ADVERSE CUTANEOUS DRUG
REACTION 51
ADVERSE CUTANEOUS DRUG REACTIONS IC0:10:T88.7
• Adverse cutaneous drug reactions (ACDRs) are unpredictable They affect 2 to 3% of inpatients and
lead to 0.1 to 0.396 of hospital fatalities.
• In the United States, adverse drug events account for up to 140,000 deaths and $136 billion In costs
annually.
• Most reactions are mild, accompanied by pruritus, and resolve promptly after the offending drug is
discontinued.
• Drug eruptions can mimic virtually all the morphologic expressions in dermatology and must be the first
consideration In the differential diagnosis ofa suddenly appearing eTUptlon.
• Drug eruptions are caused by immunologic or nonimmunologic mechanisms and are provoked by
systemic or topical administration of a drug.
• The majolity are based on a hypersensitivity mechanism and are thus immunologic and may be of
types I, II, Ill, or IV.
CLASSIFICATION
IMMUNOLOGICALLY MEDIATED ACDII.
(see 'llablt: »-1) It should be noted that in
most reactions both cellular and humoral
immune reactions are Involved. Nonimmun~
logic reactions are summarized in Table 23-2.
GUIDELINES FOR ASSESSMENT
OF POSSIBLE ACDRS
• Bxdwie alternative causes, especially
infections (most commonly viral).
• Examine interval between introduction of a
drug and onset of the reaction.
• Note any improvement after drug
withdrawal.
• Determine whether similar reactions have
been a&SOciated with the same compound.
• Note any reaction on readmJnlstration of the
drug.
FINDINGS INDICATING POSSIBLE
• Fadal edema or central faclal. involvement
• Palmar/plantar paiDful erythema.
• Epidermal detachment and blisters.
• Positive Nikolsky sign.
• MucoUB membrane erosiWlS.
• Urticaria.
• Swelling of the tongue.
• High fever (temperature >.W"C).
• Enlarged. lymph nodes.
• Arthralgia.
• Shortness of breath. wheezing, and
hypotension.
• Palpable purpura.
• Skin necrosis.
CLINICAL TYPES OF ADVERSE
DRUG REACTIONS
ACDR.s can be exanthematous and can manifelt as urticaria/angioedema, anaphylaxis, and
anaphylactoid react:iWlS, or serwu sickness.
They can mimic: other dermatoses and they can
LIFE-THREATENING ACDR
also present as cutaneous necrosis, pigmentation, alopecia. and hypertrichosis. They can
• Skinpaln.
• Comluent erythema.
indu.ce nail changes. An overview is presented
in Tables 23-3 and 23-4.
'Skin reactio.us or clwige3 .reguhlrly ocx:urriDg a1\er high d.oee or prolonged admininration of~ drugs lib glo~­
all'tkolda, retinoid&, cydoaporlne, and others are not discussed In this section but throupout the book whenever these
drop are dlsGussed.ln greater deta1l.
489
PART II DERMATOLOGY AND INTERNAL MEDICINE
TABLE 23-1 Immunologically Mediated Adverse Cutaneous Drug Reactions*
Type of Reaction Pathogenesis
Examples of
Causative Drug
Type I
lgE-mediated; immediatetype Immunologic
reactions
Penicillin, other
antibiotics
Type II
Drug+ cytotoxic antibodies Penicillin,
cause lysis of cells such as
sulfonamides,
platelets or leukocytes
quinidine,
Isoniazid
Type Ill
lgG or lgM antibodies
formed to drug; immune
complexes deposited
in small vessels
activate complement
and recruitment of
granulocytes
Type IV
Cell-mediated immune
Sulfamethoxazole,
reaction; sensitized
anticonvulsa nts,
lymphocytes react with
allopurinol
drug, liberating cytokines,
which trigger cutaneous
inflammatory response-
lmmunoglobullns,
antibiotics,
rituximab,
infliximab
Clinical Patterns
Urticaria/angioedema of
skin/mucosa, edema
of other organs, and
anaphylactic shock
Petechiae due to
thrombocytopenic
purpura, drug-induced
pemphigus
Vasculitis, urticaria, serum
sickness
Morbilliform exanthematous
reactions, fixed drug
eruption, lichenoid
eruptions, StevensJohnson syndrome, toxic
epidermal necrolysis
*After the Gell and Coombs classification of immune reactions.
