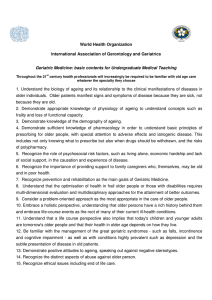
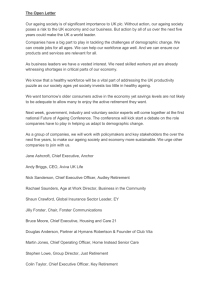
JEADV DOI: 10.1111/j.1468-3083.2010.03963.x REVIEW ARTICLE Skin ageing E. Kohl,†,* J. Steinbauer,† M. Landthaler,† R.-M. Szeimies‡ † Department of Dermatology, Regensburg University Hospital, Regensburg, and ‡Department of Dermatology and Allergology, Hospital Vest, Recklinghausen, Germany *Correspondence: E. Kohl. E-mail: elisabeth.kohl@klinik.uni-regensburg.de Abstract Similar to the entire organism, skin is subject to an unpreventable intrinsic ageing process. Additionally, skin ageing is also influenced by exogenous factors. Ultraviolet radiation in particular results in premature skin ageing, also referred to as extrinsic skin ageing or photoageing, which is the main cause of the changes associated with the ageing process in sun-exposed areas. Despite their morphological and pathophysiological differences, intrinsic and extrinsic ageing share several molecular similarities. The formation of reactive oxygen species and the induction of matrix metalloproteinases reflect the central aspects of skin ageing. Accumulation of fragmented collagen fibrils prevents neocollagenesis and accounts for the further degradation of the extracellular matrix by means of positive feedback regulation. The importance of extrinsic factors in skin ageing and the detection of its mechanisms have furthered the development of various therapeutic and preventive strategies. Received: 13 May 2010; Accepted: 14 December 2010 Keywords extrinsic skin ageing, intrinsic skin ageing, matrix metalloproteinases, photoageing, retinoids, UV radiation Conflict of interest None declared. Introduction Skin ageing, a highly complex but not yet fully understood process, is particularly interesting because of the continuously increasing life expectancy in many countries. Several theories have been developed to comprehend this progressive process. Ageing may be considered as the accumulation of different deleterious changes in cells and tissues. These changes may progressively impair biological functions, increase the risk of developing diseases and ultimately lead to death.1 Up to now, no integrative concept exists connecting the ageing models evolved so far. Intrinsic and extrinsic skin ageing Pathomechanisms of intrinsic skin ageing Intrinsically aged skin is usually found in sun-protected areas. Photoageing may be considered a superposition of chronological skin ageing by UV-radiation. Skin may serve as a model organ for investigating both endogenous and exogenous ageing models. Extrinsic and intrinsic skin ageing show similarities in molecular mechanisms. The following aspects are discussed in several theories on intrinsic skin ageing: Cellular ageing (Hayflick-Limit) and shortening of telomeres, mutations of mitochondrial DNA, oxidative stress, JEADV 2011, 25, 873–884 genetic mutations and decrease of several hormone levels.2 According to the free radical theory of ageing, reactive oxygen species (ROS), primarily arising from oxidative cell metabolism, play a major role in both chronological ageing and photoageing.3 Despite several antioxidative mechanisms, which deteriorate with increasing age, abound ROS damage cellular components. This damage leads to increasing ROS and decreasing antioxidative capacities and finally to cellular ageing.2,4 ROS in extrinsic and intrinsic skin ageing may be assumed to induce the transcription factor c-Jun via MAPK (mitogen-activated protein kinases). This induction activates the decisive transcription factor AP-1 (activator protein 1), leads to the expression of matrix metalloproteinases MMP-1 (interstitial collagenase), MMP-3 (stromelysin 1), and MMP-9 (gelatinase b) and prevents the expression of procollagen1.5 In accordance with these results, elevated levels of partially degraded collagen are present in intrinsically aged skin similar to photoaged skin. Recently, an in vivo study has indicated that reduced expression of the connective tissue growth factor (CTGF) and reduced transforming growth factor (TGF)-b ⁄ Smad signalling are probably responsible for the loss of type I procollagen expression in intrinsically aged skin.6 Intrinsic skin ageing is strongly influenced by hormonal changes.7 Production of sex hormones in the gonads, the pituitary, ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Kohl et al. 874 and adrenal glands already gradually declines in the mid-twenties. Oestrogens and progesterone decay in line with the menopause. In particular, the deficiency in oestrogens and androgens cause dryness, wrinkling, epidermal atrophy, collagen breakdown and loss of elasticity.8,9 mutations of mitochondrial DNA lead to dysfunctional oxidative phosphorylation. Thus, more ROS are generated, causing even more mutations.15 A causative relationship must be assumed for the depletion of mitochondrial DNA, resulting in oxidative stress and increased expression of MMP-1.16 Pathomechanisms of photoageing Role of telomeres Telomeres consisting of 1000-fold tandem repeats of TTAGGG in humans form the chromosome ends. Telomeres do not encode any gene products and constitute the last 7000–12 000 base pairs. Telomere length varies with species and decreases with increasing age.17 Telomeres consist of a double-strand region composed of TTAGGG repeats and a much shorter single-strand 3¢ overhang at the distal end. Telomeres form a 3-dimensional structure (t-loop) that is required for telomere capping. The t-loop is secured by insertion of the 3¢ overhang into the proximal double-stranded DNA. T-loops prevent the chromosome ends to be recognized as double-strand breaks, defending them from instability as a fusion of chromosomes. A complete replication of the final bases by DNA-polymerase is not possible. For this reason, telomeres shorten with each cell division by approximately 100 base pairs.18 Therefore, the number of cell divisions is confined to 50–70 because of critical telomere shortening.19 Critical shortening of telomeres induces disruption of the t-loop configuration, exposing the 3¢ overhang. This process initiates DNA-damage response, entailing to apoptosis, senescence or cell cycle arrest.20 Besides shortening telomeres with each round of cell division, UV-radiation or other DNA-damage may lead to loop disruption, exposing the TTAGGG tandem repeat sequence. This process elicits the above-mentioned DNA-damage response, indicating the possible existence of a common mechanism for intrinsic ageing and photoageing.21 UV-exposure particularly damages telomeres because of their higher number of TT- and G-bases compared with the other part of the chromosome. UV-radiation particularly targets TT- and G-bases, possibly destabilizing the t-loop configuration and activating the common signalling pathway.22 The impact of telomeres on the aetiopathology of photoageing was also put into question.23 Telomere lengths in photoaged and photoprotected skin did not differ; altogether, telomere length was shorter in the epidermis than in the dermis.24 Expression of telomerase is maintained in early embryonic, malignant and germ cells. Telomerase acts as a maintenance mechanism of telomere length, synthesizing TTAGGG sequences.23 Contrary to most somatic cells, expression of telomerase is maintained in the hematopoietic system and in the gastrointestinal tract. Evidence suggests expression of telomerase in the keratinocytes of rapidly