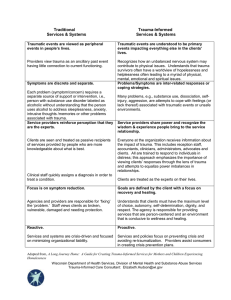
1 Childhood Trauma LO3 NRSG 243 CHILDREN AND ADOLESCENTS J MITCHELL ADAPTED BY T NELSON ADAPTED BY D MCCRAE (2021) ADAPTED BY E DYCK (2022) Stress VS Trauma What is the difference between stress and trauma? 2 Stress Vs. Trauma Stressful event: Not as extreme May not lead to mental health disorders Stress is not always traumatic Stress is part of the human condition 3 Stress Vs. Trauma Cont. Traumatic event: Traumatic experiences are stressful An impairment of some kind following a life-threatening event It can be a direct threat, witnessed or potential threat It can lead to acute stress disorder, posttraumatic stress disorder (PTSD) 4 Traumatic Stress Is not an expected consequence of a stressful event It is connected to how the individual processes and perceives the event, and the available resources to help them cope. Mental health professionals must be careful not to imply trauma even if the event were traumatizing to us. 5 Traumatic Stress Is now a separate diagnostic domain in the DSM-5. Now DSM-5 trauma and stressor related disorders include reactive attachment disorder, acute stress disorder, adjustment disorders, PTSD, disinhibited social engagement disorder. 6 Trauma Related Diagnosis 7 Trauma and Stress Disorders: • • • • • Acute Stress Disorder - extreme stress symptoms Adjustment Disorder - emotional/behavioral symptoms in response to stressor(s) Posttraumatic Stress Disorder - extreme stressor. Disinhibited Social Engagement Disorder - A form of inappropriate attachment, these children typically lack the ability to develop deep, meaningful connections with others and demonstrate inappropriate behaviours with unfamiliar individuals. Reactive Attachment Disorder – withdrawn behavior, inappropriate attachment (do not form a secure attachment with their caregivers), and typically have difficulty managing their emotions. Sources of Trauma Events Causing Trauma(not an exhaustive list) Maltreatment: Neglect (educational, physical, and emotional) Physical abuse Psychological abuse Sexual abuse Witnessing violence Disasters (earthquakes, storms, fires) Accidents Loss Intergenerational trauma (residential schools, 60’s scoop) 8 Complex Trauma Complex trauma is: “Repeated exposure to traumatic events, often of an invasive, interpersonal nature, and longterm impact of this exposure.” 8 Complex Trauma Cont. Initial traumatic experiences (parental abuse, witnessing domestic violence) may result in: Emotional dysregulation; Loss of a safe base, loss of direction; And, inability to respond to danger cues often lead to subsequent trauma exposure (sexual abuse) 10 Complex Trauma in Children The DSM-5 classification does not capture the full range of difficulties and challenges that traumatized children often experience. PTSD diagnosis is often used; however this does not capture the extentTreatment often focuses on addressing behaviours such as with conduct disorder, which does not represent the whole picture of the child’s experience. 11 Seven Primary Domains of Impairment 12 These domains include: Attachment Biology Affect regulation Dissociation Behavioral regulation Cognition Self-concept Please see Table 1 - Complex Trauma in Children and Adolescents. (Link in course manual under LO3 under reading assignment) Complex trauma in Children - Domains Attachment - distrust and suspiciousness, social isolation Biology - hypersensitivity to physical contact, somatization (sometime conversion disorder) Affect regulation - difficulty describing feelings and internal experience, difficulty regulating outward emotional response to stress Dissociation - failure to integrate information, depersonalization, amnesia, distinct alterations in consciousness 13 Domains of Impairment Cont. Behavioral Control - self-destructive behavior, aggressive tendencies, eating disorders, substance abuse, trauma reenactment in play Cognition - learning difficulties, problems with language development, difficulty with focusing, fear of abandonment or object constancy Self-concept - shame, guilt, low selfesteem, body image disturbance 14 Complex Trauma and Children/Adolescents Affect dysregulation, impaired academic performance, difficulty with interpersonal relationships, low self-esteem, high risk behavior, and symptoms of PTSD Developmentally, children have egocentric views - may express feelings of guilt and personal responsibility for the traumatic events. I.e. “It’s my fault, I am damaged.” 15 Traumatic Childhood Experiences A significant risk factor for the development of later onset psychopathology, and major increases in health risks and physical illness as adults. PTSD is often times comorbid with other disorders such as mood, anxiety or substance use disorders. Children usually meet oppositional defiant disorder or separation anxiety disorder diagnosis criteria (APA, 2013). 