-1")
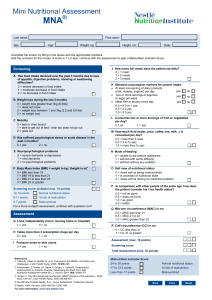
N421: Holistic Gerontological Nursing THE GASTROINTESTINAL SYSTEM Learning Objectives Describe age-related changes that affect gastrointestinal function and nutrition. Evaluate physiological, emotional, social, and economic factors related to nutrition. Discuss holistic nutritional assessment of the older adult. Develop appropriate pharmacologic and nonpharmacologic nursing interventions to improve health and function of the older person with gastrointestinal problems. Introduction The gastrointestinal (GI) tract is responsible for four major functions relating to food ingestion: Digestion Absorption Secretion Motility Impact of ARCs on Nutrition Decreased thirst and hunger drive Decreased intake Decreased caloric needs Decreased protein levels Increased risk for aspiration, dehydration, & constipation Nutritional vitamin deficiencies Psychosocial Influences on Nutrition Social Psychological Isolation Depression Loneliness Anxiety Poverty Dementia Dependency Bereavement Impact of Chronic Conditions & Medications Respiratory disease- decreased intake Digoxin- decreased intake Alcohol & Antacids- decreased absorption Anticholinergics- increased dry mouth & decreased intake ACE Inhibitors- increased dry mouth, altered taste Nutritional Assessment Parameters Nutritional risk screening should be a part of the CGA A comprehensive nutritional assessment reviews: Anthropometrics Laboratory Values Nursing Assessment Nutritional History Anthropometrics Serial body weights Assess over time for changes 5% change over 1 month or 10% change over 6 months- clinically significant BMI- 19-25 is normal Not reliable in older adults Improved health outcomes with BMI 26-28 Triceps skinfold, mid-upper arm or calf circumference, Lab Values and Malnutrition Serum Albumin- 3.5 – 5.5g/dl, < 3.0 malnutrition Serum prealbumin- 15-35mg/dL, < 11 mg/dl Transferrin- 170-370 mg/dl, <100 Protein energy malnutrition Cholesterol < 150 mg/dl Decreased leptin levels associated with malnutrition Blood counts used to assess for anemias Labs for vitamin deficiencies Nursing Assessment Observe food intake Functional assessment Oral Assessment Sores, infections, issues with teeth, dentures, swallowing Abdominal assessment Changes in bowels Pain Mental Health Screening ***Medication Review*** Access to food & food preparation Nutritional Assessment Mini Nutritional Assessment A simple and reliable tool An 18-item questionnaire that takes 10 to 15 minutes to administer. A score between 8 and 11 indicates an increased risk for malnutrition, and a score <7 reflects malnutrition. Questions examine food intake, weight loss, body mass index, psychological stress/acute disease incidence, neuropsychological problems, and mobility. 24 hour recall Food Journal/Diary Concerns Related to GI Nutritional Deficiencies Malnutrition/ Anorexia of aging Dehydration Oral Care Dysphagia Constipation Health Promotion & Prevention: Nutritional Needs Decreased absorption of Vitamin D, B12, Calcium, iron, copper, zinc, fatty acids, & cholesterol Supplementation used to treat symptomatic deficiency (Vit. D, B12, and Calcium) Vitamin D Risk factors: limited sun exposure, decrease dairy intake, steroid use <70 – 600IU >70 – 800IU Nutritional Needs Calcium Risk Factors: decreased intake, increased caffeine consumption > 50- 1200mg Vitamin B12 Risk factors: decreased absorption due to ARCs, use of antacids, alcohol abuse Eat fortified foods Be aware of symptoms, folic acid supplementation can mask Vit B12 deficiency 2.4 mcg Protein Needs Essential amino acids (EAAs)most important factor for protein synthesis Aged muscles have reduced response to low doses of EAAs Require higher levels of EAAs and protein intake 1.0-1.2g/kg/day Increased protein intake has shown to maintain muscle mass and decrease sarcopenia Lean meats, soybeans, peanuts, lentils Supplement Savvy 70% of older adults take a dietary