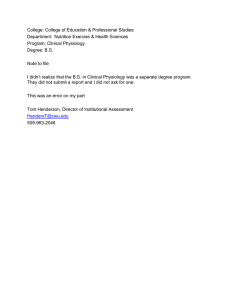
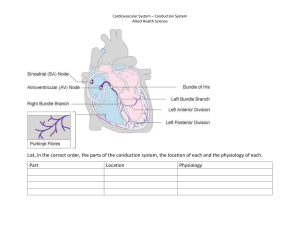
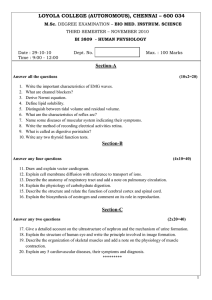
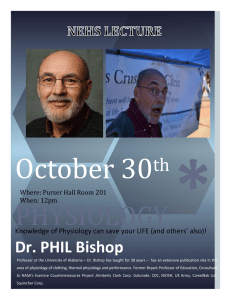
ALTERED COMFORT Donna Woshinsky, MSN RN CNE “PAIN” Class Objectives physiology and classifications of pain pain assessment nursing diagnoses interventions for pain evaluation “Pain is whatever the experiencing person says it is, existing whenever he says it does”. McCaffery, 1979 “Pain is an unpleasant subjective sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” Merskey & Bogduk, 1994 PAIN subjective experience PAIN PHYSIOLOGY nociception neural mechanism by which pain is recognized, transmitted and perceived nociceptors: sensory nerve fibers that transmit pain signals nociceptors densely packed on outer layers of body, more diffuse and unevenly distributed in viscera nociceptors-afferent nerve fibers Nociception: 4 steps PAIN PHYSIOLOGY nociception: transduction transduction PAIN PHYSIOLOGY nociception: transduction Neurotransmitters (biological soup) -bradykinin -cytokines -cox 1 & 2 -prostaglandins -substance P PAIN PHYSIOLOGY nociception: transduction -Inhibit transduction: inhibition of prostaglandin synthesis by blocking action of cyclooxygenase: example: NSAIDs PAIN PHYSIOLOGY nociception: transmission neurotransmitters (prostaglandins, substance P, etc.) cause pain fiber to be depolarized sodium channel activated, generates the action potential A delta and C fibers PAIN PHYSIOLOGY nociception: transmission -Some Drugs inactivate the sodium channel, inhibiting the action potential: Lidocaine, procaine (Novocain) -Some drugs raise threshold for activation (anti-seizure drugs): Lamotrigine (Lamictal) carbamazepine(Tegretol) Gabapentin (Neurontin) PAIN PHYSIOLOGY nociception: transmission Dorsal Horn Synapse: -excitatory neurotransmitters: substance p prostaglandins PAIN PHYSIOLOGY nociception: Gate Theory • another stimulus is able to “close the gate” on the transmission of the pain impulse • Theoretical rationale for acupressure, massage, TENS (transcutaneous electrical nerve stimulation) • Descending impulses from the brain can also open or close the “gate” PAIN PHYSIOLOGY nociception: PERCEPTION -somatosensory cortex: interpretation of pain -RAS: warning individual to attend to pain stimulus -limbic system: emotional aspect to pain -frontal cortex: pain recognition and definition Pain Threshold vs. Pain Tolerance Pain threshold: lowest intensity of a stimulus that causes recognition of pain; experience with pain can lower the threshold. Pain tolerance: Pain level a person can endure; varies person to person, and even in same person under different circumstances. PAIN PHYSIOLOGY nociception: PERCEPTION Opioid analgesics alter the perception and emotional response to pain PAIN PHYSIOLOGY nociception: MODULATION Occurs at any level of pain neural pathway exogenous: medication endogenous: descending inhibitory neural pathways neurotransmitters: serotonin, endorphins, GABA, enkephalins, norepinephrine PAIN PHYSIOLOGY nociceptive process Transduction: pain signal initiated Transmission: pain signal travels to spinal cord, then to thalamus and beyond Perception: pain signal recognized and interpreted by brain Modulation: pain signal inhibited PAIN “A self-limiting phenomenon” Tissue healing and repair Inflammation decreases Breakdown of facilitators and neurotransmitters Modulation via descending inhibitory pathways So why “Chronic Pain”? TYPES OF PAIN by origin Cutaneous Pain Somatic pain Visceral pain Neuropathic pain Malignant pain Cutaneous Pain -Involves superficial structures such as skin, and subcutaneous tissue -sharp, stinging, burning SOMATIC PAIN -Structural pain: bones, muscles, joints, tendons, ligaments -well localized -achy, dull, throbbing -Massage, heat, cold all mechanisms for relief Radiating Pain Starts at pain origin, extends to other locations Patient can locate origination and points of extension VISCERAL PAIN -Originates from viscera -not well localized -result of stretching, distention, ischemia or inflammation of internal organs -deep, cramping, pressure -can be referred to distant sites REFERRED PAIN •Pain fibers from viscera and neural touch fibers synapse onto wide dynamic range neurons in dorsal horn •when signal transmitted to brain, brain presumes pain signal came from area innervated by the neural touch fibers REFERRED PAIN Radiating vs referred pain NEUROPATHIC PAIN -Source of pain is nerve damage -nerve fiber has reduced firing threshold-hyperexcitable -cross-over of touch fibers possible -example: phantom limb pain -burning, searing, tingling, numbness, “pins and needles” NEUROPATHIC PAIN ALLODYNIA – normally non-painful stimulus causes pain HYPERALGESIA – increased pain response to mildly noxious stimuli MALIGNANT PAIN (Intractable Pain) -Often mix of visceral, somatic, and neuropathic -results from tumor, pressure, inflammation, side effects of treatment -overwhelming, all-consuming TYPES OF PAIN by duration Acute pain- Rapid onset, disappears when underlying cause resolved Chronic pain-persists beyond normal healing period ACUTE PAIN -guarding, wincing, moaning, crying -elevated BP, pulse, respiratory rate -pallor, diaphoresis -anxiety -mask of pain Anxiety and worry -usually aggressively managed -ex. post-surgical pain CHRONIC PAIN -may have no outward manifestations -normal vital signs -slackened facial features, flattened affect -social isolation, decreased engagement with usual activities of daily living, fatigue, depression, hopelessness possible -sometimes unknown source -unpredictable course ASPECTS OF THE PAIN EXPERIENCE physiological emotional behavioral cognitive FACTORS AFFECTING THE PAIN EXPERIENCE AGE (developmental level) Misconception: infants do not feel pain, or, do not feel as intense pain as older children and adults Fetus: neural mechanism for processing pain stimuli fully developed by mid to late gestation Inadequately controlled pain in infancy/childhood may lead to decreased pain tolerance in adulthood. FACTORS AFFECTING THE PAIN EXPERIENCE Elderly no scientific evidence pain sensitivity decreases with age elderly tend to underreport pain elderly have learned coping mechanisms for pain FACTORS AFFECTING THE PAIN EXPERIENCE opioid use in elderly elderly as group fear addiction healthcare workers fear side effects ”start low, go slow” long acting opioid preparations, patches or pills, used with adjuvants, can be very successful FACTORS AFFECTING THE PAIN EXPERIENCE CULTURE Acceptable means of expressing pain are learned FACTORS AFFECTING THE PAIN EXPERIENCE ANXIETY pain can cause anxiety anxiety may activate physiological mechanisms that facilitate pain signal transmission anxiety decreases pain tolerance NURSING PROCESS RELATED TO PAIN: ASSESSMENT -assess when behavioral manifestations of pain -assess when pain is suspected and patient cannot or will not express pain -do not make assumptions -caution: patients may use alternative terminology NURSING PROCESS RELATED TO PAIN: ASSESSMENT Onset and duration location intensity quality Pattern (chronology) Aggravating/alleviating factors associated symptoms PAIN INTENSITY PAIN INTENSITY NURSING PROCESS RELATED TO PAIN: ASSESSMENT Onset and duration location intensity quality Pattern (chronology) Aggravating/alleviating factors associated symptoms NURSING PROCESS RELATED TO PAIN: ASSESSMENT Assess the effect of the pain on the patient physiologically, emotionally, behaviorally physiological signs of pain anxiety depression coping ability ability to manage ADL behaviors, and ability to socialize SPECIAL ASSESSMENT INFANTS CRIES assessment tool crying requires oxygen increased vital signs expressions sleeplessness SPECIAL ASSESSMENT IMPAIRED ELDERLY APP, utilize input of family observe and score behaviors change in behavior, particularly restlessness, withdrawal, or decreased mobility change appearance change in vocalizations Agitation, aggression SPECIAL ASSESSMENT: FLACC - NURSING DIAGNOSIS Acute Pain (incisional) r/t tissue trauma secondary to surgery AEB client states incision pain is “8” Chronic Pain (joint) r/t inflammation of joints secondary to rheumatoid arthritis AEB client states “I’ve had this pain for years.” Anxiety r/t perceived threat to biological integrity AEB client stating “it hurts so much to move, something must be wrong!” NURSING DIAGNOSIS Insomnia r/t difficulty assuming usual sleep position secondary to pain AEB client states “I always sleep on my side, but it hurts too much to turn that way”. Self care deficit bathing r/t post-op pain AEB client stating “I am in too much pain to wash up. I’ll do it tomorrow.” Impaired Mobility r/t pain AEB client stating “I don’t want to walk, my leg hurts too much.” PLANNING Overall goal in pain management: Patient will have maximal pain relief and quality of life. PLANNING GOALS -Patient will report reduced pain intensity and quality within 2 hours. -Patient will demonstrate use of behavioral techniques to reduce pain by (date). -Patient will recognize causal factors for pain and use measures to modify these by (date) INTERVENTIONS Non-pharmacological (complementary) -comfort measures -distraction: music, Lamaze -guided imagery -relaxation/meditation -mindfulness-based stress reduction -cutaneous stimulation INTERVENTIONS heat and cold TENS- transcutaneous electrical nerve stimulation Disturbed Energy Field Therapeutic Touch, Reiki techniques to rebalance, or unblock the flow of Chi W.H.O. ANALGESIC LADDER FREEDOM FROM PAIN STRONG OPIOID + NONOPIOID + ADJUVANT PAIN PERSISTING OR INCREASING WEAK OPIOID+ NON-OPIOD+ ADJUVANT PAIN PERSISTING OR INCREASING NON-OPIOID+ ADJUVANT PAIN WHO ANALGESIC LADDER EVALUATION Does the patient have maximal pain relief? Revisit assessment: assess intensity, quality, associated symptoms, level of activity If necessary, revise plan, try other interventions, report to MD