Pneumonia Patient Care Plan: Nursing Diagnosis & Interventions
advertisement

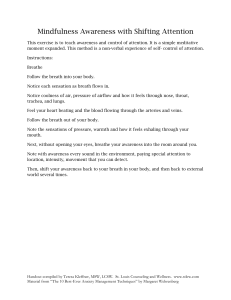
Student Name/Date _02/03/2020_ Disease Process _Pneumonia__ Pathology (at cellular level-Define tech terms) Risk Factors/Causes (list classic &* if your pt has) -Abdominal or thoracic surgery -Age >65 yr* -Air pollution -Altered consciousness: alcoholism, head injury, seizures, anesthesia, drug overdose, stroke -Bed rest and prolonged immobility -Debilitating illness -Inhalation or aspiration of noxious substances -Intestinal and gastric feedings via nasogastric or nonintentional tubes -IV drug use -Malnutrition -Resident of a long-term care facility -Smoking -Upper respiratory tract infection Inflammation in the lungs results in filling of the alveolar May lead air spaces with exudate, inflammatory cells, and fibrin. The neutrophils present in the air spaces kill pathogens to by releasing enzymes and antimicrobial proteins. The inflammatory injury causes the lining to secret mucus secretions, reduced ventilation, and impair gas exchange. Classic Treatments (* those pt receiving & specify name of med your pt on) Medical: -PT daily* -OT daily* -SCDs while in bed* Results -Oxygen 2L NC prn to keep sats >92%* Determin e -Control fever with aspirin or nonsteroidal antiinflammatory drugs* _________________________________________ Nursing (include edu): -Educated pt on importance of ambulation -Out of bed for meals* -IS q1hr while awake* -Encourage deep breathing exercises, caution patient to stop if feeling lightheaded or shortness of breath If treatment unsuccessful Classic Complications (*those pt has- Define technical term) -Atelectasis(collapsed, airless alveoli) of one or another lobe in the lungs -Pleurisy (inflammation of the pleura) -Pleural effusion (fluid in the pleural space) -Bacteremia (bacteria infection in the blood) -Meningitis (inflammation of the protective membranes covering the brain and spinal cord) -Acute respiratory failure (damages the lungs ability and the exchange of O2 and CO2) -Sepsis/septic shock (occurs when bacteria within alveoli enter the bloodstream) -- Cite Sources (Lewis et al, 11th edition)_ Classic Imaging and Tests to confirm this Disease_ Test Classic Result Pt Result -chest x-ray -patchy or infiltrates -interstitial infiltrates Signs & Symptoms (list classic &* those pt has. Define technical terms) Manifests As -cough* -fever* (low grade 99.8) -chills -Dyspnea* -Tachypnea* -Pleuritic chest pain -Sputum* (yellow) -confusion* -stupor -hypothermia - Fine or coarse crackles* Led to hospitalization Patient Information: Initials _RB___ Rm # _301 Age_86_ Sex__M__ Adm Date ______ MD __Michael -low O2 Sat (90%) Chief -92% McCaffery__ Concern Allergies _NKDA_ Code Status __FULL____ Prompts Diet __Regular____Chief Concern _Shortness of breath with activity and a productive cough_ Diagnosis Comorbidity Abnormal Imaging and other Tests _Pneumonia__ Surgery and Date: Test Result Your Pt’s Etiology V/S & Pain Level on Day of Care: _ Temp 99.8, Pulse 102, -R hip X-ray: -Intertrochanteric -pt fell 2 weeks ago Blood Pressure 166/87, Resp 24, O2 Saturation 92% on 2L fracture of the NC, Pain 3/10 _ femur, pelvic Hendrich Score with interp ___5: High risk__ osteopenic Braden Score with interp _18: Mild risk for pressure ulcers IV site: None (continuous or saline lock-circle one) Activity Level: Weight bearing with walker, up adlib, out of bed for all meals Tubes/Drains: None Treatments (circle all ordered and list other) IS, O₂ SCDs, Classic Lab Tests that confirm Disease Process OT, PT, RT, Accu√, Dressing Chg, Other: _________ Test Normal Classic Trend Pt’s Result New meds for new problems: enoxaparin, polyethylene WBC 4.0-11.0 elevated 12.6 (HIGH) glycol, hydrocodone/apap, lisinopril, Sputum Negative Positive Not done Currently pt is ( circle one: improving/stable/ worsening) culture & state supporting rationale : RB is not participating in PT at this time, refusing to transfer OOB for meals. Comorbidity Abnormal Lab Results Past Med/ Surgical History (* those R/T admit) Test Normal Pt’s Result Etiology -Hypertension -Gastroesophageal reflux disease HgB 11.5-15.4 9.9 (Low) Anemia-blood -Chronic joint and back pain Hct 34.0-45.0 29.4(Low) loss -Benign prostatic hyperplasia Calcium 8.8-10.5 8.0(Low) Anemia-blood -Right forearm fracture (two years ago) RBC 3.80-5.10 2.83(Low) loss -Tonsillectomy (age 15) Albumin 3.5-5 3.0 (Low) Hypocalcemia Recent -Cataract removal (1998) surgery -Fracture Right Ulna (2009) Poor appetite -Fracture Right Hip two weeks ago with ORIF* -pulse oximetry Student Name/Date: NPR Steps 2-5 (DIAGNOSIS, PLANNING, INTERVENTON, EVALUATION) Step 2: NANDA Nursing Diagnosis Step 3: Planning SMART Goal #1 Nursing Diagnosis- Infective Airway Clearance R/T Retained secretions AEB: Course lung sounds, yellow septum, and shortness of breath Plan: Pt. Smart Goal- To address