regenerating epidermis.25 The epidermis in situ showed a mean telomere loss of 25 bp per year. A telomerase-based mechanism to maintain telomere length in keratinocytes must be assumed because of the high proliferation rate of keratinocytes in contrast to slowly Extrinsic skin ageing primarily arises from UV-light exposure. Approximately 80% of facial skin ageing is attributed to UV-exposure.10 Further relevant exogenous factors are exposure to tobacco smoke, airborne particulate matter, infrared radiation, ozone and malnutrition. Premature skin ageing or photoageing are synonyms for extrinsic skin ageing. The biological effects of UV-radiation are based on light absorption in chromophores and the subsequent conversion of energy in chemical reactions. UVA ⁄ UVB-radiation contribute to biological effects, resulting in skin ageing and photocarcinogenesis. The exact action spectrum, i.e., the biological effects depending on wavelengths, remains unclear. Short wave UVB is mainly absorbed in the epidermis, generating DNA-damage by forming photocarcinogenic cyclobutane pyrimidine dimers (CPDs) and 6,4-photoproducts. UVA-light is absorbed by cellular chromophores, such as urocanic acid, melanin precursors and riboflavin. These lightexposed chromophores generate ROS, which damage lipids, proteins and DNA. UVA-light is exceptionally relevant in photoageing because of its high penetration depth.11 Mutations of mitochondrial DNA The main endogenous source of ROS is mitochondria, and ROS are built from approximately 1% of the oxygen consumed in the mitochondria. ROS, in addition to their physiological role as signalling molecules, lead to oxidative stress after exhaustion of cellular defence mechanisms. Because of their proximity, ROS generated in the respiratory chain are particularly important for mitochondrial (mt) DNA. The human mtDNA consists of up to 10 copies of a double-stranded circular DNA-molecule comprising 16 559 base pairs, which encodes proteins of the respiratory chain. mtDNA shows considerably higher mutation rates than nuclear DNA because of its inefficient recognition and repair mechanisms.12 Mutations of mitochondrial DNA are important for ageing processes, photoageing and various neurological diseases. Photoaged skin shows more mutations in mtDNA than sun-protected skin.13 The most frequent mitochondrial mutation is a large-scale 4977 base-pair deletion termed ‘common deletion’, whose induction is directly related to chronic UVA-exposure. In vivo repetitive exposure of previously unirradiated skin to physiological doses of UVA-light increased the level of common deletion in human skin by 40%. The 4977 bp-deletions persisted and were detectable even months after cessation of irradiation. The levels of common deletion continued to increase and partly showed an up to 32-fold accumulation 16 months after irradiation.14 These observations are in accordance with the theory proposing that ROS-induced JEADV 2011, 25, 873–884 ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Skin ageing 875 proliferating fibroblasts with a reported telomere loss of 25 bp per year. The evidence for functionally active telomerase in human epidermis and the lack of considerable telomere loss of keratinocytes and fibroblasts suggest that telomere loss does not play a key role in intrinsic skin ageing.23 Matrix metalloproteinases and signal transduction pathways As a major structural protein of the extracellular matrix (ECM), type I collagen is secreted by fibroblasts, forming more than 90% of the dry weight of the dermis. Besides, MMPs are secreted, hydrolyzing ECM proteins, such as collagen fibres. After exposure to suberythematous UVB-doses, sustained elevations of MMPs were assessed.26 MMP-1 initiates cleavage of type I collagen and is thus particularly important for degrading the ECM. Additionally, UV-exposure involves considerably decreased collagen production. Photoaged skin is designated with a collagenous matrix fragmented by MMPs. UV-induced oxidative stress initiates signalling cascades via the activation of several cell surface receptors. This activation results in the degradation of the ECM and in the down-regulation of neocollagenesis. Receptor activation effects stimulation of MAP-kinases p38, JNK (c-Jun amino-terminal kinase), and ERK (extracellular signal-regulated kinases), consequently inducing the transcription factor AP-1. AP-1 induces collagen degradation by up-regulation of MMP-1, MMP-3 and MMP-9.26 In addition, procollagen synthesis is inhibited by the UV-induced transcription factor AP-1. Increased transcription of AP-1 inhibits the effects of TGF-b (transforming growth factor b), a cytokine promoting collagen production.27 Extracellular matrix degradation is further enhanced by UV-induced activation of the transcription factor NF-jB. This factor stimulates the expression of MMPs and several cytokines and enforces UV-response by activating respective cell surface receptors. UV-induced elevated levels of MMPs are not accompanied by the compensatory augmented production of their physiological inhibitors, the TIMPs (tissue inhibitor of matrix metalloproteinases). Induction of MMPs may be effected by UVA and UVB.28 Expression of MMP-1, MMP-3 and MMP-9 occurs in both keratinocytes and fibroblasts. In vivo studies have shown that MMPs in UV-exposed skin (solar simulated UV irradiation) primarily derive from epidermal keratinocytes and diffuse into the dermis; here, they bind directly to ECM.29 Mechanical tension and ECM Loss of mechanical tension contributes to molecular changes detectable in aged skin. Beyond the cellular ageing process of fibroblasts, reduced neocollagenesis may be ascribed to the reduced mechanical stimulation of fibroblasts. In aged skin, fibroblasts collapse because of the loss of mechanical tension caused by the accumulation of fragmented collagen and concomitant loss of binding sites between intact collagen and fibroblasts. This process concurs with an increase in MMPs, the intracellular oxidative level, protein oxidation, the transcription factor AP-1 and with a reduction of collagen production, resulting JEADV 2011, 25, 873–884 in a self-perpetuating cycle (see Fig. 1).30 Degradation of elastic fibres is also relevant in skin ageing processes and particularly in wrinkle formation. The findings obtained in animal experiments suggest repetitive UVB-exposure as a cause of wrinkle formation through loss of skin elasticity. The expression of fibroblast elastase is stimulated by UVB-induced cytokine secretion of keratinocytes. Up-regulated activity of fibroblast elastase damages elastic fibres facilitating wrinkle formation.31 Within the framework of UV-exposure (solar simulated UV irradiation), infiltrating neutrophil granulocytes release MMP-1, MMP-8 (neutrophil collagenase), MMP-9 and neutrophil elastase and participate in the degradation of the ECM. Neutrophil granulocytes are assumed to play a critical role in the pathogenesis of photoageing.32 Vascular alterations Skin ageing also involves alterations of dermal vascularization. In the papillary dermis of photoaged skin, both vessel size and density are significantly decreased. However, intrinsically aged skin only shows a decrease in vessel size because the density of dermal blood vessels is age-independent.33 Imbalance of the angiogenesis inhibitor thrombospondin-1 (TSP-1) and the vascular endothelial growth factor (VEGF) is of particular importance in UV-induced vascular changes. Acute Figure 1 This model schematically depicts factors of pathogenic relevance for skin ageing. The induction of matrix metalloproteinases is of particular importance as they degrade collagen and other components of the extracellular matrix (ECM). Mainly UVinduced reactive oxygen species (ROS) and DNA damage lead to increased induction of matrix metalloproteinases in keratinocytes and fibroblasts. Proteolytic enzymes such as elastase and matrix metalloproteinases derived from neutrophil granulocytes contribute to the degradation of the ECM. Besides, UV-exposure directly stimulates the production of elastase in fibroblasts. As a result, partially degraded collagen and reduced mechanical tension of fibroblasts inhibit neocollagenesis. Reduced mechanical tension leads to further production of ROS, which again results in increased expression of matrix metalloproteinases. ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Kohl et al. 876 UVB-irradiation results in pronounced generation of immature vessels, possibly arising from the down-regulation of TSP-1 and the up-regulation of VEGF.34 UVB-irradiated transgenic mice with overexpression of TSP-1 showed decreased skin vascularization as well as reduced wrinkle formation compared with the control group.35 The causes of the aforementioned reduction of dermal vessels in photoaged skin in contrast to the proangiogenic effects of acute UV-exposure require further investigations. Altered ECM in photoaged skin is assumed to allow the regression of dermal vessels.33 Protein oxidation Ageing cells show accession of oxidized proteins and consequently declining proteasome activities.36 Activity of the proteasome, a multicatalytic protease that degrades oxidized proteins, declines with age.37 Protein oxidation results from UV-induced depletion of antioxidant enzyme expression. The epidermis of photodamaged skin shows significantly lower levels of antioxidant enzymes than photoprotected skin. As the levels of antioxidant enzymes in the dermis are considerably lower than those in the epidermis, photoaged skin shows accumulation of oxidized proteins in the upper dermis. In combination with the lower proliferative activity of fibroblasts compared with that of keratinocytes, the low enzyme levels may explain the pattern of distribution of oxidized proteins.37 Accumulation of oxidized and cross-linked proteins results in the aggregation of proteins and lipofuscin, progressively inhibiting all proteasome activities. The quantity of dermal oxidized proteins correlates well with the severity of the clinical features of photoageing.37 Figure 2 Deep furrows, solar elastosis, focal hypopigmentation and solar lentigines in the face of a 66-year-old patient with Fitzpatrick’s skin type II. Clinical and histological changes in intrinsically and extrinsically aged skin Intrinsically aged skin is uniformly pigmented, showing loss of elasticity, cigarette paper-like wrinkling, and rarefied hair follicles, sweat glands and sebaceous glands. The cumulative UV-dose and the Fitzpatrick skin type assign the degree of sun-induced cutaneous changes. People with skin types I and II show atrophic skin changes with focal depigmentation, epidermal atrophy, ephelides and pseudoscars and may develop malignant or non-malignant skin cancer. By contrast, people with skin types III and IV show diffuse irreversible hyperpigmentation, leathery appearance, deep wrinkles and lentigines (Figs 2–4). Because of the distinct extension of cell cycles, the epidermis is renewed much slower in elderly people. The epidermal turnover rate is up to 50% lower in the eighth decade of life. Moreover, intrinsically aged skin shows epidermal atrophy, which particularly affects the stratum spinosum, ranging from 10% to 50%.38 From the age of 30 onwards, the number of melanocytes abates by 8% to 20% per decade.39 The notably fewer Langerhans cells present show morphological alterations and are functionally impaired. The dermis of photoprotected aged skin shows fewer JEADV 2011, 25, 873–884 Figure 3 Deep perioral wrinkles of the same patient with a 10-year history of smoking cigarettes. mast cells and fibroblasts than photoprotected young skin, and collagen fibres and elastic fibres are rarefied.40 Collagen synthesis declines by 30% in the first 4 years of menopause, then by 2% annually.41 The epidermis in sun-exposed areas is thicker than in intrinsically aged skin, whereas severe photodamage elicits epidermal ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Skin ageing 877 Similar to UV-radiation, IRA is capable of inducing ECM degradation, thus accelerating the skin ageing process. Already in 1982 was exposure to IRA found to result in dermal damage, resembling solar elastosis.47 IRA radiation causes ROS formation in the mitochondria and increases expression of MMP-1 and MMP-9. Antioxidants that specifically target the mitochondria [MitoQ (mitoquinone)] block the IRA-induced expression of MMP-1 in human fibroblasts, whereas the UVA ⁄ UVB-induced increased expression of MMP-1 remains unaffected.48 Besides the increased expression of MMP-1, IRA-exposure decreases the production of procollagen 1.49 Similar to UV-exposure, acute exposure to IRA elicits neoangiogenesis and accumulation of infiltrating inflammatory cells.50 Prevention and therapy Figure 4 The back of the hands of a 23-year-old woman (top left corner) without any signs of photoageing and of a 46-year-old woman (top right corner) with lentigines and fine wrinkles. On the bottom right, the back of the hand of a 61-year-old woman with lentigines and wrinkles and, on the bottom left, the back of the hand of an 83-year-old woman showing loss of subcutaneous fat, lentigines, hypopigmented spots, deep wrinkles and atrophy. Inorganic and organic sunscreens atrophy.42 Sun-induced molecular effects are primarily located in the dermis and the dermoepidermal junction. Histopathologically, photoaged skin is distinguished by solar elastosis, i.e., the accumulation of degraded elastic tissue in the dermis. Elastotic material consists of elastin, fibrillin, glycosaminoglycans, particularly hyaluronic acid, and versican, a large chondroitin sulphate proteoglycan. The pathogenesis of solar elastosis is not yet fully understood but is assumed to derive from both degradation and de novo synthesis.43 Photoprotection is essential for preventing UV-induced premature skin ageing. In vivo studies have indicated that the regular application of sunscreen may avoid or at least diminish UV-induced epidermal and dermal changes.51 Topical sunscreens are divided into inorganic (formerly referred to as physical) and organic sun protection (formerly referred to as chemical). Inorganic sunscreens as titanium dioxide and zinc oxide reflect, scatter, or absorb UV-radiation depending on the particle size and the wavelength of the light. Zinc oxide and titanium dioxide neither have any skin-irritating or skin-sensitizing properties nor penetrate into the layers below the stratum corneum. Modern micronized forms show a decreased particle size of 10–50 nm, offering more transparent and cosmetically appealing formulations. Organic sunscreens absorb UV-radiation, whereby the agent’s electrons reach an excited state. For a more detailed description of this topic, we refer to several excellent reviews.52,53 Skin ageing induced by other exogenous