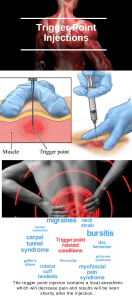
ADMINISTRATION OF OIL-BASED DEPOT AND OTHER LONGACTING INTRAMUSCULAR ANTI-PSYCHOTIC INJECTIONS TO ADULTS PROCEDURE The key messages the reader should note about this document are: 1. This procedure aims to guide practitioners involved in the administration of oilbased depots and other long-acting anti-psychotic medication to ensure that safe and effective care is delivered. 2. Deep Intramuscular Injections form part of a wider care plan. 3. Importance of clear and transparent documentation. 4. Consent to treatment should be obtained before each administration. 5. It is considered good practice, where additional practitioners are available, for a second check to be made in order to minimise the risk of error. Furthermore, individual teams should ensure a robust system is in place to identify when service user’s injections are due in the event of staff sickness or annual leave. NB: The second checker – This does not need to be performed by a qualified member of staff. However the second check needs to performed by someone who is competent to do so and is able to understand the following: Name of the depot injection (drug name) againt the depot prescribed on the prescription _ both need to be the same Appropriatly strength vial to ensure the least volume of depot is administered to the service users Feel confident to escalate or request advice regarding any issue related to the checking process This policy/procedure may refer to staff as qualified/registered/professional or other such term to describe their role. These terms have traditionally referred to individuals in a clinical role at band 5 or above. Please note that the use of these terms may or may not include nursing associates or associate practitioners (band 4). For clarification on whether a nursing associate or associate practitioner is an appropriate person to take on the identified roles or tasks in this policy/procedure please refer to the job description and job plan for the individual, or local risk assessment. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 1 of 28 DOCUMENT SUMMARY SHEET ALL sections of this form must be completed. Document title Administration of oil-based depot and other long-acting intramuscular antipsychotic injections to adults procedure Document Reference Number MM-0003 Key searchable words Depot, injection, administration, competence, training, safety, documentation. Executive Team member responsible (title) Medical Director Document author (name and title) Rob Edwards Clinical Lead Nurse and Non-Medical Prescribing Lead (Nursing) Approved by (Committee/Group) MOG – Medicines Optimisation Group Date approved 14 December 2017 Ratified by Policy & Procedure Group Date ratified 21 December 2017 Review date 11th December 2020 Frequency of review At least every three years Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 2 of 28 Amendment detail Version Amendment Reason 2.0 Placed into new procedural format Updated documentation 2.0 Record keeping section Added detail required to reflect current practice. 2.0 Safe disposal of sharps section Added detail required to reflect up-to-date information. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 3 of 28 CONTENTS Section Description 1 2 Page The content of the procedural document 1.1 Flow chart of procedure 4 1.2 Description of procedure/process 5 Appendices included as relevant Appendix A – Standard Operating Procedures 11 Appendix B – Maximum volume for oil-based depot administration into a single site 17 Appendix C – Training 18 Appendix D – Glossary of Definitions 19 Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 4 of 28 1. THE PROCEDURE 1.1 Flow chart of procedure Assessment of Service User and information exchange, assessment of cpacity to consent to treatment Dose calculation - test dose required on treatment initiatiation Choice of syringe and needle; prepare and draw up medication Choice of injection site based on drug license; adminstration of medication Evaluation of injection site and safe dispose of sharps Record-keeping; arrange next appointment. Review care plan at least every 6 months Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 5 of 28 1.2 Description of procedure General Preparation for the Deep IM Injection Depot preparations should be a treatment option where a service user expresses a preference for such treatment because of its convenience, or as part of a treatment plan in which the avoidance of covert non-adherence with antipsychotic drugs is a clinical priority (NICE, 2009). The administration of any medication is an opportunity for assessment and information exchange with the service user and carer(s), where appropriate. Preparation should include assessment to ascertain if the physical and/or mental health of the service user has changed since the previous contact. Any beneficial effects or side-effects experienced since the last injection should be considered and questions asked of the service user and their carer (where appropriate) to elicit any concerns or information needs. Prior to administration, the service user’s