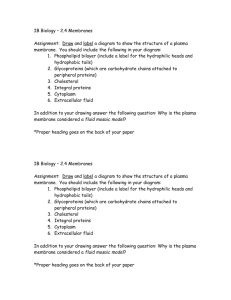
BIOCHEMISTRY Blood Chemistry Dr. Igrobay BLOOD INTRODUCTION Blood is one of the largest organ systems of the body It is the liquid that flows in an enclosed circulation that is part of the circulatory or cardiovascular system It consists of blood cells suspended in the plasma Plasma is the liquid portion of the unclotted blood Blood constitutes around 5-7% of the total body weight To know one’s blood volume, it is around 6% of your total weight in kg Specific gravity of blood is 1.06 pH of blood is 7.4 o Normal pH is 7.35-7.45 o Average pH is 7.4 Viscosity of blood is 1.7-2.0 Freezing point of blood is -0.56oC Osmotic pressure of blood at 37oC is 7.6 atm pressure 1. 2. 3. MAJOR FUNCTIONS OF BLOOD Respiration – transport oxygen from lungs to the tissues and of CO2 from the tissues to the lungs Nutrition – transport of absorbed food materials Excretion – transport of metabolic waste to the kidneys, lungs, skin, and intestines for removal Capillaries are the main site of respiration, exchange nutrition, and waste products 4. 5. 6. Maintenance of the normal acid-base balance in the body Regulation of water balance through the effects of blood on the exchange of water between the circulating fluid and the tissue fluid Regulation of body temperature by the distribution of body heat o Normal body temperature is 36.5-37.5oC o Average body temperature is 37oC o >37.5oC = hyperthermia o <36.5oC = hypothermia 7. Defense against infection by the white blood cells and circulating antibodies 8. Transport of hormones and regulation of metabolism 9. Transport of metabolites and regulation of metabolism 10. Coagulation – clot formation Plasma Fraction It has 2 constituents: diffusible and non-diffusible Diffusible constituents means it can spread in the body Non-diffusible constituents means it only focuses on a certain part of the body Diffusible constituents examples are: o Electrolytes o Sodium o Calcium o Potassium o Hormones o Vitamins Non-diffusible constituents examples are: o Proteins o Polypeptides PLASMA Plasma is the liquid part of fluid blood Serum is the fluid remaining after blood coagulates Plasma proteins consist of water, electrolytes, metabolites, nutrients, proteins and hormone Water and electrolyte composition of plasma is practically the same as that of all extracellular fluids Laboratory determination of levels of Na, K, Ca, Mg, HCO3 , PaCO2 and of blood pH are important in clinical management Plasma Proteins Majority of the plasma proteins is made up of water It is around 7.0 – 7.5 g/dL It is a complex mixture of glycoprotein and lipoproteins The plasma proteins can be separated into 3 major groups: 1. Fibrinogen 2. Albumin 3. Globulins Fibrinogen is involved in the coagulation cascade or clot formation. Fibrinogen will be converted to fibrin by the help of thrombin Albumin is a protein that serves as a transport vehicle that carries also bile salts and fatty acids Globulins are involved in the immune system (immunoglobulins) COMPOSITION OF BLOOD Picture above: There are two fractions: one is liquid which is the plasma and the other one is solid which is cellular (buffy coat + RBC). The plasma has the highest percentage compared to the cellular part. For the cellular fraction it is exemplified by the RBC which is the most abundant followed by the buffy coat. The buffy coat is composed of the white blood cells and the platelets The concentration of proteins in the plasma is important in determining the hydrostatic pressure and osmotic pressure in the body Edema can happen when either of the hydrostatic or oncotic pressure malfunctions Most plasma proteins are synthesized in the liver They are generally synthesized on membrane-bound polyribosomes Most of which are synthesized as preproteins Many of them exhibit polymorphism But each plasma protein has a characteristic half-life in the circulation The levels of certain proteins in plasma increase during acute inflammatory states or secondary to certain types of tissue damage The diversity of their biochemical properties attributes to their varying functions #GrindNation “Strength In Knowledge” BESHYWAP 1 BIOCHEMISTRY Blood Chemistry Dr. Igrobay 1. 2. 3. 4. 5. 6. 