Chimeric Antigen Receptor T cells, Current State of Development and Future Outlook Bachelor thesis: Biology, Utrecht University By: Mattijs Kaemingk (3993884) Date: 13-04-2018 1st supervisor: Rob de Boer, Theoretical Biology & Bioinformatics, Utrecht University 2nd supervisor: Can Kesmir, Theoretical Biology & Bioinformatics, Utrecht University 1 Index Abstract p. 3 Introduction p. 3 Chapter 1: CAR T Cells: Structure, Function and Maintenance p. 4 Chimeric antigen receptors CAR T cells CAR T cells in vivo Engineering immune cells: The living drug aspect p. 4 p. 5 p. 5 p. 5 Chapter 2: Manufacturing CAR T cells p. 6 Common steps Isolation and enrichment Activation Gene delivery Expansion Strategy combinations Clinical variability p. 6 p. 6 p. 6 p. 7 p. 8 p. 9 p. 9 Chapter 3: Clinical Results of CAR T cell treatment Successes and Limitations p. 9 FDA approval Kymriah (tisagenlecleucel) Yescarta (axicabtagene ciloleucel) Cytokine release syndrome On target tumor effects The immunosuppressive tumor-microenvironment p. 9 p. 9 p. 11 p. 12 p. 12 p. 12 Chapter 4: Ongoing Research Regarding Possible Improvements on CAR T Cell Therapy p. 14 Suicide gene Avoiding off-tumor toxicity Approaches to improve CAR T cell efficacy when treating solid tumors Combining antitumor strategies Allogeneic T cells CRISPR/Cas gene editing p. 14 p. 14 p. 15 p. 18 p. 19 p. 19 Chapter 5: Future Outlook on CAR T Cell Therapy p. 20 2 Abstract Although CAR T cell therapies are currently only approved for treatment of hematological malignancies, current research shows that CAR T cells could be eligible for much broader application. Many different strategies to further improve CAR T cells have been proposed and theoretically CAR T cell treatment has very few limits. However, in a practical sense, improving CAR T cells will face many challenges: toxicity, immunosuppressive factors, variable treatment results, and a highly variable, uncontrolled and unstructured manufacturing process. In order to lift CAR T cell therapy to its potential, very recent techniques like the production of safe allogeneic T cells and application of CRISPR/Cas gene editing need to be applied. Further research will provide more insight in the safety and efficacy of these techniques and thus give an indication of how realistic their application actually is. Introduction The immune system consists of various cells that have unique properties. They can move freely around the body and detect pathogens, virus infected cells, and other malignancies. Different subsets of immune cells form a complex, yet effective, mechanism to respond to such pathologic insults and deviations. Together, the immune cells can execute highly controlled specific counteractions like targeted cytotoxic activity, phagocytosis or more subtle actions like the secretion of cytokines that can mobilize other immune cells. Because of the powerful nature of immune responses, the immune system is highly controlled through various mechanisms. Various checkpoints keep lymphocyte activation and proliferation in check in order to prevent causing damage to healthy tissues during the process of disarming pathologic dangers. There are some diseases, such as cancer and autoimmunity, that can avoid immune responses. These diseases effectively impair the immune cells with immunosuppressive features that diminish lymphocyte activation, cytokine production or both. To achieve immune responses despite these complications, we could try to artificially adapt the immune system (Zhang et al., 2018). Synthetic immunology uses gene editing techniques to engineer lymphocytes. As a result, chimeric antigen receptor (CAR) T cells have emerged (Roybal & Lim, 2017). CARs are receptors that allow T cells to bypass other immune cells that are normally needed for activation and directly apply cytotoxic activity to their target (Rivière & Sadelain, 2017). Thus, effectively avoid immune complications caused by cancers or autoimmune diseases. CAR T cell therapy is currently applied to patients suffering from various hematological malignancies (Maude et al., 2018; Neelapu et al., 2017). Although this therapy has a promising potential in theory, its practical application faces many challenges (Zhang et al., 2018). CAR T cells need to be improved in various ways in order to lift its use in therapy to the next level. This review describes CAR T cells structure function, the manufacturing process currently in use and current clinical applications. Limitations of CAR T cell therapy and their various possible solutions are described, and a future outlook on what the future of CAR T cell therapy may look like is given. 3 Chapter 1 CAR T Cells: Structure, Function and Maintenance Chimeric antigen receptors CARs consist of three domains: An extracellular antigen-specific target binding domain. This domain is derived from an antibody’s single chain variable fragment (scFv) and binds the antigen on the target cell. This fragment is connect to the T cell with a hinge and a transmembrane segment, usually derived from CD8α or IgG4 (Schubert, et al., 2017). An intracellular domain is connected to the transmembrane segment and conducts the internal signalling by which the T cell is activated after binding to the antigen. There are different generations of CAR T cells, all are distinguished by their intracellular domain (figure 1) (Schubert et al., 2017). First generation CAR-T cells: In the first generation of CAR T cells, the ζ-subunit from the TCR/CD3 receptor complex is connected to the scFv part of the receptor (Schubert, et al., 2017). The ζ-subunit couples antigen recognition to several intracellular signal-transduction pathways (DeFord-Watts et al., 2011). This results in T cell activation similar to a TCR-mediated response. Second and third generation CAR T cells: In the second generation, a costimulatory signal to the intracellular domain is added to the intracellular component of the CAR. Examples of co-stimulatory domains used are CD28, CD27, DAP-12 and others (Savoldo et al., 2011). These co-stimulatory domains were shown to enhance and prolong CAR T cell activation (Chmielewski & Abken, 2015). Currently applied CAR T cell therapies make use of this generation CAR T cells and show promising results (Maude et al., 2018; Neelapu et al., 2017). The third generation CAR T cells use a combination of two of these co-stimulatory domains which further improves CAR T cell efficacy (Till et al., 2008). Fourth generation of CAR T cells: The fourth developed CAR T cell generation has additional genes engineered into its genome that code for secreted products (Chmielewski & Abken, 2015). The expression cassette from which these proteins are produced can be inducible, or constitutive, and can have a variety of functions (Zhang, Gu, & Xu, 2018). Possible examples are: proteins that diminish immunosuppressive environments frequently observed around solid tumors, or cytokines that recruit other immune cells to the site at which the target cell is present (Zhang et al., 2018). Figure 1: Schematic representation of the four currently developed generations CAR T cells. The 1 st generation consists of the ζ-subunit from the TCR/CD3 receptor complex. The 2nd generation adds a co-stimulatory molecule and in the 3rd generation two co-stimulatory molecules are added. The fourth generation also has an inducible or constitutive expression cassette of a transgenic protein. Figure taken from Chmielewski & Abken, 2015. and edited for lay-out purposes. 4 CAR T cells Chimeric antigen receptors (CARs) are synthetic immune receptors. They can be artificially engineered into T cells using gene editing techniques (Vormittag, et al., 2018). The CAR T cells are placed in vivo where they directly target their antigen on the target cell-surface. Normally, TCRs are activated by antigen presenting cells through the human leukocyte antigen (HLA). When binding its target, CAR can bypass HLA restriction and directly cause T cell activation. This is caused by the intracellular domain constructed onto CARs which starts the same signalling process as that of a normal TCR. Thus, making CAR T cells independent of antigen presenting and HLA downregulation. This is exceptionally beneficial when treating cancer because HLA downregulation frequently occurs in tumors. CAR T cells are able to recognise structures that are normally not targeted by TCRs, such as lipids or carbohydrates. This means that CAR T cells have a broader range of target antigens than the wild type T cell (Ramello, et al., 2018). When a CAR T cell activates by binding its target cell, it may undergo clonal proliferation to multiply and broaden their cytotoxic activity and releases cytokines that enhance immune activity, ultimately leading to lysis of the target cell. CAR T cells in vivo When T cells mature in the thymus they can express either CD4 glycoprotein or CD8 glycoprotein on their surface. CD8+ T cells are called cytotoxic T cells and CD4+ T cells are called T helper cells. Naive T cells can differentiate into different subsets: T stem memory cells (TSCM), T central memory cells (TCM), T effector memory cells (TEM) and T effector cells (TEFF) (Golubovskaya & Wu, 2016). CD8+ Teff cells are the cytotoxic form of T cells and kill their targets when activated. Additionally, after activation, they proliferate and can form TEM as a result. CD8+ TEFF cells are short-lived. If not for the formation of TEM the CAR T cell response would quickly fade after infusion because of cell death. TEM have a longer lifespan and can therefore facilitate a longer efficacy of CAR T cell treatment. CD4+ T cells are essential for CD8+ TEM cell formation (Shedlock & Shen, 2003). Thus, it is important to include CD4+ T cells into CAR T cell treatment to maximise its persistence. Research has shown that the ratio CD4+:CD8+ is very important for treatment efficacy. It was also shown that less differentiated subsets of T cells yield better results than cells that are differentiated towards the effector phenotype. The most optimal subsets are naive T cells (TN), memory stem T cells (TSCM) and central memory T cells (TCM) and thus these subsets are used for CAR T cell therapy (Gattinoni et al., 2011; Jensen & Riddell, 2014). Generation of memory cells is not only beneficial in the initial attack against tumor cells but may also have a great advantage against eventual relapses in patients. Theoretically, when patients have relapses after CAR T cell therapy, there is no need for a renewed treatment since they now possess the ability to fight the tumor cells on their own. Engineering immune cells: The living drug aspect Most traditional drugs are based on relatively simple molecules which target one specific molecule and disrupt or activate its function. Engineered cells, however, have the potential to operate as smarter therapeutics. They can detect environmental inputs and act accordingly applying comprehensive response programs. In other words: ‘’a molecular drug is a tool that is designed to do a single job, whereas a cell is a device that, like a computer, can be programmed to deploy the right set of tools, depending on the situation (Roybal & Lim, 2017)’’. Because lymphocytes are all part of the immune system and all influence other immune cells in particular ways, engineering these cells can create impacts on large parts of the immune network. Other reasons for engineering immune cells are that they can easily be harvested, engineered and transferred back in vivo, and that they have the potential to survive persistently over the course of decades (Roybal & Lim, 2017). Immune cells can also detect the progression of a disease and adapt accordingly (Roybal & Lim, 2017). 