16 Other Common Issues: Other common issues with abused and neglected children: • Depression • Attention Deficit Hyperactivity Disorder • Self-Harm • Substance Abuse Disorders • Eating Disorders • Conduct Disorders 17 Importance of Attachment Attachment: Early caregiver relationship provides a relational context. Children develop their earliest model of self, other and self in relation to others. 18 Insecure Attachment Failure to create a safe, dyadic relationship may leave an environment of vulnerability allowing for the occurrence of complex trauma exposure. Insecure or anxious attachments may be further compounded if children perceive their caretaker as too distressed to deal with the experience 19 Attachment Cont. Children with insecure attachment patterns may be classified as avoidant, ambivalent or disorganized. Avoidant attachment style children may learn to distrust their emotions, relationships, and even their own bodies due to caregivers rejecting them. 20 Attachment Styles Cont. Ambivalent Attachment patterns - these children cope by disconnection to important adults that reject or overly engage due to the mixed messages from their caregivers of validation and invalidation. Disorganized attachment style - erratic behavior in young children; excessively clingy, aggressive. 21 Disorganized AttachmentAdolescents/Adults This presents as helplessness such as abandonment, betrayal, or any expression of anger. Children living with unpredictable violence and repeated abandonment often fail to develop appropriate language and verbal processing abilities. 22 Cont. Disorganized attachment has been hypothesized to interfere with development of neural connections in critical brain areas (Schore, 2001). This attachment style may result in impairment in stress management, empathy, affect regulation, prosocial concern for others, use of language to solve relational problems, and further lead to personality disorders (Herman, Perry,& van der Kolk, 1989; Main, 1995). 23 Impaired Attachment • Extreme high or low levels of stimulation such as stress are thought to trigger adaptive adjustments in the brain • Toddlerhood and early childhood • Middle childhood • Traumatized youth frequently suffer from body dysregulation, meaning they over-respond or under-respond to sensory stimuli. 24 Children and Traumatic Stress Data suggests children exposed to physical & sexual abuse in first 5 yrs of life are more likely to suffer symptoms of anxiety and depression with HPA axis dysregulation. Research suggesting atrophy of the brain’s hippocampus in the limbic system or emotional brain in adults who were abused as children. Also, initial cortisol increases upon exposure to trauma become disapated or reduced with chronic stress exposure. 25 Developmental Psychopathology Is the interplay of biological, social-contextual and psychological aspects of normal and abnormal development across the life span. (Recommended Video – Dr. Emily Taylor Developmental Psychopathology) 26 Developmental Psychopathy Impairments 27 with Complex Trauma Cognitive: • Confusion • Distorted thinking • Memory Disturbances • Trouble problem solving • Language deficits • Abstract thinking deficits • Time disorientation Behavioral: • Immature • Withdrawn • Violent • Impulsive • Engage in criminal activities • Engage in risk taking activities • Self-harm Affective: • Loss of identity • Troubles trusting others • Insecurity, inferiority, fear, shame, and guilt • Sense of isolation • Inability to derive pleasure • Troubles forming healthy relationships • Guarded Self-Concept: • Disturb body image • Low self-esteem • Loss of identity Family’s Role in Overcoming Trauma 28 Family plays a role in determining how the child adapts to the trauma experience. Factors influencing the child’s response: • The extent that the family was involved in the trauma • The parental response to the traumatic event or disclosure • The extent that the parent themselves are influenced by their own childhood histories of loss and trauma • Parental psychopathology Understanding the Survivor • Focus on the complete child’s experience/developmental stage and not just the problem. • Understanding the child also includes understanding the family, social and community contexts. • Understand from the child’s perspective. • Seek to understand and assess trauma from a cultural context that includes the ethnic background, community, language, & spirituality. 29 Trauma Informed Care 1. Begins with providing safety both physically and emotionally to the traumatized child. 2. Screening and assessment. 3. Understanding of the trauma experience. 