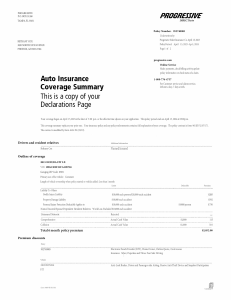
Form_SCTNID_CTGRY.FL01186489_DECPAGE <docindex><index>DECPAGE</index></docindex> PROGRESSIVE P.O. BOX 31260 TAMPA, FL 33631 Policy Number: 952740085 Underwritten by: Progressive Select Insurance Co October 6, 2021 Policy Period: Oct 1, 2021 - Apr 1, 2022 Page 1 of 2 CASEY D JOHNSON 912 KLONDIKE AVE WINTERGARDEN, FL 34787 progressive.com Online Service Make payments, check billing activity, update policy information or check status of a claim. Auto Insurance Coverage Summary This is a copy of your Declarations Page 1-800-776-4737 For customer service and claims service, 24 hours a day, 7 days a week. Your coverage began on October 1, 2021 at the later of 12:01 a.m. or the effective time shown on your application. This policy period ends on April 1, 2022 at 12:01 a.m. This coverage summary replaces your prior one. Your insurance policy and any policy endorsements contain a full explanation of your coverage. The policy contract is form 9611D FL (07/17). The contract is modified by form A261 FL (05/19). Drivers and ……………………………………………………………………………………………………………………………………………………….. resident relatives Additional information Casey D Johnson Named insured Outline of coverage 2014 KIA OPTIMA 4 DOOR SEDAN VIN: 5XXGM4A75EG281854 Garaging ZIP Code: 34787 Primary use of the vehicle: Commute Length of vehicle ownership when policy started or vehicle added: Less than 1 month Limits Deductible Premium ……………………………………………………………………………………………………………………………………………………….. Liability To Others Bodily Injury Liability $10,000 each person/$20,000 each accident $285 Property Damage Liability $10,000 each accident 592 ……………………………………………………………………………………………………………………………………………………….. Personal Injury Protection/Deductible applies to $10,000 $1,000/person 750 Named Insured/Spouse/Dependent Resident Relatives Work Loss Excluded ……………………………………………………………………………………………………………………………………………………….. -Uninsured Motorist Rejected ……………………………………………………………………………………………………………………………………………………….. Comprehensive Actual Cash Value $1,000 115 ……………………………………………………………………………………………………………………………………………………….. Collision Actual Cash Value $1,000 310 ……………………………………………………………………………………………………………………………………………………….. Total 6 month policy premium $2,052.00 Premium discounts Policy ……………………………………………………………………………………………………………………………………………………….. 952740085 Electronic Funds Transfer (EFT), Home Owner, Online Quote, Continuous Insurance: Silver, Paperless and Three-Year Safe Driving Vehicle ……………………………………………………………………………………………………………………………………………………….. 2014 KIA OPTIMA Form 6489 FL (01/18) Anti-Lock Brakes, Driver and Passenger-side Airbag, Passive Anti-Theft Device and Snapshot Participation 4 Continued <docindex><index>DECPAGE</index></docindex> Policy Number: 952740085 Casey D Johnson Page 2 of 2 Lienholder and additional interest information Vehicle Lienholder Additional interest 2014 KIA OPTIMA 5XXGM4A75EG281854 Af title co dba financial Memphis, TN 38115 Af title co dba financial Memphis, TN 38115 ……………………………………………………………………………………………………………………………………………………….. Policyholder inquiries You may call Customer Service at 1-800-776-4737 to present inquiries or obtain information about coverage, and to obtain assistance with any complaints. Agent signature Company officers Secretary Form 6489 FL (01/18)