5 Chapter 2 Manufacturing CAR T cells Common steps There are various ways of manufacturing T cells which express CARs. However, they do all follow the same common steps. First, the lymphocytes cells are obtained from the patients by leukapheresis (Vormittag et al., 2018). When the lymphocytes are isolated they are activated, transduced with the CAR transgene, multiplied to the cell number required for therapy, formulated and filled (Vormittag et al., 2018). Isolation and enrichment The lymphocytes are isolated from the blood by a method called leukapheresis (Levine, 2015). Leukapheresis is a more specific form of apheresis, the more general term for isolating a specific part of blood. The blood components are separated based on density by centrifugation. The red blood cells, blood platelets and the anticoagulants added during the leukapheresis are removed in a cell washer (Levine, et al., 2017; Vormittag et al., 2018). They are seen as contaminations since anticoagulants can potentially alter the behaviour of the lymphocytes during activation and the red blood cells can lead to clumping (Engstad et al., 1997; Fesnak, et al., 2006; Vormittag et al., 2018). When the bulk of the leukapheresis buffer and anticoagulants are washed out, the solution is enriched for lymphocytes by counterflow centrifugal elutriation which separates the cells by size (Vormittag et al., 2018). In this step, monocytes, residual red blood cells and platelets are removed from the product (Bruce L. Levine et al., 2017) . Activation To activate normal T cells, their T cell receptors (TCRs) must be presented with antigen they do not recognise as a familiar structure. In vivo, T cells are activated by antigen presenting cells (APCs), which present antigen to the T cells using the major histocompatibility complex (MHC). The TCR interacts with the MHC aided by costimulatory molecules such as CD28, OX40 and others (Chen & Flies, 2013). Activating T cells using antigen presenting cells is a very slow and complicated process (Levine, 2015). Methods that mimic stimulation of T cells have been developed to avoid using these cells to activate the T cells. Monoclonal antibodies and interleukins: One approach to artificially activate T cells is through the use of OKT3 (anti-CD3 monoclonal antibody (mAb)) and interleukin 2 (IL-2). The anti-CD3 mAbs are recognised by the CD3 co-receptors on the T cells on both CD4+ and CD8+ T cells. This recognition leads to the onset of T cell activation. IL-2 is essential for T cell proliferation (Golubovskaya & Wu, 2016). The concentration of IL-2 used varies considerably in different trials (Vormittag et al., 2018). When using excessive IL-2 concentrations exhausted T cell products were observed that were close to a dysfunctional state (Barrett et al., 2014). Because of this, other interleukins like IL-7 and IL-15 instead of IL-2 were tested, resulting in a higher percentage of memory T cell subsets (Ghassemi et al., 2016). Cell-sized anti-CD3/CD28 antibody coated magnetic beads: An alternative to mAbs combined with interleukins is the anti-CD3/CD28 antibody coated magnetic beats strategy. These are magnetic beads roughly representing APCs in size and shape covered with antibodies against the CD3 and CD28 costimulatory receptors. After the activation process, the beads can be efficiently removed with an electromagnet (Vormittag et al., 2018). 6 Gene delivery Gene delivery into T cells can be achieved using viral vectors or non-viral vectors. Both approaches have their own advantages and disadvantages. Viral Vectors: Retro virus derived vectors as well as lentiviral vectors can be used to transduce T cells. These vectors can result in high transduction efficiencies (Vormittag et al., 2018). When using viral vectors activation of T cells is required, especially when using retrovirus vectors which only transduce dividing cells (Riviere & Sadelain, 2017). The viral vectors both integrate in the human genome in a semi random way. They both have a preference for transcribed regions with a subtle difference: retroviral vectors have a preference for transcriptional start-sites and lentiviral vectors distribute themselves more evenly along the transcribed areas (Riviere & Sadelain, 2017). This difference in transduction-preference is thought to contribute to the slightly higher genotoxicity of retroviral vectors (Riviere & Sadelain, 2017). Transposon Vectors: Alternatively, DNA transposon plasmids can be used for gene delivery. Transposons are DNA sequences that can insert themselves into a genome via transposase excision and insertion (Ivics, et al., 1997). These transposons can be used to insert the CAR transgene into T cell genomes. The CAR transgene can be inserted into a transposon sequence on a DNA plasmid. On this plasmid a transposase gene should also be encoded. These CAR-containing-transposon plasmids can then be inserted into the T cells using electrophoresis. When the construct enters the cell, the transposase excises the CAR-containing-transposon and inserts the sequence into the T cell genome (Vormittag et al., 2018). In contrast to viral vectors, when using transposon vectors for gene delivery, cells can be transfected before cell activation (Vormittag et al., 2018). This means that no non-transfected cells proliferate during the activation step and thus yielding only transfected cells instead of a mixture of transfected and non-transfected cells (Vormittag et al., 2018). Transposon vectors are significantly cheaper than their viral counterparts due to the fact that these vectors do not need expensive biosafety testing and storage (Riviere & Sadelain, 2017; Vormittag et al., 2018). Additionally, the maximum size of DNA transfected is bigger when using transposon vectors than when using viral vectors. Viral vectors can only transduce approximately 10kB base pairs into the T cells (Ptáčková et al., 2018). This might become a problem since recent evidence suggests that there is need to transfer multiple transgenes simultaneously to better control CAR T cells when in vivo (this is further described in chapter 4) (Kakarla & Gottschalk, 2014). Sleeping beauty: Transposon vectors seem promising in CAR T cell development. The Sleeping Beauty (SB) transposon system has been used to produce CAR T cells with promising clinical results (Singh et al., 2011). The Sleeping Beauty gene integration was also found to be the safest gene integration method concerning genotoxicity when compared to viral vectors and other transposon plasmids (Gogol-Döring et al., 2016; Vormittag et al., 2018). One disadvantage of the plasmid vector system is that generating the required cell numbers takes significantly longer as opposed to when using viral vectors (Kebriaei et al., 2015). Currently, viral vector gene integration is most commonly used to create CAR T cells (Vormittag et al., 2018). However, if it can be proved that the relatively new Sleeping Beauty vector can create a safe an effective product, this approach will most likely become the new standard for T cell transduction. 7 Expansion When the T cells are successfully transduced or transfected with the CAR genes they must be multiplied to a cell number adequate for therapy. This can be achieved by increasing the container volume in which the T cells are present after activating them, so they can proliferate and reach higher cell numbers. For this, a variety of methods are possible which can be divided into three approaches: T flasks, static culture bags and the rocking motion (RM) bioreactor (Vormittag et al., 2018). T-flasks: The T cells can be expanded by placing them on multiple tissue culture plates or flasks (Till et al., 2008). This approach needs frequent medium changes and thus is very labour intensive. Because of this, this approach is not optimal for large-scale manufacturing and this method is primarily used for smaller patient groups (Vormittag et al., 2018). Static culture bags: Alternatively, static culture bags can be used. This means scaling up the containers in which the cells are cultured rather than dividing them over more containers. This method is advantageous because the bags can be connected in a sterile way which reduces the amount of handling steps and thus the labour intensity (Tumaini et al., 2013). Rocking motion bioreactor: The most advanced technique utilises the most recent technology. The culturing starts in bags or flasks but is ultimately finished inside of a RM bioreactor (Tumaini et al., 2013). This bioreactor reduces labour intensity even further using a perfusion regime on the media which removes the growth-inhibiting substances and ensures constant amounts of nutrients (Janas et al., 2015). This means less media is needed to culture the cells as opposed to the culture bags. It was found that using this method instead of the culture bags/flasks reduced labour intensity to 33% and media consumption to 50% (Sadeghi et al., 2011). Figure 2: A schematic representation of the commonly followed steps when manufacturing CAR T cells. The grey circles represent the percentages of clinical trials that used the respective method. Coloured lines depict the most used combinations of methods in all analysed clinical trials. Image was taken from Vormittag et al., (2018) and edited for layout purposes. 