & Larry A Tucker (2018) A comparison of the agreement, internal consistency, and 2-day ® test stability of the InBody 720, GE iDXA, and BOD POD gold standard for assessing body composition, Measurement in Physical Education and Exercise Science, 22:3, 231-238, DOI: 10.1080/1091367X.2017.1422129 To link to this article: https://doi.org/10.1080/1091367X.2017.1422129 Published online: 05 Jan 2018. Submit your article to this journal Article views: 481 View related articles View Crossmark data Citing articles: 3 View citing articles Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=hmpe20 MEASUREMENT IN PHYSICAL EDUCATION AND EXERCISE SCIENCE 2018, VOL. 22, NO. 3, 231–238 https://doi.org/10.1080/1091367X.2017.1422129 A comparison of the agreement, internal consistency, and 2-day test stability of the InBody 720, GE iDXA, and BOD POD® gold standard for assessing body composition Bruce W Bailey, Gabrielle LeCheminant, Timothy Hope, Mathew Bell, and Larry A Tucker Department of Exercise Sciences, Brigham Young University, Provo, UT ABSTRACT ARTICLE HISTORY The study compared the agreement, internal consistency, and measurement stability of the GE iDXA, BOD POD, and InBody 720. Body composition of 43 men and 37 women (31.4 ± 10.7 years; 90% Caucasian and 10% other) was assessed in triplicate using each method over two different days. Mean percent body fat (% BF) of the participants was different for all three machines (27.6 ± 10.0% [GE iDXA)] 25.6 ± 10.4% [BOD POD], and 21.3 ± 10.6% [InBody 720]; p < .05). The coefficient of variation for same day repeated measures was 1.06% (GE iDXA), 3.29% (BOD POD), and 2.97% (InBody 720). The coefficient of variation for 2-day repeated measures was 1.81% (GE iDXA), 4.61% (BOD POD), and 4.24% (InBody 720). The difference between the GE iDXA and BOD POD was within acceptable variability, while the InBody 720 significantly underestimated % BF. The internal consistency was highest for the GE iDXA, followed by the InBody 720, and then the BOD POD. Received 20 June 2017 Revised 22 December 2017 Accepted 23 December 2017 Research Highlights ● ● ● ● ● The InBody 720 significantly underestimated percent body fat (% BF) compared to the GE iDXA and BOD POD. Device differences were similar for men and women. Agreement between machines was better at higher BMIs. Order of internal consistency strength was GE iDXA (strongest), InBody, and BOD POD. Two-day test stability was best for the GE iDXA and similar for InBody and BOD POD. Introduction Assessing body composition accurately is important for determining the health status of an individual. Measuring body composition rather than body mass index (BMI) is more salient for determining disease risk. This is specifically true for those in the intermediate range for BMI (Bigaard et al., 2004; Dervaux, Wubuli, Megnien, Chironi, & Simon, 2008; Flegal et al., 2009; Frankenfield, Rowe, Cooney, Smith, & Becker, 2001; Gomez-Ambrosi et al., 2012; Muller et al., 2012; Okorodudu et al., 2010). KEYWORDS Percent body fat; agreement; reliability; dual energy X-ray absorptiometry; air displacement plethysmography; bioimpedance; adiposity However, cost, accessibility, as well as concerns regarding reliability, have prohibited body composition from being used more frequently. In addition, there are concerns about the lack of agreement between different methods of measuring body composition and between different manufacturers using the same method. There are currently a variety of methods of indirectly measuring body composition. Three common methods include dual energy X-ray absorptiometry (DXA), air displacement plethysmography, and bioelectrical impedance. DXA allows for the assessment of body composition into three compartments, accounting for variation in bone mineral content, lean body mass, and fat mass (Laskey, 1996). The DXA has been validated against a four-compartment model and is used frequently as a point of reference or Gold Standard (Ballard, Fafara, & Vukovich, 2004; Sardinha, Lohman, Teixeira, Guedes, & Going, 1998; Sopher, Horlick, Wang, Pierson, & Heymsfield, 2002). In contrast to the DXA, the BOD POD uses air displacement plethysmography to determine body composition. The BOD POD was first used over 20 years ago and is often compared to hydrostatic weighing in its validity and reliability (McCrory, Gomez, Bernauer, & Mole, 1995; Wagner, Heyward, & Gibson, 2000). Although the reliability of the BOD POD has been evaluated in several studies, the results CONTACT Bruce W Bailey bruce.bailey@byu.edu Department of Exercise Sciences, Brigham Young University, Provo, UT 267 SFH. All authors are from Department of Exercise Sciences at Brigham Young University, 106 SFH, Brigham Young University, Provo, UT, 84602-2216 Color versions of one or more of the figures in the article can be found