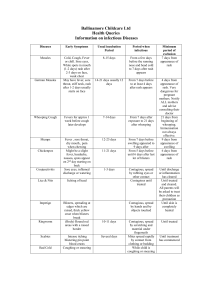
THE CHILD WITH AN INFECTIOUS DISEASE Viral Exanthems Rubeola (Measles) Causative agent Manifestations Complications Management RNA Virus 3-5 days before the appearance of the rash to 4-6 days after appearance of the rash RNA Virus 14- 21 Days Ranges from 7 days before onset of symptoms to 14 days after appearance of the rash Secondary infections such as otitis media, bronchopneumonia, and laryngotracheobronchitis, and myocarditis and pericarditis, can cause premature birth and miscarriage in pregnant women. Most common are arthritis and arthralgia occur more often in adult women than in children or adolescents. Mild thrombocytopenia may also occur a rare complication is Encephalitis Symptomatic, require airborne isolation precaustions. (MMR) and varicella vaccine. Rubella (German Measles, 3-day Measles) Prodrome period with fever that rises gradually and the three “Cs” Coryza, Cough, and Conjunctivitis last 2-4 days Koplik spots 1-4 days before rash last 6-7 days A rash begins on face, neck, and scalp and spreads downward to entire body; fades on face as it spreads to trunk. Pinkish, maculopapular rash, reddish, pinpoint petechial may occur on soft palate Erythema Infectiosum (Fifth disease, Parvovirus B19) Parvovirus B19 4-17 days but can be up to 28 days shedding of virus occurs between days 5 and 12 of the infection Because the disease is mild, complications are not usually reported. Patients with sickle cell disease or beta thalassemia are at risk for anemia and aplastic crisis. Roseola Infantum (Exanthema subitum 3-day fever) Human Herpesvirus 6 (HHV-6) Incubation period 5 – 15 days. Contact transmission (saliva, cerebrospinal fluid) Airborne particles, respiratory droplets, blood, and transplacental transmission fiery red, edematous rash on the cheeks “slapped cheek” appearance rash that comes and goes. Nonspecific symptoms such as headache, runny nose, malaise, and mild fever. Erythematous, maculopapular rash appears on Sudden onset high fever 103 F to 106 F, malaise, and irritability, mild cough, runny nose, abdominal pain, headache, vomiting, and diarrhea. Rash consist of rose-pink maculopapular or macules that blanch with pressure on the neck and trunk may be surrounded by a whitish ring. Febrile seizures Supportive and symptomatic the disease is self-limiting with resolution within 5 days. Exclusion of affected children from other child is 7 days after the rash begins. Considered contagious until age 1 year or nasopharyngeal and urine cultures for the rubella virus are repeatedly negative. Adm. Rubella vaccine in combination with measles and mumps vaccine. (MMR) Treatment is symptomatic and supportive. Treatment is symptomatic Viral Exanthema Causative agent Mumps Paramyxovirus, single-stranded RNA Prodromal manifestations include fever, myalgia, headache, and malaise. Classic clinical sign of parotid glandular swelling and fever. Manifestations Complications Management Most common complication is aseptic meningitis, with the virus identified in the CSF, Signs of CNS involvement include nuchal rigidity, lethargy, and vomiting. A less common CNS complication is meningoenchalomyelitis manifested by fever, headache, nausea, vomiting, nuchal rigidity, and changes in sensorium The potential complication of most concern to parents is orchitis (inflammation of a testis). Seen in adolescent boys and almost never before puberty, Can cause sensorineural hearing impairment. Rare exanthems and hepatitis. Most serious complications involve the pulmonary, neurologic, and hematopoietic systems. The risk of splenic rupture, Swelling of the pharynx and tonsils can be severe enough to compromise respirations. Avoidance of acidic foods such as orange juice is helpful. Droplet precaution are indicated until 9 days after the onset of the parotid swelling. Absolute avoidance of any form of aspirin. Orchitis requires bed rest, intermittent application of ice packs, pain management, emotional support, and diversional activities. Epstein-Bar Virus (Infectious Mononucleosis) Epstein-Barr virus (EBV, a herpes-like virus) doublestranded DNA Most common in older children and young adults with the highest prevalence in 15-19 year-olds. Fever exudative pharyngitis, lymphadenopathy (cervical, axillary and inguinal), hepatosplenomegaly. Some develop a maculopapular rash, after treatment with an amino penicillin antibiotic. Children may report malaise, headache, fatigue, nausea, and abdominal pain. Bacterial Infections Causative agent Scarlet Fever Group A Betahemolytic streptococci Manifestations Complications Management Abrupt fever, vomiting, headache, abdominal pain, pharyngitis, and chills characterize the onset. Within 24 hours, a fine red popular rash appears in the axillae, groin, and neck, which feels like sandpaper to the touch. By the fourth Result from extension of the streptococcal infection. Sinusitis, otitis media, mastoiditis, peritonsillar abscess, bronchopneumonia, meningitis, osteomyelitis, rheumatic fever, and glomerulonephritis Rapid streptococcal screening in an office setting. The preferred treatment for any streptococcal infection is penicillin. Children allergic to penicillin can be given erythromycin a cephalosporin. Supportive, Use of steroids to treat acute tonsillar swelling and other symptoms of infectious mononucleosis is effective in managing inflammation. Pertussis (Whooping Cough) Bordetella pertussis (a gramnegative bacillus) day the papillae slough off, leaving a red, swollen tongue the tonsils are edematous and may be covered with a gray-white exudate, petechial hemorrhages cover the soft palate. The three stages of pertussis are catarrhal, paroxysmal, and convalescent, lasting a total of 6 to 12 weeks The classic stages are not commonly seen in infants younger than 3 months. The most frequent complication of Pertussis is pneumonia. Prevention through vaccine in combinations with tetanus and diphtheria (DTaP)