factors Antioxidants Tobacco smoking Besides UV-exposure, alcohol consumption, skin type and gender, exposure to tobacco smoke is a major factor contributing to premature skin ageing.44 Several studies have indicated that cigarette smoking furthers wrinkle formation. Analysis of skin surface structure showed that people with a smoking history of at least 35 pack years showed significantly deeper wrinkles than non-smokers, yet line density was decreased compared with non-smokers.45 Similar to UV-exposure, nicotine abuse induces expression of MMPs degrading ECM in human skin.46 Infrared radiation Infrared (IR) radiation (k = 760 nm to 1 mm) comprises 54.3% of total incident solar energy and may be subdivided according to wavelength into IRA (k = 760 nm to 1440 nm), IRB (k = 1440 nm to 3000 nm), and IRC (k = 3000 nm to 1 mm). The depth of penetration into the skin declines with increasing wavelength in the IR region. JEADV 2011, 25, 873–884 The formation of free radicals and ROS is of particular importance for photocarcinogenesis and skin ageing. Because the topical application of sunscreens does not offer complete protection against UVdamage, antioxidants play a major role in the prevention and therapy of UV-induced skin ageing. The enzymatic and non-enzymatic antioxidants of the skin are depleted by UV-induced oxidative stress.54 In the skin, important non-enzymatic antioxidants are ascorbic acid, coenzyme Q 10, vitamin E, niacinamide and b-carotene. Besides the topical application of antioxidants, endogenous photoprotection through dietary micronutrients is becoming more important, because the biggest part of a cumulative UV-dose is obtained in everyday life without topically applied sunscreens. Contrary to previous assumptions, at least 75% of a lifetime UV-dose is attained after the age of 18.55 Topical application of antioxidants and supplementation with micronutrients, such as polyphenols and b-carotene, should be complementarily effected with topical sunscreen.56 ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Kohl et al. 878 However, no significant long-term studies are yet available on topical antioxidants and supplementation of antioxidants proving photoprotective properties. Vitamins As other antioxidants, vitamin C is very instable when exposed to air because of oxidation. Therefore, esterified derivatives are used for topical application. Besides its antioxidative properties, vitamin C is essential for collagen biosynthesis because it serves as a cofactor for two enzymes.57 In an animal model, vitamin C has shown to be photoprotective by decreasing UVBinduced erythema and the number of sunburn cells.58 The photoprotective effects of vitamin E have been shown in numerous studies.59 Vitamin C and coenzyme Q10 synergistically interact with vitamin E by reducing oxidized vitamin E, thus enhancing the antioxidative properties of vitamin E.60 Niacinamide, also known as nicotinamide, is the amide of niacin (vitamin B3). The application of creams containing 4% and 5% niacinamide significantly reduced wrinkles and improved skin elasticity (see Table 1).61,62 Although less potent than retinoids, niacinamide is particularly suited for the periocular region because of its non-irritating properties. Carotenoids protect plants against oxidative stress and excess light and exhibit an extended system of conjugated double bonds essential for antioxidative properties.63 A meta-analysis showed that oral supplementation with b-carotene protects against UVBinduced erythema. For significant protection against sunburn, a minimum supplementation period of 10 weeks was noted.64 Carotenoids at high doses may have prooxidative effects. Endogenous photoprotection attainable with b-carotene complies with sun protection factor 4 at the most.64 Coenzyme Q10 Coenzyme Q10 (CoQ10, ubiquinone) is a fatsoluble antioxidant. In vitro CoQ10 reduced the UVA-induced production of MMP in human fibroblasts.65 So far, only one study showed wrinkle improvement using 1% CoQ10 cream for 5 months.66 Table 1 Overview of studies on topical antioxidants for the treatment of skin ageing Authors No. patients Study design Study medication Application Duration Clinical results Bissett et al. (2005) 50 Double-blind, left-right randomized 5% niacinamide vs. vehicle Twice daily to half of the face and its vehicle control to the other half 12 weeks After 12 weeks significant reductions in - fine lines and wrinkles (P = 0.0005) - hyperpigmented spots (P = 0.006) - red blotchiness (P = 0.03) - skin sallowness (P = 0.0004) (yellowing) compared with vehicle control - improvement of skin elasticity compared with vehicle control (P < 0.05) Kawada et al. (2008) 30 Randomized, placebo-controlled, split face study 4% niacinamide vs. vehicle Once daily to half of the face and its vehicle control to the other half 8 weeks After 8 weeks - marked resp. moderate improvement of wrinkles in 64% of the subjects with a significant difference compared with the control site (P < 0.001) - wrinkle grades were significantly reduced compared with control (P < 0.001) Humbert et al. (2003) 20 Randomized placebo-controlled, double-blind study Cream containing 5% vitamin C vs. vehicle Once daily on low-neck and arms 6 months - significant improvement, in terms of the ‘global score’ (hydration, roughness, suppleness, wrinkles and laxity) compared with control - highly significant increase in the density of skin microrelief - ultrastructural evidence of the elastic tissue repair due to reappearance of ‘composite’ elastic fibres in the papillary dermis of vitamin c-treated sides - no changes of dermal collagen JEADV 2011, 25, 873–884 ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Skin ageing 879 Polyphenols Polyphenols are secondary plant substances consisting of polycyclic aromatic compounds bonded with hydroxyl groups. Polyphenols dispose of both anti-inflammatory and antioxidant effects and are capable of modulating several signalling cascades. The photoprotective properties of green tea have been extensively investigated. Green tea is obtained from the leaves of the plant camellia sinensis that mainly contain the polyphenols (-)epicatechin (EC), (-)-epigallocatechin (EGC), (-)-epicatechin-3gallate (ECG) and (-)-epigallocatechin-3-gallate (EGCG), which have antioxidant properties. Green tea offers potent anti-inflammatory, antioxidant and photoprotective qualities67,68 that may prevent UV-induced skin changes. In animal models, topical application or oral supplementation with green tea polyphenols decreased UVA-induced roughness and sagginess,69 attenuated UVB-induced erythema,70 and inhibited UVB-induced protein oxidation in the dermis. Besides, green tea polyphenols were shown to diminish expression of MMPs in vivo and in vitro.71 Topically administered polyphenols from green tea dosedependently inhibited UVB-induced CPD formation in the human epidermis and dermis.72 Moreover, topically applied green tea extracts prior to exposure to solar simulated radiation reduced the number of histologically verifiable sunburn cells, inhibited UV-induced erythema, maintained the depletion of Langerhans cells,68 and inhibited UV-induced increase of epidermal thickness (Table 2).9 The UV-protective effects of green tea polyphenols are presumably due to enhanced IL-12 mediated DNA-repair.73 Silymarin, a flavonoid from milk thistle (Silybum marianum), also reduced UVA ⁄ B-induced oxidative stress in animal models74 and attenuated photocarcinogenesis.75 Extracts of the fern polypodium leucotomos is endued with strong antioxidant, anti-inflammatory and photoprotective properties.76–78 In humans, UV-induced skin changes were reduced by oral supplementation with Polypodium leucotomos, which – prior to exposure to solar simulated radiation – decreased UV-induced erythema, the formation of sunburn cells, DNA-damage and Table 2 Overview of clinical studies on photoprotective effects of green tea polyphenols and Polypodium leucotomos Authors No. subjects Study design Study medication Results Elmets et al. (2001) 6 Areas of skin were treated with an extract of green tea or one of its constituents. 