supplement Food is always preferred to supplements Increased risk of drug interactions, must tell provider Supplements are not FDA regulated Vitamin E can interact with coagulants Fat soluble vitamins- toxic at large doses Malnutrition/Anorexia of Aging Malnutrition prevalence Community 15% Nursing homes 30-85% Sarcopenia Cachexia Metabolic process Loss of fat and muscle Anorexia Severe wasting https://www.agingresearch.org/ Assessment & Interventions Assessment: Comprehensive Nutritional Assessment Assess oral cavity, abdomen Lab work Rule out other conditions Medication Review Interventions: Small frequent meals Liquid supplements are NOT meal replacements Should be provided at least 1 hour prior or after meals Incorporate preferences and provide choice Further testing, EGD, colonoscopy Enhanced eating environment Assess patient food preferences Improve taste perception, nutrient density, and feeding assistance Health Promotion & Prevention: Dehydration More susceptible Decreased thirst response Decreased total body fluid Decline in kidney function Risk Factors: Age > 85, people of color at higher risk Problems accessing water, increased dependency Cognitive disorders Dysphagia Vomiting, diarrhea Assessment Skin turgor- not reliable Cracks or furrows in tongue Lab Values: Serum Na > 150 BUN/Creatinine ratio: ≥ 25:1 Interventions: Dehydration Health Promotion & Prevention: Oral Care Use of dental services is the lowest of all adults Barriers to oral/dental care Limited Medicare/Medicaid funding Tooth loss seen as normal aging Increased risk for dental carries Lifelong regular dental care Brush and floss 2x per day Rinse mouth daily Clean gums and dentures Healthy nutrition Xerostomia- dry mouth Common problem that negatively impacts nutrition Results in difficulty forming a food bolus and swallowing, decreases ability to taste food Often cased by medication in older adults Treatment Maintain hydration Sugar free candies or gum, xylitol Saliva substitute Dysphagia Dysphagia – is defined as difficulty in any part of the process involved with swallowing solid foods or liquids. Swallowing involves approximately 50 muscles 60% of those in long term care have symptoms of dysphagia. Risk Factors: PD, AD, and stroke Frailty Early detection is vital Dysphagia Diagnosis Swallowing evaluation and diet recommendations made by ST Risk for aspiration, malnutrition Aspiration Precautions Health Promotion & Prevention: Constipation Increased risk due to ARCs Interventions: Constipation Dietary changes Fiber intake 20-35g of fiber per day Increase fluid intake Avoid use of laxatives (assess for misuse) Increase activity Bulk forming agents should be used only if adequate fluid intake AntibioticAssociated Colitis and Diarrhea (p. 546) Risk Factors: • Older adults in hospital or LTC • Recent Antibiotic use, surgery • PPI use Signs & Symptoms: • Mild to severe diarrhea, colitis • Watery diarrhea, possibly bloody • Lower abdominal pain, cramping • Symptoms may occur up to 10 weeks after abx Clostridioides Difficile Increased risk for dehydration, hypotension, colonic perforation, and skin impairment Diagnosis: stool culture Two negative specimens required to rule out C. Diff • Metronidazole 500mg po 4x a day, 10-14 days • • Effective in mild to moderate cases Less expensive, drug of choice • Refractory cases, much more expensive • Vancomycin 125mg po 4x a day, 10-14 days • • • • • • If fever is present, usually resolves within 24 hours Diarrhea decreases over 4-5 days Antidiarrheal medications should not be used Prevent dehydration Prevent skin breakdown Fecal transplant GI review Identify normal aging changes of GI tract What are the nutritional risks and needs of older adults? Ways to prevent nutritional deficiencies and malnutrition. How can the nurse manage dysphagia to prevent aspiration, constipation, and dehydration? What nursing management is required to care for an older adult with C. Diff?