online at www.tandfonline.com/hmpe. © 2018 Taylor & Francis 232 B. W. BAILEY ET AL. vary widely (coefficients of variations between 1.7% and 4.5% for same-day test–retest), making a direct comparison of this method of measuring body composition to other methods difficult (Biaggi et al., 1999; Iwaoka et al., 1998; McCrory et al., 1995; Miyatake, Nonaka, & Fujii, 1999; Noreen & Lemon, 2006; Sardinha et al., 1998; Tucker, Lecheminant, & Bailey, 2014; Vescovi et al., 2001). Bioelectrical impedance estimates body composition by measuring the voltage drop initiated from a current as it passes between electrodes. Historically, results from bioelectrical impedance have been viewed as less consistent than other measures of body composition, but recently there have been some changes to bioelectrical impedance that are thought to have improved the outcomes. First, segmental assessment allows the estimation of lean and fat mass for arms, legs, and trunk separately, recognizing that each segment has a different resistance. Additionally, multifrequency bioelectrical impedance uses a large range of electrical frequencies that allows for better assessment of extracellular water (Anderson, Erceg, & Schroeder, 2012; Benton, Swan, Schlairet, & Sanderson, 2011; Mally & Dittmar, 2012). One machine that takes advantage of these improvements in bioelectrical impedance is the InBody 720. There have been a couple of studies that have compared the measurements of DXA, air-displacement plethymsmography, and bioelectrical impedance (Biaggi et al., 1999; Lazzer et al., 2008). However, these studies have exclusively looked at agreement of the measurements and have not directly compared the internal consistency (same-day test– retest) or test stability of these measurements between days. In addition, previous studies have evaluated older models, different manufacturers, or single-frequency bioelectrical impedance. These studies have also failed to examine how body size influences agreement, internal consistency, and test stability. The purpose of this study was to directly compare the agreement, internal consistency, and test stability of the GE iDXA, and BOD POD and InBody 720 for measuring percent body fat (% BF). Materials and methods To accomplish the purpose of the study, a repeated measures design was used with randomized test order on three different methods of measuring body composition. Eighty men and women were recruited to participate in the study. Each participant had body composition measured on two separate days over a 3-day period. On the first visit to the lab, height and weight were determined as well as body composition from each of three different methods (GE iDXA, BOD POD, and InBody 720). Each of these methods of assessing body composition was performed twice on each individual during the first assessment day. The second assessment day was 2 days later and, again, weight and body composition, using each of the three methods, were assessed; however, during this appointment, assessments were performed only once for each method. Procedures Once participants were screened and eligibility determined, they were scheduled for two appointments. During the first visit, two DXA scans, two BOD POD tests, and two segmental multifrequency bioelectircal impedances were performed. Participants arrived at the lab having fasted for a minimum of 3 h, not exercised for 12 h, not consumed caffeine for 6 h, and not consumed alcohol for 12 h. While participants were asked to abstain from caffeinated drinks and alcohol, they were also asked to maintain normal hydration per manufacturer’s recommendation. Beyond asking participants to maintain normal hydration, there was no effort to standardize hydration status between days. The participants’ heights were then measured. After this assessment, the participants were measured using each of the three body composition methods. After all three tests were completed, the measurements were performed again. The second visit involved only one measurement on each of the three machines. These measurements were taken at the same time of the day as the first assessments. All other procedures and instructions were identical to the first visit. Participants Participants included 43 men and 37 women between the ages of 18 and 55 years. Participants were excluded if pregnant or lactating. There was no restriction on the fitness level of the participants. Recruitment was performed by word of mouth, fliers, and posters. The study was approved by the university Institutional Review Board and written informed consent was given prior to testing. Measurements Anthropometrics Body weight was measured using a digital scale (Tanita Corp., Inc., Japan) accurate to ±.1 kg with participants barefoot and wearing a standardized one-piece swimsuit or lycra shorts. Height