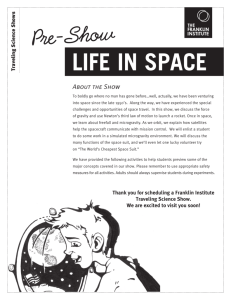
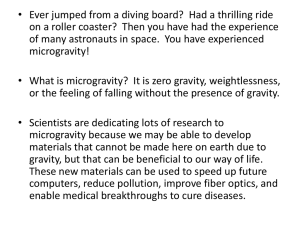
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/6562793 Emergency medicine in space Article in Journal of Emergency Medicine · February 2007 DOI: 10.1016/j.jemermed.2006.05.031 · Source: PubMed CITATIONS READS 50 1,148 3 authors, including: Lowan H. Stewart 8 PUBLICATIONS 62 CITATIONS Donald D Trunkey Oregon Health and Science University 232 PUBLICATIONS 9,460 CITATIONS SEE PROFILE SEE PROFILE All content following this page was uploaded by Lowan H. Stewart on 22 April 2019. The user has requested enhancement of the downloaded file. The Journal of Emergency Medicine, Vol. 32, No. 1, pp. 45–54, 2007 Copyright © 2007 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/07 $–see front matter doi:10.1016/j.jemermed.2006.05.031 Clinical Communications EMERGENCY MEDICINE IN SPACE Lowan H. Stewart, MD,* Donald Trunkey, MD,† and G. Steve Rebagliati, MD, MBA‡ *Department of Emergency Medicine, †Department of Surgery, and ‡Medical Affairs and Quality Management, Department of Emergency Medicine, Oregon Health and Science University, Portland, Oregon Reprint Address: Lowan H. Stewart, MD, Department of Emergency Medicine, Willamette Falls Hospital, 1500 Division St., Oregon City, OR 97045 e Abstract—Recent events, including the development of space tourism and commercial spaceflight, have increased the need for specialists in space medicine. With increased duration of missions and distance from Earth, medical and surgical events will become inevitable. Ground-based medical support will no longer be adequate when return to Earth is not an option. Pending the inclusion of sub-specialists, clinical skills and medical expertise will be required that go beyond those of current physicianastronauts, yet are well within the scope of Emergency Medicine. Emergency physicians have the necessary broad knowledge base as well as proficiency in basic surgical skills and management of the critically ill and injured. Space medicine shares many attributes with extreme conditions and environments that many emergency physicians already specialize in. This article is an introduction to space medicine, and a review of current issues in the emergent management of medical and surgical disease during spaceflight. © 2007 Elsevier Inc. mental issues throughout the development of the Russian and United States space programs, even before Yuri Gagarin’s first flight. To this day, the effectiveness of each mission to space depends on the health and wellbeing of each astronaut. The first successful Apollo mission, Apollo 7, became known as the “ten-day cold capsule” after the entire crew developed viral upper respiratory infections. The first deaths during spaceflight occurred in 1971 when three cosmonauts died due to rapid decompression of the Soyuz 11 capsule during reentry. Some of the more common medical problems encountered include minor trauma, burns, dermatologic and musculoskeletal conditions, respiratory illness, headache, insomnia, and space motion sickness (2). The relatively benign nature of these problems has primarily been a function of the short duration of individual spaceflights, careful selection of healthy astronauts, medical prophylaxis, and rigorous countermeasures to the effects of environmental factors and prolonged microgravity. Predicting the expected incidence and character of medical events during extended spaceflight has been difficult due to the small number of astronauts who have completed long-duration missions. Epidemiological data extrapolated from isolated U.S. Navy submariners suggest one mission-impacting medical event per 6-month mission with a crew of seven astronauts (3). Similar work has predicted a major surgical case to occur every 9 years and acute appendicitis every 35 years (4). As we embark upon a new era in space exploration, in which we expect e Keywords—space; spaceflight; microgravity; emergency medicine; emergency procedures “Human beings are the product of a long evolutionary process that has made us fully adapted to the Earth environment . . . When exposed to a space environment, the human body reaches a new homeostasis . . .” A.I. Grigoriev (1) INTRODUCTION Preventive medicine and contingency planning for acute care of the human during spaceflight have been funda- RECEIVED: 9 March 2005; FINAL ACCEPTED: 9 May 2006 SUBMISSION RECEIVED: 26 September 2005; 45 46 L. H. Stewart et al. continuous human inhabitation of the International Space Station (ISS) and eventual extended manned missions to the Moon and Mars, illness and injuries that once were rare will be encountered routinely, and with time, those scenarios merely probable will become certain. Earthbased medical support services at the American Mission Control Center and the Institute for Biomedical Problems in Russia will be increasingly augmented by telemedicine and intelligent computational neural networks, providing assistance to low-Earth orbit missions (5). Our ability to provide advanced medical care for acute illness and injury and safely return our astronauts to Earth is a prerequisite to interplanetary travel and prolonged human spaceflight beyond low-Earth orbit. Current training for astronaut crew medical officers only includes limited medical instruction and minor surgical skills such as basic suturing (6). As space vehicles move farther from the Earth’s orbit, telemetric medical support and traditional communication traveling at the speed of light will be significantly delayed. In the case of Mars, two-way radio contact would take a minimum of 44 min. These longer missions will require the presence of a physicianastronaut crewmember with a wide breadth of medical knowledge who is skilled in basic surgical procedures and the complex medical management of the acutely ill and injured. Pending the ultimate sub-specialization of medical care in space, when available resources might allow for options such as a surgical suite on a Lunar or Martian base, the next phase of space medicine will call for versatile medical providers with familiarity with the whole spectrum of human disease and disability. This article serves as an introduction to some of the current issues in acute space medicine pertinent to the emergency physician, who has the ideal background training for this specialized position. We will discuss the basics of space medicine and physiology, environmental factors, and