7. The normal total serum protein concentration is 6-8 g/dL (60-80 g/L) and is determined as a fraction containing albumin and the serum globulins >8 g/dL = Hyperproteinemia <6 g/dL = Hypoproteinemia The fibrinogen was discarded in the clot that separated from the plasma to form the serum specimen Increased concentration is termed as hyperproteinemia and this could be due to water depletion, multiple myeloma, macroglobulinemia, and sarcoidosis Decreased concentration is termed hypoproteinemia and this could be secondary to any organ dysfunction such as congestive heart failure, peptic ulcer, nephrosis, and cirrhosis Functions of the Plasma Proteins Antiproteases Blood clotting factors Enzyme hormones Immune defense Inflammatory responses Oncofetal Transport or binding proteins MAJOR TYPES OF PLASMA PROTEINS Albumin (69 kDa) The major plasma protein in humans 3.4-4.7 g/dL Makes up approximately 60% of the total plasma protein About 40% is present in the plasma and 60% in the extracellular space It is initially synthesized as preprotein in the liver (12 g/day) The concentration of the serum albumin controls the passage of water through the cell membrane by osmosis and is responsible for 75-80% of the osmotic pressure of human plasma In addition, it serves as a protein stores for the body that can be utilized when a deficit develops It serves as a solvent for fatty acids and bile salts It serves as a transport vehicle by loosely binding hormones, amino acids, drugs and metals Increased concentration (hyperalbuminemia) has no significant correlation with diseases. The reduction of circulating albumin concentration results in a shift of fluid from intravascular to extravascular spaces and is most commonly manifested as edema and/or congestion Decrease concentration (hypoalbuminemia) may be due to several mechanisms but the most common one is a decrease in the production of albumin in the liver Acute hepatitis and Chronic Liver Disease If the liver is defective, plasma protein is affected Treatment for hypoalbuminemia is letting the patient drink egg white Causes of albuminemia: 1. Reduced synthesis of albumin Malnutrition Protein calorie malnutrition such as in Kwashiorkor Malabsorption syndrome Intestines cannot absorb properly Chronic Inflammatory Disease Pulmonary tuberculosis 2. Genetic abnormalities Familial or hereditary disease 3. Increased loss of albumin Nephrotic syndrome Kidneys are defective = proteinuria Massive burns The higher the surface area of skin burned, the higher is the protein necessary to be repaired Protein losing enteropathy Protein losses at the GIT, goes in the stool 4. Increased catabolism of albumin Fast breaking own of albumin like in massive burns and widespread malignancy (Stage 3 or 4) Cancer cells uses protein in order to survive 5. Multifactorial Cirrhosis of liver or heart Congestive heart failure Pregnancy Haptoglobin (Hp) It is a plasma glycoprotein that binds extracorpuscular hemoglobin in a tight non-covalent complex [Hp-Hp (155kDa)], preventing the loss of free hemoglobin into the kidney thus conserving valuable iron present in hemoglobin The binding between haptoglobin and hemoglobin is highly specific It exists in three polymorphic forms: o Hp 1-1 o Hp 2-1 o Hp 2-2 The simplest of which is Hp 1-1 (90kDa) and is found in humans In extensive hemolysis, haptoglobin in the serum is depleted Thus, haptoglobin measurement is useful for the clinical assessment of hemolysis Haptoglobin is an acute phase reactant and is frequently elevated in medically stressful situations Transferrin (76 kDa) The transport of iron in the plasma is accomplish by transferrin, which migrates in the ß-globulin region 1 molecule of transferrin can bind 2 ions of iron It shuttles iron as Fe2+ (Ferrous) to sites where it is needed, either for storage or utilization In female who are part of the reproductive age group are prone to iron deficiency anemia due to menstruation Treatment to this is iron supplements and Vitamin C Iron supplements are in the Ferrous state (absorbable form) Vitamin C enhances the absorption of iron in the intestines #GrindNation “Strength In Knowledge” BESHYWAP 2 BIOCHEMISTRY Blood Chemistry Dr. Igrobay Ceruloplasmin (160 kDa) It is an α2-macroglobulin with a blue color because of its high copper content It carries 90% of the copper present in plasma Each molecule of ceruloplasmin binds six atoms of copper very tightly, so that the copper is not readily exchangeable Albumin carries the 10% of plasma copper and bind to it less tightly, donating it more readily to tissues than ceruloplasmin Ceruloplasmin exhibits a copper-dependent oxidase activity but physiologic significance has not been clarified