8 Strategy combinations An analysis of data published from all the CAR T cell clinical trials between 2002 to 2017 shows that the anti-CD3/CD28 antibody coated magnetic beats strategy is currently most used for activating T cells, 66% of all clinical trials used this method (Vormittag et al., 2018). Most trials used lentiviruses to transduce T cells (54%), but also a significant number of trials used the retrovirus approach (41%). For T cell expansion most trials used the rocking motion bioreactor (43%), T-flasks (22%) and static culture bags (35%) were less frequently applied (Vormittag et al., 2018). Analysis of what routes clinical trials took to manufacture CAR T cells yielded different approaches. The route of activation through coated magnetic beats combined with the RM bioreactor was the most used combination (43%) (Vormittag et al., 2018). The second most used route combined mAb/IL-2 activation with expansion in static culture bags (19%) (Vormittag et al., 2018). Third most used was the combination of magnetic bead activation and static culture bags (18%) (Vormittag et al., 2018). Additionally, all the data together shows that CAR T cell culturing typically takes 20 days or more (Vormittag et al., 2018). Clinical variability Many factors in the steps of CAR T cell production yield variable products. Apheresis products are individually different for each patient and the rate at which the T cell expand can vary substantially (Vormittag et al., 2018). One clinical trial reported between 23.6 and 385-fold expansion in ten patients in the almost the same culture time (Brentjens et al., 2011). These results indicate the unpredictability of T cells in the process of CAR T cell culturing. Transduction efficiencies are divergent as well, in the same study, transduction efficiencies between 4% and 70% were described (Brentjens et al., 2011). The CAR T cell doses which are infused vary between different studies. There is no clear correlation between CAR T cell dosage and treatment efficacy either, a sufficient expansion rate can compensate for low infusion dosage and vice versa (Vormittag et al., 2018). Chapter 3 Clinical Results of CAR T Cell Treatment; Successes and Limitations FDA approval Because of positive results in the treatment of B-derived malignancies the U.S. Food and Drug Administration (FDA) approved two gene therapies for B cell malignancies based on CAR T cells (Ramello et al., 2018). Kymriah (tsigenlecleucel) was approved for the treatment of B-cell precursor acute lymphoblastic leukemia (ALL) for patients up to 25 years of age and Yescarta (axicabtagene ciloleucel) was approved for patients with diffuse/refractory large B-cell lymphoma (Ramello et al., 2018). Kymriah (tisagenlecleucel) CTL019, called Kymriah after FDA approval, is a 2nd generation anti CD19 CAR T cell line with the costimulatory CD137 (4-1BB) domain (Kalos et al., 2011). CTL019 is currently used in treatment of Bcell precursor ALL (Ramello et al., 2018). B-cell precursor ALL is a stem cell disorder that causes an overproduction of B cell lymphoblasts in the bone marrow causes lymphocytosis (Randolph, 2004). CTL019 targets CD19, which is a cell-surface protein of human B lymphocytes whose expression 9 persists throughout the B cell differentiation (Tedder & Isaacs, 1989). The 4-1BB domain improves the persistence of the CAR T cells through delaying T cell exhaustion (Long et al., 2015). A phase 2 pivotal, multisite study of CTL019 treatment which included 25 study sites in 11 countries across the world was initiated to analyse the efficacy and safety of the treatment using a global supply chain to provide the clinical centres with the required materials (S. L. Maude et al., 2018). In this study CTL019 was generated using a lentiviral vector to transduce autologous T cells with a CAR which contained a CD3-ζ domain for T cell activation and a 4-1BB (CD137) domain as a co-activator. High risk pediatric patients treated suffered from relapsed or refractory B cell ALL. The primary end point of this study was an overall remission rate of 20% (null hypothesis). Overall remission rate was defined as the rate of an overall response within three months. Responses were required to be maintained for at least 28 days to be eligible (S. L. Maude et al., 2018). A total of 107 patients were screened of which 92 enrolled in the trial. Of these, 17 potential patients were found not eligible and thus 75 were infused with CTL019. An overall remission rate of 81% was found in the 75 treated patients within three months (61 patients with a full remission). These remissions were durable for at least 28 days. Relapse free survival rate of 80% was observed at six months and 59% at 12 months after infusion. 17 patients with complete remission had a relapse before they received additional anticancer therapy. The median response duration was not reached before the results were reported (Figure 3A). At 6 months, the rate of event free survival was 73% in all 75 patients. At 12 months, this was 50%. The rates of overall survival were 90% at 6 months and 76% at 12 months after infusion. The median event free survival was not found. Nineteen patients died after CTL019 infusion (Figure 3B). Ongoing CTL019 persistence was observed more than 1 year after treatment. Figure 3 A: A graphical depiction of the duration of remission in 61 patients that had an overall response of complete remission after treatment with Tisagenlecleucel (CTL019) CAR T cell treatment, described by Maude et al., (2018). The duration of remission is defined as the time to relapse after the onset of remission. B: the black line depicts event free survival among all 75 treated patients defined as the time from infusion to the earliest of events like: no response (8 patients), relapse before maintenance of response for 28 days (2 patients), or relapse after having a complete remission (17). The grey line represents the overall survival rate. 19 patients died after CTL019 infusion (events defined as deaths), 56 patients had their data censured at the time of the last follow up. Graph taken from Maude et al., (2018) and edited for lay-out purposes. 10 All risks associated with CTL019 were mitigated in most patients with supportive measures and cytokine blockade. These results show that CTL019 treatment can lead to high remission rates and a long-term persistence in patients up to 25 years old with relapsed or refractory B cell ALL. Thus, proving to be a viable option for high risk pediatric patients. Yescarta (axicabtagene ciloleucel) Axicabtagene ciloleucel (axi-cel) is a 2nd generation CAR-T cell with a CD3-ζ domain for T cell activation connected to a CAR that targets CD19. This type of synthetic T cell differs from CTL019 in its costimulatory intracellular domain, it replaces 4-1BB with CD28. Axi-cel therapy is mostly used for treatment of diffuse large B cell lymphoma (DLBCL). This is the most common type of lymphoma (Neelapu et al., 2017). There are numerous subtypes of DLBCL, including primary mediastinal B cell lymphoma and transformed follicular lymphoma. Efficacy and long-term viability of the axi-cel treatment has been tested in a study which observed patients for several years after infusion. Ongoing remissions beyond 4 years after infusion were observed in patients infused with axi-cel T cells (Kochenderfer et al., 2017). A phase 2 multisite study regarding safety and efficacy has been conducted for this treatment (Neelapu et al., 2017). The target of these trials were to get response rates higher than those of existing therapies, which are objective response rates of 26% and complete response rates of 7% of all patients treated (Crump et al., 2017). A total of 111 patients enrolled in the study. For 110 axi-cel treatment was manufactured and administered to 101 patients. Median age of the patients was 58 years, and all suffered from stage III or IV diffuse large B cell lymphoma (DLBCL), transformed follicular lymphoma (TFL) or primary mediastinal B cell lymphoma (PMBCL). At 6 months after infusion, the objective response rate was 82% with a 54% complete response rate (figure 4). The response rates were consistent across age, disease stage, cell of origin subtype and method of side effect treatment. These results together with the observation of remissions beyond 4 years after infusion show that axicel can contribute substantially to clinical treatment for refractory lymphoma (Kochenderfer et al., 2017; Neelapu et al., 2017). Figure 4: Graph depicting the objective response rate (ORR) among patients that received axicabtagene (axi-cel ) CAR T cell treatment, observed by Neelapu et al., (2017). ORR is calculated as a complete response (CR) plus partial response (PR) as well as the response among patients with stable disease (SD), disease progression (DP) and patients that could not be evaluated (NE). Results are shown for patients suffering from diffuse mediastinal large B cell lymphoma (first panel), patients suffering from primary mediastinal large B cell lymphoma or transformed follicular lymphoma (second panel), and all patients taken together (third panel). Image was taken from Neelapu et al., (2017) and was edited for layout purposes. 11 Cytokine release syndrome Both phase 2 studies described above reported severe side effects when analysing the CAR T cell treatments. The most common and serious side effect of these treatments is cytokine release syndrome (CRS). In the study concerning CTL019 treatment 73% of the patients were found to suffer from CRS and in the axi-cel study this percentage was 93% (S. L. Maude et al., 2018; Neelapu et al., 2017). Systematic review of six clinical trials conducted in four different institutions found that CRS occurs in nearly two-third of patients treated wit CAR T cell infusion (Xu & Tang, 2014). CRS is caused by the release of cytokines after cell lysis induced by cytotoxic activity of effector T cells (Breslin, 2007). These cytokines accumulate and when a certain concentration is reached, cause a constellation of symptoms like fever, chills, headache, nausea, fatigue and hypotension that usually start within a week after treatment (Breslin, 2007; Perales, et al., 2018). CRS can eventually progress to severe CRS which shows symptoms like: hypotension, capillary leak, respiratory compromise and sometimes macrophage activation syndrome (Perales et al., 2018). Marked elevation of IFN- γ, soluble IL-2 receptor and IL-6 can identify which patients will develop severe CRS. These cytokines appear to play an important role in the CRS process (Perales et al., 2018). Disrupting IL-6 function is currently the most used strategy to combat CRS. Tocilizumab, an IL-6 receptor antagonist was used in both phase 2 studies previously described and is the most common medicine used (S. L. Maude et al., 2018; Neelapu et al., 2017; Perales et al., 2018). Other IL-6 inhibitors such as siltuximab, an antibody that binds directly to IL-6, might be a better fit and are under investigation for potential future use to treat CRS (Perales et al., 2018). On-target off-tumor effects When CAR T cell therapy is used to treat cancer, tumor specific antigens (TSAs) are commonly targeted by the CARs of the infused T cells. Most potential targets are show some level of expression on other body tissues as well. This can be problematic for treatment because it can lead to CAR T cell-mediated attack on healthy cells and result in an on-target off-tumor toxicity of the treatment (Ebert, et al., 2018). When treating B-lymphoma by targeting CD19 this is also the case. The CD19 CAR T cells not only target the cancerous B cells but also the healthy ones. This often leads to complete depletion of B cell lines in patients resulting in