some of the issues involved with the management of medical and surgical emergencies during spaceflight. THE HUMAN BODY IN SPACE “While acknowledging that three types of basic interaction (strong, weak, and electromagnetic) are the true fundamental prerequisites for life, as a quantitatively new, high form of existence of matter, we must also note that the fourth type of basic interaction— gravitational— serves as a kind of sculptor or architect of the universe, as well as of the varied forms of life and the substrate on which they can develop.” I.D. Pestov (7) In the decades since the first manned spaceflight by Yuri Gagarin, we have accumulated a tremendous amount of data regarding the human body in space (8). During the early years of space exploration, the study of space medicine and physiology uncovered a myriad of seemingly pathological changes in the human body exposed to microgravity. Because of the changes, even the physical examination itself must be adapted to this environment (9). Over time, a new paradigm has emerged, with the weight of evidence suggesting that these changes reflect adaptation to a unique environmental condition rather than irreversible pathology. Whether this will hold true remains one of the fundamental questions of space biology, as we await a complete understanding of the effects of long-duration exposure to microgravity. The longest continuous inhabitation of space was performed by the Russian physician-cosmonaut Valeri Polyakov, when he lived aboard space station Mir for 438 days. Very few people have spent more than a few months in space, limiting our ability to accurately predict long-term health risks. A more thorough understanding of physiologic changes during extended duration spaceflight is the prerequisite to a safe transition to interplanetary travel, such as a manned flight to Mars. CARDIOVASCULAR SYSTEM The human body consists of approximately 60% fluid. Under different accelerational, positional, and gravitational conditions, the intravascular fluid exerts variable hydrostatic pressure on the walls of elastic blood vessels, triggering specific responses to maintain homeostasis in the body. Upon entering the weightless environment of space, the absence of gravity-induced hydrostatic forces causes a cephalad shift and equilibration of intravascular fluid from the lower extremities to the trunk and upper extremities (approximately 2 L). This is followed by a transcapillary shift of fluid from the extravascular compartment to the intravascular compartment in the lower body, and from the blood vessels to the extravascular compartment in the upper body. Space travelers experience this as a sensation of fullness in the head, nasal congestion, facial edema, scleral and oral mucosal injection, and decreased leg circumference (what astronauts refer to as “chicken legs”). These symptoms decrease over time, but remain present throughout the course of even very long space flights. The discomfort of the fluid shift is transiently alleviated by lower body exercise. One astronaut reported alleviation of symptoms after meals (presumably from the shunting of blood to the gastrointestinal tract) (10). During the first few days of space flight, there is an average 2.5 kg body mass loss. This is a consequence of fluid diureses, primarily from the extracellular compartment, and decreased fluid intake. Increased central venous pressure (CVP) is thought to stimulate cardiac baroreceptors and initiate a reduction in plasma volume, Emergency Medicine in Space the so-called Henry-Gauer response, but studies including in-flight central venous catheterization have failed to demonstrate elevated CVP (11). This may be secondary to compensatory reactions during the pre-launch period in the supine position, and is also complicated by the practice of astronauts restricting fluid intake days before flight to avoid the inconvenient diuresis first experienced by Mercury astronauts on arrival to space. Cardiac dynamics in space have been measured directly with echocardiography and electrocardiography. Heart rate is increased significantly during launch, orbit entry, extravehicular activity (EVA), and reentry, attributed to cardiovascular deconditioning in weightlessness and physical and autonomic stress (12–14). Measurements of cardiac output, stroke volume, and left ventricular end diastolic volume have not been significantly different from ground-based observations, however, some recent data suggest decreased ejection fraction and reduction of overall cardiac function proportional to long mission duration (15). Electrocardiography has demonstrated the presence of occasional premature atrial contractions (PAC) and premature ventricular contractions (PVC). Observations during Space Shuttle EVA showed that PACs or PVCs were present in 30% of astronauts at some point during this period of strenuous activity in a 100% oxygen hypobaric environment (16). There have been reports of electrocardiographic long QTc intervals as well as brief episodes of ventricular tachycardia during extended spaceflights (17,18). These events may be related in part to sympathetic tone and elevated catecholamine levels present during spaceflight (19). The ectopy and brief dysrhythmias observed in astronauts are somewhat similar to those seen in healthy athletes during physical stress, but are of uncertain clinical significance in the space environment (20,21). Upon return to Earth, there is decreased tolerance to orthostatic stress. The cardiovascular system is unable to maintain an adequate blood pressure in the upper body, and symptoms of orthostasis have been observed, including diaphoresis, nausea, presyncope and syncope. G-suits are used after landing, and measures such as exercise and end-of-mission salt and volume loading are performed prophylacticly. The cardiovascular system seems to respond appropriately and adequately to the physiologic requirements of the weightless environment in space. This new homeostatic set point becomes maladaptive during the period of and soon after landing on Earth, but normal function is regained over days to weeks. ENDOCRINE AND ELECTROLYTE CHANGES The fluid shift secondary to the reduction of hydrostatic pressure gradients during spaceflight causes profound 47 changes in the physiologic systems regulating fluid balance. These hormone and electrolyte responses are further complicated by intimate connections with the systems