prescription should be checked to ensure that it is legal and valid. Allergy status should be checked. The LYPFT Medicines Code (MM-0004) outlines the required standards and the responsibilities of registered practitioners in prescribing, dispensing and administering medication. If administering Olanzapine depot injection the elearning must be completed prior to prescribing or administering the medication for the first time. Registration is required for access to the elearning which can be found at https://www.ZypAdhera.co.uk . Dose calculations Some drug administrations require complex calculations to ensure the correct volume of medication is administered. Appendix B illustrates the maximum volume for oil-based depot administration into a single site. If a greater volume is required, the practitioner should consider whether an alternative strength of the product is available. strength available (mg/ml) x required dose (mg) = volume required (ml) e.g. To give a dose of Zuclopenthixol Decanoate 350mg using the 200mg in 1ml ampoule (1 ÷ 200) x 350 = 1.75 Volume required = 1.75ml Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 6 of 28 When preparing for the administration of medication, it is considered good practice, where additional practitioners are available, for a second check to be made in order to minimise the risk of error. This second check may be undertaken by another registered practitioner or ‘medicines competent’ member of staff (see LYPFT Medicines Code (MM-0004). Choice of syringe and needle Where the product is provided in a pack with a syringe and needle for administration (i.e. Risperdal Consta, Xepilon or ZypAdhera) the syringe and needle provided should always be used and the manufacturer’s instructions followed. Practitioners should ensure that all needles used for the administration of depot medication incorporate a ‘sharp safe’ mechanism. Where the practitioner has to select an appropriate syringe and/or needle, it is necessary to consider the following: Needle length is indicated on the needle pack in inches and/or millimetres. An assessment of the length of needle required to reach the appropriate muscle should be made, taking into account any subcutaneous fat. If the chosen needle is not long enough to reach the muscle, consideration needs to be given as to which needle to use. Advice should be sight from the prescribing practitioner and also pharmacy. The gauge of the needle refers to the outer diameter of the needle. A smaller number indicates a larger outer diameter. 21 gauge needles (green hub) are most commonly used for intramuscular injections. The narrowest needle which complies with the product licence should be used. Where needles are supplied with an injection, only those needles should be employed. The smallest possible size of syringe should be used to accommodate the volume of the product given. Hand hygiene The Trust’s Hand Hygiene Procedure (IC-0002) describes the hand cleansing technique which should be adhered to. WHO (2010) recommends that non-sterile, well-fitting, single-use gloves must be worn if the practitioner’s or service user’s skin is not intact (e.g. through eczema, burns or skin infections) or when there is a likelihood of coming into direct contact with a service user’s blood or other potentially infectious materials. See the Standard Infection Control Precautions Protocol (ICDate effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 7 of 28 0004). It should be noted that gloves do not provide protection against needle-stick injuries and all sharps should be handled with caution. Preparing and drawing up medication Medication should be prepared immediately prior to its administration and practitioners should ensure all necessary equipment is available before proceeding. Practitioners must ensure that the expiry dates of all equipment are checked prior to use. Where medication requires reconstitution this should be carried out in line with manufacturer’s guidance. Blunt drawing-up needles with an internal filter are available to prevent the accidental drawing up of contaminants from glass ampoules. However, the viscosity (thickness) of the oil and size of the molecules in some oil-based depot injections may make drawing up through a filter needle difficult and could result in some of the product being discarded with the draw up needle when it is changed to the needle for administration. They are therefore NOT recommended for such injections (Hunter, 2008; Feetham & White, 2010) It is common practice to change the needle used for drawing up to a different needle for administration, however, this is only necessary where there has been a risk of blunting the needle (e.g. by perforating a rubber bung or by scratching it on the inside of an ampoule, Feetham & White, 2010). Choice of injection site Most oil-based depot antipsychotic injections must be administered only into the gluteal muscle by deep intramuscular (IM) injection. The exceptions to this are flupentixol and zuclopenthixol depots which are also licensed to be administered via the lateral thigh. Other long acting injections permit administration into either the deltoid or gluteal muscle. It is good practice for the prescriber to stipulate the muscle where the depot is to be given on the prescription, not just ‘I.M’. Appendix A illustrates the most common injection techniques. Further information regarding each technique can be found within the Royal Marsden Handbook of Clinical Nursing Procedures and video tutorials produced by the University of Hull can be found here: www.reach4resource.co.uk. The Summary of Product Characteristics for each anti-psychotic injection contains full details of the sites for which each injection is licensed and can be accessed online from the Electronic Medicines Compendium: www.medicines.org.uk/emc. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 8 of 28 Where, according to the product licence, a choice of injection site exists, this should be discussed with the service user. A joint decision on the preferred site should be made and recorded in the service user’s clinical record. Whichever site is selected, the registered practitioner must rotate the site and alternate between the left and right side of the body on each occasion the injection is administered. The site used on each occasion must be documented accordingly. The service user should be assisted into the chosen position for administration of the injection, according to the appropriate chosen site. Privacy and dignity should be maintained at all times. It is important to evaluate the injection site both pre and post injection observing for any signs of swelling, pain, inflammation, infection or tissue damage. If any of these signs are present or there are any other concerns, advice should be sought from an appropriate member of the care team before continuing with the procedure. Practitioners should ensure that an accurate reflection of any discussions that may take place is recorded in the service user’s clinical record. The site may be cleaned prior to injection using an alcohol swab. A period of 60 seconds must elapse before the injection to ensure the alcohol has dried on the skin. Z-Track Administration Technique (See Appendix A: SOP 2) Z-tracking is the recommended technique for all deep IM injections as it creates a broken injection pathway (the Z track), containing the medicine in the intended target muscle and preventing it from moving back up the track to leak out at the skin surface. This has the advantage of achieving the correct plasma concentration whilst minimising the risk of pain or lesions at the injection site. The injection site should not be massaged as this may interfere with the absorption rate of the depot and cause irritation by forcing the medication into subcutaneous tissue. Safe disposal of sharps Sharps should be disposed of at the point of use in a secure sharps bin. Needles should never be re-sheathed and the ‘safe sharp’ mechanism should be engaged as directed and discarded appropriately. In the event of a needlestick injury, the directions included within the Trust’s Blood Borne Viruses; including Sharps, Inoculation and Needle stick injury Protection and management procedure (IC-0003) must be followed. Sharp-safe needles are now commonplace in practice. Record keeping Good record keeping is essential for safe service user outcome, transparent practice and clinical audit. The clinical record should reflect the registered practitioner’s full, chronological account of assessment, planning and care and provide information relevant to the procedure at the time of the administration of the injection. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 9 of 28 No action or omission by the registered practitioner must compromise patient safety; records must demonstrate this duty of care. The Nursing and Midwifery Council (NMC) Record Keeping Standards clearly outline expectations in detail and should be referred to. As a minimum, the date and time of the injection, the name of the medicine and dose administered, the site of administration together with the registered practitioner’s signature and, where applicable, a signature from a second registered practitioner should be recorded on the service user’s prescription and administration chart. If a student administers the injection under supervision then their signature must be countersigned by the supervising registered practitioner. These will normally be recorded on the prescription and administration record. Ensure that the assessment of the patient’s capacity to consent is assessed and the legal requirements of the Mental Health Act are met and both must be recorded. Record the clinical intervention and specific references to any patient or carer concerns chronologically. A template for the assessment of mental capacity is available on paris. A link to assessment of mental capacity is also available on the LYPFT Staffnet at: http://staffnet/supportservices/Governance/mha/Mental Capacity Act/MCA - Forms/MCA1 - Capacity Assessment.doc. The practitioner should calculate when the next injection is due and arrange a convenient appointment with the service user. The next due date should be recorded in the