Copper Metabolic Diseases: Menke’s diseases Also known as kinky or steely hair disease X-linked disorder due to mutation in the gene encoding a Copper-binding P-Type ATPase Willson’s disease Genetic disease wherein copper fails to be excreted in the bild Results to copper toxicosis Kayser-Fleischer ring - green or golden pigment ring around the cornea due to deposition of copper in Descemet’s membrane α1 – Antiproteinase (α1-Antitrypsin) (52 kDa) It is a major component of the α1 fraction (>90%) of human plasma It is synthesized by hepatocytes and macrophages Function of α1-antitypsin is to inhibit the production of elastase Elastase is secreted by bacterial neutrophils Elastase functions to recoil the lungs If α1-antitrypsin is affected, there is no recoil = barreled chest It is the principal serine protease inhibitor (serpin, or Pi) and has at least 75 polymorphic forms Congenital deficiency of α1 – antiproteinase can result in premature emphysema Volatile irritants found in cigarette smoking stimulate the release of proteases in the lungs Without α1-antiproteinase to inhibit these enzymes, it would cause considerable destruction to the lung parenchyma leading to severe often fatal emphysema A second clinical syndrome associated with congenital deficiency of α1-antiproteinase in children is cirrhosis of liver This disorder may require liver transplantation in severe cases α2 – Macroglobulin (720 kDa) A large plasma glycoprotein which transports approximately 10% of Zinc in plasma It is synthesized by variety of cell types including monocytes, hepatocytes, and astrocytes It is a major member of a group of plasma proteins that include complement proteins C3 and C4 These proteins contain a unique internal cyclic thiol ester bond and for this reason have been designated as the thiol ester plasma protein family This bond is highly reactive and is involved in some of the biologic actions of α2-macroglobulin It is an important panproteinase inhibitor, binding to many proteinases Panproteinase inhibitor means that α2-macroglobulin inhibits the enzyme responsible for degrading or hydrolyzing the whole polypeptide chain In deficiency of α1-proteinase, α2-macroglobulin probably is the primary protease inhibitor In nephrotic syndrome, α2-macroglobulin is allowed to retain in the circulation because of its large molecular weight, even in profound proteinuria In severe cases, the concentration of α2-macroglobulin in serum may approach or even exceed that of albumin Fibrinogen (340 kDa) A soluble plasma glycoprotein which consists of three non-identical pairs of polypeptide chains covalently linked by disulfide bonds All three chains are synthesized in the liver Half-life: 3.5 – 4 days It is a clotting factor 1: involve in the clot formation Causes of increase: Homeostatic stress (bleeding or hemorrhage) Nonspecific stressor of inflammation Pregnancy Autoimmune disorders All are pathologic except pregnancy Amyloidosis Amyloidosis is a disorder due to accumulation of various insoluble fibrillary proteins between cells of tissues to an extent that affects function It is generally due to either increased production of certain proteins or accumulation of mutated forms of other proteins DIFFERENTIATION OF RBC and OTHER BLOOD CELLS Hematopoiesis It refers to the formation and development of all types of blood cells from their parental precursors The marrow is a special environment for hematopoietic growth and development When the hematopoietic marrow cells are mature and ready to circulate to the peripheral blood, the cells leave the marrow parenchyma and emerge into venous sinuses The parental precursors are hematopoietic stem cells. Stem cells are pluripotential cells which means that they have the capability to become different kind of cells Stem cells can be found in the bone marrow or umbilical cord #GrindNation “Strength In Knowledge” BESHYWAP 3 BIOCHEMISTRY Blood Chemistry Dr. Igrobay Clinical Importance of Hematopoietic Stem Cells: Stem cell is a cell with a unique capacity to produce unaltered daughter cells (self-renewal) and to generate specialized cell types (potency) Stem cells may be: o Totipotent (capable of producing all the cells in an organism) o Pluripotent (able to differentiate into cells of any of the three germ layers) o Multipotent (produce only cells of a closely related family) o Unipotent (produce only one type of cell) Cell-cell interaction and the release of the humoral factors (CSFs, e.g. GMCSF/G-CSF: deficiency of which may result to neutropenia) do control the production and maturation of white cells Lymphopoiesis This is the growth and maturation of lymphocytes Lymphocytes are conditioned by two main organ systems, the thymus (T-lymphocytes) or the bone marrow (B-lymphocytes) Megakaryopoiesis This is the process of platelet development from megakaryocytes Thrombopoietin is a hormone that controls proliferation and maturation of megakaryocytes Different Progenitors of Hematopoietic Stem Cell Platelets are formed by the development of demarcation membranes within the cytoplasm, and individual platelets are extruded into the venous sinuses The RBC and platelets share a common pathway of differentiation. Each pathway is regulated by various factors (e.g. Stem cell factor (SCF), thrombopoietin (TPO), Interleukins (IL), erythropoietin (EPO), various colony stimulating factors (CSFs) Stem cell factor is a cytokine that plays an important role in the proliferation of hematopoietic stem cells and some of their progeny Thrombopoietin is a glycoprotein that is important in regulating the production of platelets by the bone marrow Interleukins are cytokines produced by leukocytes; they regulate various aspects of hematopoiesis and of the immune system Picture Above: The multipotential hematopoietic stem cell derived from the bone marrow can give rise to different progenitors. First it branches into two: Myeloid progenitor and Lymphoid progenitor. In Myeloid progenitor it gives rise to: o Granulocytes – Basophils, Eosinophils, Neutrophils (BEN) o Erythrocytes o Monocytes – differentiates into macrophages or dendritic cells o Mast cells o Megakaryocytes – becomes thrombocytes (platelets) For the Lymphoid progenitor, it gives rise to: o B lymphocyte o T lymphocyte o Natural killer cell Erythropoiesis Are derived from the committed erythroid precursor cells through a process of mitotic growth and maturation Erythropoietin (EPO) is a hormone produced largely by the kidney that stimulates CFU-E stem cells to speed up growth and enhance maturation Granulopoiesis It is the replacement of leukocytes by cell division and production of new white cells in the marrow A process of differentiation occurs, whereby immature white cells gradually develop and exhibit characteristics of mature functional leukocytes RED BLOOD CELLS (ERYTHROCYTES) Non-nucleated, biconcave in shape and devoid of intracellular organelles It functions mainly in the delivery of O2 and excretion of CO2 It has a lifespan of 120 days (it goes to the spleen after it dies) Approximately <1% of RBC is replaced daily at a rate of 2M/sec Has glucose transporter (GLUT 1) in its membrane and has powerful oxidants which are produced during the course of metabolism: Superoxide, Hydrogen peroxide, Peroxyl and Hydroxyl radicals and ROS Normal red cell count ranges from 4.2-6.2 x 10(6) Polycythemia literally means “many blood cells” but usually refers to increased red cell mass. A better term for this is erythrocytosis or erythremia Secondary or reactive polycythemia is due to a recognizable physiologic stimulus Polycythemia vera or True polycythemia is spontaneous or unprovoked increased in the red blood cells Anemia is defined as a decrease in the concentration of hemoglobin. This is often the end result of red blood cell abnormalities The red blood cell has a unique and relatively simple metabolism Continued next page….. #GrindNation “Strength In Knowledge” BESHYWAP 4 BIOCHEMISTRY Blood Chemistry Dr. Igrobay Red Blood Cell Membrane It consists of an integral layer of lipids, including phospholipids and cholesterol, which contain an intimate association of proteins These proteins may be integral or peripheral proteins Peripheral membrane proteins – associated with its surface, generally via protein-protein interactions, determining shape and flexibility Integral membrane proteins – glycosylated and span the membrane 3. Spectrin o o o Major protein of the cytoskeleton and confers the flexibility of the membrane of the RBC It has four binding sites: self association, Ankyrin, actin and protein 4.1 The disorder of which will lead to Hereditary Spherocytosis and also Hereditary Elliptocytosis Hereditary Spherocytosis - The protein-lipid composition is important in maintaining the integrity of the red cell membrane The membrane also resists an uncontrolled influx of sodium ions, which are present in higher concentrations in plasma