30 min later, the treated sites were exposed to a 2 MED solar simulated UVR 5% solution of green tea polyphenols (GTPs) Green tea polyphenols resulted in a dose-dependent inhibition of UV-induced erythema. The (-)-epigallocatechin-3-gallate (EGCG) and (-)-epicatechin-3gallate (ECG) polyphenolic fractions were most efficient at inhibiting erythema. Histologically, application of green tea polyphenols resulted in a reduction of sunburn cells by 66% (P < 0.01) and reduced depletion of Langerhans cells. Green tea polyphenols also reduced significantly the DNA damage that formed after UV radiation. Middelkamp-Hup et al. (2004) 9 Subjects were exposed to varying doses of UV radiation without and after oral administration of Polypodium leucotomos (7.5 mg ⁄ kg) Oral administration of Polypodium leucotomos (7.5 mg ⁄ kg) A significant decrease in erythema was found in PL-treated skin (P < 0.01). Histologically, PL-treated biopsy specimens showed less sunburn cells (P < 0.05), cyclobutane pyrimidine dimers (P < 0.001), proliferating epidermal cells (P < 0.001), and dermal mast cell infiltration (P < 0.05). A trend towards Langerhans cell preservation was seen. 10 Randomized, investigatorblinded, controlled study. Subjects were exposed to UVA without and after oral administration of Polypodium leucotomos Oral administration of Polypodium leucotomos 240 mg, 8 h and 2 h before UVA exposure A trend towards prevention of the increase of the common deletion in the Polypodium leucotomosgroup was seen. Villa et al. (2010) JEADV 2011, 25, 873–884 ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Kohl et al. 880 dermal mast cell infiltration.76 Polypodium leucotomos may be administered orally and topically. Eicosapentaenoic acid In human skin, topical application of eicosapentaenoic acid (EPA) before UVA ⁄ B-exposure reduced epidermal thickening and inhibited UV-induced decrease of procollagen expression in vivo. In intrinsically aged human skin, topical application of EPA increased expression of ECM proteins (Table 3).79 Retinoids The efficacy of topically applied tretinoin (all-trans-retinoic acid) for the treatment of photoageing has been convincingly documented in several trials (Table 4). Significant effects were induced by concentrations of 0.02% or higher, whereas a dose–response relationship exists for both effectiveness and skin irritation. Significant improvements were found for fine wrinkling, skin roughness, mottled hyperpigmentation, sallowness and the overall severity of photodamage.80,81 Clinical improvement occurred after several months of application; in addition, skin conditions continued to improve with an application duration of at least 10–12 months. Clinical results are reversible after cessation of therapy; thus, longterm treatment three to four times a week is recommended to maintain clinical benefits. In the US, Tretinoin 0.05% is approved by the FDA for the mitigation of fine wrinkles, mottled hyperpigmentation and tactile roughness of facial skin. Tazarotene, another retinoid approved by the FDA to ameliorate some of the signs of photoageing, is assumed to be as effective as tretinoin.82 Topical application of tretinoin prevents the UVB-induced expression of MMPs through inhibition of the nuclear transcription factor AP-1 and obviates collagen degradation, which is already initiated by low-dose UVB-irradiation.26 Histological effects differ depending on use duration. Initially, increase of epidermal thickness and anchoring fibrils are observed. Dermal effects in terms of neocollagenesis are not evident before 12 month application.83 According to the clinical effects described above, histological examination shows an increase of collagen in the papillary dermis accompanied by a decrease of solar elastosis.84 The melanin content also continues to decrease with the increasing duration of therapy, correlating with improved mottled hyperpigmentation and solar lentigines.83 Evidence suggests that intrinsically aged skin may also benefit from the application of topical retinoids.85 Hormones and growth factors Study results on the cutaneous effects of hormone replacement therapy are inconsistent.86 However, several studies have indicated that hormone replacement therapy or the topical application of oestrogen may ameliorate the effects of hormone deficiency. In comparison to control groups, prevention of and improvements in wrinkles have been documented87 as well as enhanced hydration88 and elasticity,88,89 accession of skin thickness88 and increased collagen.8 Because of the well-documented side-effects, risks and benefits should be diligently analysed before the inception of oestrogen supplementation.90 Table 3 Photoprotective effects and effects on extracellular matrix of eicosapentaenoic acid in human skin Author No. subjects Study design Study medication Results Kim et al. (2006) 7 resp. 4 (A) Topical application of EPA 2% under occlusion vs. vehicle once daily for 2 days before UV-exposure (2 MED) in volunteers (average age: 28 years) (B) Topical application of EPA 2% vs. vehicle three times a week for 2 weeks under occlusion in volunteers (average age: 76 years) 2% EPA in ethanolpolyethylene glycol (70 : 30) vs. vehicle (A) EPA inhibited UV-induced epidermal thickening by 72 ± 12.6% (P < 0.05) compared with vehicle. EPA prevented UV-induced decrease of procollagen expression compared with vehicle. Inhibition of UV-induced MMP-1 expression by 55 ± 13% (P < 0.05) and MMP-9 expression by 75 ± 7% (P < 0.05) compared with vehicle. Inhibition of UV-induced c-Jun phosphorylation by 79 ± 11% (P < 0.05) compared to vehicle. Inhibition of UV-induced COX-2 expression by 76 ± 4% (P < 0.05) compared with vehicle. (B) EPA increased the expression of procollagen by 218 ± 39% (P < 0.05) compared with vehicle. EPA increased the level of tropoelastin and fibrillin-1 by 420 ± 53% (P < 0.05) compared with vehicle. JEADV 2011, 25, 873–884 ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Skin ageing 881 Table 4 Overview of studies on topical retinoids for treatment of skin ageing Authors No. Study design patients Retinoid Frequency of Duration application Clinical results Randomized, double-blind, placebo-controlled phase and an additional 6-month open-label phase Tretinoin microsphere gel 0.1% Once daily on 6 months resp. facial skin 12 months At 6 months statistically significant improvement relative to placebo in - overall severity of photodamage (P = 0.0003) - investigator’s global assessment of clinical response (P < 0.0001) - fine wrinkling (P < 0.0001), - mottled hyperpigmentation (P = 0.0002) - yellowing ⁄ sallowness (P < 0.0001) - lentigines (P = 0.0054) Weiss et al. (2006) 45 Kang et al. (2005) 