service user’s clinical record and diarised where appropriate. Individual teams should ensure a robust system is in place to identify when service user’s injections are due in the event of staff sickness or annual leave. This can include a second practitioner who has already met the service user and where possible already administered the depot injection. Practitioners should ensure they adhere to the NMC (2010) Recordkeeping Standards, recording an accurate reflection of any discussions and decisions made. Any deviation from normal practice must be clearly recorded in the service user’s clinical record with the rationale for the clinical decision to do so. Any incidents, errors or near misses must be reported as described in the Trust’s Management of Incidents, Including Serious Incidents Procedure (RM-0002). Monitoring and review Immediately following administration the service user should be observed for adverse effects. Any special instructions for post-injection monitoring in the product licence must be planned for and followed. For example, after the administration of olanzapine long-acting injection the service user must be monitored for at least 3 hours for signs and symptoms consistent with olanzapine overdose. All service users must have their long-acting antipsychotic treatment reviewed by the clinical team on a regular basis. Such reviews should consider efficacy, including any changes in symptoms and behaviour, side effects, adherence and physical health (NICE, 2009). Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 10 of 28 Regular monitoring of side effects should be carried out using a validated tool, such as the Glasgow Antipsychotic Sidee Effect Scale (GASS). The GASS assessment tool is available on PARIS. Clinical reviews must be undertaken at least every six months in discussion with the service user, carer (where appropriate) and the care team, and will usually take place as part of the Care Programme Approach review. This should be a minimum of annualy but best practice is for the care plan to be reviewed based on needs and clinical presentation. Shared care guidelines Practitioners should ensure they are aware of the Leeds Health Pathways shared care guidelines which relate to the prescribing of depot medications and transfer of care to primary care. These can be found at: http://nww.lhp.leedsth.nhs.uk. Test dose For oil based depot IM anti-psychotic injections it is necessary to give a test dose before treatment is initiated to assess for tolerability to both the active ingredients as well as the oily vehicle. Occasionally a service user with a nut allergy may react to the oil and if a full dose is given from the outset then the service user may experience more severe, protracted discomfort. For this reason it is important to check the summary of product characteristics and the service user’s allergy status prior to administration. Full details of test doses for the oil-based depot injections are given in each individual Summary of Product Characteristics (SmPC) as well as in the British National Formulary (BNF). Missed appointments Missed appointments or changes to the planned injection due date should be communicated with the prescriber and documented appropriately in the service user’s clinical record. Some depot injections have information in their product literature which can be found at www.medicines.org.uk about what action to take if the dose is missed e.g. if missed paliperidone monthly depot by more that 6 weeks since the last dose extra doses need to be given. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 11 of 28 2. APPENDICES Appendix A SOP 1 Standard Operating Procedure 1 General Preparation for Deep Intramuscular (IM) Injection Applicable to: Registered nurses required to administer oil-based depots and other long-acting intramuscular antipsychotic injections in the course of their practice. Process 1 Read the prescription and check that the prescription is for that service user. Establish the identity of the service user using two sources of information e.g. visual/ wristband and date of birth. Process 2 Check to see if the service user’s physical or mental health has changed since the previous contact, including the health of any previous injection sites. Process 3 Ask about perceived benefits and any side effects experienced since the last injection (if this is not the first). Process 4 Check the prescription to ensure: Process 5 It is legal and valid The dose is due and has not already been administered There are no contra indications or allergies Locate the medication and check: The expiry date of the medication to be administered has not passed It is the correct formulation Process 6 Confirm that the service user has the capacity to consent and gives their consent to the procedure. Record the assessment of capacity clearly in thr clinical casenotes. Process 7 Wash your hands according to procedure and put on disposable gloves. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 12 of 28 Process 8 Prepare the injection, making any necessary dose calculations and using the correct equipment. Process 9 Carry out a final check of all items in processes 4, 5, 6 & 8. Where possible get a second practitioner to double check. Process 10 Chose the site of administration according to the licensed indication for the injection and in collaboration with the service user. SOP 2 Standard Operating Procedure 2 Z-Track Administration Technique Applicable to: Registered nurses required to administer oil-based depots and other long-acting intramuscular antipsychotic injections in the course of their practice. This technique should be used for all IM injections Process 1 Pull the skin in the target area taut and to one side with either the thumb or side of the non-dominant hand and maintain firm traction of the skin throughout the procedure Process 2 Insert the needle with a darting motion at a 90 degree angle to the skin surface to an adequate depth to allow the needle to penetrate the muscle. Keep the graduation markings on the syringe barrel visible at all times Process 3 For dorsogluteal injections only Steady the barrel of the syringe with the remaining fingers of the nondominant hand and pull back on the plunger with the dominant hand to aspirate. Should blood appear in the syringe all the equipment must be discarded and the whole procedure started again. If no blood appears it is safe to continue. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 13 of 28 (Where injections are to be administered into sites where there are no major blood vessels below the injection site this step is unnecessary) Process 4 Depress the plunger slowly (1ml per 10 seconds) to allow the muscle fibres to expand to accommodate the drug Process 5 Wait a further 10 seconds before removing the needle and once it has been removed , only then release the traction on the skin Process 6 If necessary the injection site may be wiped with a dry gauze swab Process 7 A plaster may be applied if this is the patient’s choice and if they have no known allergy to latex, iodine or elastoplast® SOP 3 Standard Operating Procedure 3 Administration Technique for the Deltoid Site Applicable to: Registered nurses required to administer oil-based depots and other longacting intramuscular antipsychotic injections in the course of their practice. Process 1 Ask the service user to sit down and loosen their clothes so their arm and shoulder are exposed. Ask them to place their hand on their stomach and relax the arm Process 2 Follow processes 1-10 in SOP 1 Process 3 Palpate the upper arm and find the landmarks of the acromion process and the axilla. The target injection site can be found by visualising an inverted triangle which extends from the acromion process and down to a point level Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 14 of 28 with the axilla. Form a rectangle within the original triangle by placing two fingers below the acromion process to form the top edge of the rectangle and with the bottom edge level with the axilla. The side edges of the rectangle should be parallel to the arm. The injection site is in the middle of this visualised rectangle. Process 4 Clean the skin, if necessary with an alcohol swab Process 5 Administer the injection using a Z-track technique (SOP 2) Process 6 Dispose of all equipment immediately with safe disposal of sharps into an appropriate, puncture proof, correctly labelled sharps bin. Do not re-sheath needle Process 7 Remove gloves and wash your hands according to Trust procedure Process 8 Document on the prescription/administration chart and in the clinical record the date, time and dose of medication administered, injection site and side of the body plus any deviation from standard practice with a rationale for the clinical decision to do so. Process 9 Exchange information about monitoring arrangements, how to manage common side effects and what to and what to do if the service user experiences any change to their mental or physical health status before the next clinical contact Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 15 of 28 SOP 4 Standard Operating Procedure 4 Administration Technique for the Dorsogluteal Site Applicable to: Registered nurses required to administer oil-based depots and other longacting intramuscular antipsychotic injections in the course of their practice. Process 1 Follow processes 1-10 in SOP 1 Process 2 Ask the patient to lie down and loosen their clothes so one buttock is exposed. Ask them to either lie on their front or side with the femur internally rotated to minimise pain on administration. The service user may prefer to stand or bend over a chair rather than to lie down. In such cases the service user should be asked to take the weight off their foot on the side where the injection is to be administered. Process 3 If a syringe and/or needle is provided in the product pack by the manufacturer this must be used. If not select an appropriate needle length to reach the gluteus muscle. Consider the Body Mass Index (BMI) and gender of the service user. In obese service users with a BMI of 30 or more, a 50mm needle may be required. Process 4 Draw an imaginary cross onto one buttock and identify the upper outer