and an efflux of potassium ions, which are present in higher concentrations within the red cell - Spherocytes (RBC’s without biconcave shape & central pallor) having low surface-to-volume ratio Cause hemolytic anemia Causes splenomegaly due to plugging of easilyruptured spherocytes in sinusoids of the spleen Susceptible to osmotic lysis Abnormal spectrin makes it unable to react with membrane proteins → weakened cell membrane and spherocytic shape Some of the Major Proteins of the RBC Membrane Hereditary Elliptocytosis - - 4. Ankyrin o o o 1. Anion exchange protein (Band 3) o C terminal is external and N terminal is internal o A multipass membrane protein, extending across the bilayer o Responsible for the reaction wherein from the tissues, CO2 is obtained CO2 from tissues enter the RBC as HCO3- → exchanged for Cl- in the lungs (chloride shift) Maintain electroneutrality within the cell o o 2. Elliptical RBs Defective spectrin or Glycophorin C or protein 4.1 (points of attachment) A pyramid-shaped protein that binds spectrin Also binds tightly to band 3, securing the attachment of spectrin to the membrane Sensitive to proteolysis 5. Actin (Band 5) o Exists in RBC as short, double-helical filaments of F-actin o The tail end of spectrin dimers bind to actin o Also binds to protein 4.1 6. Protein 4.1 o A globular protein that binds tightly to the spectrin forming a protein 4.1 – spectrinactin ternary complex o Also binds to the integral proteins Exists as a dimer in the membrane, in which it forms a tunnel, permitting the exchange of chloride for bicarbonate Cytosolic N terminal binds to Hb, protein 4.1 and 4.2, Ankyrin and several glycolytic enzymes Glycophorin A, B, and C o Transmembrane glycoprotein which is of the single-pass type o C terminal bind spectrin to cell membrane via protein 4.1 o Contains binding sites for influenza virus and Plasmodium falciparum (parasite that causes malaria) Table above: Just take not that most of the major proteins are peripheral proteins. The only integral proteins are anion exchange protein and glycophorin A, B, C #GrindNation “Strength In Knowledge” BESHYWAP 5 BIOCHEMISTRY Blood Chemistry Dr. Igrobay ABO BLOOD GROUP Blood Group Defined system of RBC antigens (blood group substances controlled by a genetic locus having variable number of alleles Blood Type It is the antigenic phenotype usually recognized by the use of appropriate antibodies ABO substances These are complex oligosaccharides present in most cells of the body and in certain secretions On membranes of the red blood cell, oligosaccharides that determine the specific natures of the ABO substances appear to be mostly present in glycosphingolipids¸ whereas in secretions are present in glycoproteins H substance Also known as H antigen or O antigen or O substance The precursor of both A and B substances The blood group substance found in persons of type O Formed by the action of fucosyltransferase (product of the H gene) which catalyzes the addition of the fucose to the terminal Gal residue of the precursor substance resulting to H substance Antigen Glycosyltransferase Immunodominant Sugar A α-3-N-acetylgalactosaminyltransferase N-acetyl-Dgalactosamine B O α-3-D-galactosyltransferase α-2-L-fucosyltransferase D-Galactose L-Fucose The product of A gene is the GalNac transferase that adds the terminal GalNac (immunodominant sugar of blood group A) to the O substance The product of B gene is the Gal transferase that adds the terminal Gal (immunodomonant sugar of blood group B) to the O substance Individuals with type AB possess both enzymes (GalNac and Gal transferase) and thus have two oligosaccharide chains Individuals of type O apparently synthesize an inactive protein, thus H substance in their ABO blood group substance ABO BLOOD GROUP SYSTEM System was first discovered by Landsteiner in 1900 when investigating the basis of compatible and incompatible transfusion in humans The genes responsible for the production of the ABO substances are present on the long arm of chromosome 9 Three alleles, two of which codominant (A & B) and the third (O) recessive; ultimately determine the four phenotypic produces are: A, B, AB, and O substances Picture Above: The one in the blue box is called the oligosaccharide chain or precursor substance. It is composed of 2 galactose and 1 N-acetylglucosamine linked together by ß1→4 and ß1→3 linkage. With the action of fucosyltransferase, the sugar “fucose” will then be