involved in mineral homeostasis, which are also perturbed by the effect of weightlessness on muscles and bones. Over time, the initial diuresis stabilizes and urine osmolarity is actually increased. Evaporative water loss from sweat is decreased, even during exercise. This is thought to be from the development of a sweat film on the skin, inhibiting further sweating in the absence of convective air movement. Renin, angiotensin, and aldosterone levels are elevated during spaceflight (22). Norepinephrine and antidiuretic hormone are also increased (23). In conjunction with a “disuse atrophy” of the musculoskeletal system, spaceflight causes increased urinary excretion of sodium, potassium, calcium, and phosphate (24). Despite some departures from normal Earth-based equilibrium during spaceflight, the observed changes in the endocrine system and fluid and electrolyte balance seem to establish a new non-pathologic steady state and return to functionally normal values after return to the Earth environment. HEMATOLOGIC SYSTEM Plasma volume and red blood cell (RBC) mass have been shown to be decreased post-spaceflight (25). On arrival to a weightless environment, total vascular space is reduced by the initial rapid diuresis. This results in decreased plasma volume and increased hemoglobin concentration, which is followed by a compensatory decrease in erythropoietin production. An optimal equilibrium for the weightless environment is achieved with smaller plasma volume and RBC mass. The functional impairment of this “anemia of spaceflight” is not present during normal spaceflight conditions, but contributes to the orthostatic intolerance upon return to a 1 g environment (the Earth’s gravitational force at sea level g ⫽ 9.81 m/s2) during the first days to weeks after return to Earth. A decreased reserve, however, might impair the physiologic response to hypovolemic shock in microgravity. IMMUNE FUNCTION Human and animal studies have described several factors affecting the immune system during spaceflight. Altered immune function has been linked to microgravity, hypokinesia, the neuroendocrine stress response, radiation exposure, sleep disruption, isolation, and the effects of a closed environment with various gases and airborne contaminants (26). Specific abnormalities in cellular immunity include alterations in leukocyte formation, cytokine 48 L. H. Stewart et al. production, and natural killer cell activity during both short-term and long-term flights (27–29). Down-regulation of cellular immunity may contribute to the reactivation of latent viral infections seen in some astronauts (30). The question remains, however, as to what effect, if any, these alterations have on host susceptibility to infection or neoplasia during spaceflight (31). motion sickness. Space motion sickness (SMS) is a subset of SAS and includes symptoms of flushing, anorexia, nausea, vomiting, and malaise. Space motion sickness usually begins within an hour of flight and lasts no longer than 72 h. The incidence of SMS has been reported to be 50% and 35–70% of crewmembers based on Russian and American experience, respectively (37). Intramuscular promethazine is the current treatment of choice. MUSCULOSKELETAL SYSTEM The absence of weight loading and relative hypokinesia in space results in muscle atony and decreased protein synthesis (32). The tonic effect of passive stretch is also lost. Lower extremity weight-bearing muscles important for ambulation on Earth lose this function in microgravity and therefore undergo significant atrophy. The vertebral column lengthens up to 7 cm in space, and over two-thirds of astronauts report low back pain (33). Like muscle, bone is not static tissue but an active and dynamic organ involved in mineral homeostasis and hematopoiesis, in addition to providing mechanical support for movement. In microgravity, bone mineral density in the legs, pelvis, and lumbar vertebrae decreases by about 1% per month, secondary to both increased bone resorption and decreased formation (34). It is currently unknown whether there is a ceiling to this effect by reaching a new equilibrium during long-duration spaceflights, or if the osteopenia will progress to become a limiting factor on mission duration. The primary effect of lost bone mass would be a substantial increased risk of fracture during strenuous activity and trauma. Extensive research on bed-rest and hypokinesia on Earth suggests that osteopenia can be countered by physical exercise, mineral supplements, and drugs such as bisphosphonates (35). However, data on the recovery of bone mass of astronauts upon return to a 1 g environment are sparse and highly variable between individuals. Early development of osteoporosis on Earth may be a significant concern regarding mission duration. SPACE ADAPTATION SYNDROME Exposure to microgravity provides unique and highly unusual stimuli to human skin, muscle, joint, visual, and vestibular receptors. Until they can adapt to the new environment, space travelers experience abnormalities in movement, coordination, visual gaze, and can have illusions of motion. These physiologic responses to the environment of microgravity have been collectively termed space adaptation syndrome (SAS) (36). The most acutely uncomfortable aspects of SAS are the sensory and autonomic responses that are similar to terrestrial SPACEFLIGHT AND SPACECRAFT ENVIRONMENT The closed cabin spacecraft environment is somewhat similar to that of submarines and to large buildings with the sealed recirculated air responsible for what is known as “tight” or “sick” building syndrome. Even very low levels of volatile organic compounds in recirculated areas have been shown to be deleterious to memory (38). General factors affecting astronaut health include high levels of physical and psychological stressors, and exposure to noise, vibration, and long periods of isolation. Countermeasures to the development of psychological stress include ground-based support and the performance of multiple tasks to stay active. Sleep patterns are disturbed and shortened in duration, with altered circadian zeitgeibers in the spacecraft environment where the Sun appears to “set” approximately every 90 min (39). The low barometric pressure and artificial gas composition of some spacecraft atmospheres can expose crew to factors such as hyper- or hypoxia, hypercapnea, lung atelectasis, altitude decompression sickness, possible