quadrant. Divide this first quadrant into quarters. The injection site is located within the upper outer quadrant of the upper outer quadrant, approximately 5 to 7.5cm below the iliac crest. Process 5 Clean the skin if necessary using an alcohol swab Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 16 of 28 Process 6 Administer the injection using a Z-track technique (SOP 2) Process 7 Dispose of all equipment immediately with safe disposal of sharps into an appropriate, puncture proof, correctly labelled sharps bin. Do not re-sheath needle Process 8 Remove gloves and wash your hands according to Trust procedure Process 9 Document on the prescription/administration chart and in the clinical record the date, time and dose of medication administered, injection site and side of the body plus any deviation from standard practice with a rationale for the clinical decision to do so. Process 10 Exchange information about monitoring arrangements, how to manage common side effects and what to and what to do if the service user experiences any change to their mental or physical health status before the next clinical contact SOP 5 Standard Operating Procedure 5 Administration Technique for the Ventrogluteal Site Applicable to: Registered nurses required to administer oil-based depots and other longacting intramuscular antipsychotic injections in the course of their practice. Process 1 Follow processes 1-10 in SOP 1 Process 2 Ask the patient to lie down and expose their hip. Where the service user prefers to stand they should be asked to take the weight off their foot on the side where the injection is to be administered. Process 3 Palpate the greater trochanter. Place the heel of the opposite hand to the service user’s leg on the greater trochanter (i.e. your left hand on their right leg or vice versa). Locate and place index finger of on the anterior superior ileac spine and travel along it until your index finger is in line with the vertical axis of the body. Your thumb should be pointing towards the front of the leg. Spread the middle finger to form a ‘V’. The injection site is in the middle of this ‘V’ level with the first knuckles of your fingers. Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 17 of 28 Process 4 Visualise the site and remove your hand to prevent needlestick injury Process 5 Clean the skin if necessary using an alcohol swab Process 6 Administer the injection using a Z-track technique (SOP 2) Process 7 Dispose of all equipment immediately with safe disposal of sharps into an appropriate, puncture proof, correctly labelled sharps bin. Do not re-sheath needle Process 8 Remove gloves and wash your hands according to Trust procedure Process 9 Document on the prescription/administration chart and in the clinical record the date, time and dose of medication administered, injection site and side of the body plus any deviation from standard practice with a rationale for the clinical decision to do so. Process 10 Exchange information about monitoring arrangements, how to manage common side effects and what to and what to do if the service user experiences any change to their mental or physical health status before the next clinical contact Video tutorials of these procedures can be found at: www.reach4resource.co.uk Date effective from: 21/12/17 Document Reference Number: MM-0003 Version No: 2.0 Page 18 of 28 Appendix B Maximum volume for oil-based depot administration into a single site Generic Name Brand/Trade name Max. Volume Flupentixol decanoate 20mg in 1ml Depixol Injection 2ml Flupentixol decanoate 100mg in 1ml Depixol Concentrate 2ml Flupentixol decanoate 200mg in 1ml Depixol Low Volume Injection 2ml Fluphenazine decanoate 25mg in 1ml Modecate Injection Not specified in SPC Fluphenazine decanoate 100mg in 1ml Modecate Concentrate injection Not specified in SPC Haloperidol decanoate 50mg in 1ml Haldol Decanoate 50mg in 1ml 3ml Haloperidol decanoate 100mg in 1ml Haldol Decanoate 100mg in 1ml 3ml Zuclopenthixol decanoate 200mg in 1ml Clopixol Injection 2ml Zuclopenthixol decanoate 500mg in 1ml Clopixol Concentrate Injection 2ml As cited in: Guidance on the administration to adults of oil-based depot and other long-acting intramuscular antipsychotic injections: Fourth Edition (2014) Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 17 of 28 Appendix C TRAINING There is a requirement that all registered practitioners involved in prescribing, preparing, administering and monitoring oil-based depot and other long-acting intramuscular anti-psychotic injections receive training in order to be able to meet the expected level of competency and standards outlined to prevent harm to patients through safe practice (NPSA, 2007). All registered nurses must complete the Trust’s Medicines Calculations and Medicines Administration for Nurses (available on iLearn) in order to evidence their competency in this area. Medicines calculations are also available on iLearn and needs to be completed annually. Nurses wishing to refresh their skills and knowledge may do so by accessing classroom based training or e-learning (also available on iLearn), details of which can be found on the Staffnet iLearn page. Practitioners should recognise and work within the limits of their competence, seeking advice and support from an appropriate source where required. Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 18 of 28 Appendix D GLOSSARY OF DEFINITIONS Definition Meaning Deltoid site The location for administration of injection into the deltoid muscle. Depot In mental health, this is the term used for oil-based long acting intramuscular (IM) antipsychotic injections designed to be given by deep IM injection. They consist of the antipsychotic esterified to a decanoate or palmitate dissolved in an oily vehicle. The volume to be injected is deposited deep into the gluteal muscle and forms a depot from where it leaches over time according to its oil:water partition co-efficient into the blood stream. This, together with the time taken for circulating enzymes to hydrolyse the ester back to its base, is responsible for the prolonged length of action of these formulations. Dorsogluteal site The location for administration of injection into the gluteus maximus. Often referred to as the “Upper Outer Quadrant of the buttock”. This the most common site for administration of an oil-based antipsychotic depot injection. There is currently discussion as part of the rapid tranquilisation procedure update regarding the use of ventro-gluteal site as an alternative administration site, depending on the license of the drug. Long Acting In mental health, this is the term preferred for non oil-based long-acting Injection (LAI) intramuscular antipsychotic formulations such as risperidone (Risperdal Consta), paliperidone (Xeplion) and olanzapine (ZypAdhera) long-acting injections. The same careful injection technique is required to administer these products but their release characteristics are very different to each other as well as to oil-based formulations. Safer sharp The term ‘safer sharp’ means medical sharps that incorporate features or mechanisms to prevent or minimise the risk of accidental injury. Test dose An initial low dose of an oil-based depot antipsychotic injection which must be given to assess for tolerability to both the active ingredient and its vehicle or any other excipient. Vastus lateralis The lateral quadriceps muscle. Ventrogluteal The location for administration of injection into the gluteus medius and Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 19 of 28 site gluteus minimus. Colloquially referred to as the “Hip site”. Z-tracking This is the recommended technique for all deep IM injections. it displaces superficial layers of skin and tissue creating a broken injection pathway (the z-track) containing the medicine in the intended target muscle and preventing it from moving back up the track to leak out at the skin surface. This has the advantage of achieving the correct plasma concentration whilst minimising the risk of pain or lesions at the injection site. Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 20 of 28 PART B 3. IDENTIFICATION OF STAKEHOLDERS The table below should be used as a summary. List those involved in development, consultation, approval and ratification processes. Stakeholder Level of involvement Medicines Optimisation Group Development & Consultation Operational Managers Consultation Policies and Procedures Group Consultation Infection Prevention and Control Team Consultation Lead Nurses Consultation 4. REFERENCES & EVIDENCE BASE CQC (2008) Nurses, the Administration of Medicine for Mental Disorder and the Mental Health Act 1983 The Care Quality Commission: London Crowley J, Griffiths M, Hardy S et al (2008) Mental Health Practice Essential Guide: Administration of Depot and Long Acting Antipsychotic Injections Mental Health Practice 12 (2): 1-18 Dougherty L & Lister S. Eds (2011) The Royal Marsden Manual of Clinical Nursing Procedures, 8th Edition. Wiley-Blackwell: Chichester Greenway K (2004) Using the Ventrogluteal Site for Intramuscular Injection Nursing Standard 18 (25): 39-42 HSE (2012) EU Directive on preventing sharp injuries in the hospital and healthcare sector Health and Safety Executive: Bootle Hunter, J (2008) Intramuscular Injection Techniques Nursing Standard 22 (24): 3540 Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 21 of 28 Mental Capacity Act 2005 Mental Health Act 1983 (as amended by the Mental Health Act 2007) NICE (2009) Core Interventions in the Treatment and Management of Schizophrenia in Primary and Secondary Care (CG82) National Institute for Health and Clinical Excellence: London NPSA (2007) Promoting Safer Use of Injectable Medicines: Patient Safety Alert, National Patient Safety Agency: London Feetam & White J (Eds.) (2011) Guidance on the administration to adults of oilbased depot and other long-acting intramuscular antipsychotic injections: Third Edition available at www.hull.ac.uk/injectionguide. Guidance on the Administration to Adults of Oil-based Depot and other Long-Acting Intramuscular Antipsychotic Injections 4th Edition, (2014) [online]. Available at: https://my.rcn.org.uk/__data/assets/pdf_file/0003/565626/SOP_Final_2014_PDF.pdf [accessed 16th November 2017]. NICE clinical guidelines for psychosis and schizophrenia (CG 178). NICE. Feb 2014. NMC (2010b) Recordkeeping Standards Nursing and Midwifery Council: London NMC (2010a) Standards for Medicines Management. Nursing and Midwifery Council: London Prescqipp Community interest Company. Antipsychotic drugs. (2014) [online]. Available at: www.prescqipp.info/antipsychotic-drugs/send/113-antipsychoticdrugs/2876-bulletin-135-antipsychotics-update [accessed 16th November 2017]. Rodger M & King L (2000) Drawing up and administering intramuscular injections: a review of the literature Journal of Advanced Nursing 31(3): 574-582 Schizophrenia: aripiprazole prolonged-release suspension for injection, (2014) [online]. Available at: www.nice.org.uk/advice/esnm39/chapter/key-points-from-theevidence [accessed 16th November 2017]. Taylor D, Paton C & Kapur S (2012) The Maudsley Prescribing Guidelines in Psychiatry: 11th Edition Wiley-Blackwell: London Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 22 of 28 WHO (2010) Best practices for injections and related procedures toolkit World Health Organisation: Geneva Workman B (1999) Safe Injection Techniques Nursing Standard 13 (39):47-53 Zabak A, Gunes UY, Tamsel S et al (2007) Does obesity prevent the needle from reaching muscle in intramuscular injections? Journal of Advanced Nursing 58 (6):552-556. 5. ASSOCIATED DOCUMENTATION LYPFT Medicines Code (MM-0004) LYPFT Non-Medical prescribing Procedure (MM-0001) LYPFT Hand Hygiene Procedure (IC-0002) LYPFT Standard Infection Control Precautions Protocol (IC-0004) LYPFT Blood Borne Viruses; including Sharps, Inoculation and Needle stick injury Protection and management procedure (IC-0003) LYPFT The Management of Incidents, Including Serious Incidents Procedure (RM0002) 6. Standards/key performance indicators The key performance indicators below are monitored by the assurance framework outlined in the table below: safe administration of depot medication; compliance with professional and good practice standards for medicines management; compliance with the Trust’s Medicines Code. Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 23 of 28 7. EQUALITY IMPACT The Trust has a duty under the Equality Act 2010 to have due regard to the need to eliminate unlawful discrimination, advance equality of opportunity and foster good relations between people from different groups. Consideration must be given to any potential impacts that the application of this policy/procedure might have on these requirements and on the nine protected groups identified by the Act (age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion and belief, gender and sexual orientation). Declaration: The potential impacts on the application of this policy/procedure have been fully considered for all nine protected groups. Through this process I have not identified any potential negative impacts for any of the nine protected groups. Print name: Rob Edwards Job title: Clinical Lead Nurse and Non-Medical Prescribing Lead (Nursing) Date: 7th December 2017 If any potential negative impacts are identified the Diversity Team must be contacted for advice and guidance: email; diversity.lypft@nhs.net. Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 24 of 28 CHECKLIST To be completed and attached to any draft version of a procedural document when submitted to the appropriate group/committee to support its consideration and approval/ratification of the procedural document. This checklist and is part of the working papers. Title of document being newly created / reviewed: 1. 2. Title Is the title clear and unambiguous? Yes Is the procedural document in the correct format and style? Yes Development Process Is there evidence of reasonable attempts to ensure relevant expertise has been used? 3. 8. Yes Equality Impact Assessment Has the declaration been completed? 7. Yes Approval Does the document identify which committee/group will approve it? 6. Yes Content Is the Purpose of the document clear? 5. Yes / No/ Yes Review Date Is the review date identified? Yes Is the frequency of review identified and acceptable? Yes Overall Responsibility for the Document Is it clear who will be responsible for co-ordinating the dissemination, implementation and review of the document? Yes Name of the Chair of the Committee/Group approving If you are assured this document meets requirements and that it will provide an essential element in ensuring a safe and effective workforce, please sign and date below and Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Page 25 of 28 forward to the chair of the committee/group where it will be ratified. Name E Weston Date 14/12/17 Name of the chair of the Group/Committee ratifying If you are assured that the group or committee approving this procedural document have fulfilled its obligation please sign and date it and return to the procedural document author who will ensure the document is disseminated and uploaded onto Staffnet. Name C Hill Date effective from: 11th December 2014 Document Reference Number: MM-0003 Version No: 1.0 Date 21/12/17 Page 26 of 28