**For contact sensitivity see Section 2.
TABLE 23-2 Nonimmunologic Drug Reactions
Idiosyncrasy
Reactions due to hereditary enzyme deficiencies
lndMdual idiosyncrasy to a topical or systemic drug
Mechanisms not yet known
Cumulation
Reactions are dose dependent, based on the
total amount of drug ingested: pigmentation
due to gold, amiodarone, or minocycline
Reactions due to combination ofa drug with
ultraviolet irradiation (photosensitivity)
Reactions have a toxic pathogenesis but can also
be immunologic in nature (see Section 10)
l"itancy/toxicity of a topically applied drug
5-Fiuorouracil, imiquimod
Atrophy by topically applied drug
Glucocorticoids
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
TABLE 23-3 Types of Clinical ACDRs
Drugs
Comment
Exanthematous
reactions
Any
Most common; initial reaction usually
< 14 days after drug intake; recurs
after rechallenge (see page 494);
Urticaria/
angioedema
See Table 23-4
Second most common; usually within
36 h after Initial exposure; within
minutes after rechallenge (see
page 498) (Figs. 22-6 and 22-7)
Fixed drug eruptions
See Table 23-6
Third most common, see page 499
Anaphylaxis and
anaphylactoid
reactions
Antibiotics, extracts of allergens,
radlocontrast media, monoclonal
antibodies (see Table 23-5)
Most serious type of ACDR, within
minutes and hours; more common
with oral than parenteral drug
administration.
Intermittent administration of drug
may predispose to anaphylaxis
Serum sickness
IVIg, antibiotics, bovine serum
albumin (used for oocyte
retrieval in in vitro fertilization),
cefaclor, cefprozil, bupropion,
minocycline, rituximab,
infliximab
5-21 days after initial exposure
Minor form: fever, urticaria, arthralgia
Major (complete) form: fever, urticaria,
angioedema, arthralgia, arthritis,
lymphadenopathy, eosinophilia,
± nephritis, ± endocarditis.
Type
Basic Reactions
TABLE 23-4 ACDR Mimicry of Other Dermatoses
Drugs
Comment
Acneiform eruption
Glucocorticoids, anabolic steroids,
contraceptives, halogens,
isoniazid, lithium, azathioprine,
danazol, erlotinib
Mimics acne. See Section 1 and
page496
Bullous eruptions
Naproxen, nalidixic acid, furosemide,
oxaprozin, penicillamine,
piroxicam, tetracyclines
Mimics fixed drug eruption, druginduced vasculitis, StevensJohnson syndrome (SJS), toxic
epidermal necrolysis (TEN),
porphyria, pseudoporphyria,
drug-induced pemphigus, druginduced pemphigoid, druginduced linear lgA disease, bullae
over pressure areas in sedated
patients
Dermatomyositis-like
reactions
Penicillamine, NSAIDs,
carbamazepine, hydroxyurea
Mimics dermatomyositis. See
Section 14
Drug hypersensitivity
syndrome
Antiepileptic drugs, sulfonamides,
and others
Mimics exanthematous reactions;
systemic involvement (see
page 501)
Type
Basic Reactions
(continued)
PART II DERMATOLOGY AND INTERNAL MEDICINE
TABLE 23-4 ACDR Mimicry of Other Dermatoses (Continued)
Type
Drugs
Comment
Eczematous eruptions
Ethylenediamine, antihistamines,
aminophylline/aminophylline
suppositories; procaine/
benzocaine; iodides, iodinated
organic compounds, radiographic
contrast media/iodine;
streptomycin, kanamycin,
paromomycin, gentamicin/
neomycin sulfate; nitroglycerin
tablets/nitroglycerin ointment;
disulfirarn/thiuram
Systemic administration of a drug
to an individual who has been
previously sensitized to the
drug by topica I application
can provoke a widespread
eczematous dermatitis (systemic
contact-type dermatitis, see
Section 2) or urticaria
Erythema multiforme,
SJS, TEN
Anticonvulsants, sulfonamides,
allopurinol, NSAIDs (piroxicam)
See Sections 8 and 14
Erythema nodosum
Sulfonamides, other antimicrobial
agents, analgesics, oral
contraceptives, granulocyte
colony-stimulating factor (G-CSF)
See Section 7
Exfoliative dermatitis
and erythroderma
Sulfonamides, antimalarials,
phenytoin, penlclllln
See Section 8
Lichenoid eruptions
(resemble lichen
planus)
Gold, beta-blockers, ACE inhibitors,
especially captopril; antimalarials,
thiazide diuretics, furosemid,
spironolactone, penicillamine,
calcium-channel blockers,
carbamazeplne, lithium,
sulfonylurea, allopurinol
See Section 14
May be extensive, occurring weeks
to months after initiation of
drug therapy; may progress to
exfoliative dermatitis
Adnexal involvement may result in
alopecia, anhidrosis
Resolution after discontinuation
slow, 1-4 months; up to 24
months after gold
Lupus erythematosus
(LE)
Procainamide, hydralazine, isoniazid,
minocycllne, acebutolol, Ca2+
channel blockers, ACE Inhibitors,
docetaxel
See Section 14
5% of cases of systemic LE are drugInduced
Cutaneous manifestations,
including photosensitivity;
however, urticaria, erythema
multiforme-like lesions, Raynaud
phenomenon are not common
Necrosis
Warfarin, heparin, Interferon-a.