explosive decompression, fire, and abnormal heat balance. Toxic exposures are a continuous threat from gaseous and particulate contaminants resulting from human metabolism and waste, chemicals in the spacecraft, propellants, coolants, off-gassing from plastics, and particulate matter (which does not fall to the floor in microgravity). Shuttle astronauts in the 1980s reported mild coughing and eye irritation from dust while exchanging lithium hydroxide air filter cartridges. During the 1975 Apollo-Soyuz mission, an open cabin valve on reentry exposed three crewmembers to nitrogen tetroxide and monomethyl hydrazine. One astronaut lost consciousness; all developed chemical pneumonitis and were hospitalized with pulmonary edema (40). Table 1 lists some potentially toxic substances of particular concern on spacecrafts. Space crews are exposed to significant acceleration vector forces or “g-forces” during routine spaceflight. Launch can achieve up to 5 g (5 ⫻ 9.81 m/s2). Descent and landing generate 3– 8 g, but steep emergency trajectories can lead to more than 20 g (41). Depending on Emergency Medicine in Space 49 Table 1. Potentially Toxic Substances in the Spacecraft Environment Acetaldehyde Acrolein Ammonia 1,3-Butadiene Carbon dioxide Carbon monoxide Dichloroacetylene 1,2-Dichloroethane 2-Ethoxyethanol Formaldehyde Freon 113 Hydrazine Hydrogen Indole Mercury Methane Methanol Methyl ethyl ketone Methyl hydrazine Methylene chloride Nitromethane Octamethyltrisiloxane 2-Propanol Toluene Trichloroethylene Trimethylsilanol Vinyl chloride Xylene multiple factors, a force as little as 4 g is capable of inducing syncope. Radiation exposure is an important occupational risk affecting virtually all of the organ systems. The main sources of ionizing space radiation are the trappedradiation belts, galactic cosmic rays, and solar particle events from solar flares. Significant protection from ionizing radiation is provided by the Earth’s magnetosphere when in near-Earth orbit, but this shield is lost during interplanetary travel. The National Aeronautics and Space Administration (NASA) identified radiation exposure as one of the most pressing challenges to the human space program (42). Efforts to minimize damage include careful navigation planning, antioxidant vitamin supplementation, and repositioning of spacecraft during solar flares. Due to multiple confounding factors and a small experimental population, the long-term genetic and carcinogenic risks are unclear. For practical purposes, the current accepted risk for astronauts is a career limit 3% increased risk of cancer mortality from space activities (43). MEDICAL EMERGENCIES General Considerations Medical equipment, supplies, and hardware selected for use in space must fulfill rigorous specific characteristic requirements based on the remote, isolated, and dangerous environment (44). There are significant space, power, and weight constraints, as well as formative launch costs to put supplies in orbit (approximately $20,000/kg). With the Space Medicine and Healthcare Systems Office, NASA Medical Operations continues to define the optimal training and equipment required for spaceflight. Since Normand Thagard became the first American physician to fly in space, approximately 20 physicians have flown. Despite requests from many of the NASA Medi- cal Operations staff to include physicians in the ISS crew, the crew medical officer currently receives only 20 or 60 h of medical training to serve on the Shuttle and ISS, respectively (analogous to the training of an independent duty corpsman on small naval vessels). As such, the Space Shuttle and ISS are equipped for only minor procedures and basic medical treatment using the supplies manifested on the Shuttle Orbiter Medical System and the ISS Crew Health Care System (45). Table 2 lists examples of the types of oral and parenteral medications currently available. Longer and more remote missions will require more intensive medical training for crew medical officers as well as the other astronauts, who may need to assist during a medical emergency. Imaging Ultrasonography is currently the clinical imaging modality of choice for spaceflight, and is integrated with remote telemetry on the ISS. The equipment is light and useful in a broad range of clinical situations. Unlike radiography, ultrasound images are not affected by the ubiquitous space radiation. Both modalities are subject to the unique physical parameters of microgravity, i.e., there are no air/fluid “levels” and all such familiar gravitydependent radiological signs are unavailable (46). Because ultrasound cannot penetrate bone or lung parenchyma, some form of radiography will likely be part of any self-sufficient medical facility in space. One such Digital Radiographic Imaging System was dropped from the ISS design, due to the power and weight constraints discussed previously (47). Pharmacology Pharmacological aids for space medicine must be selected based on their usefulness for a wide range of indications, effective use in combination, stability in the space environment, and the expected probability of spe- Table 2. Typical Medications Currently Available During Spaceflight Acetaminophen Ampicillin Atropine Dexamethasone Diazepam Diphenhydramine Donnatal Epinephrine Erythromycin Hydroxyzine Cephalexin Lidocaine Meperidine Morphine Nitroglycerine Penicillin Prochlorperazine Promethazine Tetracycline 50 cific disease states. Our knowledge of pharmacodynamics and pharmacokinetics of therapeutic agents in vivo during spaceflight is limited. What we do know suggests that the blood levels of medications may not be predictable using Earth-based data (48). There are numerous factors that may influence drug efficacy, including the many physiologic changes and environmental factors discussed previously. Another important issue is the disturbance of endogenous endocrine and metabolic circadian rhythms. As we gather more data and experience with larger numbers of astronauts and longer missions, an evidence-based approach for medication selection will be desirable. Airway Although airway management has never been necessary during the history of manned spaceflight, there have been cases of aspiration, chemical pneumonitis, and smoke inhalation. As we extend the duration of our orbital missions and embark on interplanetary travel, airway management during respiratory failure, anesthesia for surgical procedures, and