the requirement of immunoglobulin replacement (S. Maude & Barrett, 2016). The immunosuppressive tumor micro-environment Although CAR T therapy has shown a lot of promise for cancer treatment, there are limitations that have yet to be overcome. One of these limitations is the tumor micro-environment (TME). This area contains inhibitory factors which impair CAR T cell cytotoxicity (E. Zhang et al., 2018). The TME impairs CAR T cell therapy for cancers that develop solid tumors and this is the most prominent reason this therapy is currently only applicable in hematological malignancies. Antigen heterogeneity: CAR T cell therapy is based on antigen recognition by single chain variable fragment (scFv) structures (Schubert et al., 2017). Solid tumors have poor antigen heterogeneity, this complicates antigen binding and T cell activation (Jamal-Hanjani, et al., 2015; Zhang et al., 2018). T cell checkpoints: T cell activity is limited by several checkpoints which regulate T cell function: Cytotoxic T lymphocyte-associated antigen 4 (CTLA4), programmed cell death 1 (PD1), lymphocyteactivation gene 3 (LAG3), T-cell immunoglobin mucin 3 (TIM3) and V-domain Ig suppressor of T cell activation (VISTA) (figure 5A) (E. Zhang et al., 2018). CTLA4, a homolog of CD28, is thought to recruit a 12 phosphatase to the CD3ζ domain of TCRs and deactivates its signal transduction, effectively preventing T cell activation (Bradshaw et al., 1997). PD1 is a cell surface receptor expressed only on T lymphocytes (Ishida, et al., 1992). Its ligands (PDL1 of PDL2) are presented by tumor cells and when they bind to PD1, it negatively regulates internal T cell activation signals (Blank & Mackensen, 2007). The protein LAG3 is an important inhibitory receptor which binds MHCII with an higher affinity than CD4, effectively preventing antitumor responses by blocking target cell recognition (Kisielow, et al., 2005). TIM3 initiates the TIM3/Galectin-9 signalling pathway, this pathway inhibits T cell responses and can promote their apoptosis pathways (E. Zhang et al., 2018; Zhu et al., 2005). VISTA is a receptor expressed on hematopoietic cells and leukocytes which can reduce the activity of T cell and production of cytokines (Wang et al., 2011; E. Zhang et al., 2018). Figure 5: A schematic representation of the TME and its immunosuppressive features. A: Activated T cells often express immune checkpoints that diminish their own activity (CTLA4, PD1, LAG3, TIM3 and VISTA), target cells express some immune checkpoint ligands (PDL1, PDL2). T cells lack receptors like CCR2b or CCR4 to recognise tumor chemokines. B: In the TME immunosuppressive cells (Tregs, MDSCs and TAMs) and cytokines (TGFβ and IL-10) are present which impair cytotoxic functionality. C: Physical barriers of the TME, an abundance of ECM (HSPGs) inhibit the penetration of T cells. D: The intratumoral microenvironment is hypoxic, poor nutrient concentrations and a low pH. E: Other immunosuppressive factors like CD47, CD73 derived adenosine and IDO further inhibit CAR T cell function. Image was taken from E. Zhang et al., (2018) and edited for lay-out purposes. 13 Poor T cell homing due to missing receptors: Another obstacle when using CAR T cell therapy to treat solid tumors is the poor homing of these cells to the tumor bed because of inadequate chemokine recognition. Tumors express and secrete chemokines, like CXCL12 and CXCL5, but these are not matched by receptors on the CAR T cells and thus do not contribute to their targeting of tumor cells. (Harlin et al., 2009; E. Zhang et al., 2018). Immunosuppressive cells and cytokines: The TME houses several immunosuppressive cells and secreted cytokines; regulatory T cells (Tregs), myeloid derived suppressor cells (MDSCs) and tumor associated macrophages (TAMs) (figure 5B). These all secrete various cytokines, like IL 10 and TGFβ which suppress T cell function (E. Zhang et al., 2018). They also take up IL-2 which is needed for T cell proliferation and thus diminishes the T cell mediated immunity (E. Zhang et al., 2018). Tumor extracellular matrix and intratumoral microenvironment: An additional challenge of the ECM for CAR T cells is its extracellular matrix (ECM) (figure 5C). This matrix includes proteoglycans and glycopeptidases and is physically almost impossible to penetrate for CAR T cells (E. Zhang et al., 2018). The hostile tumor environment is characterised by poor oxygen (O2) and nutrient supply (Balkwill, et al., 2012). Additionally, low pH levels are frequently observed in the TME as a result of high hydrogen ion levels which originating from lactic acid and carbonic acid (figure 5D) (Ganapathy, et al., 2009). Other immunosuppressive factors: Other immunosuppressive factors in the human immune system are CD47, adenosine and indoleamine 2,3-dioxygenase (IDO) (figure 5E). CD47 is a transmembrane protein which is overexpressed on the surface of solid tumors (Oldenborg et al., 2000; E. Zhang et al., 2018). It suppresses immune activity against solid tumors by interacting with the signal regulatory protein α (SIRPα) used by macrophages to conduct immune surveillance (Barclay & van den Berg, 2014). CD47-SIRPα interaction suppresses macrophage activation and thus acts as an immune suppressor. Adenosine is generated from extracellular adenosine monophosphate (AMP) by the CD73 ectoenzyme expressed by tumor cells or immunosuppressive cells. Adenosine can bind the adenosine 2A receptor (A2RR) on T cells which results in T cells that are not functional against solid tumors (Allard, et al., 2016). IDO can suppress T cell function by binding to tryptophan, which is a key amino acid required for T cell activity (E. Zhang et al., 2018). Chapter 4 Ongoing Research Regarding Possible Improvements on CAR T Cell Therapy Suicide gene Severe CRS, off-target effects or other toxicity side-effects are frequently observed during CAR T cell therapy. Because of this, it would be beneficial to be able to eliminate CAR T cell activity post infusion (Perales et al., 2018). One possibility for such a safety measure is the incorporation of an inducible suicide gene into the CAR T cells. A potential gene is iCaspase9 (iC9), which is composed of a drug binding domain cloned in frame with human-caspase9 (Minagawa et al., 2016). This fusion allows for conditional activation of the caspase9 domain using a small-molecule drug. Caspase genes play a role in cell apoptosis and when activated, cell death rapidly follows. Incorporation of a suicide gene into CAR T cells would provide an extra safety measure to CAR T cell therapy by adding an off-switch to CAR T cell therapy that can be induced when side effects become too dangerous. Avoiding off-tumor toxicity Tumor specific antigens: To avoid off target effects finding tumor specific antigens (TSAs), markers that are only expressed on, and presented by, tumor cells in the early stage of differentiation must be found 14 (Clevers, 2011; Kreso & Dick, 2014). If these TSAs are identified, CARs that are specific for these epitopes can be developed (figure 8A). This would aid in tumor recognition and nullify the off-target effects of CAR T cell therapy. Combinatorial CAR T cell targeting: Finding ideal TSAs to treat tumors with CAR T cell therapy is a difficult and cumbersome process. Another strategy to circumvent the on-target off-tumor complication is to make CAR T cells target two antigens (Ebert et al., 2018). A proposed method uses a T cell engineered with two CARs that each have their own specific antigen target. Both CARs lack a different intracellular domain needed for T cell activation and thus need to complement each other to fully achieve T cell activation. This results in a T cell that needs to bind two specific antigens on its target cell to get activated and thus will not attack healthy tissue expressing one of these antigens (figure 6)(Ebert et al., 2018). This strategy was applied in a trial with engineered CAR T cells which expressed two different CARs: P28BB, which targets prostate-specific membrane antigen (PSMA) and Lz1, which targets prostate stem cell antigen (PSCA) (Kloss et al., 2012). Lz1 was linked to the intracellular CD3-ζ domain and P28BB Figure 6: A schematic representation of a CAR T cells with two CARs specific for different antigens. The receptors both signal for T cell activation but both signals need to be present simultaneously to achieve successful activation of the T cell. This mechanism allows for a more specific recognition of target cells and should reduce cytotoxic activity on healthy tissue when applying CAR T cell therapy. Image was taken from Ebert et al., (2018) and edited for lay-out purposes. Figure 7: Kloss et al., (2012) used CAR T cells with two different CARs which both partly signal for CAR T cell activation. Both need to bind antigen to achieve effective T cell activation. Graphs depicting data of tumors treated with different CAR T cell lines: Blue lines represent tumor cells treated with a solution devoid of T cells. The green line represents P28BB (CAR against PSMA antigen) CAR T cell treatment, the red line represents Lz1 (CAR against PSCA antigen) CAR T cell treatment. The orange line represents Lz1 + P28BB CAR T cell treatment. Tumor growth is shown for the duration after CAR T cell treatment up until 40 days. The left panel depicts growth rates of PSCA+ PSMA+ tumor cells. The middle panel depicts growth of PSCA+ tumor cells and the right panel depicts PSMA+ tumor growth. Only the PSCA+ PSMA+ tumor that was treated with CAR T cells expressing Lz1 and P28BB was effectively diminished in growth as shown by the orange line in the left panel. These results show that both CARs need to bind antigen for a successful CAR T cell response. Picture was taken from Kloss et al., (2012) and edited for lay-out purposes. 