4. Child abuse must be reported. Services: Inpatient Services Case Management Addiction & Mental Health Services Housing Residential Services 30 Trauma Informed care Service providers routinely screen for trauma exposure and related symptoms Use evidence-based, culturally responsive assessments and treatments for traumatic stress and associated mental health symptoms Make resources available to children, and their families Engage in efforts to strengthen the resilience and protective factors of children and families impacted by and vulnerable to trauma Address parent and caregiver trauma and the impact on the family system (NCTSN, 2014). 31 Standards for Trauma Care (National Child Traumatic Stress Network) 31 Assessment Comprehensive assessment including developmental hx, family hx, trauma hx. Clinical interviews with child/adolescent, primary caretakers, and other collateral information as appropriate from pediatrician, teacher, child protection, any previous therapists. The use of standardized assessment instruments. 33 Interventions Should focus on two levels: 1. The individual level, with particular attention to issues of arousal and self-regulation. 2. The large social-environment level, so that conditions that produce or sustain maladaptive traumatic reactions are alleviated. 34 Interventions 35 Six Core Components of Complex Trauma Intervention: 1. 2. 3. 4. 5. 6. Safety: From harm. Self-regulation: Restore equilibrium. Self-reflective information processing: Engage in reflection. Traumatic experiences integration: The resolution of traumatic memories, through therapeutic strategies as meaning-making. Relational engagement: form healthy relationship skills. Positive affect enhancement: having self-worth. Central Goals in Interventions with Youth Safety – In ones home, school, environment Skills development – in emotion regulation and interpersonal functioning (trigger identification) Meaning making – about past traumatic events so that youth can consider more positive adaptive views and experience hope Enhancing resiliency and integration into social network 36 Successful Adaptation The youth is able to change/adapt on a variety of levels: • • • • • • • Physiological state Reactivity Coping skills Behavioral patterns Relating Problem solving Value 37 Recovery - Resilience ‘Resilience’ and ‘recovery’ are related but distinct concepts. Do you know the difference between the two? https://onlinelibrary.wiley.com/doi/epdf/1 0.1111/jpm.12048 38 Develop Resilience Resilience is the ability of an individual to withstand adversity and move forward. Foster resiliency with: Developing a therapeutic relationship Strength-based approach, self-compassion Teach healthy coping skills, communication skills, problem-solving skills Positive connections with supportive adults and community 39 Risk factors Risk factors for each individual are unique (see Table 8 – 1 p. 117) Individual? Family? Community? Risk factors can change in response to a new developmental stage. Protective factors are individual, family, and environmental variables that buffer the effect of risk factors and can decrease the severity of a mental disorder. 40 Protective factors Internal protective factors: Positivity Good health High stress tolerance Flexibility Spirituality Effective coping strategies External protective factors: Supportive family, social and community relationships Recreation Economic resources 41 Cognitive Behaviour Therapy [CBT] CBT - Is a combination of psycho-education, stress inoculation, and relaxation training. - Helps teach the child to put feelings into words. - Helps the child understand how they have been effected and move on. - Helps to separate thoughts, feelings, and behaviours. - Helps them to replace negative thoughts with positive thoughts. - Create a plan. 42 Healing Process How can we help a child/youth heal from trauma? With toddlers, parental attunement is the primary goal of treatment due to healthy attachment being critical for healthy development. LS5 - Problems to Component Grid(PCG) pp.41-44 provides many interventions most relevant to symptoms. 43 Interventions Play therapy for children to allow expression of trauma Sandbox and Art therapy Body oriented treatments to help children change their physiological response to threatening stimuli Social skills group therapy Family Therapy Animal therapy Pharmacological (SSRIs) combined with specific trauma treatment and not in place of it. 44 Trauma Videos Trauma Informed Counselling: https://www.bing.com/videos/search?q=trauma+informed+counseling +children+youtube+vdeo&&view=detail&mid=9DEA733C7C263BF8410 F9DEA733C7C263BF8410F&&FORM=VDRVRV Child’s Response to Trauma: 45 http://www.youtube.com/watch?v=a497RNcxTQg Prevalence video: http://www.youtube.com/watch?v=A1vbSSQJOHw THE END!