ineffective airway clearances, RB will have oxygen saturation level of at least 95% by the end of the shift. RB will demonstrate proper incentive spirometer technique before and after each meal by the end of the shift today. Nursing Interventions 1. Auscultate Breath sounds every 1 to 4 hours. Clinical Research: Breath sounds are normally clear to scattered fine crackles at bases, however coarse crackles indicate fluid in the airway, and wheezing indicated an obstructive airway. (Faucl et al, 2008 in Ackley, 11th pg 131) 2. Help the client to deep breath and perform controlled coughing. Have pt. inhale deeply, hold breath for several seconds, and cough twice with mouth open while tightening upper abdominal muscles. Clinical Research: Controlled coughing uses the diaphragm muscles which makes the cough more forceful and effective (Gosselink et al, 2008 in Ackley, 11th pg 132) 3. Teach importance of the incentive spirometer and emphasize its impact on keeping clear airways and improving clients pneumonia. Clinical Research: Inceptive spirometer as well as controlled coughing and deep breathing have a positive impact on airway clearance. (Gosselink et al, 2008 in Ackley, 11th pg 132) Evaluation: Goal not met. RB’s lungs demonstrated crackles upon auscultation in all lung fields. RB was unable to perform deep breathing exercise. RB compliments of being “short of breath”. RECOMMENED: Attempt ambulation when RB is alert, such as shortly after breakfast. Limit physical activity before deep breathing exercises to avoid shortness of breath. Step 4: Interventions & Research Rationale (cite research from Ackley) Step 5: Evaluation * Met, Partially Met, or Not Met,*In patient terms, summarize the patient’s response to interventions #2 Nursing Diagnosis- Impaired physical mobility R/T Activity intolerance, anxiety, decreases in muscle strength/control, muscle disuse, chronic pain, malnutrition AEB: Discomfort slow movement, uncoordinated movement, alteration in gait. Plan: Pt. Smart Goal– In order to address impaired physical immobility, RB will ambulate 20 ft. down the hallway and back after breakfast and lunch during my shift. #3 Nursing Diagnosis- Risk for fall R/T : Altered cognitive function or confusion, polypharmacy, age greater than 65, sleeplessness, impaired mobility, decreased physical strength, decreased lower extremity. AEB: Plan: Pt. Smart Goal- In order to address risk for falls RB will demonstrate pressing the call bell before getting out of bed by the need of my shift. Nursing Interventions Nursing Interventions 1. Before activity, observe for and if possible, treat pain with massage, heart pack to affected area, or medication, Ensure that the client is not sedated. Clinical Research: Pain limits mobility, and if exacerbated by specific movement should be temporality avoided. (America College of Sports and Medicine, 2018, 12th pg 621) 1. Screen all clients for mobility skills Clinical Research: Helpful to determine the clients functional abilities and then plan for ways to improve problem areas or determine methods to ensure safety. (Podsiadio & Richardson, 1991 in Ackley, 12th pg 372) 2. Asses for fear of falling Clinical Research: Self-reported fear of falling has been shown to be a significantly more sensitive predictor for fall risk than the STRATIFY fall risk assessment tool. (Strupelt, Buss, & Wolf-Ostermann, 2016, 12th pg 621 ) 2. When rising from a lying position, have the client change position slowly, dangle legs, and stand next to the bed before walking to prevent orthostatic hypotension. Clinical Research: Encourage client engagement in a monitored exercise program that will strengthen and lower extremities to reduce fall risk. (Grablner, 2013; Hirase et al, 2014 in Ackley 12th pg 372) 3. Increase activity tolerance with graded increase in self-care, such as bathing, walking to the bathroom, and ROM. Clinical Research: A study of FFC in older adults hospitalized after trauma found greater improvement in function, less fear of falling, and better physical resilience than controls at discharge and 30 days after discharge. (Resnick, Gallk, &Vigne, 2016 12th pg 621) Evaluation: Goal partially met. RB was only able to ambulate 50 ft with assistance once by the end of my shift. RB complained of pain of 6.10 and fatigue when attempted to ambulate the second time during my shift. RECOMMEND: teaching RB to call nurse for pain wherever 4.10 and to notify nurse of tolerable level of exercise. 3.Teach the client how to safety ambulate at home Clinical Research: per Subject Matter Expert (Greenberg, 2020 in Ackley 12th, pg 376) Evaluation: Goal was met. RB was taught and was able to performed ambulation safety. RB changed positions slowly to prevent orthostatic pressure. RECOMMED: continue to encourage RB to engage in exercise programs that will strengthen his lower extremities to reduce his risk for falling.