cytotoxic agents
Seepage506
Photosensitivity
See Tables 10-4 to 1o-6
See Section 10
Phototoxrc, photoallerglc, or
photocontact
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
TABLE 23-4 ACDR Mimicry of Other Dermatoses (Continued)
Type
Drugs
Comment
Pigmentary disorders
Amiodarone, minocycline,
antimalarials, cytotoxic agents
Seepage502
Pityriasis rosea-like
eruptions
Gold, captopril, imatinib, and others
For clinical appearance, see
Section 3
Pseudolymphoma
Phenytoin, carbamazepine,
allopurinol, antidepressants,
phenothiazines, benzodiazepine,
antihistamines, beta-blockers,
lipid-lowering agents,
cyclosporine, o-penicillamine
Papular eruptions with a histology
mimicking lymphoma
Pseudoporphyria
Tetracycline, furosemide, naproxen
See Section 10 and page 505
Psoriasiform eruption
Antimalarials, beta-blockers,
lithium salts, NSAIDs, interferon,
penicillamine, methyldopa
See Section 3
Purpura
Penicillin, sulfonamides, quinine,
isoniazid
See Section 20
Hemorrhage into morbilliform ACDR
occurs not uncommonly on the
legs
Progressive pigmented purpura also
reported associated with drugs
(see Section 14)
Pustular eruptions
Ampicillin, amoxicill in, macrol ides,
tetracyclines, beta-blockers, Cal+
channel blockers
EGFR Inhibitors (Fig. 23-4)
Acute generalized exanthematous
pustulosis (AGEP, page 496) Must
be differentiated from pustular
psoriasis; eosinophil In the
inti ltrate suggests AGEP
Scleroderma-like
reactions
Penicillamine, bleomycin,
bromocriptine, Na-valproate,
5-hyd roxytryptophan, docetaxel,
gemcitabine, acetanilidecontaining rapeseed cooking oil
See Section 14
Sweet syndrome
All-trans retinoic acid, contraceptives, See Section 7
G-CSF, granulocyte-macrophage
CSF (GM-CSF), minocycline,
lmatlnlb, trlmethoprimsu lfamethoxazole
Vasculitis
Propylthiouracil, hydralazine, G-CSF,
GM-CSF, allopurinol, cefaclor,
minocycline, penicillamine,
phenytoin, isotretinoin
See Section 14
PART II DERMATOLOGY AND INTERNAL MEDICINE
EXANTHEMATOUS DRUG REACTIONS ICD-10:T88.7
• An exanthematous drug reaction {EDR) {eruption) is an adverse hypersensitivity reaction to an
ingested or parenterally administered drug that mimics a measles-like viral exanthem.
• Most common type of cutaneous drug reaction.
• Systemic involvement is low.
• Drugs with a high probability ofreaction {3 to 5%): Penicillin and related antibiotics, carbamazepine,
allopurinol, and gold salts {10 to 20%). Medium probability. Sulfonamides {bacteriostatic, antidiabetic,
diuretic), nonsteroidal anti-inflammatory drugs {NSAIDs), hydantoin derivatives, isoniazid, chloramphenicol, erythromycin, and streptomycin. Low probability {< 1%): Barbiturates, benzodiazepines,
phenothiazines, and tetracyclines.
• Prior Drug Sensitization. Patients with a prior history of exanthematous drug eruption will most
likely develop a similar reaction if rechallenged with the same drug.
• Sensitization occurs during administration or after completing the course of drugs; peak incidence is
usually at ninth day after administration. However, EDR may occur at any time between the first day and
3 weeks after the beginning of treatment. Reaction to penicillin can begin ~2 weeks after drug is discontinued. In previously sensitized patient. eruption starts within 2 or 3 days after readministration of drug.
• Usually quite pruritic. Painful skin lesions suggest development of a more serious ACDR. such as toxic
epidermal necrolysis {TEN).
• Systems Review. ± Fever and chills.