attached to the terminal Gal residue with a α1→2 linkage creating the H substance OLIGOSACCHARIDE SEQUENCE IN RBC MEMBRANE Definition of Terms: Genotype – actual genetic information o AA/AO , BB/BO, OO, AB Phenotype – observed inherited trait o Blood types: A, B, AB, O Bombay (Oh) Phenotype Phenotype: Oh Genotype: hh or H null Inheritance of two recessive h genes Lack of L-fucose which is needed for the attachment of A and B sugars Take note of the structure of each antigens. O antigen has only fucose at the terminal Gal. A antigen has GalNac attached to the terminal Gal with α-1,3 linkage. B antigen has Gal attached to the terminal Gal with α-1,3 linkage #GrindNation “Strength In Knowledge” BESHYWAP 6 BIOCHEMISTRY Blood Chemistry Dr. Igrobay WHITE BLOOD CELLS (LEUKOCYTES) Classified according to the presence of granules (Granulocytes) or absence of granules (Agranulocytes) and their staining characteristics They are formed in the bone marrow and lymphatic tissue with a life span of 13 to 20 days Half of the circulating white cells are granulocytes, the cytoplasm of which contains readily visible granules of various chemical and enzymatic compositions The three main types of granulocytes are the: neutrophils, eosinophils, and basophils The staining characteristics of granules define the cell type: o Neutral staining – neutrophils o Reddish – eosinophils o Bluish – basophils White cells are distinguished from circulating red cells by the presence of a nucleus Automated counting procedures enumerate all nucleated cells as white cells Normal white blood cell count is 4.3-10.8 x 10 (3 µl) ↑ in WBC count is Leukocytosis ↓ in WBC count is Leukopenia Monocytes Have elongated, indented, or dark kidney-bean shaped nuclei Highly phagocytic (cell-eating) Largest WBC (16-20 µm) With delicate nuclear chromatin Constitute 5-8% of circulating blood leukocytes Basophils Least numerous (0.5-1% WBC count) Has large coarse cytoplasmic granules Contains Histamine, Serotonin, Heparin Histamine is responsible for allergic reactions Serotonin is responsible for making you feel sleepy Heparin is an anticoagulant Tissue basophils, not blood basophils, have IgE receptors adherent to cell membranes which react with allergens and IgE to induce release of vasoactive mediators Diapedesis - passage of blood cells through the intact walls of the capillaries, typically accompanying inflammation Neutrophil 55-65% of WBC count Have several lobes in nucleus Present in acute bacterial infection Active Glycolysis Active Pentose Phosphate Pathway Moderate Oxidative phosphorylation Rich in lysosomes and their degradative enzymes (used in killing bacteria and other phagocytosed substances) Unique enzymes: MPO (myeloperoxidase), NADPH oxidase Are recruited from the blood stream into the tissue to help eliminate the foreign invaders via chemotactic factors To reach the tissues, neutrophils must pass through the capillaries by the migration along the blood vessel wall and then adhere to the endothelial lining (Diapedesis) Respiratory Burst – is when neutrophils and other phagocytic cells engulf bacteria, they exhibit a rapid increase in oxygen consumption. This phenomenon produces a large amount of reactive derivatives. Some of these products are potent microbial agents Lymphocytes Has large nuclei with small amount of cytoplasm Smallest WBC (<10 µm in diameter) 25-35% of WBC Circulating blood lymphocytes constitute a tiny fraction (<5%) of the total lymphocyte pool Response in acute infection There are two primary subtypes: o T-lymphocytes o B-Lymphocytes Eosinophils Large, numerous granules Nuclei with 2 lobes 2-5% WBC count Found in lining of respiratory and digestive tracts Important functions involve protection against infections caused by parasitic worms and involvement in allergic reaction Secrete anti-inflammatory substances in allergic reactions Neutrophil in Acute Inflammation: o Entry of activated neutrophils into the tissues o Increased vascular permeability o Activation of platelets o Spontaneous resolution PLATELETS Vary in size from to about 4 µ and circulate for approximately 8-12 days as disc-shaped, anucleate cells Regulation of platelet production is ascribed to thrombopoietin Functions: 1. To protect the vascular integrity of the endothelium 2. Initiate repair when blood vessel walls are damaged Primary Homeostasis – platelet-vessel wall interaction During homeostasis or thrombosis, they become activated & help form