was obtained using a digital stadiometer accurate to ±.1 cm (SECA, Chino, CA). Body weight and height were used to calculate BMI. MEASUREMENT IN PHYSICAL EDUCATION AND EXERCISE SCIENCE Body composition All body composition assessments were performed per manufacturer’s instructions. Assessments were done in random order. The machines were calibrated prior to any assessment per manufacturer’s recommendations. Tests were conducted in a temperature controlled room (22–24°C). Dual energy X-ray absorptiometry. The participants’ body composition was measured using the GE iDXA (GE, Fairfield, CT). The GE iDXA measured adipose tissue, bone tissue, and nonbone lean mass. % BF was calculated by dividing the adipose tissue by the total body mass that included bone tissue, nonbone lean tissue, and adipose tissue. The machine was calibrated daily using a manufacturer-provided calibration block. Scans were analyzed using Encore software version 13.20.033. 233 the strength of the relationship between machines. Absolute mean differences were calculated for the sameday test–retest and the 2-day test–retest on each machine. This was done to better preserve the magnitude of the difference between test–retests, which can be lost when using only the mean of the difference. Internal consistency and test stability of the machines were analyzed using both the intraclass correlation coefficient and the coefficient of variation. The coefficient of variation (%) was calculated for each machine using the following equation: CV = ±√((∑x1 − x2)2/2n)/((∑x1 + x2)/2n) × 100. Analysis of variance was used to evaluate how the coefficient of variation for % BF differed between machines for both same-day test–retest and between-day test–retest. Significance was set at p < .05. All analyses were done using SAS version 9.4. Results BOD POD. The participants’ % BF was assessed using the BOD POD. Participants wore a lycra cap over their hair. We used the BOD POD software version 5.2.0 and body fatness was calculated using the general equation of Siri. To eliminate error from the measurement of thoracic volume, we used predicted values and the same value was used for each assessment (McCrory, Mole, Gomez, Dewey, & Bernauer, 1998; Otterstetter et al., 2015). Segmental multifrequency bioelectrical impedance. The InBody 720 (segmental multifrequency bioelectrical impedance) was used to predict % BF. The InBody 720 calculates 30 impedance measurements by using 6 different frequencies (1, 5, 50, 250, 500, and 1,000 kHz) at each of 5 different segments, which include the right arm, left arm, trunk, right leg, and left leg. Statistical analysis The primary dependent variable of interest for this study was % BF as measured by each machine. Means and standard deviations were calculated for all variables of interest (age, height, weight, BMI, and % BF for each machine). Mean difference in % BF between machines was analyzed using a mixed effects model. The impact of measurement order and gender were evaluated using partial correlation. Participants were stratified into BMI categories of less than 20, 20 to 24.9, 25 to 29.9, and 30 or greater. A mixed model was used to evaluate the interactive effects of machine and BMI category on % BF. The least squares means technique with a Tukey adjustment was used to analyze differences between machines by BMI category. Pearson correlations were calculated to evaluate Eighty participants (37 women, 43 men) completed all aspects of the study. Demographic information for the participants is presented in Table 1. The sample was 90% Caucasian and 10% African American, Asian, and Hispanic. The mean age was 30.8 ± 10.5 years, and the range was 18 to 55 years. The mean BMI was 25.8 ± 5.7, with a range from 16.1 to 46.5. Of the participants, 14% had a BMI of less than 20, 37% had a BMI between 20 and 24.9, 33% had a BMI between 25 and 29.9, and 16% had a BMI greater than 30. Agreement Figure 1 displays the Bland–Altman plots comparing the three methods of assessing body composition. The Pearson correlation was strongest between GE iDXA and BOD POD (r = .98, p < .001), followed by the correlation between the InBody 720 and GE iDXA (r = .95, p < .001) and the correlation between the Table 1. Demographic information for both men and women who participated in the study. Men (N = 43) Mean Age (yrs) 31.4 Height (cm)* 179.6 Weight (kg)* 86.7 BMI* 26.9 Body Fat GE iDXA (%)* 22.9a Body Fat BOD POD (%)* 21.2b Body Fat InBody 720 (%)* 16.8c Women (N = 37) Total (N = 80) SD Mean SD Mean ±10.7 30.0 ±10.2 30.8 ±7.5 167.5 ±8.0 174.0 ±17.7 68.9 ±18.3 78.5 ±5.3 24.4 ±5.9 25.8 ±8.8 32.9a ±8.7 27.5a b ±9.0 30.9 ±9.4 25.7b ±8.4 26.5c ±10.6 21.3c SD ±10.5 ±9.8 ±20.0 ±5.7 ±10.0 ±10.4 ±10.6 BMI: Body mass index. *Means in the same row are significantly different between men and women (p < .05). a,b,c Means in the same column with different superscript letters are significantly different (p < .05). 