15 was linked to the intracellular 4-1BB costimulatory domain. Mice suffering from tumors expressing either one or both antigens were treated with these CAR T cells only the volume of the tumors expressing both antigens was reduced. This indicates that the CAR T cells can only be activated when both CARs bind their target (figure 7) (Kloss et al., 2012). Approaches to improve CAR T cell efficacy when treating solid tumors The previous chapter described a variety of complications in CAR T cell efficacy when treating solid tumors. All these challenges to CAR T cell mediated treatment are caused by the TME and its diverse immunosuppressive characteristics. However, it might be possible to arm the CAR T cells appropriately with genes which can counter the tolerogenic environment around solid tumors (E. Zhang et al., 2018). Infiltration and homing of CAR T cells: An improvement to CAR T cells could be the incorporation of chemokine receptors in the transgene construct which can detect tumor-specific chemokines (figure 8B). Expressing chemokine receptors in T cells has been investigated: CAR T cells expressing the chemokine GD2-specific receptor CCR2b were shown to migrate significantly faster to their respective target cells (Craddock et al., 2010). Similar results were obtained when T cells were artificially engineered to express the chemokine TRAC-specific receptor CCR4 (Di Stasi et al., 2009).These results indicate that engineering chemokine-specific receptors into CAR T cells can have a positive impact on treatment of solid tumors. In another clinical trial (NCT01722149), the potential for targeting cancer-associated fibroblasts (CAFs) is being investigated. CAFs facilitate angiogenesis and play a prominent role in progression and metastasis of solid tumors (E. Zhang et al., 2018). CAFs are characterized by their abundant expression of fibroblast activation protein (FAP). In the trial, the potential of previously developed T cells with a (FAP)-specific CAR have shown antigen specific functionality in vitro and in vivo (Schuberth et al., 2013). The effectiveness of CAR T cells in vivo is limited by their inability to infiltrate the tumor parenchyma. Integrin αvβ3 is generally highly expressed on the surface of the endothelial cells of this arenchyma. Because of this, a promising theory is put forward using a CAR that targets integrin αvβ3 (figure 8B)(Fu, et al., 2013). The heparan sulphate proteoglycan (HSPG) is abundantly present in the tumor-ECM. T cells cannot degrade HSPG and therefore cannot accumulate at tumor sites. A possible solution this problem was found by incorporating of the heparanase (HSPE) gene into CAR T cells (figure 8B)(Caruana et al., 2015). CAR-T cells secreting cytokines or enzymes: Co-expression of immune factors like IL-12 or IL-15, enzymes like catalase or other soluble secretion products like the herpesvirus entry mediator (HVEM) can further improve the T cells resistance to the TME (figure 8C)(Zhang et al., 2018). CAR T cells expressing IL-12 were shown to have enhanced activation and cytotoxicity and attracted endogenous T cells and other immune cells to eradicate cancer cells (Zhang et al., 2011). It was found that IL-15 plays an important role in the trafficking of T cells in vivo and thus, could have a positive effect on the penetration of the immunosuppressive environment around tumors when expressed by CAR T cells (Hsu et al., 2007). Catalase is an enzyme that can catalyse hydrogen peroxide to water and oxygen. CAR T cells expressing catalase could potentially reduce the oxidative stress mediated suppression of the TME (Ligtenberg et al., 2016). The HVEM gene is very often mutated in germinal center lymphomas (GCL) and loss of this gene drives the development of GCL by inducing a tumor-supportive microenvironment (E. Zhang et al., 2018). CAR T cell that were engineered to carry soluble HVEM were 16 found to enhance therapeutic activity against lymphomas by release this soluble around the tumor sites (Boice et al., 2016). CAR-T cells expressing receptors: Recent reports have revealed that CAR T cells expressing receptors for CD28 (CD28L) or 4/1BB (4/1BBL) in addition to their cytoplasmic signalling domains enhance T cell activity (figure 8D)(Holohan, et al., 2015). This is thought to be the cause of bidirectional signalling, with direct signalling within the T cells and indirect triggering of other immune cells that express the Figure 8: A schematic representation of possible CAR T cell surface modifications that could potentially enhance treatment efficacy. A: CARs directed against TSAs would specifically attack tumor cells. B: Chemoreceptors CCR2b and CCR4 detect chemokines secreted by tumor cells and improve CAR T cell homing. FAP-specific CAR T cells can migrate towards tumors, similar to integrin αvβ3 (or αvβ6)-specific CAR T cells. Heparanase expression enhances T-cell infiltration and antitumor activity. C: CAR T cells engineered to secrete cytokines such as IL-12 or IL-15 to resist a hostile environment. CAR T cells expressing catalase could potentially reduce the oxidative stress mediated suppression of the TME. CAR T cell that were engineered to carry soluble HVEM enhanced therapeutic activity against lymphomas by release this soluble around the tumor sites. D: CAR T cells co-expressing various receptors like 4/1BBL and CD40L enhance T cell activity. CAR T cells expressing IL-4 exodomain and IL-7 endodomain target IL-4 and subsequently convert the immunosuppressive response. CAR-T cells expressing IL-7Rα specific for IL-7 were shown to have enhanced activation, proliferation and antitumor activity. CAR T cells with dominant double mutated DN TGFβR were shown to survive longer in the presence of solid tumors. E: Several inhibitory checkpoints on T cell function can be avoided using mAbs or the CRISPR/Cas system. PD1:CD28 CAR that fused the PD1 receptor to an internal CD28 co-stimulatory domain enhanced T cell activity. F: Other possible blockage therapies include the incorporation of inhibitors that actively diminish CD73, A2AR, IDO or CD47 activity around CAR T cells. G: CAR T cell therapy can possibly be combined with other antitumor strategies like oncolytic viruses, HIF-CAR, exosomes, nanoparticles and the modulation of T cell metabolism. Image was taken from (Zhang et al., 2018) and edited for lay-out purposes. 17 CD28 of 4/1BB receptors (E. Zhang et al., 2018). Another signalling mechanism that could potentially improve the TME resistance of CAR T cells is CD40/CD40L axis (E. Zhang et al., 2018). This signalling pathway is essential in tumor rejection by effector T cells in the presence of tumor necrosis factor (TNF) and could be applied in CAR T cells by CD40L co-expression (figure 8D)(Marigo et al., 2016). Cytokine IL-7 promotes expansion of naïve and memory T lymphocytes (E. Zhang et al., 2018). T cells artificially expressing IL-7Rα which can specifically bind to IL-7 were shown to have enhanced activation, proliferation and antitumor activity (figure 8D)(Vera et al., 2009). Adding receptors or ligands to CAR T cells can be beneficial, However, disrupting existing receptors can have positive effects as well. Recent studies tested T cells that no longer express TGF-βR (a receptor for the immunosuppressive cytokine TGF-β)(figure 8D)(E. Zhang et al., 2018). It was shown that no longer recognising the suppressive cytokine resulted in T cells with longer survival (Foster et al., 2008). Applying this strategy to CAR T cells might yield similar results. Making CAR T cells express monoclonal antibodies which bind ligands of the checkpoint receptors has shown to promote CAR T cell efficacy (E. Zhang et al., 2018). Immune checkpoint therapy: A powerful brake on the efficacy of T cells is the inhibitory receptor/ligand pathway which includes inhibitory receptors on T such as PD1, CTLA4, LAG3, TIM3 or VISTA cells and their ligands that are often present on target cells. There are some methods that can alter T cells in a way that enables them to avoid these checkpoints. Checkpoint inhibition can be achieved by the blockage of the checkpoint receptors with mAbs (figure 8E). Another way to avoid T cell checkpoint is to knock out the genes for the inhibitory receptors (figure 8E). Knock-out PD1 and CTLA4 T cells have been engineered and the knock-outs yielded positive results on tumor eradication (Shi et al., 2017; Su et al., 2016). Alternatively, it is possible to fuse the PD1 receptor to a co-stimulatory domain (figure 8E). This results in enhanced T cell activity when PD1 is bound by its ligand expressed by tumor cells (Prosser et al., 2012). Other blockage therapies: To combat adenosine-derived immune suppression the interaction between adenosine and A2AR must be interrupted. It was found that human-epidermal growth factor receptor 2 (HER2)-specific CAR T cells had a higher efficacy against tumor cells expressing HER2 in the presence of an A2AR antagonist (Beavis et al., 2017). These results suggest that CAR T cells expressing A2AR antagonists can have an enhanced therapeutic effect (figure 8F)(E. Zhang et al., 2018). Another approach to this problem is the generation of an mAb specific for CD73 which would reduce the amount of CD73 derived adenosine (figure 8F)(E. Zhang et al., 2018). The IDO and CD47 pathways also harm CAR T cell efficacy, inhibiting these mechanisms has shown promising results (Liu et al., 2015; Ninomiya et al., 2015). Incorporating inhibitors for these pathways should produce CAR T cell which have a higher efficacy when treating tumors (figure 8F). Combining antitumor strategies It might also be possible to combine CAR T cell therapy with other antitumor strategies. Examples of strategies that could be combined with CAR T are: oncolytic viruses (OV), hypoxia-targeting, exosomes and nanoparticles (figure 8G). Oncolytic viruses can selectively infect tumor cells and promote cell lysis. They also induce robust immune responses which promote antitumor activity (E. Zhang et al., 2018). Loading CAR T cells with OVs significantly enhanced the trafficking and tumor infiltration of CAR T cells (Nishio & Dotti, 2015). An interesting strategy to prevent on-target, off-tumor effects while simultaneously improving CAR T cell homing is targeting of the hypoxic environment of the TME. An oxygen sensitive sub-domain of 18 hypoxia-inducible factor 1-alpha (HIF1α) can be inserted into the CAR T cells, resulting in a HIF-CAR cell that is sensitive to hypoxic environments (Juillerat et al., 2017). CAR T cell exosomes could be isolated and infused into patients, instead of the CAR T cells themselves, to treat cancers. This method allows for a controlled cytotoxic activity and avoids some adverse effects of CAR T cell immunotherapy (Tang et al., 2015). Impressive results were obtained using nanoparticles to reprogram leukaemia-specific T cells in vivo and therefore passing over a huge part of the CAR T cell manufacturing ex vivo (Smith et al., 2017). Due to potential off-target gene transfer this method, as of now, is not safe enough to apply in a clinical context and further research is required to investigate potential solutions to this safety issue (Smith et al., 2017). In addition to engineering CAR T cells to enhance their homing and target-binding qualities, it is also possible to modify their active metabolism. For instance, it was found that elevating the intracellular concentration of L-arginine promotes the generation of central-memory like cells, and thereby enhancing the anti tumor activity (Geiger et al., 2016). Another example is a study in which the antioxidant N-acetyl cysteine (NAC) was added which improved the quality and therapeutic efficacy of adoptive T cells (Scheffel et al., 2016). Allogeneic T cells The main disadvantage of autologous cells is that they must be harvested, activated, engineered and expanded per patient. Logistically, allogeneic cells would be an incredible alternative. Instead of having to manufacture CAR T cells for every patient individually, CAR T cells would become more