hemostatic plugs or thrombi which include 3 major steps: 1. Adhesion to exposed collagen in blood vessels 2. Release (exocytosis) of the contents of their storage granules 3. Aggregation Normal platelet count is 150-350x10 (3) µl Thrombocytopenia is defined as a platelet count < 100,000 µl and causes may be due to production defects, sequestration due to splenomegaly and accelerated destruction Thrombocytosis is platelet count >350,000 µl which could be primary or secondary. Primary thrombocytosis (thrombocythemia) may be complicated by bleeding and/or thrombosis; Secondary rarely causes hemostatic problems. Disorders of platelet function are due to defects in platelet adhesion, aggregation or granule release #GrindNation “Strength In Knowledge” BESHYWAP 7 BIOCHEMISTRY Blood Chemistry Dr. Igrobay Certain Drugs that Inhibit Platelet Responses: Aspirin o Irreversibly acetylates and inhibits the platelet COX-1 involved in the formation of thromboxane A2, a potent platelet aggregator and vasoconstrictor Clopidogrel o Inhibits ADP receptor Abciximab o Interfere with fibrinogen and vWF binding (Von Willenberg Factor binding) HOMEOSTASIS Cessation of bleeding from a cut or severed vessel Process by which body simultaneously stops bleeding from an injured site, yet maintains blood in the fluid state Failure of homeostasis leads to hemorrhage Failure to maintain fluidity leads to thrombosis Homeostatic mechanisms comprise 4 main systems: 1. Vascular system 2. Platelets 3. Coagulation system 4. Fibrinolytic system 3 Phases of Homeostasis and Thrombosis: 1. Formation of loose and temporary platelet aggregate 2. Formation of fibrin mesh 3. Partial or complete dissolution of platelet plug 3 Types of Thrombi: 1. White thrombus – consists of platelets and fibrin, forms in the arteries 2. Red thrombus – consists of red cells and fibrin, forms in veins 3. Fibrin deposits – are common in capillaries Coagulation Cascade Purpose is to generate active serine protease enzyme thrombin In turn acts selectively on the soluble plasma protein fibrinogen, converting it into soluble fibrin Fibrin is the visible end product of coagulation and acts as the cement substance to stabilize the initial primary platelet plug Both Intrinsic and Extrinsic Pathways results in the formation of fibrin Coagulation pathways are complex and involved in many different proteins Proteins can be classified as: o Zymogens of serine proteases o Cofactors o Fibrinogen o Transglutaminase o Regulatory proteins EXTRINSIC PATHWAY (Factors III and VII) Initiation of fibrin clot formation in response to tissue injury (there is damage to the blood vessels or to the endothelial cells) This pathway is quicker than the intrinsic pathway Located in sub-endothelium and on activated monocyte Involves tissue factor, factors VII and X, and Ca2+ and results in factor Xa Formation of complexes between tissue factor and factor VIIa is considered the key process involved in initiation of blood coagulation in vivo #GrindNation “Strength In Knowledge” BESHYWAP 8 BIOCHEMISTRY Blood Chemistry Dr. Igrobay INTRINSIC PATHWAY (Factors XII, XI, IX, VIII) Activated by negatively charged surface in vitro Involves factors XII, XI, IX, VIII as well as prekallikrein, high-molecularweight kininogen, Ca2+ , and phospholipid It results in the production of factor Xa that is cleaved by the tenase complex With factor IXa as the serine protease and factor VIIIa as the cofactor of the intrinsic pathway Can be initiated with the “contact phase” in which prekallikrein, HMW kininogen, factor XII, and factor XI are exposed to a negatively charged activating surface FIBRINOLYTIC PATHWAY Fibrinolysis is one of the natural anticoagulant defense mechanism which is a multi-component enzyme system that results in the generation of an active enzyme plasmin Plasmin is a serine protease mainly responsible for degrading fibrin to fibrinogen, circulates in the form of inactive zymogen, plasminogen, and any small amounts of plasmin that are formed in the fluid phase under physiologic conditions are rapidly inactivated by plasmin inhibitor α2-antiplasmin Plasmin that is bound to fibrin is protected from α2-antiplasmin Other plasmin inhibitors are the plasminogen activator inhibitor and TAFIa Several activators of plasmin are: streptokinase, urokinase, and t-PA COMMON PATHWAY (Factors X, V, II, I, XIII) Both the extrinsic and the intrinsic pathways converge to form the common pathway (via the activation