204 Randomized placebocontrolled Tretinoin emollient cream 0.05% Once daily on 24 months facial skin Significantly greater improvement relative to placebo in - fine wrinkling - coarse wrinkling - mottled hyperpigmentation - lentigines - sallowness - overall photodamage severity - investigator’s global assessment of clinical response (P < 0.05) Phillips et al. (2002) 563 24-week multicentre, double-blind, randomized, vehiclecontrolled intervention study followed by a 28-week open-label extension Tazarotene cream 0.1% Once daily on 12 months facial skin Double-blind period: Tazarotene resulted in a significantly greater incidence of patients achieving treatment success (‡50% global improvement) and at least a 1-grade improvement in fine wrinkling, mottled hyperpigmentation, lentigines, elastosis, pore size, irregular depigmentation, tactile roughness, coarse wrinkling and the overall integrated assessment of photodamage (P < 0.01) 36 Randomized, doubleblind, vehiclecontrolled, left and right arm comparison study 0.4% retinol (vitamin A) lotion Up to three times per week on the upper inner portions of the arms Kafi et al. 2007) Enhancing collagen production with topical oestradiol seems to be restricted to intrinsically aged skin.91 Evidence suggests that topical application of growth factors derived from human fibroblasts improves several features of photoaged skin.92 DNA repair enzymes DNA-damage, such as CPDs, plays an essential role in photocarcinogenesis but also contributes to skin ageing. UVB-irradiated human keratinocytes are involved in the induction of MMP-1 in dermal fibroblasts via paracrine mechanisms. MMP-1 induction was reduced when keratinocytes were treated with the DNA-repair enzyme T4 endonuclease V (T4N5).93 The bacterial DNA-incision repair enzyme T4N5 is encapsulated in liposomes JEADV 2011, 25, 873–884 24 weeks After 24 weeks significant differences between retinol-treated and vehicle-treated skin for changes in fine wrinkling scores [)1.64 (95% CI: )2.06 to )1.22) vs. )0.08 (95% CI: )0.17 to 0.01); P < 0.001] for delivery into the living cells of the skin; here, the enzyme recognizes CPDs and enhances dimer removal. The topical application of a lotion containing T4N5 in patients with xeroderma pigmentosum lowered the incidence of non-melanoma skin cancer.94 Photolyase is another DNA repair enzyme, which can be found in numerous plants and animals but not in humans. Enzymatic removal of CPDs requires exposure of the dimer-photolyase complex to photoreactivating light. The application of photolyase containing liposomes considerably reduces the amount of CPDs in human skin. Besides, evidence suggests that topical application of photolyase prevents UVB-induced immunosuppression, formation of sunburn cells, erythema and tanning reactions.95 A sunscreen ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Kohl et al. 882 containing the DNA-repair enzyme photolyase is commercially available. Innovative approaches for photoprotection DNA-oligonucleotides DNA-oligonucleotides (T-oligos) show another possibility to enhance DNA-repair. DNA-oligonucleotides homologous to the telomere 3-prime overhang sequence mimic a telomere loop disruption and overhang exposure and initiate protective DNA-damage response. Treatment with t-oligos stimulates melanogenesis and enhances DNA repair capacity. This displays an innovative option for photoprotection, as both tanning and increased DNA-repair rates are physiologically induced by UVexposure and DNA-damage to protect from further damage.96 Forskolin Tanning of the skin may also be induced by the topical application of forskolin, a cell permeable diterpene that stimulates adenylate cyclase activity. This enzyme is physiologically activated after the binding of a-MSH to the melanocortin 1 receptor (MC1R), thus up-regulating cAMP-levels in melanocytes. As effects of a-MSH are cAMP-mediated, the binding of a-MSH to the MC1R may be obviated, and melanin production takes place without any previous sun-exposure. In animal models, pigmentation was compassed despite the absence of a functional MC1R. Application of the cyclic AMP-agonist forskolin induced pigmentation in fair-skinned individuals with defective MC1R who show sequence variants of the MC1Rgene.97 Besides, in vitro induction of pigmentation with forskolin also showed enhanced DNA-repair, removing CPDs and 6,4photoproducts more efficiently.98 a-MSH analogues a-MSH, mediating UV-induced tanning, is regarded as a cytoprotective agent. Synthesis of melanin may also be stimulated by analogues of a-MSH that bind to melanocortin1-receptor on melanocytes. [Nle4-D-Phe7]-a-MSH (MT-1 or Melanotan-1), a derivative of a-MSH with higher potency and prolonged chemical stability than a-MSH, entails an explicit increase of the melanin content in human skin in vivo when injected subcutaneously. This effect was most pronounced in fair subjects with a low minimal erythema dose threshold.99 However, new findings indicate that a-MSH may actually increase mtDNA damage because of increased oxidative stress within the frame of elevated melanin synthesis.100 References 1 Harman D. Aging: overview. Ann N Y Acad Sci 2001; 928: 1–21. 2 Makrantonaki E, Zouboulis CC, William J. Cunliffe Scientific Awards. Characteristics and pathomechanisms of endogenously aged skin. Dermatology 2007; 214: 352–360. 3 Fisher GJ, Kang S, Varani J et al. Mechanisms of photoaging and chronological skin aging. Arch Dermatol 2002; 138: 1462–1470. 4 Sohal RS, Weindruch R. Oxidative stress, caloric restriction, and aging. Science 1996; 273: 59–63. JEADV 2011, 25, 873–884 5 Chung JH, Kang S, Varani J, Lin J, Fisher GJ, Voorhees JJ. Decreased extracellular-signal-regulated kinase and increased stress-activated MAP kinase activities in aged human skin in vivo. J Invest Dermatol 2000; 115: 177–182. 6 Quan T, Shao Y, He T, Voorhees JJ, Fisher GJ. Reduced expression of connective tissue growth factor (CTGF ⁄ CCN2) mediates collagen loss in chronologically aged human skin. J Invest Dermatol 2010; 130: 415– 424. 7 Makrantonaki E, Adjaye J, Herwig R et al. Age-specific hormonal decline is accompanied by transcriptional changes in human sebocytes in vitro. Aging Cell 2006; 5: 331–344. 8 Brincat MP. Hormone replacement therapy and the skin. Maturitas 2000; 35: 107–117. 9 Makrantonaki E, Zouboulis CC. Androgens and ageing of the skin. Curr Opin Endocrinol Diabetes Obes 2009; 16: 240–245. 10 Uitto J. Understanding premature skin aging. N Engl J Med 1997; 337: 1463–1465. 11 Klotz LO, Holbrook NJ, Sies H. UVA and singlet oxygen as inducers of cutaneous signaling events. Curr Probl Dermatol 2001; 29: 95–113. 12 Wallace DC 1994 William Allan Award Address. Mitochondrial DNA variation in human evolution, degenerative disease, and aging. Am J Hum Genet. 1995; 57; 201–223. 13 Berneburg M, Gattermann N, Stege H et al. Chronically ultravioletexposed human skin shows a higher mutation frequency of mitochondrial DNA as compared to unexposed skin and the hematopoietic system. Photochem Photobiol 1997; 66: 271–275. 14 Berneburg M, Plettenberg H, Medve-Konig K et al. Induction of the photoaging-associated mitochondrial common deletion in vivo in normal human skin. J Invest Dermatol 2004; 122: 1277–1283. 15 Birch-Machin MA, Tindall M, Turner R, Haldane F, Rees JL. Mitochondrial DNA deletions in human skin reflect photo- rather than chronologic aging. J Invest Dermatol 1998; 110: 149–152. 