234 B. W. BAILEY ET AL. b Bland-Altman Plot for Percent Body fat: InBody 720 vs. GE iDXA 25 20 20 15 15 Diff: InBody 720 minus GE iDXA Diff: GE iDXA minus BodPod a Bland-Altman Plot for Percent Body fat: BOD POD vs. GE iDXA 25 10 5 0 -5 0 10 20 30 40 50 60 -10 -15 10 5 0 -5 0 10 20 30 40 50 60 -10 -15 -20 -20 -25 -25 c Bland-Altman Plot for Percent Body fat: BOD POD® vs. InBody 720 25 Diff: InBody 720 minus BodPod 20 15 10 5 0 -5 0 10 20 30 40 50 60 -10 -15 -20 -25 Figure 1. (a) Bland–Altman plot for percent body fat: BOD POD vs. GE iDXA. (b) Bland–Altman plot for percent body fat: InBody 720 vs. GE iDXA. (c) Bland–Altman plot for percent body fat: BOD POD® vs. InBody 720. Note: The x-axis for all three plots represents the mean percent body fat for the two measures of body composition being expressed in the plot. The line of best fit was added to visually express how the agreement between the two measures of body fat change as percent body fat increases or decreases. InBody 720 and BOD POD (r = .93, p < .001). However, both the BOD POD and InBody 720 produced significantly lower body fat results than the GE iDXA (see Table 1). The mean difference between GE iDXA and BOD POD was 1.80 ± 2.23 percentage points, between the GE iDXA and the InBody 720 was 6.24 ± 3.37 percentage points, and between the BOD POD and the InBody 720 was 4.42 ± 4.06 percentage points. The intraclass correlation between GE iDXA and BOD POD was .975 (p < .001), between GE iDXA and InBody 720 .877 (p < .001), and between BOD POD and InBody 720 was .914 (p < .001). The differences between the three different measures of body fat were similar for men and women. In addition, the differences between the measures of body fat did not change based on the order of the assessments. The differences between machines were greater for those with lower BMIs and became progressively smaller as BMIs increased (F = 5.05, p = .004; see Figure 2). Internal consistency The absolute mean difference for same-day test–retest was .29 ± .30 percentage points for GE iDXA, .92 ± .76 for the BOD POD, and .83 ± 1.87 for the InBody 720. For same-day test–retest, 88% of tests were within .5 percentage points for GE iDXA, 33% for BOD POD, and 69% for the InBody 720. Similarly, 98% of test–retests were within 1 percentage point for GE iDXA, 59% for BOD POD, and 87% for InBody 720. There were no paired tests that differed by more than two percentage points for GE iDXA; however, 8% and 13% of same-day tests–retests differed by greater than 2 percentage points for BOD POD and the InBody 720, respectively. For the InBody 720, there were four tests that differed by more than 5 percentage points. The coefficient of variation for repeated measures was 1.06%, 3.29%, and 6.70% for the GE iDXA, BOD POD, and InBody 720, respectively. When outliers were removed (measurements > 5 percentage points apart, N = 4), the coefficient of variation for the InBody was reduced to 2.97%. With outliers removed (N = 4), the coefficient of variation for BOD POD was significantly higher than both the GE iDXA (p < .001) and InBody 720 (p = .018). The same-day test–retest intraclass correlation for GE iDXA, BOD POD, and InBody 720 was .999 (p < .001), .990 (p < .001), and .996 (p < .001), respectively. The same-day test–retest differences between measured % BF for GE iDXA and BOD POD were not different between genders. There was a difference between genders for the InBody 720 (p = .015); however, once outliers (N = 4) were removed, the difference was nonsignificant. When comparing how internal consistency differs by BMI, the same-day test–retest was not different for any of the MEASUREMENT IN PHYSICAL EDUCATION AND EXERCISE SCIENCE 12 235 * Difference in Percent Body Fat * 10 * * 8 * * * 6 * 4 * 2 0 GE iDXA vs. BOD POD GE iDXA vs. InBody 720 Underweight n = 9 Normal n = 32 BOD POD vs. InBody 720 Overweight n = 27 Obese n = 12 Figure 2. Differences in percent body fat between GE iDXA, BOD POD, and InBody 720 by BMI Category. *Difference between machines is significantly different than zero (p < .05).Error bars represent the standard deviation. machines; however, there was a significant relationship for BOD POD (r value = − .23, p = .049) with better agreement for individuals with higher BMIs compared to lower BMIs. Two-day test stability The absolute mean difference for test–retest separated by 2 days was .51 ± .49 percentage points for GE iDXA, 1.22 ± 1.14 for the BOD POD, and .96 ± 2.54 for the InBody 720. For the 2-day test–retest, 66% of tests were within .5 percentage points for GE iDXA, 30% for BOD POD, and 41% for the InBody 720. In addition, 91% of tests were within 1 percentage point for the GE iDXA, 61% for the BOD POD, and 70% for