of factor X to Xa), which will ultimately activate the plasma protein prothrombin (factor II) into thrombin (factor IIa). This require the assembly of prothrombinase complex (ionized calcium, prothrombin, factor Va, factor Xa) Thrombin converts fibrinogen to fibrin It also converts factor XIII to factor XIIIa, a highly specific transglutaminase that covalently cross-links molecules, yielding a more stable fibrin clot This fibrin mesh serves to stabilize the hemostatic plug or thrombus #GrindNation “Strength In Knowledge” BESHYWAP 9 BIOCHEMISTRY Blood Chemistry Dr. Igrobay Regulation of Thrombosis: Outside the vascular system, blood can be kept fluid by either removing fibrinogen or by adding anticoagulants, most of which prevent coagulation by chelating or removing calcium ions Citrate, Oxalate, and EDTA are anticoagulants of the chelating category Heparin prevents coagulation by directly inhibiting thrombin; prevents conversion of fibrinogen to fibrin by augmenting a natural anticoagulant molecule, anti-thrombin III to neutralize thrombin Protein C, like vitamin K-dependent coagulation factors, is also a vitamin K-dependent polypeptide manufactured by the liver and circulates in its inactive form. This process is also modulated by an additional substance produced by the blood vessel termed thrombomodulin, which may help focus neutralization at the site of vascular injury. Protein C as an anticoagulant is due to its rapid neutralizing activity of factors VIIIa and Va Protein S accelerates the inactivation of Va and VIIIa by protein C DISORDERS OF COAGULATION & THROMBOSIS Disorders of blood coagulation may either be congenital or acquired in origin Congenital Disorder: o Hemophilia A – deficiency in factor VIII o Hemophilia B- deficiency in factor IX o Von Willebrand’s disease – defect in factor VIII-related antigen produced by platelets and endothelium result in abnormal platelet function Acquired Coagulation Disorder: o Vitamin K deficiency o Liver disease o Rattlesnake bites o Coagulation factor deficiencies due to autoimmune diseases and massive blood transfusion Thrombosis may occur either the venous or arterial system, and the pathogenesis of each is somewhat different o Venous thrombosis involves venous stasis, vascular damage and hypercoagulability o Arterial thrombosis, it may involve platelet-platelet interaction or platelet-vessel wall interaction and thrombin interaction Factors Favoring Thrombotic Tendency Blood stasis Local Factors Vascular damage Unimpeded activation of coagulation – DIC (intravascular thrombin generation) Deficiency of natural anticoagulants Antithrombin III Coagulation-fibrinolytic Protein C & S imbalance Defective fibrinolysis and abnormal plasmin generation Quantitative depletion Qualitative abnormalities Prosthetic valves Increased platelet turnover Valvular heart disease LABORATORY TESTS Closure time/Clotting time o Reflects the time required for the generation of thrombin o If the plasma concentration of prothrombin or of some of the other factors are low (or if the factor is absent, or functionally inactive), clotting time will be prolonged o The expected range for clotting time is 3-6 minutes using slide and capillary method o Looks at overall platelet & vessel wall function aPTT (Activated Partial Prothrombin Time) o Measure of the Intrinsic Pathway and common pathways of coagulation o Monitors heparin toxin o Measures factor I, II, V, VIII, IX, X, XI, XII o Normal activated partial prothrombin time is 30-35 seconds PT (Prothrombin Time) o Measure of the Extrinsic Pathway and common pathways of coagulation o Measures effectivity of anti-coagulants o Measures factors I, II, V, VII, X o Normal prothrombin time is 12-15 seconds Normal Values for Coagulation Studies Clotting time, Lee-White 4-8 mins Activated coagulation (celite) < 100 sec Prothrombin time (PT) 11-13 sec or within 2 sec of control Activated partial prothrombin time 30-40 sec or within 5 sec of control (aPTT) 10-15 sec or within 1.3 times as long Thrombin clotting time (TCT) as control Fibrinogen 150-450 mg/dl Clot dissolution (5-M urea) Clot intact at 1 hr, 24 hr Euglobulin lysis Lysis in 2-6 hrs Fibrinogen degradation products Latex particles < 20 µg/ml Tanned red cells < 5 µg/ml Antithrombin III Coagulation assay > 50% of normal pool Spectrophotometric 85-125% of normal pool REFERENCES Biochemistry Manual (2018) Dr. Igrobay Recordings #GrindNation “Strength In Knowledge” BESHYWAP 10