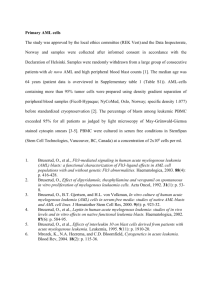
Introduction: Hematopoietic Neoplasms (Acute Leukemia) 1 2 Introduction: Hematologic Neoplasm • Dysregulated Proliferation • Benign • Differentiated cells, organized growth • Does not spread • Malignant • Anaplastic, proliferating cells (clones of abnormal cells) • Often metastasizes (characteristically) 3 WHO Classification of Hematologic Neoplasms • Select Diseases • Myeloproliferative neoplasms (MPNs) • Acute myeloid leukemia (AML) and related neoplasms • Precursor Lymphoid Neoplasms (B & T lymphoblastic leukemia/lymphoma) • Mature B cell neoplasms (including chronic lymphocytic leukemia, CLL) 4 Molecular Basis of Cancer • Oncogenes • Proto-oncogene Oncogene • Proto-oncogenes • Growth factors • Growth factor receptors • Proteins involved in signal transduction • Signal transducers • Transcription factors 5 Molecular Basis of Cancer • Tumor suppressor genes • Code for proteins that inhibit cell growth in normal cells (p53 & RB) • Mutations lead to loss of function • loss of protein’s normal, growth inhibitory effect • Example: Mutation of p53 • Loss of function of p53 allows damaged cells to proceed through cell cycle • Unregulated proliferation of the damaged cell 6 Molecular Basis of Cancer • Epigenetics • Heritable changes in gene expression not caused by changes in DNA sequence • Epigenetic changes • DNA methylation of CpG dinucleotides • Transcriptional silencing of a gene as a result of hypermethylation of CpG dinucleotides in the gene’s promoter region • Histone deacetylation • Hypo-acetylated histones bind tightly to phosphate backbone of DNA and chromatin remains in its heterochromatin state – genes are silenced 7 Leukemogenesis • Genetic susceptibility -> Down’s Syndrome • Somatic mutation • Ionizing radiation • Drugs • Chemicals • Viral infection • Immunologic dysfunction • Other factors • Secondary to treatment for primary disease • Other hematologic disease (e.g., PNH) 8 WHO Classification of Hematologic Neoplasms • Morphology • Cytochemical stains • Immunophenotyping • Detection of genetic abnormalities 9 Cytochemical Reactions 10 Myeloperoxidase (MPO) Benzidene dihydrochloride + H2O2 MPO Oxidized benzidene + H2O • Positive in myeloblasts • Negative in lymphoblasts 11 Immature myeloid cells demonstrating MPO positivity 12 Auer Rods 13 Sudan Black B (SBB) • Diazo dye – fat soluble dye • Soluble in cellular lipids • Phospholipids, neutral fats, and sterols • Parallels MPO 14 Immature myeloid cells demonstrating SBB positivity 15 Non-specific Esterase (NSE) naphthyl acetate NSE naphthol + acetate Diazonium salt colored product • Found in monocytes and macrophages • Can inactivate the enzyme in monocytes by adding sodium fluoride to incubation mixture 16 Immature monocytic cells demonstrating NSE positivity 17 Periodic Acid Schiff (PAS) Stains glycogen and polysaccharides Positive in mature neutrophils, monocytes, platelets, megakaryocytes Positive in erythroleukemia (malignant erythroblasts) 18 Malignant erythroblasts demonstrating PAS positivity 19 20 Acute Myeloid Leukemias 21 FAB Classification 22 Acute Myeloid Leukemia • General Findings: • More common in adults • Clinical presentation: pallor, weak, tired, bone pain • Laboratory presentation (general): • thrombocytopenia, variable WBC count, anemia, • Bone marrow – hypercellular • >20% blasts • Auer rods • MPO & SBB positive blasts 23 Figure 2. A high power view cofirms these cells as blasts Maslak, P. ASH Image Bank 2004;2004:101032 24 Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. Figure 3. Other marrow elements are sparse Maslak, P. ASH Image Bank 2003;2003:100838 25 Copyright ©2003 American Society of Hematology. Copyright restrictions may apply. Figure 1. An Auer rod (arrow)is appreciated in this blast from a bone marrow aspirate of a patient with AML Maslak, P. ASH Image Bank 2002;2002:100454 26 Copyright ©2002 American Society of Hematology. Copyright restrictions may apply. A differential report notes the presence of more than 20% blasts. This number supports the diagnosis of: A. CML B. AML C. CLL D. MDS 27 An Auer rod is best described as: A. Threads of chromosomal DNA found within the cytoplasm B. Inappropriately fused primary granules C. Excessive accumulations