the InBody 720. Only 3% of the 2-day test–retests differed by more than 2% for GE iDXA, while 14% differed by more than 2 percentage points for the BOD POD and 11% for the InBody 720. The coefficient of variation for 2-day repeated measures was 1.81%, 4.61%, and 6.73% for the GE iDXA, BOD POD, and InBody 720, respectively. When outliers were removed (measurements > 5 percentage points apart, N = 3), the coefficient of variation for the BOD POD was reduced to 4.24, and the coefficient of variation for the InBody 720 was reduced to 4.36%. Once outliers (N = 3) were removed, the coefficient of variation for the GE iDXA was significantly lower than either the InBody 720 (p < .001) or the BOD POD (p < .001); however, there was no difference between the InBody 720 and the BOD POD. The 2-day test–retest intraclass correlation for the GE iDXA, BOD POD, and InBody 720 was .997 (p < .001), .987 (p < .001), and .992 (p < .001), respectively. Discussion The accurate measurement of adiposity is important to help individuals understand weight-related disease risk. All three measures that were tested in this study were significantly different with the greatest disagreement between the GE iDXA and InBody 720 (6.2 ± 3.4%). However, agreement was better at higher BMIs, although the mean difference between machines remained significant. While the accurate assessment of body fat is important at all BMIs, the better agreement at high BMIs between the three different methods is encouraging since these are the individuals that would benefit from body fat testing to confirm that they have excess body fat and are at risk of weight related diseases. Since the three machines use different methods to estimate % BF, they are subject to different assumptions and limitations that could explain some of the discrepancies between machines. For example, based on the attenuation properties of X-rays, water will appear to have about 8% fat content (Kohrt, 1995). In contrast, because of the conducting properties of water, increased water volume in the body would favor a lower fat content using bioelectircal impedance. However, the large difference between the InBody 720 and GE iDXA suggests that the reason for the difference goes beyond participant differences and the assumptions made by each measurement method. This was shown in another study that also reported the InBody 720 underestimating % BF (JenskySquires et al., 2008). Given the relatively high correlation coefficients between the measurements of body composition, it seems that agreement could be improved. Previous research demonstrates that agreement between machines may be manufacturer and model dependent. In previous studies, the BOD POD has shown good agreement to DXA, but those studies have generally used Hologic machines. To date, we are not aware of studies that have compared the BOD POD to GE machines and specifically to the GE iDXA. Internal consistency is a reliability measure evaluating the error inherent within the instrument and is performed by taking multiple measurements back-to-back on the same day. This same-day test–retest measure was good 236 B. W. BAILEY ET AL. for all three measures of body composition. While the internal consistency was reasonable for all three measures of body composition, the GE iDXA was far superior to either the BOD POD or the InBody 720 (coefficient of variations of 1.06%, 3.29%, and 2.97%, respectively). However, the internal consistency of the InBody 720 was very good and slightly better than the BOD POD. One concern about the InBody 720 is that a small percentage (4 scans out of the 240 performed) of the scans was drastically off (>5 percentage points). The occurrence of this measurement error seems to be random and can be easily caught by performing two measurements back-toback to ensure consistency of results and to catch the occasional erroneous measurement. Since this measurement takes less than 2 min to perform, it would be easy to perform repeated measures on this device. For the BOD POD, over 40% of the same-day test– retests differed by more than 1 percentage point compared to 2% and 13% for the GE iDXA and InBody 720, respectively. Unlike the InBody 720, the same-day test–retest for the BOD POD did not result in any tests that were extremely different (>5 percentage points). However, other studies that have looked at the internal consistency of the BOD POD have reported tests that differed by as much as 12.3% (Noreen & Lemon, 2006; Wells & Fuller, 2001). Our findings are similar to those of Tucker et al. who did test–retest on over 200 women (Tucker et al., 2014). The results from this study demonstrated that one in three measurements were greater than 1 percentage point apart. This study also showed that some of the limitations in the internal consistency of the BOD POD can