16 Schroeder P, Gremmel T, Berneburg M, Krutmann J. Partial depletion of mitochondrial DNA from human skin fibroblasts induces a gene expression profile reminiscent of photoaged skin. J Invest Dermatol 2008; 128: 2297–2303. 17 Nakamura K, Izumiyama-Shimomura N, Sawabe M et al. Comparative analysis of telomere lengths and erosion with age in human epidermis and lingual epithelium. J Invest Dermatol 2002; 119: 1014–1019. 18 Harley CB, Futcher AB, Greider CW. Telomeres shorten during ageing of human fibroblasts. Nature 1990; 345: 458–460. 19 Hayflick L. The limited in vitro lifetime of human diploid cell strains. Exp Cell Res 1965; 37: 614–636. 20 Lombard DB, Chua KF, Mostoslavsky R, Franco S, Gostissa M, Alt FW. DNA repair, genome stability, and aging. Cell 2005; 120: 497–512. 21 Gilchrest BA, Eller MS, Yaar M. Telomere-mediated effects on melanogenesis and skin aging. J Investig Dermatol Symp Proc 2009; 14: 25–31. 22 Kosmadaki MG, Gilchrest BA. The role of telomeres in skin aging ⁄ photoaging. Micron 2004; 35: 155–159. 23 Krunic D, Moshir S, Greulich-Bode KM et al. Tissue context-activated telomerase in human epidermis correlates with little age-dependent telomere loss. Biochim Biophys Acta 2009; 1792: 297–308. 24 Sugimoto M, Yamashita R, Ueda M. Telomere length of the skin in association with chronological aging and photoaging. J Dermatol Sci 2006; 43: 43–47. 25 Harle-Bachor C, Boukamp P. Telomerase activity in the regenerative basal layer of the epidermis inhuman skin and in immortal and carcinoma-derived skin keratinocytes. Proc Natl Acad Sci USA 1996; 93: 6476–6481. 26 Fisher GJ, Datta SC, Talwar HS et al. Molecular basis of sun-induced premature skin ageing and retinoid antagonism. Nature 1996; 379: 335– 339. 27 Quan T, He T, Voorhees JJ, Fisher GJ. Ultraviolet irradiation induces Smad7 via induction of transcription factor AP-1 in human skin fibroblasts. J Biol Chem 2005; 280: 8079–8085. ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Skin ageing 883 28 Brenneisen P, Sies H, Scharffetter-Kochanek K. Ultraviolet-B irradiation and matrix metalloproteinases: from induction via signaling to initial events. Ann N Y Acad Sci 2002; 973: 31–43. 29 Quan T, Qin Z, Xia W, Shao Y, Voorhees JJ, Fisher GJ. Matrix-degrading metalloproteinases in photoaging. J Investig Dermatol Symp Proc 2009; 14: 20–24. 30 Fisher GJ, Quan T, Purohit T et al. Collagen fragmentation promotes oxidative stress and elevates matrix metalloproteinase-1 in fibroblasts in aged human skin. Am J Pathol 2009; 174: 101–114. 31 Imokawa G. Recent advances in characterizing biological mechanisms underlying UV-induced wrinkles: a pivotal role of fibrobrast-derived elastase. Arch Dermatol Res 2008; 300(Suppl. 1): S7–20. 32 Rijken F, Bruijnzeel PL. The pathogenesis of photoaging: the role of neutrophils and neutrophil-derived enzymes. J Investig Dermatol Symp Proc 2009; 14: 67–72. 33 Chung JH, Eun HC. Angiogenesis in skin aging and photoaging. J Dermatol 2007; 34: 593–600. 34 Yano K, Kadoya K, Kajiya K, Hong YK, Detmar M. Ultraviolet B irradiation of human skin induces an angiogenic switch that is mediated by upregulation of vascular endothelial growth factor and by downregulation of thrombospondin-1. Br J Dermatol 2005; 152: 115–121. 35 Yano K, Oura H, Detmar M. Targeted overexpression of the angiogenesis inhibitor thrombospondin-1 in the epidermis of transgenic mice prevents ultraviolet-B-induced angiogenesis and cutaneous photo-damage. J Invest Dermatol 2002; 118: 800–805. 36 Widmer R, Ziaja I, Grune T. Protein oxidation and degradation during aging: role in skin aging and neurodegeneration. Free Radic Res 2006; 40: 1259–1268. 37 Sander CS, Chang H, Salzmann S et al. Photoaging is associated with protein oxidation in human skin in vivo. J Invest Dermatol 2002; 118: 618–625. 38 Lavker RM. Structural alterations in exposed and unexposed aged skin. J Invest Dermatol 1979; 73: 59–66. 39 Gilchrest BA, Blog FB, Szabo G. Effects of aging and chronic sun exposure on melanocytes in human skin. J Invest Dermatol 1979; 73: 141– 143. 40 Braverman IM, Fonferko E. Studies in cutaneous aging: I. The elastic fiber network. J Invest Dermatol 1982; 78: 434–443. 41 Zouboulis ChC. Intrinsic skin aging. A critical appraisal of the role of hormones. Hautarzt 2003; 54: 825–832. 42 Bhawan J, Andersen W, Lee J, Labadie R, Solares G. Photoaging versus intrinsic aging: a morphologic assessment of facial skin. J Cutan Pathol 1995; 22: 154–159. 43 Sellheyer K. Pathogenesis of solar elastosis: synthesis or degradation? J Cutan Pathol 2003; 30: 123–127. 44 Morita A, Torii K, Maeda A, Yamaguchi Y. Molecular basis of tobacco smoke-induced premature skin aging. J Investig Dermatol Symp Proc 2009; 14: 53–55. 45 Boyd AS, Stasko T, King LE Jr, Cameron GS, Pearse AD, Gaskell SA. Cigarette smoking-associated elastotic changes in the skin. J Am Acad Dermatol 1999; 41: 23–26. 46 Lahmann C, Bergemann J, Harrison G, Young AR. Matrix metalloproteinase-1 and skin ageing in smokers. Lancet 2001; 357: 935–936. 47 Kligman LH. Intensification of ultraviolet-induced dermal damage by infrared radiation. Arch Dermatol Res 1982; 272: 229–238. 48 Schroeder P, Lademann J, Darvin ME et al. Infrared radiation-induced matrix metalloproteinase in human skin: implications for protection. J Invest Dermatol 2008; 128: 2491–2497. 49 Kim MS, Kim YK, Cho KH, Chung JH. Regulation of type I procollagen and MMP-1 expression after single or repeated exposure to infrared radiation in human skin. Mech Ageing Dev 2006; 127: 875–882. 50 Kim MS, Kim YK, Lee DH et al. Acute exposure of human skin to ultraviolet or infrared radiation or heat stimuli increases mast cell numbers and tryptase expression in human skin in vivo. Br J Dermatol 2009; 160: 393–402. JEADV 2011, 25, 873–884 51 van der Pols JC, Xu C, Boyle GM, Parsons PG, Whiteman DC, Green AC. Expression of p53 tumor suppressor protein in sun-exposed skin and associations with sunscreen use and time spent outdoors: a community-based study. Am J Epidemiol 2006; 163: 982–988. 52 Lautenschlager S, Wulf HC, Pittelkow MR. Photoprotection. Lancet 2007; 370; 528–537. 53 Palm MD, O’Donoghue MN. Update on photoprotection. Dermatol Ther 2007; 20: 360–376. 54 Rhie G, Shin MH, Seo JY et al. Aging- and photoaging-dependent changes of enzymic and nonenzymic antioxidants in the epidermis and dermis of human skin in vivo. J Invest Dermatol 2001; 117: 1212–1217. 55 Godar DE, Urbach F, Gasparro FP, van der Leun JC. UV doses of young adults. Photochem Photobiol 2003; 77: 453–457. 56 Matsui MS, Hsia A, Miller JD et al. Non-sunscreen photoprotection: antioxidants add value to a sunscreen. J Investig Dermatol Symp Proc 2009; 14: 56–59. 57 Humbert PG, Haftek M, Creidi P et al. Topical ascorbic acid on photoaged skin. Clinical, topographical and ultrastructural evaluation: double-blind study vs. placebo. Exp Dermatol 2003; 12: 237– 244. 58 Darr D, Combs S, Dunston S, Manning T, Pinnell S. Topical vitamin C protects porcine skin from ultraviolet radiation-induced damage. Br J Dermatol 1992; 127: 247–253. 59 Thiele JJ, Hsieh SN, Ekanayake-Mudiyanselage S. Vitamin E: critical review of its current use in cosmetic and clinical dermatology. Dermatol Surg 2005; 31: 805–813; discussion 813. 60 Lin JY, Selim MA, Shea CR et al. UV photoprotection by combination topical antioxidants vitamin C and vitamin E. J Am Acad Dermatol 2003; 48: 866–874. 