of an ‘’off the shelf’’ medicine. To achieve this, donor T cells must be deprived of their alloreactive potential, so they do not mediate graft-versus-host disease (GVHD). Currently’, there are two approaches to removing the alloreactivity of T cells (Riviere & Sadelain, 2017). One potential strategy for reducing alloreactivity of T cells is selecting for virus-specific T cells which do not target host antigen when infused (Rivière & Sadelain, 2017). An alternative to prevent GVHD when using allogeneic cells is the ablation of TCR in donor cells. When T cells do not express functional TCR, they cannot attack host tissue without being specifically targeted by CARs (Riviere & Sadelain, 2017). A restriction of TCR ablation is the fact that TCR mediated signalling plays a part in T cell maintenance (Myers, et al., 2017). Removal of the TCR results in a gradually decreasing cell number in the T cell population (Myers, et al., 2017). In addition to TCR mediated T cell maintenance, it was found that other pathways can contribute to T cell survival as well (Myers, et al., 2017). T cell maintenance can also be mediated by tonic signalling. Tonic signalling is a process in which T cells induce memory cell formation by selfrecognition. It has been found that tonic signalling is independent of TCRs (Wiehagen et al., 2010). It might be possible to exploit this mechanism in order to generate allogeneic CAR T cells that are long lived. Tonic signalling is not yet fully understood and further research will show the validity of this approach (Myers, et al., 2017). CRISPR/Cas gene editing The vectors that are currently used introduce the CAR genes into T cells rely on random integration into the host cell genome. While this method has proven to be effective it does yield some variegated expression because of chromosomal position effects (Perales et al., 2018). Newer methods for gene editing have surfaced which can be used to insert the CAR genes into T cells. Perhaps the most promising of them is CRISPR/Cas. This targeted nuclease system is operationally simple and particularly precise, using a guide RNA to direct a short lived nuclease enzyme to the target site in the genome where it makes double strand breaks and the CAR gene can be inserted (Doudna & Charpentier, 2014). 19 Using this technique (Eyquem et al., 2017) disrupted the TRAC locus and placed a CD-19 specific CAR under its transcriptional control. The TRAC genus normally encodes TCRs and thus when CAR was placed under its control it would be regulated by the endogenous signalling a wild type TCR is normally subject to. When compared to a virally transduced CAR T cell, the endogenous regulation of CAR expression yielded reduced T cell acceleration and reduced exhaustion. It also increased the therapeutic potency of the engineered T cells rejecting solid tumours in mice. This was attributed to the differential recovery of cell surface CAR depending on the endogenous transcription regulated provided by enhancer and promoter elements regulating CAR expression (Eyquem et al., 2017). Gene editing using CRISP/Cas provides a safer way of placing the CAR transgene into the genome of T cells. By being able to hand-pick the location it gets integrated (Eyquem et al., 2017) were able to use TCR regulation on CAR expression which lead to beneficial results. Gene editing with CRISPR/Cas could also be beneficial when designing CAR T cells with larger cell constructs. When constructing 3rd and 4th generation CAR T cells, large DNA constructs have to be incorporated in T cells. These might be too large for viral integration. CRISPR/Cas can be used to achieve this instead. Additionally, CRISPR/Cas is an effective and reliable method for gene disruption. In a study investigating new gene editing techniques, a high disruption rate of the TRAC-locus was observed using CRISPR/Cas to create allogeneic T cells (Osborn et al., 2016). Chapter 5 Future Outlook on CAR T Cell Therapy CAR T therapy, while effective, is considered to be dangerous due to its various potential toxicity effects (Perales et al., 2018).This safety concern has been addressed in various studies and several adaptations to CAR T cells have been proposed. A safety switch such as an inducible caspase gene would make CAR T therapy reversible when side-effects become too dangerous (Minagawa et al., 2016). Target-specificity can be improved by finding tumor specific antigens or combinational CAR T cell targeting and further reducing toxicity of the therapy. Despite remarkable successes treating hematological malignancies, CAR T cell mediated treatment of solid tumors lags behind. The biggest obstacle when treating diseases featuring solid tumors is the immunosuppressive micro environment they entail. Many options are currently being investigated to engineer CAR T cells that are resilient against the TME immunosuppression and solutions have been proposed for almost all its complications (E. Zhang et al., 2018). Incorporation of these strategies into CAR T cell therapy might result in a CAR T cell line that can be used to treat solid tumors. This would increase the scale of CAR T cell therapy immensely by multiplying its applications. Proposed strategies to arm CAR T cells versus the TME all rely on advanced CAR generations; many studies engineered additional receptors or genes coding for protein secretion. Since all proposed methods only target one specific feature of the TME immunosuppression, a combination of these methods is required. However, this would lead to a transgene construct that codes for many genes. Such a construct might become too large to be incorporated by viral vectors. Thus, causing complications manufacturing these CAR T cells for therapy. CRISPR/Cas gene editing could potentially solve many problems in CAR T cell therapy. By being able to select a precise location in the genome to place the transgene product. Potential toxicity caused by random integration could be avoided. When using CRISPR/Cas, larger transgene constructs can be engineered into T cells. This would allow the production of CAR T cells which could potentially disarm the immunosuppression of CAR T cells. 20 As was shown by data analysis of trials applying CAR T cell therapy, current processes in clinical trials are divergent and use a variety of different technologies (Vormittag et al., 2018). This, together with the fact that primary apheresis products differ substantially per patient, expansion variability, transduction variability and the fact that there is no demonstrable correlation between CAR T cell dosage and therapeutic effectivity leads to a wide variety of results between clinical trials (Vormittag et al., 2018). Production processes should be highly controlled and minimise variability amongst different clinical institutes. Effective coordination amongst the collection, manufacturing and treatment sites that are involved in the production process is crucial. The materials must be handled correctly, and patients should be appropriately scheduled for treatment. To achieve consistent results in CAR T cell therapy, a standardised protocol which leads to a uniform product is of utmost importance. In the hypothetical case that CAR T cell therapy might become applicable for treating solid tumors, the scale of CAR T therapy will undoubtedly grow exponentially. Currently, manufacturing CAR T cells and applying treatment requires a lot of expertise. A global demand would mean an immense amount of education in clinical instances. Perhaps the most important implication of CRISPR/Cas for CAR T cell therapy is its ability to disrupt genes. If TRAC-genes can be successfully knocked out in T cells, allogeneic T cells can be produced. Allogeneic T cells would allow for a structured manufacturing process. When CAR T cells can be produced in bulk and distributed to medical clinics, only the infusion process has to be applied on site and this would effectively reduce the amount of training necessary for CAR T cell therapy. This would effectively solve the manufacturing problem and reduce the demand for trained experts in CAR T cell treatment. Allogeneic T cells would also solve the manufacturing problem. A defined protocol can be established and carried out in a highly controlled manner when producing CAR T cells in bulk. CAR T cell therapy has the potential for many applications. In theory, the various obstacles that are currently limiting its applicability can all be overcome. However, to achieve this, application of very recently developed techniques is required. These techniques, like CRISPR/Cas, are in very early stages of development and it will take time testing them for efficacy and safety. 21 References Allard, B., Beavis, P. A., Darcy, P. K., & Stagg, J. (2016). Immunosuppressive activities of adenosine in cancer. Current Opinion in Pharmacology, 29, 7–16. https://doi.org/10.1016/j.coph.2016.04.001 Balkwill, F. R., Capasso, M., & Hagemann, T. (2012). The tumor microenvironment at a glance. Journal of Cell Science, 125(23), 5591–5596. https://doi.org/10.1242/jcs.116392 Barclay, A. N., & van den Berg, T. K. (2014). The Interaction Between Signal Regulatory Protein Alpha (SIRP <scp>α</scp> ) and CD47: Structure, Function, and Therapeutic Target. Annual Review of Immunology, 32(1), 25–50. https://doi.org/10.1146/annurev-immunol-032713-120142 Barrett, D. M., Singh, N., Liu, X., Jiang, S., June, C. H., Grupp, S. A., & Zhao, Y. (2014). Relation of clinical culture method to T-cell memory status and efficacy in xenograft models of adoptive immunotherapy. Cytotherapy, 16(5), 619–630. https://doi.org/10.1016/j.jcyt.2013.10.013 Beavis, P. A., Henderson, M. A., Giuffrida, L., Mills, J. K., Sek, K., Cross, R. S., … Darcy, P. K. (2017). Targeting the adenosine 2A receptor enhances chimeric antigen receptor T cell efficacy. Journal of Clinical Investigation, 127(3), 929–941. https://doi.org/10.1172/JCI89455 Blank, C., & Mackensen, A. (2007). Contribution of the PD-L1/PD-1 pathway to T-cell exhaustion: an update on implications for chronic infections and tumor evasion. Cancer Immunology, Immunotherapy, 56(5), 739–745. https://doi.org/10.1007/s00262-006-0272-1 Boice, M., Salloum, D., Mourcin, F., Sanghvi, V., Amin, R., Oricchio, E., … Wendel, H. G. (2016). Loss of the HVEM Tumor Suppressor in Lymphoma and Restoration by Modified CAR-T Cells. Cell, 167(2), 405–418.e13. https://doi.org/10.1016/j.cell.2016.08.032 Bradshaw, J. D., Lu, P., Leytze, G., Rodgers, J., Schieven, G. L., Bennett, K. L., … Kurtz, S. E. (1997). Interaction of the cytoplasmic tail of CTLA-4 (CD152) with a clathrin- associated protein is negatively regulated by tyrosine phosphorylation. Biochemistry, 36(50), 15975–15982. https://doi.org/10.1021/bi971762i Brentjens, R. J., Rivière, I., Park, J. H., Davila, M. L., Wang, X., Stefanski, J., … Sadelain, M. (2011). Safety and persistence of adoptively transferred autologous