be overcome by performing measurements in duplicate and then performing a third measurement if the first two are greater than 1 percentage point apart. The mean of the two measurements that are in agreement is then used. The measure of test stability evaluates the error inherent in the machine and the relative ability of the machine to reproduce results over time and withstand changes that occur in the environment and within the individual. All three measures of % BF were relatively stable. However, the InBody 720 lost some of the advantage it had in terms of reliability over the BOD POD, and while the absolute mean difference was still lower than the BOD POD, the coefficient of variation for repeated measures was no longer statistically different from the BOD POD. There are very few studies that have evaluated the reliability of DXA for assessing % BF and none, to our knowledge, that have been performed using the GE iDXA. Coefficients of variation ranging from .6 and 1.6% have been reported for bone mineral content, bone mineral density, and lean tissue mass (Cordero-MacIntyre et al., 2002, 2000; Heymsfield, Lohman, Wang, & Going, 2005). The coefficient of variation observed in our study for % BF is within this range of coefficients, but it is hard to say if this is better or worse than what has been observed previously, since none of these previous observations have evaluated % BF. One study looked at the stability of the measurement over several days and found a coefficient of variation of 1.89% for body fat, which was similar to our study (Kiebzak, Leamy, Pierson, Nord, & Zhang, 2000). Several studies have evaluated the reliability of the BOD POD for measuring adiposity. The results from these studies are similar to the results from our study. Coefficients of variation between 1.7 and 4.5 for same-day test–retest have been observed. The results of our study are in the middle of this range (Biaggi et al., 1999; Iwaoka et al., 1998; McCrory et al., 1995; Miyatake et al., 1999; Noreen & Lemon, 2006; Sardinha et al., 1998; Tucker et al., 2014; Vescovi et al., 2001). The between-day coefficient of variation for the BOD POD has been shown to be between 2.0% and 2.3%, which is lower than what we observed (Levenhagen et al., 1999; Miyatake et al., 1999; Nunez et al., 1999). However, it is unclear if the coefficient of variation for these studies was calculated in the same way. For studies that clearly reported how they calculated the coefficient of variation, our results compared well. Vescovi et al. found a coefficient of variation of 3.4% and Noreen et al. found a coefficient of variation of 3.1% (Noreen & Lemon, 2006; Vescovi et al., 2001). Our study also supports previous research that has indicated that the BOD POD is more precise at higher BMIs (Collins & McCarthy, 2003; Wells & Fuller, 2001). Few studies have been conducted evaluating the reliability of the InBody 720. Jensky-Squires et al. (2008) evaluated the internal consistency of the InBody 320 and found a coefficient of variation of 1.83, which was lower than what was observed in our study. However, how the coefficient of variation was calculated was not clear in this study. While our study has strengths, there are a few limitations that should be pointed out. First, although participants were asked to maintain normal hydration, there was no effort to standardize hydration between days. This could be a problem since hydration status adds to the error seen by each machine between days of assessment. This is especially true for bioelectrical impedance and the InBody 720, which can be very sensitive to alterations in hydration status. Dehydration increases the body’s electrical resistance and can result in overestimating fat mass and underestimating fat free mass. In addition, since we rotated through the machines, there may have been some shifts in fluid distribution throughout the body. Shifts in fluid distribution in the body could have an impact on bioelectrical impedance (InBody 720) test results MEASUREMENT IN PHYSICAL EDUCATION AND EXERCISE SCIENCE specifically. However, the order of the tests was randomized and there were no order effects observed. Finally, we did not control for menstrual cycle, which also could affect hydration status and may have a small impact on the results for women. Despite these limitations, the study adds significance to the current literature and can help when choosing a body composition assessment for tracking changes in % BF. To our knowledge, the GE iDXA has not been evaluated specifically for reliability, and there is little information, in general on the precision of DXA for measuring % BF. The GE iDXA is very precise; however, widespread use is limited given the high cost of the assessment and it uses radiation to measure body fat (although the radiation