treatment of traumatic injuries will be inevitable. A comparison of airway devices using a water immersion model demonstrated no differences in difficulty of placement of the cuffed oropharyngeal airway, laryngeal mask airway, and intubating laryngeal mask airway, with or without stabilizing restraints (49). Laryngoscopy for placement of an endotracheal tube was more prone to failure during free-floating conditions. Based on experience during parabolic flight, grasping the head with one’s knees has been suggested as a technique L. H. Stewart et al. to facilitate laryngoscopy of the unrestrained patient in microgravity (50) (Figure 1). Anesthesia Although there are no direct observations of anesthetic use during human spaceflight, it is clear that astronauts are a unique population subject to significant physiologic and environmental stressors. Anesthetic agents in space must therefore be used with the expectation of a hypovolemic patient with altered regulatory systems and significant skeletal muscle atrophy. It has been suggested that after significant exposure to microgravity, induction be performed with etomidate and midazolam to avoid the hemodynamic effects of other agents (51). In the setting of up to 20% muscle atrophy, succinylcholine use may be relatively contraindicated to avoid hyperkalemia. Unlike the 100% oxygen atmosphere that caused a deadly fire in the Mercury project, supplemental oxygen is safe in the Earth-like atmosphere on current spacecraft. Gas anesthesia cannot be used due to the risk of contamination of the closed-loop atmosphere in a spacecraft. More benign nebulized medications could be used cautiously, with attention to airflow and perhaps using a mask or specialized hood if needed. Spinal anesthetics can flow cephalad in weightlessness and are therefore unpredictable. Therefore, the only practical means of anesthesia in space are local, regional, and intravenous medication delivery (52). Simple procedures such as starting an intravenous line and administering fluids are feasible but have unique technical considerations in the absence of gravity. For example, there is no air-fluid separation in a bag of saline. In space, the air must first be removed, and a pressurized system is necessary for flow. SPECIFIC MEDICAL EMERGENCIES Cardiovascular Emergencies Figure 1. Endotracheal intubation in simulated microgravity during parabolic flight. Used with permission from Dr. William Norfleet and Lippincott Williams and Wilkins, Inc.: (48) Norfleet WT. Anesthetic concerns of spaceflight. Anesthesiology 2000;92(5):1219 –22. The high incidence of ectopy, tachycardia, and other minor dysrhythmias observed during spaceflight have an uncertain etiology but may be related to high catecholamine levels. The predominately young and healthy crew have tolerated these episodes, but the cardiovascular effects of long-duration spaceflight are largely unknown. With the recent advent of commercial space tourism, older and less physically conditioned astronauts will be more commonplace. Burt Rutan’s SpaceshipOne launched the first private astronaut into space in 2004, and Richard Branson plans to develop the ship for ticketed passengers on the first space airline, Virgin Galactic. Eventually, more significant and deleterious cardiac events are ex- Emergency Medicine in Space pected. The ISS has cardiac telemetry capability, and the advanced cardiac life support procedures such as cardiac defibrillation could all be performed. Cardiopulmonary resuscitation (CPR), vascular access, intravenous fluid infusion, bladder catheterization, and gastric tube placement have all been demonstrated experimentally in microgravity (53). Although these procedures can be performed on a spacecraft, modifications are invariably necessary to adapt to the unique environment. For example, in the absence of gravitational assistance, conventional CPR technique is ineffective in generating adequate intrathoracic pressure. Work with mannequins and swine in microgravity suggests the best technique is chest compression of a restrained patient by a rescuer in an upside-down handstand position with arms extended and using the knees to push off the “ceiling” of the spacecraft (Figure 2) (54,55). Although most of the car- 51 diac changes noted in astronauts have been either transient or benign, halogenated hydrocarbons in the environment could theoretically sensitize the myocardium in the setting of a toxic contamination. An automatic external cardiac defibrillator is currently available on the ISS alone. The Space Shuttle cannot be used for emergent evacuation of a critical patient because it takes more than a month to ready the vehicle, and the currently utilized Russian Soyuz escape capsule can take only three persons in a sitting position with no room for any cardiac or other medical support equipment. Infection Despite numerous countermeasures, bacteria, fungi, and viruses are ubiquitous inhabitants of spacecraft. Some of the microorganisms found on spacecraft include Bacillus, Corynebacterium, Enterobacter, Escherichia, Klebsiella, Staphylococcus, Streptococcus, Aspergillus, Mycoplasma, Candida, and Penicillium. Humans are the main source of these organisms. It has been estimated that the average person sheds about 40 billion bacteria daily from skin particles alone (56). All of the Apollo 11 crew reported symptoms suggestive of a viral upper respiratory infection (57). After Apollo 13, routine preflight quarantines have significantly reduced the incidence of infectious diseases during spaceflight. Since then, primarily minor infections such as boils, sty formation, and gingivitis have been reported (58). The depressed immune system in microgravity might result in more serious infections on longer flights. Extravehicular Activity and Dysbarism Figure 2. Chest compressions in simulated microgravity during parabolic flight. Used with permission from Dr. Gregory D. Jay and the Aerospace Medical Society: (54) Jay GD, Lee PHU, Goldsmith H, et al. CPR effectiveness in microgravity: comparison of three positions and a mechanical device. Aviat Space Environ Med 2003;74:1183–9. Since Alexi Leonov made the first “spacewalk” in 1965, extravehicular activity (EVA) has been recognized as one of the most strenuous space environments. Astronauts working outside spacecraft are exposed to higher levels of radiation, increased physical workload with deconditioned and atrophic muscles, altered