of ribosomal RNA D. Golgi apparatus that have not been enzymatically degraded 28 WHO Classification of Acute Myeloid Leukemias • AML with recurrent genetic abnormalities • AML with myelodysplasia-related changes • Therapy-related myeloid neoplasms • AML not otherwise categorized • Myeloid sarcoma • Myeloid proliferations related to Down syndrome https://ashpublications.org/blood/article/127/20/2391/35255/The2016-revision-to-the-World-Health-Organization 29 Acute Myeloid Leukemia • AML not otherwise categorized • Acute myeloid leukemia without maturation • One of most common in adults • Bone marrow • >90% of non-erythroid cells are blasts • Maturation beyond blast stage is <10% • MPO and SBB positivity in >3% blasts 30 Figure 3. Multiple small nucleoli are apparent in these blasts Maslak, P. ASH Image Bank 2004;2004:101032 PB: AML without maturation Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. 31 Figure 1. Bone marrow aspirate shows increased blasts Maslak, P. ASH Image Bank 2002;2002:100473 BM: AML without maturation Copyright ©2002 American Society of Hematology. Copyright restrictions may apply. 32 Acute Myeloid Leukemia • AML with recurrent genetic abnormalities • Acute myeloid leukemia with t(8;21)(q22;q22) • Peripheral blood: observe pseudo Pelger-Huet cells • Bone marrow: 30-90% blasts 33 Acute Myeloid Leukemia • AML with recurrent genetic abnormalities • Acute myeloid leukemia with t(8;21)(q22;q22) • Peripheral blood Hyposegmentation 34 Hypogranulation Figure 1. Blasts are increased but other myeloid elements are present as well (MacNeal Tetrachrome 400x) Maslak, P. ASH Image Bank 2002;2002:100480 BM: AML with t(8:21) Copyright ©2002 American Society of Hematology. Copyright restrictions may apply. 35 Figure 7. Diagrammatic representation of balanced translocation which defines this distinct biologic AML subtype Maslak, P. ASH Image Bank 2001;2001:100215 Cytogenetic analysis: t(8;21) Copyright ©2001 American Society of Hematology. Copyright restrictions may apply. 36 Acute Myeloid Leukemia • AML with recurrent genetic abnormalities • Acute myeloid leukemia with t(8;21)(q22;q22) • Genes involved • Chr 8: RUNX1T1 (also called ETO) • Chr 21: RUNX1 (formerly AML1) • Hybrid gene: ETO/RUNX1 • Fusion protein = ETO/RUNX1 • acts as transcriptional repressor because fusion protein can’t bind to DNA and promote transcription of genes/proteins that promote cellular differentiation • Net effect: cell differentiation is blocked and proliferation of leukemic cells is increased 37 Acute Myeloid Leukemia/ APL • AML with recurrent genetic abnormalities • Acute myeloid leukemia with PML-RAR • Predominantly malignant promyelocytes present • Possess multiple auer rods (faggot cells) • Common complication: disseminated intravascular coagulation (DIC) • Two types: • Hypergranular: folded or bilobed nucleus • Microgranular: WBC markedly increased; multilobed nucleus 38 Figure 1. Peripheral smear from a 15 year old male shows blast-like cells with agranular cytoplasm and convoluted nuclei Lazarchick, J. ASH Image Bank 2004;2004:101007 Microgranular Variant Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. 39 Figure 4. The "bi-lobed" nuclear morphology typical of hypogranular promyelocytes is seen in this view Lazarchick, J. ASH Image Bank 2004;2004:101007 PB: Microgranular Variant Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. 40 Figure 5. A low power view (H&E 4x) of the marrow shows essentially 100% cellularity with an apparent monomorphic infiltrate Lazarchick, J. ASH Image Bank 2004;2004:101007 41 Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. Figure 7. Another view of the same biopsy illustrating the nuclear abnormalities previously described Lazarchick, J. ASH Image Bank 2004;2004:101007 42 Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. Figure 1. This cell found in the bone marrow of a patient with APL contains multiple Auer rods in the cytoplasm Maslak, P. ASH Image Bank 2002;2002:100587 Faggot cell Copyright ©2002 American Society of Hematology. Copyright restrictions may apply. 43 Figure 3. Promyelocytes are heavily granulated Maslak, P. ASH Image Bank 2004;2004:101126 Hypergranular variant Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. 