is minimal, similar to cross country flight). Reliability of the BOD POD has been evaluated, but the range of coefficient of variations is relatively large (1.7–4.5). This makes it difficult to compare the consistency of the BOD POD measurements to other methods of measuring body fat in different studies. Finally, the InBody 720 is a newer method of assessing body fat and there is limited information on the reliability of this instrument. The ease of the measurement makes it attractive for measuring body fat and, based on this study, it is reliable, comparing favorably to the BOD POD for reliability. Conclusion The GE iDXA, BOD POD, and InBody 720 each demonstrates good reliability for measuring adiposity. While the GE iDXA had a coefficient of variation that was three times smaller than either the BOD POD or InBody 720, it is not practical for all situations. Choosing either the BOD POD or the InBody 720 would result in similar internal consistency and test stability; however, there is a high percentage of tests that are separated by more than 1 percentage point and there is also the possibility of erroneous measurements. Because of this, we recommend that the BOD POD and InBody 720 be repeated until two tests are within 1 percentage point of each other and the mean of the two closest tests be used. Finally, while all the machines produced mean values that differed significantly, the difference between the GE iDXA and BOD POD was within acceptable variability, while the InBody 720 significantly underestimated % BF. Acknowledgments This research did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors. 237 References Anderson, L. J., Erceg, D. N., & Schroeder, E. T. (2012). Utility of multifrequency bioelectrical impedance compared with dual-energy x-ray absorptiometry for assessment of total and regional body composition varies between men and women. Nutrition Research, 32(7), 479–485. Ballard, T. P., Fafara, L., & Vukovich, M. D. (2004). Comparison of Bod Pod and DXA in female collegiate athletes. Medicine and Science in Sports and Exercise, 36 (4), 731–735. Benton, M. J., Swan, P. D., Schlairet, M. C., & Sanderson, S. (2011). Comparison of body composition measurement with whole body multifrequency bioelectrical impedance and air displacement plethysmography in healthy middleaged women. Health Care for Women International, 32 (12), 1068–1078. Biaggi, R. R., Vollman, M. W., Nies, M. A., Brener, C. E., Flakoll, P. J., Levenhagen, D. K., . . . Chen, K. Y. (1999). Comparison of air-displacement plethysmography with hydrostatic weighing and bioelectrical impedance analysis for the assessment of body composition in healthy adults. American Journal of Clinical Nutrition, 69(5), 898–903. Bigaard, J., Frederiksen, K., Tjonneland, A., Thomsen, B. L., Overvad, K., Heitmann, B. L., & Sorensen, T. I. (2004). Body fat and fat-free mass and all-cause mortality. Obesity Research, 12(7), 1042–1049. Collins, A. L., & McCarthy, H. D. (2003). Evaluation of factors determining the precision of body composition measurements by air displacement plethysmography. European Journal of Clinical Nutrition, 57(6), 770–776. Cordero-MacIntyre, Z. R., Peters, W., Libanati, C. R., Espana, R. C., Abila, S. O., Howell, W. H., & Lohman, T. G. (2002). Reproducibility of DXA in obese women. Journal of Clinical Densitometry, 5(1), 35–44. Cordero-MacIntyre, Z. R., Peters, W., Libanati, C. R., Espana, R. C., Howell, W. H., & Lohman, T. G. (2000). Reproducibility of body measurements in very obese postmenopausal women. Annals of the New York Academy of Sciences, 904, 536–538. Dervaux, N., Wubuli, M., Megnien, J. L., Chironi, G., & Simon, A. (2008). Comparative associations of adiposity measures with cardiometabolic risk burden in asymptomatic subjects. Atherosclerosis, 201(2), 413–417. Flegal, K. M., Shepherd, J. A., Looker, A. C., Graubard, B. I., Borrud, L. G., Ogden, C. L., . . . Schenker, N. (2009). Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. American Journal of Clinical Nutrition, 89(2), 500–508. Frankenfield, D. C., Rowe, W. A., Cooney, R. N., Smith, J. S., & Becker, D. (2001). Limits of body mass index to detect obesity and predict body composition. Nutrition, 17(1), 26–30. Gomez-Ambrosi, J., Silva, C., Galofre, J. C., Escalada, J., Santos, S., Millan, D., . . . Fruhbeck, G. (2012). Body mass index classification misses subjects with increased cardiometabolic risk factors related to elevated adiposity. International Journal of Obesity (2005), 36(2), 286–294. Heymsfield, S. B., Lohman, T. G., Wang, Z., & Going, S. B. (2005). Human body composition (2nd ed.). Champaign, IL: Human Kinetics. 