CD19-targeted T cells in patients with relapsed or chemotherapy refractory B-cell leukemias. Blood, 118(18), 4817–4828. https://doi.org/10.1182/blood-2011-04-348540 Breslin, S. (2007). Cytokine-Release Syndrome: Overview and Nursing Implications. Clinical Journal of Oncology Nursing, 11(0), 37–41. https://doi.org/10.1188/07.CJON.S1.37-42 Caruana, I., Savoldo, B., Hoyos, V., Weber, G., Liu, H., Kim, E. S., … Dotti, G. (2015). Heparanase promotes tumor infiltration and antitumor activity of CAR-redirected T lymphocytes. Nature Medicine, 21(5), 524–529. https://doi.org/10.1038/nm.3833 Chen, L., & Flies, D. B. (2013). Molecular mechanisms of T cell co-stimulation and co-inhibition. Nature Reviews. Immunology, 13(4), 227–242. https://doi.org/10.1038/nri3405 Chmielewski, M., & Abken, H. (2015). TRUCKs: the fourth generation of CARs. Expert Opinion on Biological Therapy, 15(8), 1145–1154. https://doi.org/10.1517/14712598.2015.1046430 Clevers, H. (2011). The cancer stem cell: Premises, promises and challenges. Nature Medicine, 17(3), 313–319. https://doi.org/10.1038/nm.2304 Craddock, J. A., Lu, A., Bear, A., Pule, M., Brenner, M. K., Rooney, C. M., & Foster, A. E. (2010). Enhanced Tumor Trafficking of GD2 Chimeric Antigen Receptor T Cells by Expression of the 22 Chemokine Receptor CCR2b. Journal of Immunotherapy, 33(8), 780–788. https://doi.org/10.1097/CJI.0b013e3181ee6675 Crump, M., Neelapu, S. S., Farooq, U., Van Den Neste, E., Kuruvilla, J., Westin, J., … Gisselbrecht, C. (2017). Outcomes in refractory diffuse large B-cell lymphoma: Results from the international SCHOLAR-1 study. Blood, 130(16), 1800–1808. https://doi.org/10.1182/blood-2017-03-769620 DeFord-Watts, L. M., Dougall, D. S., Belkaya, S., Johnson, B. A., Eitson, J. L., Roybal, K. T., … van Oers, N. S. C. (2011). The CD3 zeta subunit contains a phosphoinositide-binding motif that is required for the stable accumulation of TCR-CD3 complex at the immunological synapse. Journal of Immunology (Baltimore, Md. : 1950), 186(12), 6839–6847. https://doi.org/10.4049/jimmunol.1002721 Di Stasi, A., De Angelis, B., Rooney, C. M., Zhang, L., Mahendravada, A., Foster, A. E., … Savoldo, B. (2009). T lymphocytes coexpressing CCR4 and a chimeric antigen receptor targeting CD30 have improved homing and antitumor activity in a Hodgkin tumor model. Blood, 113(25), 6392–6402. https://doi.org/10.1182/blood-2009-03-209650 Doudna, J. A., & Charpentier, E. (2014). The new frontier of genome engineering with CRISPR-Cas9. Science. https://doi.org/10.1126/science.1258096 Ebert, L. M., Yu, W., Gargett, T., & Brown, M. P. (2018). Logic-gated approaches to extend the utility of chimeric antigen receptor T-cell technology. Biochemical Society Transactions, BST20170178. https://doi.org/10.1042/BST20170178 Engstad, C. S., Gutteberg, T. J., & Osterud, B. (1997). Modulation of blood cell activation by four commonly used anticoagulants. Thrombosis and Haemostasis, 77(4), 690–696. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9134644 Eyquem, J., Mansilla-Soto, J., Giavridis, T., Van Der Stegen, S. J. C., Hamieh, M., Cunanan, K. M., … Sadelain, M. (2017). Targeting a CAR to the TRAC locus with CRISPR/Cas9 enhances tumour rejection. Nature, 543(7643), 113–117. https://doi.org/10.1038/nature21405 Fesnak, A., Lin, C., Siegel, D. L., & Maus, M. V. (2016). CAR-T Cell Therapies From the Transfusion Medicine Perspective. Transfusion Medicine Reviews, 30(3), 139–145. https://doi.org/10.1016/j.tmrv.2016.03.001 Foster, A. E., Dotti, G., Lu, A., Khalil, M., Brenner, M. K., Heslop, H. E., … Bollard, C. M. (2008). Antitumor activity of EBV-specific T lymphocytes transduced with a dominant negative TGF-beta receptor. Journal of Immunotherapy (Hagerstown, Md. : 1997), 31(5), 500–505. https://doi.org/10.1097/CJI.0b013e318177092b Fu, X., Rivera, A., Tao, L., & Zhang, X. (2013). Genetically modified T cells targeting neovasculature efficiently destroy tumor blood vessels, shrink established solid tumors and increase nanoparticle delivery. International Journal of Cancer, 133(10), 2483–2492. https://doi.org/10.1002/ijc.28269 Ganapathy, V., Thangaraju, M., & Prasad, P. D. (2009). Nutrient transporters in cancer: Relevance to Warburg hypothesis and beyond. Pharmacology and Therapeutics. https://doi.org/10.1016/j.pharmthera.2008.09.005 Gattinoni, L., Lugli, E., Ji, Y., Pos, Z., Paulos, C. M., Quigley, M. F., … Restifo, N. P. (2011). A human memory T cell subset with stem cell-like properties. Nature Medicine, 17(10), 1290–1297. https://doi.org/10.1038/nm.2446 Geiger, R., Rieckmann, J. C., Wolf, T., Basso, C., Feng, Y., Fuhrer, T., … Lanzavecchia, A. (2016). LArginine Modulates T Cell Metabolism and Enhances Survival and Anti-tumor Activity. Cell, 23 167(3), 829–842.e13. https://doi.org/10.1016/j.cell.2016.09.031 Ghassemi, S., Bedoya, F., Nunez-Cruz, S., June, C., Melenhorst, J., & Milone, M. (2016). Shortened T cell culture with IL-7 and IL-15 provides the most potent chimeric antigen receptor (CAR)modified T cells for adoptive immunotherapy. The Journal of Immunology, 196(1 Supplement). Gogol-Döring, A., Ammar, I., Gupta, S., Bunse, M., Miskey, C., Chen, W., … Ivics, Z. (2016). Genomewide Profiling Reveals Remarkable Parallels Between Insertion Site Selection Properties of the MLV Retrovirus and the piggyBac Transposon in Primary Human CD4+ T Cells. YMTHE, 24, 592– 606. https://doi.org/10.1038/mt.2016.11 Golubovskaya, V., & Wu, L. (2016). Different Subsets of T Cells, Memory, Effector Functions, and CART Immunotherapy. Cancers, 8(3), 36. https://doi.org/10.3390/cancers8030036 Harlin, H., Meng, Y., Peterson, A. C., Zha, Y., Tretiakova, M., Slingluff, C., … Gajewski, T. F. (2009). Chemokine expression in melanoma metastases associated with CD8+ T-cell recruitment. Cancer Research, 69(7), 3077–3085. https://doi.org/10.1158/0008-5472.CAN-08-2281 Holohan, D. R., Lee, J. C., & Bluestone, J. A. (2015). Shifting the Evolving CAR T Cell Platform into Higher Gear. Cancer Cell. https://doi.org/10.1016/j.ccell.2015.09.014 Hsu, C., Jones, S. A., Cohen, C. J., Zheng, Z., Kerstann, K., Zhou, J., … Morgan, R. A. (2007). Cytokineindependent growth and clonal expansion of a primary human CD8+T-cell clone following retroviral transduction with the IL-15 gene. Blood, 109(12), 5168–5177. https://doi.org/10.1182/blood-2006-06-029173 Ishida, Y., Agata, Y., Shibahara, K., & Honjo, T. (1992). Induced expression of PD-1, a novel member of the immunoglobulin gene superfamily, upon programmed cell death. The EMBO Journal, 11(11), 3887–3895. https://doi.org/10.1128/MCB.25.21.9543 Ivics, Z. N., Hackett, P. B., Plasterk, R. H., & Izsvá, Z. (1997). Molecular Reconstruction of Sleeping Beauty, a Tc1-like Transposon from Fish, and Its Transposition in Human Cells its original location and promotes its reintegration else- where in the genome (Plasterk, 1996). Autonomous mem- bers of a transposon family can express an active trans- posase, the transacting factor for transposition, and thus are capable of transposing on their own. Nonauton. Cell, 91, 501–510. Retrieved from https://ac.els-cdn.com/S0092867400804365/1-s2.0S0092867400804365-main.pdf?_tid=94222377-b22c-4191-94072ea61271a14b&acdnat=1520844735_d7a734bce509fdfd9fa60f9eb1b88815 Jamal-Hanjani, M., Quezada, S. A., Larkin, J., & Swanton, C. (2015). Translational Implications of Tumor Heterogeneity. Clinical Cancer Research, 21(6), 1258–1266. https://doi.org/10.1158/1078-0432.CCR-14-1429 Janas, M., Nunes, C., Marenghi, A., Sauvage, V., Davis, B., Bajaj, A., & Burns, A. (2015). Perfusion’s role in maintenance of high-density T-cell cultures. BioProcess International, 13(1). Jensen, M. C., & Riddell, S. R. (2014). Design and implementation of adoptive therapy with chimeric antigen receptor-modified T cells. Immunological Reviews, 257(1), 127–144. https://doi.org/10.1111/imr.12139 Juillerat, A., Marechal, A., Filhol, J. M., Valogne, Y., Valton, J., Duclert, A., … Poirot, L. (2017). An oxygen sensitive self-decision making engineered CAR T-cell. Scientific Reports, 7. https://doi.org/10.1038/srep39833 Kakarla, S., & Gottschalk, S. (2014). CAR T cells for solid tumors: armed and ready to go? Cancer Journal (Sudbury, Mass.), 20(2), 151–155. https://doi.org/10.1097/PPO.0000000000000032 24 Kalos, M., Levine, B. L., Porter, D. L., Katz, S., Grupp, S. A., Bagg, A., & June, C. H. (2011). T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Science Translational Medicine, 3(95). https://doi.org/10.1126/scitranslmed.3002842 Kebriaei, P., Huls, H., Ciurea, S., Liu, T., Singh, H., Su, S., … Cooper, L. (2015). Donor-derived, CD19directed, car-modified t cells infused after allogeneic hematopoietic stem cell transplantation as pre-emptive donor lymphocyte infusion in patients with CD19+malignancies. Haematologica, 100(23), 320. Retrieved from http://www.bloodjournal.org/content/126/23/862?ssochecked=true Kisielow, M., Kisielow, J., Capoferri-Sollami, G., & Karjalainen, K. (2005). Expression of lymphocyte activation gene 3 (LAG-3) on B cells is induced by T cells. European Journal of Immunology, 35(7), 2081–2088. https://doi.org/10.1002/eji.200526090 Kloss, C. C., Condomines, M., Cartellieri, M., Bachmann, M., & Sadelain, M. (2012). Combinatorial antigen recognition with balanced signaling promotes selective tumor eradication by engineered T cells. Nature Biotechnology, 31(1). https://doi.org/10.1038/nbt.2459 Kochenderfer, J. N., Somerville, R. P. T., Lu, T., Yang, J. C., Sherry, R. M., Feldman, S. A., … Rosenberg, S. A. (2017). Long-Duration Complete Remissions of Diffuse Large B Cell Lymphoma after AntiCD19 Chimeric Antigen Receptor T Cell Therapy. Molecular Therapy, 25(10), 2245–2253. https://doi.org/10.1016/j.ymthe.2017.07.004 Kreso, A., & Dick, J. E. (2014). Evolution of the cancer stem cell model. Cell Stem Cell. https://doi.org/10.1016/j.stem.2014.02.006 Levine, B. L. (2015). Performance-enhancing drugs: design and production of redirected chimeric antigen receptor (CAR) T cells. Cancer Gene Therapy, 22(2), 79–84. https://doi.org/10.1038/cgt.2015.5 Levine, B. L., Miskin, J., Wonnacott, K., & Keir, C. (2017). Global Manufacturing of CAR T Cell Therapy. Molecular Therapy - Methods and Clinical Development, 4, 92–101. https://doi.org/10.1016/j.omtm.2016.12.006 Ligtenberg, M. A., Mougiakakos, D., Mukhopadhyay, M., Witt, K., Lladser, A., Chmielewski, M., … Kiessling, R. (2016). Coexpressed Catalase Protects Chimeric Antigen Receptor–Redirected T Cells as well as Bystander Cells from Oxidative Stress–Induced Loss of Antitumor Activity. The Journal of Immunology, 196(2), 759–766. https://doi.org/10.4049/jimmunol.1401710 Liu, X., Pu, Y., Cron, K., Deng, L., Kline, J., Frazier, W. A., … Xu, M. M. (2015). CD47 blockade triggers T cell-mediated destruction of immunogenic tumors. Nature Medicine, 21(10), 1209–1215. https://doi.org/10.1038/nm.3931 Long, A. H., Haso, W. M., Shern, J. F., Wanhainen, K. M., Murgai, M., Ingaramo, M., … Mackall, C. L. (2015). 