thermoregulation, and hypobaria. The American space suit for EVA is called the extravehicular mobility unit. It weighs 113 kg on Earth and is difficult to maneuver even in microgravity. To reduce the work required to move in the suit, the internal pressurization is kept at only about 30% of the sea level pressure within the Shuttle. This pressure differential creates the possibility of decompression sickness (DCS). Decompression sickness results from the formation of gas bubbles in tissues exposed to relatively hypobaric environments. The symptoms can be divided into the joint and musculoskeletal pain known as the “bends” (DCS type I), and severe pulmonary, cardiovas- 52 cular and neurologic events (DCS type II). Experimental work in hypobaric chambers suggests an expected 17% incidence of DCS symptoms under simulated space extravehicular activity (59). Perhaps due to the difficulty of differentiating the musculoskeletal discomfort of working during EVA and the symptoms of mild DCS, astronauts have not reported DCS (60). Another confounding factor is astronaut reluctance to report minor medical problems due to concern they might not be selected for future missions. Currently, there is no equipment available for hyperbaric therapy on the ISS. On missions out of near-Earth orbit, a portable hyperbaric chamber could be life-saving. Ultrasonography potentially could be used to detect intravascular bubbles, however, the mere presence of bubbles does not define the clinical syndrome of DCS. Urologic Emergencies The negative calcium balance induced by bone remodeling in space leads to increased urinary calcium. Urine pH and citrate are reduced favoring saturation of calcium salts and the formation of renal calculi (61). Renal colic has occurred during spaceflight and will need to be managed effectively both prophylactically and medically. During the Apollo 13 mission, two astronauts developed urinary tract infections. In-flight treatment with tetracycline was ineffective, and their urine later grew out Pseudomonas aeruginosa (62). Trauma and Surgical Emergencies Although there are significant technical barriers to performing surgery in space, it is feasible. The question is, at what point would it be necessary to have a surgical suite. This threshold becomes lower when evacuation is impossible in the case of interplanetary travel, and extended missions of larger numbers astronauts. Surgery has yet to be performed during spaceflight. One mission was nearly aborted when a cosmonaut developed right lower quadrant abdominal pain thought to be appendicitis, but resolved as an uncomplicated ureterolithiasis (63). The likelihood of a surgical event is expected to increase proportional to the duration of spaceflight. Traumatic injury will be one of the greatest risks to human space exploration, secondary to its expected incidence and the resulting impact on crew health and mission (64). Penetrating trauma will likely occur during EVA, resulting in rapid decompression and death when the space suit integrity is disrupted. This leaves blunt trauma (also most likely during EVA) and subsequent organ L. H. Stewart et al. damage and hemorrhagic shock as the primary concerns during extraterrestrial trauma. The goal of management of traumatic injuries and other serious surgical problems that occur during near-Earth spaceflight is stabilization and damage control pending rapid and safe return to Earth. The Space Shuttle and ISS are only equipped for minor surgical procedures. In the absence of comprehensive onboard surgical capabilities, treatment of severe traumatic injuries will focus on temporizing measures. During long missions when return to Earth is not an option, the most serious traumatic injuries may necessitate comfort care. British and American submarine experience has also shown that many surgical diseases can be approached medically in remote and isolated conditions. Indeed, the current US Navy protocol for appendicitis has a 75% success rate with i.v. antibiotics (65). This could be augmented by percutaneous ultrasound guided catheter drainage if an abscess were to develop on an extended mission. Since the first report of animal laparotomy in the experimental microgravity of parabolic flight in 1967, much work has been done to develop the techniques, procedures and equipment necessary to perform basic surgery in space (66). Some of the important logistic issues include careful restraint of the physician, patient and supplies during weightlessness, maintenance of sterile technique, and trash disposal (67). Due to the lack of gravity, the atmospheric particle count on the ISS is almost 10 times that of a conventional operating room (68). Because of surface tension and the formation of fluid domes, hemorrhage is easily located and does not contaminate the environment. Laparotomy, large vessel repair and wound closure have not been found to be significantly more difficult during weightlessness despite the tendency of the bowels to float up against the abdominal wall (69). On the STS-90 Neurolab Shuttle mission, astronauts working with rats demonstrated intramuscular anesthesia, dissection, hemostatis, and wound closure to be feasible and no more difficult than in a 1 g environment (70). The standard advanced trauma life support (ATLS) procedures have been demonstrated to be feasible in microgravity, using animal models and standard equipment manifested on the ISS (71). Procedures that were not significantly more technically difficult to perform in microgravity than in a 1 g environment included: intravenous fluid infusion, Foley catheter drainage, laceration closure, artificial endotracheal ventilation, chest tube insertion and suction, percutaneous tracheostomy, and crichothyrotomy. Percutaneous diagnostic peritoneal lavage had an increased risk of bowel perforation secondary to the bowel floating up against the anterior peritoneum in the 0 g environment. This procedure may be replaced by Emergency Medicine in Space abdominal sonography for the identification of intraperitoneal fluid in space. Because hemorrhage is the primary cause of death from traumatic injuries on Earth, effective fluid resuscitation will likely be vital to the management of trauma victims in space. Currently, normal saline is the only intravenous fluid manifested on the Space Shuttle and ISS. Hypertonic saline and hemoglobin-based oxygen carriers may eventually replace normal