61 Bissett DL, Oblong JE, Berge CA. Niacinamide: a B vitamin that improves aging facial skin appearance. Dermatol Surg 2005; 31: 860– 865; discussion 865. 62 Kawada A, Konishi N, Oiso N, Kawara S, Date A. Evaluation of antiwrinkle effects of a novel cosmetic containing niacinamide. J Dermatol 2008; 35: 637–642. 63 Stahl W, Sies H. Carotenoids and flavonoids contribute to nutritional protection against skin damage from sunlight. Mol Biotechnol 2007; 37: 26–30. 64 Kopcke W, Krutmann J. Protection from sunburn with beta-carotene – a meta-analysis. Photochem Photobiol 2008; 84: 284–288. 65 Hoppe U, Bergemann J, Diembeck W et al. Coenzyme Q10, a cutaneous antioxidant and energizer. Biofactors 1999; 9: 371–378. 66 Inui M, Ooe M, Fujii K, Matsunaka H, Yoshida M, Ichihashi M. Mechanisms of inhibitory effects of CoQ10 on UVB-induced wrinkle formation in vitro and in vivo. Biofactors 2008; 32: 237–243. 67 Hsu S. Green tea and the skin. J Am Acad Dermatol 2005; 52: 1049– 1059. 68 Elmets CA, Singh D, Tubesing K, Matsui M, Katiyar S, Mukhtar H. Cutaneous photoprotection from ultraviolet injury by green tea polyphenols. J Am Acad Dermatol 2001; 44: 425–432. 69 Kim J, Hwang JS, Cho YK, Han Y, Jeon YJ, Yang KH. Protective effects of (-)-epigallocatechin-3-gallate on UVA- and UVB-induced skin damage. Skin Pharmacol Appl Skin Physiol 2001; 14: 11–19. 70 Jeon HY, Kim JK, Kim WG, Lee SJ. Effects of oral epigallocatechin gallate supplementation on the minimal erythema dose and UV-induced skin damage. Skin Pharmacol Physiol 2009; 22: 137–141. 71 Vayalil PK, Mittal A, Hara Y, Elmets CA, Katiyar SK. Green tea polyphenols prevent ultraviolet light-induced oxidative damage and matrix metalloproteinases expression in mouse skin. J Invest Dermatol 2004; 122: 1480–1487. 72 Katiyar SK, Perez A, Mukhtar H. Green tea polyphenol treatment to human skin prevents formation of ultraviolet light B-induced pyrimidine dimers in DNA. Clin Cancer Res 2000; 6: 3864–3869. 73 Schwarz T, Schwarz A. DNA repair and cytokine responses. J Investig Dermatol Symp Proc 2009; 14: 63–66. ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology Kohl et al. 884 74 Katiyar SK, Meleth S, Sharma SD. Silymarin, a flavonoid from milk thistle (Silybum marianum L.), inhibits UV-induced oxidative stress through targeting infiltrating CD11b+ cells in mouse skin. Photochem Photobiol 2008; 84: 266–271. 75 Katiyar SK, Korman NJ, Mukhtar H, Agarwal R. Protective effects of silymarin against photocarcinogenesis in a mouse skin model. J Natl Cancer Inst 1997; 89: 556–566. 76 Middelkamp-Hup MA, Pathak MA, Parrado C et al. Oral Polypodium leucotomos extract decreases ultraviolet-induced damage of human skin. J Am Acad Dermatol 2004; 51: 910–918. 77 Zattra E, Coleman C, Arad S et al. Polypodium leucotomos extract decreases UV-induced Cox-2 expression and inflammation, enhances DNA repair, and decreases mutagenesis in hairless mice. Am J Pathol 2009; 175: 1952–1961. 78 Villa A, Viera MH, Amini S et al. Decrease of ultraviolet A lightinduced ‘‘common deletion’’ in healthy volunteers after oral Polypodium leucotomos extract supplement in a randomized clinical trial. J Am Acad Dermatol 2010; 62: 511–513. 79 Kim HH, Cho S, Lee S et al. Photoprotective and anti-skin-aging effects of eicosapentaenoic acid in human skin in vivo. J Lipid Res 2006; 47: 921–930. 80 Samuel M, Brooke RC, Hollis S, Griffiths CE. Interventions for photodamaged skin. Cochrane Database Syst Rev. 2005; 1: CD001782. 81 Weiss JS, Shavin JS, Nighland M, Grossman R. Tretinoin microsphere gel 0.1% for photodamaged facial skin: a placebo-controlled trial. Cutis 2006; 78: 426–432. 82 Kang S, Krueger GG, Tanghetti EA et al. A multicenter, randomized, double-blind trial of tazarotene 0.1% cream in the treatment of photodamage. J Am Acad Dermatol 2005; 52: 268–274. 83 Bhawan J. Short- and long-term histologic effects of topical tretinoin on photodamaged skin. Int J Dermatol 1998; 37: 286–292. 84 Woodley DT, Zelickson AS, Briggaman RA et al. Treatment of photoaged skin with topical tretinoin increases epidermal-dermal anchoring fibrils. A preliminary report. JAMA 1990; 263: 3057–3059. 85 Kafi R, Kwak HS, Schumacher WE et al. Improvement of naturally aged skin with vitamin A (retinol). Arch Dermatol 2007; 143: 606–612. 86 Phillips TJ, Symons J, Menon S. Does hormone therapy improve age-related skin changes in postmenopausal women? A randomized, double-blind, double-dummy, placebo-controlled multicenter study assessing the effects of norethindrone acetate and ethinyl estradiol in the improvement of mild to moderate age-related skin changes in postmenopausal women. J Am Acad Dermatol 2008; 59: 397–404. 87 Dunn LB, Damesyn M, Moore AA, Reuben DB, Greendale GA. Does estrogen prevent skin aging? Results from the First National Health and JEADV 2011, 25, 873–884 88 89 90 91 92 93 94 95 96 97 98 99 100 Nutrition Examination Survey (NHANES I). Arch Dermatol 1997; 133: 339–342. Sator PG, Sator MO, Schmidt JB et al. A prospective, randomized, double-blind, placebo-controlled study on the influence of a hormone replacement therapy on skin aging in postmenopausal women. Climacteric 2007; 10: 320–334. Wolff EF, Narayan D, Taylor HS. Long-term effects of hormone therapy on skin rigidity and wrinkles. Fertil Steril 2005; 84: 285–288. Chlebowski RT, Kuller LH, Prentice RL et al. Breast cancer after use of estrogen plus progestin in postmenopausal women. N Engl J Med 2009; 360: 573–587. Rittie L, Kang S, Voorhees JJ, Fisher GJ. Induction of collagen by estradiol: difference between sun-protected and photodamaged human skin in vivo. Arch Dermatol 2008; 144: 1129–1140. Sundaram H, Mehta RC, Norine JA et al. Topically applied physiologically balanced growth factors: a new paradigm of skin rejuvenation. J Drugs Dermatol 2009; 8: 4–13. Dong KK, Damaghi N, Picart SD et al. UV-induced DNA damage initiates release of MMP-1 in human skin. Exp Dermatol 2008; 17: 1037– 1044. Yarosh D, Klein J, O’Connor A, Hawk J, Rafal E, Wolf P. Effect of topically applied T4 endonuclease V in liposomes on skin cancer in xeroderma pigmentosum: a randomised study. Xeroderma Pigmentosum Study Group. Lancet 2001; 357: 926–929. Stege H, Roza L, Vink AA et al. Enzyme plus light therapy to repair DNA damage in ultraviolet-B-irradiated human skin. Proc Natl Acad Sci USA 2000; 97: 1790–1795. Arad S, Konnikov N, Goukassian DA, Gilchrest BA. Quantification of inducible SOS-like photoprotective responses in human skin. J Invest Dermatol 2007; 127: 2629–2636. D’Orazio JA, Nobuhisa T, Cui R et al. Topical drug rescue strategy and skin protection based on the role of Mc1r in UV-induced tanning. Nature 2006; 443: 340–344. Passeron T, Namiki T, Passeron HJ, Le Pape E, Hearing VJ. Forskolin protects keratinocytes from UVB-induced apoptosis and increases DNA repair independent of its effects on melanogenesis. J Invest Dermatol 2009; 129: 162–166. Barnetson RS, Ooi TK, Zhuang L et al. [Nle4-D-Phe7]-alpha-melanocyte-stimulating hormone significantly increased pigmentation and decreased UV damage in fair-skinned Caucasian volunteers. J Invest Dermatol 2006; 126: 1869–1878. Böhm M, Kokot A, Luger TA, Dermody J, Hill HZ. Mitochondrial metabolism and DNA integrity – novel targets for alpha-MSH on human keratinocytes and melanocytes after UVB irradiation. Exp Dermatol 2010; 19: 174 A043. ª 2011 The Authors Journal of the European Academy of Dermatology and Venereology ª 2011 European Academy of Dermatology and Venereology