4-1BB costimulation ameliorates T cell exhaustion induced by tonic signaling of chimeric antigen receptors. Nature Medicine, 21(6), 581–590. https://doi.org/10.1038/nm.3838 Marigo, I., Zilio, S., Desantis, G., Mlecnik, B., Agnellini, A. H. R., Ugel, S., … Bronte, V. (2016). T Cell Cancer Therapy Requires CD40-CD40L Activation of Tumor Necrosis Factor and Inducible NitricOxide-Synthase-Producing Dendritic Cells. Cancer Cell, 30(3), 377–390. https://doi.org/10.1016/j.ccell.2016.08.004 Maude, S., & Barrett, D. M. (2016). Current status of chimeric antigen receptor therapy for haematological malignancies. British Journal of Haematology, 172(1), 11–22. https://doi.org/10.1111/bjh.13792 25 Maude, S. L., Laetsch, T. W., Buechner, J., Rives, S., Boyer, M., Bittencourt, H., … Grupp, S. A. (2018). Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. New England Journal of Medicine, 378(5), 439–448. https://doi.org/10.1056/NEJMoa1709866 McFarland, D. C., Zhang, C., Thomas, H. C., & T L, R. (2006). Confounding effects of platelets on flow cytometric analysis and cell-sorting experiments using blood-derived cells. Cytometry. Part A : The Journal of the International Society for Analytical Cytology, 69(2), 86–94. https://doi.org/10.1002/cyto.a.20207 Minagawa, K., Jamil, M. O., AL-Obaidi, M., Pereboeva, L., Salzman, D., Erba, H. P., … Di Stasi, A. (2016). In Vitro Pre-Clinical Validation of Suicide Gene Modified Anti-CD33 Redirected Chimeric Antigen Receptor T-Cells for Acute Myeloid Leukemia. PLOS ONE, 11(12), e0166891. https://doi.org/10.1371/journal.pone.0166891 Myers, D. R., Zikherman, J., & Roose, J. P. (2017). Tonic Signals: Why Do Lymphocytes Bother? https://doi.org/10.1016/j.it.2017.06.010 Neelapu, S. S., Locke, F. L., Bartlett, N. L., Lekakis, L. J., Miklos, D. B., Jacobson, C. A., … Go, W. Y. (2017). Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. New England Journal of Medicine, NEJMoa1707447. https://doi.org/10.1056/NEJMoa1707447 Ninomiya, S., Narala, N., Huye, L., Yagyu, S., Savoldo, B., Dotti, G., … Ramos, C. A. (2015). Tumor indoleamine 2,3-dioxygenase (IDO) inhibits CD19-CAR T cells and is downregulated by lymphodepleting drugs. Blood, 125(25), 3905–3916. https://doi.org/10.1182/blood-2015-01621474 Nishio, N., & Dotti, G. (2015). Oncolytic virus expressing RANTES and IL-15 enhances function of CARmodified T cells in solid tumors. OncoImmunology, 4(2), 1–3. https://doi.org/10.4161/21505594.2014.988098 Oldenborg, P. A., Zheleznyak, A., Fang, Y. F., Lagenaur, C. F., Gresham, H. D., & Lindberg, F. P. (2000). Role of CD47 as a marker of self on red blood cells. Science, 288(5473), 2051–2054. https://doi.org/10.1126/science.288.5473.2051 Osborn, M. J., Webber, B. R., Knipping, F., Lonetree, C., Tennis, N., DeFeo, A. P., … Blazar, B. R. (2016). Evaluation of TCR Gene Editing Achieved by TALENs, CRISPR/Cas9, and megaTAL Nucleases. Molecular Therapy, 24(3), 570–581. https://doi.org/10.1038/MT.2015.197 Perales, M.-A., Kebriaei, P., Kean, L. S., & Sadelain, M. (2018). Reprint of: Building a Safer and Faster CAR: Seatbelts, Airbags, and CRISPR. Biology of Blood and Marrow Transplantation : Journal of the American Society for Blood and Marrow Transplantation, 24(3S), S15–S19. https://doi.org/10.1016/j.bbmt.2017.12.789 Prosser, M. E., Brown, C. E., Shami, A. F., Forman, S. J., & Jensen, M. C. (2012). Tumor PD-L1 costimulates primary human CD8+ cytotoxic T cells modified to express a PD1: CD28 chimeric receptor. Molecular Immunology, 51(3–4), 263–272. https://doi.org/10.1016/j.molimm.2012.03.023 Ptáčková, P., Musil, J., Štach, M., Lesný, P., Němečková, Š., Král, V., … Otáhal, P. (2018, February). A new approach to CAR T-cell gene engineering and cultivation using piggyBac transposon in the presence of IL-4, IL-7 and IL-21. Cytotherapy. https://doi.org/10.1016/j.jcyt.2017.10.001 Ramello, M. C., Haura, E. B., & Abate-Daga, D. (2018). CAR-T cells and combination therapies: What’s next in the immunotherapy revolution? Pharmacological Research, 129, 194–203. https://doi.org/10.1016/J.PHRS.2017.11.035 Randolph, T. R. (2004). Advances in acute lymphoblastic leukemia. Clinical Laboratory Science : 26 Journal of the American Society for Medical Technology, 17(4), 235–245. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15559730 Riviere, I., & Sadelain, M. (2017). Chimeric Antigen Receptors: A Cell and Gene Therapy Perspective. Molecular Therapy : The Journal of the American Society of Gene Therapy, 25(5), 1117–1124. https://doi.org/10.1016/j.ymthe.2017.03.034 Rivière, I., & Sadelain, M. (2017). Chimeric Antigen Receptors: A Cell and Gene Therapy Perspective. https://doi.org/10.1016/j.ymthe.2017.03.034 Roybal, K. T., & Lim, W. A. (2017). Synthetic Immunology: Hacking Immune Cells to Expand Their Therapeutic Capabilities INTRODUCTION: IMMUNE CELLS ARE AN IDEAL PLATFORM FOR INTERFACING WITH DISEASE. Annu. Rev. Immunol, 35, 229–253. https://doi.org/10.1146/annurev-immunol Sadeghi, A., Pauler, L., Annerén, C., Friberg, A., Brandhorst, D., Korsgren, O., & Tötterman, T. H. (2011). Large-scale bioreactor expansion of tumor-infiltrating lymphocytes. Journal of Immunological Methods, 364(1–2), 94–100. https://doi.org/10.1016/j.jim.2010.11.007 Savoldo, B., Ramos, C. A., Liu, E., Mims, M. P., Keating, M. J., Carrum, G., … Dotti, G. (2011). CD28 costimulation improves expansion and persistence of chimeric antigen receptor-modified T cells in lymphoma patients. Journal of Clinical Investigation, 121(5), 1822–1826. https://doi.org/10.1172/JCI46110 Scheffel, M. J., Scurti, G., Simms, P., Garrett-Mayer, E., Mehrotra, S., Nishimura, M. I., & VoelkelJohnson, C. (2016). Efficacy of adoptive T-cell therapy isimproved by treatment with the antioxidant N-acetyl cysteine, which limits activation-induced T-cell death. Cancer Research, 76(20), 6006–6016. https://doi.org/10.1158/0008-5472.CAN-16-0587 Schubert, M. L., Hoffmann, J. M., Dreger, P., Müller-Tidow, C., & Schmitt, M. (2017). Chimeric antigen receptor transduced T cells: Tuning up for the next generation. International Journal of Cancer. https://doi.org/10.1002/ijc.31147 Schuberth, P. C., Hagedorn, C., Jensen, S. M., Gulati, P., van den Broek, M., Mischo, A., … Petrausch, U. (2013). Treatment of malignant pleural mesothelioma by fibroblast activation proteinspecific re-directed T cells. Journal of Translational Medicine, 11(1), 1–11. https://doi.org/10.1186/1479-5876-11-187 Shedlock, D. J., & Shen, H. (2003). Requirement for CD4 T cell help in generating functional CD8 T cell memory. Science (New York, N.Y.), 300(5617), 337–339. https://doi.org/10.1126/science.1082305 Shi, L., Meng, T., Zhao, Z., Han, J., Zhang, W., Gao, F., & Cai, J. (2017). CRISPR knock out CTLA-4 enhances the anti-tumor activity of cytotoxic T lymphocytes. Gene, 636, 36–41. https://doi.org/10.1016/j.gene.2017.09.010 Singh, H., Figliola, M. J., Dawson, M. J., Huls, H., Olivares, S., Switzer, K., … Cooper, L. J. N. (2011). Reprogramming CD19-specific T cells with IL-21 signaling can improve adoptive immunotherapy of B-lineage malignancies. Cancer Research, 71(10), 3516–3527. https://doi.org/10.1158/00085472.CAN-10-3843 Smith, T. T., Stephan, S. B., Moffett, H. F., McKnight, L. E., Ji, W., Reiman, D., … Stephan, M. T. (2017). In situ programming of leukaemia-specific T cells using synthetic DNA nanocarriers. Nature Nanotechnology. https://doi.org/10.1038/nnano.2017.57 Su, S., Hu, B., Shao, J., Shen, B., Du, J., Du, Y., … Liu, B. (2016). CRISPR-Cas9 mediated efficient PD-1 disruption on human primary T cells from cancer patients. Scientific Reports, 6. 27 https://doi.org/10.1038/srep20070 Tang, X.-J., Sun, X.-Y., Huang, K.-M., Zhang, L., Yang, Z.-S., Zou, D.-D., … Luo, J. (2015). Therapeutic potential of CAR-T cell-derived exosomes: a cell-free modality for targeted cancer therapy. Oncotarget, 6(42), 44179–44190. https://doi.org/10.18632/oncotarget.6175 Tedder, T. F., & Isaacs, C. M. (1989). Isolation of cDNAs encoding the CD19 antigen of human and mouse B lymphocytes. A new member of the immunoglobulin superfamily. The Journal of Immunology, 143(2), 712–717. Retrieved from http://www.jimmunol.org/content/143/2/712.abstract Till, B. G., Jensen, M. C., Wang, J., Chen, E. Y., Wood, B. L., Greisman, H. A., … Press, O. W. (2008). Adoptive immunotherapy for indolent non-Hodgkin lymphoma and mantle cell lymphoma using genetically modified autologous CD20-specific T cells. Blood, 112(6), 2261–2271. https://doi.org/10.1182/blood-2007-12-128843 Tumaini, B., Lee, D. W., Lin, T., Castiello, L., Stroncek, D. F., Mackall, C., … Sabatino, M. (2013). Simplified process for the production of anti-CD19-CAR-engineered T cells. Cytotherapy, 15(11), 1406–1415. https://doi.org/10.1016/j.jcyt.2013.06.003 Vera, J. F., Hoyos, V., Savoldo, B., Quintarelli, C., Giordano Attianese, G. M. P., Leen, A. M., … Dotti, G. (2009). Genetic manipulation of tumor-specific cytotoxic T lymphocytes to restore responsiveness to IL-7. Molecular Therapy, 17(5), 880–888. https://doi.org/10.1038/mt.2009.34 Vormittag, P., Gunn, R., Ghorashian, S., & Veraitch, F. S. (2018). A guide to manufacturing CAR T cell therapies. Current Opinion in Biotechnology, 53, 164–181. https://doi.org/10.1016/j.copbio.2018.01.025 Wang, L., Rubinstein, R., Lines, J. L., Wasiuk, A., Ahonen, C., Guo, Y., … Noelle, R. J. (2011). VISTA, a novel mouse Ig superfamily ligand that negatively regulates T cell responses. The Journal of Experimental Medicine, 208(3), 577–592. https://doi.org/10.1084/jem.20100619 Wiehagen, K. R., Corbo, E., Schmidt, M., Shin, H., Wherry, E. J., & Maltzman, J. S. (2010). Loss of tonic T-cell receptor signals alters the generation but not the persistence of CD8+ memory T cells. Blood, 116(25), 5560–5570. https://doi.org/10.1182/BLOOD-2010-06-292458 Xu, X.-J., & Tang, Y.-M. (2014). Cytokine release syndrome in cancer immunotherapy with chimeric antigen receptor engineered T cells. Cancer Letters, 343(2), 172–178. https://doi.org/10.1016/j.canlet.2013.10.004 Zhang, E., Gu, J., & Xu, H. (2018). Prospects for chimeric antigen receptor-modified T cell therapy for solid tumors. Molecular Cancer, 17(1). https://doi.org/10.1186/s12943-018-0759-3 Zhang, L., Kerkar, S. P., Yu, Z., Zheng, Z., Yang, S., Restifo, N. P., … Morgan, R. A. (2011). Improving adoptive T cell therapy by targeting and controlling IL-12 expression to the tumor environment. Molecular Therapy, 19(4), 751–759. https://doi.org/10.1038/mt.2010.313 Zhu, C., Anderson, A. C., Schubart, A., Xiong, H., Imitola, J., Khoury, S. J., … Kuchroo, V. K. (2005). The Tim-3 ligand galectin-9 negatively regulates T helper type 1 immunity. Nature Immunology, 6(12), 1245–1252. https://doi.org/10.1038/ni1271 28
 0
0
advertisement
Related documents

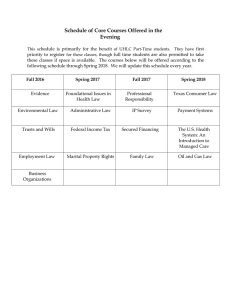
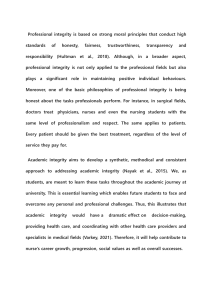
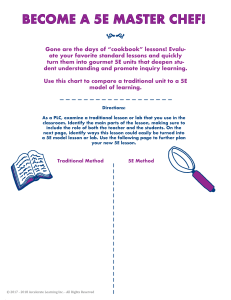



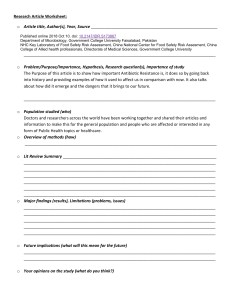
Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users