saline, with the goal of selecting therapies with the greatest efficacy to mass ratio (72). An important consideration during extraterrestrial shock is the exposure to g-forces if emergency descent is necessary. A crew member with decreased intravascular volume already in shock might then sustain significant secondary end-organ insult with prolonged tissue hypoxia. Hypoxic and traumatic brain injury could also be exacerbated by the underlying decreased cerebrovascular tone that has been noted, as well as the inability to “elevate” the head to decrease intracranial pressure in space (73). CONCLUSIONS Spaceflight presents a unique and challenging medical setting with complex physiologic changes and extreme environmental conditions. Over the last century we have learned a tremendous amount about human adaptation to microgravity and the rigors of spaceflight. But this is only the beginning of this frontier of medicine; and there is much to learn as more humans travel to and spend more time in space. Selection of preventive and therapeutic strategies for illness has long been driven by Earth-based medical support. This has worked well for near-Earth orbit missions, when consultation can be obtained, communication is relatively constant, and reentry to Earth is a viable possibility. Nevertheless, the presence of a physician will always broaden the capabilities of in-flight medical care independent of the availability of ground support. As we explore further into our solar system, ground-based medical support will no longer be possible when acute medical decision-making is required and return to Earth is not an option. Pending the permanent inhabitation of space stations or lunar bases with sub-specialized physicians and advanced surgical equipment, a broadly trained physician will be needed with a diverse range of medical and surgical capabilities. Emergency physicians possess these diverse skills and would be well suited to fill the function of a physician-astronaut in the unique medical environment of space. 53 REFERENCES 1. Grigoriev AI, Orlov OI. Commentary: telemedicine and spaceflight. Aviat Space Environ Med 2002;73:688 –93. 2. Gontcharov IB, Kovachevich IV, Pool SL, et al. Short communication: medical care system for NASA-Mir spaceflights. Aviat Space Med 2002;73:1219 –23. 3. Thomas TL, Garland FC, Mole D, et al. Health of U.S. submarine crew during periods of isolation. Aviat Space Environ Med 2003; 74:260 –5. 4. Tansley WA, Wilson JM, Schaefer KE. Analysis of health data from 10 years of Polaris submarine patrols. Undersea Biomed Res Submar Suppl 1979;S217– 46. 5. Harnett BM, Doarn CR, Russell KM, et al. Wireless telemetry and Internet technologies for medical management: a Martian analogy. Aviat Space Environ Med 2001;72:1125–31. 6. Medical Operations Branch. International Space Station Crew Medical Officer Training Syllabus. Houston, TX. NASA Johnson Space Center; 1998. 7. Pestov ID. Principles of gravitational biology. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 1. Reston, VA: AIAA; 1996:1–30. 8. Nicogossian AE, Mohler S, Gazenko O, Grigoriev A. Humans in spaceflight. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3. Reston, VA: AIAA; 1996:1–594. 9. Harris BA, Billica RD, Roger D, et al. Physical examination during spaceflight. Mayo Clin Proc 1997;72:301– 8. 10. Gibson EG. Skylab-4 crew observations. In: Johnston RS, Dietlein LF, eds. Biomedical results from Skylab, NASA SP-377. Washington, DC: US Government Printing Office; 1977:22– 6. 11. Buckey J, Gaffney F, Lane L, et al. Central venous pressure in space. N Engl J Med 1993;328:1853– 4. 12. Kotovskaya AR, Simpura AR, Vartbaranov RV. Human physiologic reactions under the action of transverse accelerations after hypodynamia. Probl Kosm Biol 1967;6:106 –17 (Also NASA TTF528, 1969). 13. Hoffler GW, Wolthuis RA, Johnson RL. Apollo space crew cardiovascular evaluations. Aerosp Med 1974;45:807–20. 14. Catterson AD, McCutcheon EP, Minners HA, et al. Aeromedical observations. Mercury Project Summary, NASA SP-45. Washington, DC: US Government Printing Office; 1963:299 –326. 15. Martin DS, South DA, Wood ML, et al. Comparison of echocardiographic changes after short- and long-duration spaceflight. Aviat Space Environ Med 2002;73:532– 6. 16. Charles JB, Frey MA, Fritsch-Yelle JM, et al. Cardiovascular and cardiorespiratory function. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 1. Reston, VA: AIAA; 1996:63– 88. 17. D’Aunno DS, Dougherty AH, DeBlock HF, et al. Effect of shortand long-duration spaceflight on QTc intervals in healthy astronauts. Am J Cardiol 2003;91:494 –7. 18. Fritsch-Yelle JM, Leuenberger UA, D’Aunno DS, et al. An episode of ventricular tachycardia during long-duration spaceflight. Am J Cardiol 1998;81:1391–2. 19. Mills PJ, Meck JV, Waters WW, et al. Peripheral leukocyte subpopulations and catecholamine levels in astronauts as a function of mission duration. Psychosom Med 2001;63:886 –90. 20. Bjornstad H, Storstein L, Dyre Meen H, et al. Electrocardiographic findings of heart rate and conduction times in athletic students and sedentary control subjects. Cardiology 1993;83:258 – 67. 21. George KP, Wolfe LA, Burggraf GW. The ‘athletic heart syndrome’. A critical review. Sports Med 1991;11:300 –30. 22. Drummer C, Norsk P, Heer M. Water and sodium balance in space. Am J Kidney Dis 2001;38:684 –90. 23. Christensen NJ, Drummer C, Norsk P. Renal and sympathoadrenal responses in space. Am J Kidney Dis 2001;38:679 – 83. 24. Huntoon CSL, Cintron NM. Endocrine system and fluid and electrolyte balance. In: Nicogossian AE, Gazenko OG, eds. Space 54 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. L. H. Stewart et al. biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 1. Reston, VA: AIAA; 1996:89 –104. Johnson PC. The erythropoietic effects of weightlessness. In: Dunn CDR, ed. Current concepts in erythropoiesis. New York: John Wiley and Sons Ltd; 1983:279 –300. Konstantinova IV. Immune system. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 1. Reston, VA: AIAA; 1996: 117–33. Tipton CM, Greenleaf JE, Jackson CGR. Neuroendocrine and immune system responses with spaceflights. Med Sci Sports Exerc 1996;28:988 –98. Talor GR, Konstantinova IV, Sonnenfeld G, et al. Changes in the immune system during and after spaceflight. Adv Space Biol Med 1997;6:1–32. Sonnenfeld G. Extreme environments and the immune system: effects of spaceflight on immune responses. J Allergy Clin Immunol 2001;107:19 –20. Stowe RP, Mehta SK, Ferrando AA, et al. Immune responses and latent herpesvirus reactivation in spaceflight. Aviat Space Environ Med 2001;72:884 –91. Committee on Space Biology and Medicine. A strategy for research for space biology and medicine for the new century. Washington, DC. Space Studies Board, National Research Council, National Academy of Sciences; 1998. Kozlovskaya IB, Shenkman BS. Muscle structure and metabolism. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 1. Reston, VA: AIAA; 1996:231– 46. Wing PC, Tsang IKY, Susack L, et al. Back pain and spinal changes in microgravity. Orthop Clin North Am 1991;22:255– 6. Oganov VS, Schneider VS. Skeletal system. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 1. Reston, VA: AIAA; 1996:247– 66. Grigoriev AI, Morukov BV, Oganov VS, et al. Effect of exercise and bisphosphonate on mineral balance and bone density during 360-day antiorthostatic hypokinesia. J Bone Min Res 1992;7: S449 –55. Homick JL, Reschke MF, Vanderploeg JM. Space adaptation syndrome. Incidence and operational implications for the space transportation system program. In: Motion sickness: mechanisms, prediction, prevention, and treatment, CP-372.Williamsburg, VA: Advisory Group for Aerospace Research; 1984. Reschke MF, Kornilova LN, Harm DL, et al. Neurosensory and sensory-motor function. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 1. Reston, VA: AIAA; 1996:135–93. Molhave L, Bach B, Pederson OF. Human reactions to low concentrations of volatile organic compounds. Environ Int 1986;12: 167–75. Gundel A, Polyakov VV, Zolly J. The alteration of human sleep and circadian rhythms during spaceflight. J Sleep Res 1997;6:1– 8. Dejournette R. Rocket propellant inhalation in the Apollo-Soyuz astronauts. Radiology 1977;125:21– 4. Kotovskaya AR, Vartbaronov RA. Sustained linear acceleration. In: Nicogossian AE, Gazenko OG, eds. Space biology and medicine, joint US/Russian publication in five volumes, vol. 3, book 2. Reston, VA: AIAA; 1996:279 –313. DeCampi W. Radiation. In. Exploring the universe, a strategy for space life sciences. Washington, DC: NASA; 1988:53– 66. National Research Council, National Council on Radiation Protection and Measurements.Guidance on radiation received in space activities. Report number 98. Washington, DC: National Academy Press; 1989. Houtchens BA. Medical care systems for long-duration space missions. Clin Chem 1993;39:13–21. Barratt M. Medical support for the International Space Station. Aviat Space Environ Med 1999;70:155– 61. Hart R, Campbell MR. Technical note: digital radiography in space. Aviat Space Environ Med 2002;73:601– 6. View publication stats 47. Billica RD, Doarn CR. A health maintenance facility for space station freedom. Cutis 1991;48:315– 8. 48. Putcha L, Cintron NM. Pharmacokinetic consequences of space flights. Ann N Y Acad Sci 1991;618:615– 8. 49. Keller C, Brimacombe J, Giampalmo M, et al. Airway management during spaceflight: a comparison of four airway devices in simulated microgravity. Anesthesiology 2000;92:1237– 41. 50. Norfleet WT. Anesthetic concerns of spaceflight. Anesthesiology 2000;92:1219 –22. 51. Agnew JW, Fibuch EE, Hubbard JD. Anesthesia during and after exposure to microgravity. Aviat Space Environ Med 2004; 75:571– 80. 52. Stazhadze LL, Goncharov IB, Neumyzakin IP, et al. Anesthesia, surgical aid and resuscitiation in manned space missions. Acta Astronaut 1981:8:1109 –10. 53. McCuaig KE, Houtchens BA. Management of trauma and emergency surgery in space. J Trauma 1992;33:610 –25. 54. Jay GD, Lee PHU, Goldsmith H, et al. CPR effectiveness in microgravity: comparison of three positions and a mechanical device. Aviat Space Environ Med 2003;74:1183–9. 55. Johnston SL, Campbell MR, Billica RD, et al. Cardiopulmonary resuscitation in microgravity: efficacy in the swine during parabolic flight. Aviat Space Environ Med 2004;75:546 –50. 56. Mims CA. The pathogenesis of infectious disease, 3rd edn. New York: Academic Press; 1987:8 – 47. 57. Berry CA. Summary of medical experience in the Apollo 7-11 manned spaceflights. Aerosp Med 1970;41:500 –19. 58. Taylor GR, Graves RC, Brockett RM, et al. Skylab environmental and crew microbiology studies. In: Johnston RS, Dietlein LF, eds. Biomedical results from Skylab. NASA SP-377. Washington, DC: NASA; 1977:53– 63. 59. Kumar KV, Waligora JM, Powell MR. Epidemiology of decompression sickness under simulated space extravehicular activities. Aviat Space Environ Med 1993;64:1032–9. 60. Cowell SA, Stocks JM, Evans DJ, et al. Review article: the exercise and environmental physiology of extravehicular activity. Aviat Space Environ Med 2002;73:54 – 67. 61. Whitson PA. Renal stone risk assessment during Space Shuttle flights. J Urol 1997;158:2305–10. 62. Berry CA. Medical legacy of Apollo. Aerosp Med 1974;45:1046 –57. 63. Lebedev V. Diary of a cosmonaut. 211 days in space. New York: Bantam Books; 1983. 64. Billica RD, Pool SL, Nicogossian AE. Crew health care programs. In: Nicogossian AE, Huntoon CL, Pool SL, eds. Space physiology and medicine, 3rd edn. Baltimore, MD: Williams & Wilkins; 1994: 402–23. 65. Campbell MR. Surgical care in space. Aviat Space Environ Med 1999;70:181– 4. 66. Yaroshenko GL, Terentyev BG, Mokrov MN. Characteristics of surgical intervention in conditions of weightlessness. Voen Med Zh 1967;10:69. 67. Campbell MR, Dawson DL, Melton S, et al. Surgical instrument restraint in weightlessness. Aviat Space Environ Med 2001;72: 871– 6. 68. Campbell MR, Billica RD. A review of microgravity surgical investigations. Aviat Space Environ Med 1992;63:524 – 8. 69. Campbell MR, Billica RD, Johnston SL III. Animal surgery in microgravity. Aviat Space Environ Med 1993;64:58 – 62. 70. Campbell MR, Williams DR, Buckey JC Jr, Kirkpatrick AW. Animal surgery during spaceflight on the Neurolab Shuttle mission. Aviat Space Environ Med 2005;76:589 –93. 71. Campbell MR, Billica RD, Johnston SL III, et al. Technical note: performance of advanced trauma life support procedures in microgravity. Aviat Space Environ Med 2002;73:907–12. 72. Kirkpatrick AW, Dulchavsky SA, Boulanger BR, et al. Extraterrestrial resuscitation of hemorrhagic shock: fluids. J Trauma 2001; 50:162– 8. 73. Turchaninova VF, Domracheva MV. Results of studies of pulsed blood flow and regional vascular tonus during flight in the first and second expeditions aboard the Salyut 6-Soyuz orbital complex. Kosm Biol Aviakosm Med 1980;14:11– 4.