44 Acute Myeloid Leukemia • AML with recurrent genetic abnormalities • Acute myeloid leukemia with PML-RAR • First identified mutation: t(15;17)(q22;q21) • Genes involved • Chr 15: PML = promyelocytic leukemia gene • Chr 17: RAR = retinoic receptor gene • Hybrid gene: PML/RAR 45 A laboratory professional reviewed the CBC of a patient who had a WBC count of 5 × 103/μL with 32% blasts present. Follow up testing with cytogenetics revealed t(15;17)(q22;q12). Which of the following is a likely diagnosis for the patient? A. APL B. MDS C. MPN D. CLL 46 The leukemia that belongs to the WHO classification of AML with recurrent genetic abnormalities is: A. APL with PML-RARA B. Megakaryoblastic leukemia C. Pure erythroid leukemia D. AML minimally differentiated 47 Figure 8. Diagram of the t(15;17)(q22;q21) rearrangement that characterizes classic APL Maslak, P. ASH Image Bank 2004;2004:101126 48 Copyright ©2004 American Society of Hematology. Copyright restrictions may apply. Acute Myeloid Leukemia • AML with recurrent genetic abnormalities • Acute myeloid leukemia with PML-RAR • Hybrid gene: PML/RAR • Fusion protein = PML/RAR • Binds to RA-responsive elements of specific target genes & forms complex with RXR protein • Complex recruits corepressor proteins and deacetylates histones; thus prevents transcription of specific target genes and blocks granulocytic differentiation • Unlike normal RAR protein, physiologic levels of RA can’t induce conformational change in fusion protein and release corepressor molecules and activate gene transcription • Net effect: granulocytic differentiation is blocked • Specific therapeutic intervention 49 Predict the typical platelet concentration of a patient with AML. A. Marked decreased B. Marked increased C. Normal D. Cannot be determined 50 A PAS stain is ordered on a leukemic patient. The test is performed, and the technologist confirms that the PAS stain is positive with coarse granularity. Based on these findings, from what is the patient most likely suffering? A. Acute myelomonocytic leukemia B. Acute erythroleukemia C. Acute megakaryoblastic leukemia D. AML with minimal differentiation 51 Acute Lymphoblastic Leukemias PRECURSOR LYMPHOID NEOPLASMS 52 Acute Lymphoblastic Leukemia • General Findings • Found primarily in young children (2-5 yr) • Clinical presentation: easy bruising, fatigue, weight loss, fever, bone pain • Laboratory Presentation • Peripheral blood: >50% of cases have increased WBC, thrombocytopenia, anemia • Bone marrow: >20% lymphoblasts • lymphoblasts: MPO & SBB negative 53 Figure 1. Cluster of blasts from a patient with ALL have a regular appearance and are devoid of granules in the cytoplasm (MacNeal Tetrachrome 1000x) Maslak, P. ASH Image Bank 2002;2002:100384 54 Copyright ©2002 American Society of Hematology. Copyright restrictions may apply. Figure 3. Bone marrow aspirate reveals increased blasts and immature lymphocytes (400X MacNeal tetrachrome) Maslak, P. ASH Image Bank 2002;2002:100400 55 Copyright ©2002 American Society of Hematology. Copyright restrictions may apply. WHO Classification of Lymphoid Leukemias/Lymphomas • Precursor Lymphoid Neoplasms • B Lymphoblastic leukemia/lymphoma • B Lymphoblastic leukemia/lymphoma with recurrent genetic abnormalities • B Lymphoblastic leukemia/lymphoma not otherwise categorized • T Lymphoblastic leukemia/lymphoma 56 Precursor Lymphoid Neoplasms • B Lymphoblastic Leukemia with recurrent genetic abnormalities • B lymphoblastic leukemia with t(12;21) • Bone Marrow • hypercellular • greater than 20% blasts • Cytochemical stains • MPO: blasts are negative • SBB: blasts are negative 57 B Lymphoblastic Leukemia with recurrent genetic abnormalities • B lymphoblastic leukemia with t(12;21) • Bone Marrow 58 B Lymphoblastic Leukemia with recurrent genetic abnormalities • B lymphoblastic leukemia with t(12;21) • What would immunophenotyping by flow cytometry reveal? CD 34 CD 19 + Tdt HLA-DR CD 10 + Cytoplasmic CD 3 CD 33 CD 20 = CD 2 Cytoplasmic μ + CD 5 CD 13 + + CD 14 CD 22 CD 7 CD 61 CD 24 CD 4 CD 25 CD 8 + 59 Which of the following laboratory results are most commonly found in ALL? A. Eosinophilia & basophilia B. Neutropenia & thrombocytopenia C. Neutrophilia & thrombocytopenia D. Lymphocytosis & thrombocytosis 60 61