238 B. W. BAILEY ET AL. Iwaoka, H., Yokoyama, T., Nakayama, T., Matsumura, Y., Yoshitake, Y., Fuchi, T., . . . Tanaka, H. (1998). Determination of percent body fat by the newly developed sulfur hexafluoride dilution method and air displacement plethysmography. Journal of Nutritional Science and Vitaminology, 44(4), 561–568. Jensky-Squires, N. E., Dieli-Conwright, C. M., Rossuello, A., Erceg, D. N., McCauley, S., & Schroeder, E. T. (2008). Validity and reliability of body composition analysers in children and adults. British Journal of Nutrition, 100(4), 859–865. Kiebzak, G. M., Leamy, L. J., Pierson, L. M., Nord, R. H., & Zhang, Z. Y. (2000). Measurement precision of body composition variables using the lunar DPX-L densitometer. Journal of Clinical Densitometry, 3(1), 35–41. Kohrt, W. M. (1995). Body composition by DXA: Tried and true? Medicine and Science in Sports and Exercise, 27(10), 1349–1353. Laskey, M. A. (1996). Dual-energy X-ray absorptiometry and body composition. Nutrition, 12(1), 45–51. Lazzer, S., Bedogni, G., Agosti, F., De Col, A., Mornati, D., & Sartorio, A. (2008). Comparison of dual-energy X-ray absorptiometry, air displacement plethysmography and bioelectrical impedance analysis for the assessment of body composition in severely obese Caucasian children and adolescents. British Journal of Nutrition, 100(4), 918–924. Levenhagen, D. K., Borel, M. J., Welch, D. C., Piasecki, J. H., Piasecki, D. P., Chen, K. Y., & Flakoll, P. J. (1999). A comparison of air displacement plethysmography with three other techniques to determine body fat in healthy adults. Journal of Parenteral and Enteral Nutrition, 23(5), 293–299. Mally, K., & Dittmar, M. (2012). Comparison of three segmental multifrequency bioelectrical impedance techniques in healthy adults. Annals of Human Biology, 39(6), 468–478. McCrory, M. A., Gomez, T. D., Bernauer, E. M., & Mole, P. A. (1995). Evaluation of a new air displacement plethysmograph for measuring human body composition. Medicine and Science in Sports and Exercise, 27(12), 1686–1691. McCrory, M. A., Mole, P. A., Gomez, T. D., Dewey, K. G., & Bernauer, E. M. (1998). Body composition by air-displacement plethysmography by using predicted and measured thoracic gas volumes. Journal of Applied Physiology, 84(4), 1475–1479. Miyatake, N., Nonaka, K., & Fujii, M. (1999). A new air displacement plethysmograph for the determination of Japanese body composition. Diabetes, Obesity & Metabolism, 1(6), 347–351. Muller, M. J., Lagerpusch, M., Enderle, J., Schautz, B., Heller, M., & Bosy-Westphal, A. (2012). Beyond the body mass index: Tracking body composition in the pathogenesis of obesity and the metabolic syndrome. Obesity Reviews, 13 (Suppl 2), 6–13. Noreen, E. E., & Lemon, P. W. (2006). Reliability of air displacement plethysmography in a large, heterogeneous sample. Medicine and Science in Sports and Exercise, 38(8), 1505–1509. Nunez, C., Kovera, A. J., Pietrobelli, A., Heshka, S., Horlick, M., Kehayias, J. J., . . . Heymsfield, S. B. (1999). Body composition in children and adults by air displacement plethysmography. European Journal of Clinical Nutrition, 53(5), 382–387. Okorodudu, D. O., Jumean, M. F., Montori, V. M., RomeroCorral, A., Somers, V. K., Erwin, P. J., & Lopez-Jimenez, F. (2010). Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. International Journal of Obesity (2005), 34(5), 791–799. Otterstetter, R., Johnson, K. E., Kiger, D. L., Agnor, S. E., Kappler, R. M., Reinking, M., & Tessmer, K. (2015). Comparison of air-displacement plethysmography results using predicted and measured lung volumes over a protracted period of time. Clinical Physiology and Functional Imaging, 35(5), 328–331. Sardinha, L. B., Lohman, T. G., Teixeira, P. J., Guedes, D. P., & Going, S. B. (1998). Comparison of air displacement plethysmography with dual-energy X-ray absorptiometry and 3 field methods for estimating body composition in middle-aged men. American Journal of Clinical Nutrition, 68(4), 786–793. Sopher, A. B., Horlick, M., Wang, J., Pierson, R. N., & Heymsfield, S. B. (2002). Pediatric percent body fat (% BF): BIA and bodpod compared to DXA. FASEB Journal, 16(5), A1020–A1021. Tucker, L. A., Lecheminant, J. D., & Bailey, B. W. (2014). Test-retest reliability of the bod pod: The effect of multiple assessments. Perceptual and Motor Skills, 118(2), 563–570. Vescovi, J. D., Zimmerman, S. L., Miller, W. C., Hildebrandt, L., Hammer, R. L., & Fernhall, B. (2001). Evaluation of the BOD POD for estimating percentage body fat in a heterogeneous group of adult humans. European Journal of Applied Physiology, 85(3–4), 326–332. Wagner, D. R., Heyward, V. H., & Gibson, A. L. (2000). Validation of air displacement plethysmography for assessing body composition. Medicine and Science in Sports and Exercise, 32(7), 1339–1344. Wells, J. C., & Fuller, N. J. (2001). Precision of measurement and body size in whole-body air-displacement plethysmography. International Journal of Obesity and Related Metabolic Disorders, 25(8), 1161–1167.