• Skin Lesions. Macules and/or papules, a few millimeters to 1 em in size (Fig. 23-1 ). Bright or'drug•
red. In time, lesions become confluent forming large macules, polycyclidgyrate erythema, reticular
eruptions, sheet-like erythema {Fig. 23-1), or erythroderma; also erythema multiforme-like. Purpura
may be seen in lesions of the lower legs. In individuals with thrombocytopenia, exanthematous
eruptions can mimic vasculitis because ofintralesional hemorrhage. Scaling and/or desquamation
may occur with healing.
• Distribution. Symmetric {Fig. 23-1 ). AI most always occurs on the trunk and extremities. In children,
it may be limited to the face and extremities.
• Mucous Membranes. Enanthem on buccal mucosa.
• Laboratory. Peripheral eosinophilia. Dermatopathology: Perivascular lymphocytes and eosinophils.
• Differential diagnosis includes all exanthematous eruptions: Viral exanthem, secondary syphilis, atypical pityriasis rosea, and early widespread allergic contact dermatitis.
• After discontinuation of the drug, the rash usually fades. However, it may worsen for a few days. The
eruption may also begin after the drug has been discontinued. Eruption usually recurs with rechallenge.
• The definitive step in management is to identify the offending drug and discontinue it. Oral antihistamine can alleviate pruritus. Glucocortlcoids. Potent Topical Preparation, Oral or N. lfthe offending
drug cannot be substituted or omitted, systemic glucocorticoids can be administered to treat the
ACDR. Prevention. Patients must be aware of their specific drug hypersensitivity and that other
drugs of the same class can cross-react. Wearing a medical alert bracelet is advised.
REACTIONS TO SPECIFIC
DRUGS (SELECTED)
AllopurinoL Incidence: 5%. Begins on the
face, spreads rapidly to all areas; may occur in
photodistribution. Onset: 2 to 3 weeks after
initiation of therapy. Associated findings: Facial
edema; systemic vasculitis, especially involving
kidneys. The rash may fade in spite of continued administration.
Ampicillin, Amoxidllin. In up to 100% of
patients with EBV or CMV mononucleosis
syndrome. Increased incidence of EDR to
penicillins in patients taking allopurinol. Ten
percent cross-react with cephalosporins.
Carbamazepine. Morphology: diffuse erythema; severe erythroderma may follow. Site:
Begins on the face, then spreads rapidly to all
areas; may occur in photodistribution. Onset:
2 weeks after initiation of therapy. Associated
findings: Facial edema.
Hydantoin Derivatives. Macular -+ contl.uent erythema. Begins on the face, then spreads
to trunk and extremities. Onset: 2 weeks after
initiation of therapy. Associated findings: Fever,
peripheral eosinophilia; facial edema; lymphadenopathy (can mimic lymphoma histologically).
Sulfonamides. Occurs in up to 50 to 60% of
HIVI AIDS-infected patients (trimethoprirn
sulfarnethoxazole). Patients sensitized to one
sulfa-based drug may cross-react with another
sulfa drug in 20%.
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
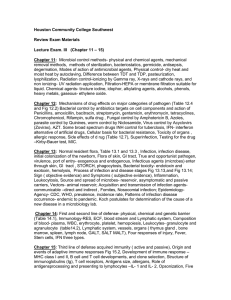
FIGURE 23-1 Exllrrthernatous drug eruption: ampldllln Symmetrically arranged,
brightly erythematous macules and papules, discrete in some areas, and confluent in others,
on the trunk and the extremities.
PART II DERMATOLOGY AND INTERNAL MEDICINE
PUSTULAR ERUPTIONS ICD-1 0; 188.7
• Acute generalized exonthemotous pusrulosls (AGEP) Is an acute febrile eruption that Is often associated
with leukocytosis (Fig. 23·2). Afrer drug administration, it may take 1 to 3 weeks before skin lesions
appear. However; in previously sensitized patients, the skin symptoms may occur within 2 to 3 days.
• Onset is acute, most often following drug intake, but viral infections can also trigger the disease.
• AGEP typically presents with nonfollicular sterile pustules occurring on a diffuse, edematous erythema (Fig. 23·2).
• May be irregularly dispersed (Fig. 23·2) or grouped (Fig. 23·3), usually starting in the folds and/or
the face.
• Fever and elevated blood neutrophils are common.
• Histopathology typically shows spongiform subcomeal and/or intraepidermal pustules; a marked
edema of the papillary dermis; and eventually vasculitis, eoslnophlls, and/or focal necrosis of
keratinocytes.
• Pustules resolve spontaneously in < 15 days and generalized desquamation occurs approximately
2 weeks later.
• Differential diagnosis includes pustular psoriasis, the hypersensitivity syndrome reaction with pustu·
latlon, subcomeal pustular dermatosis (Sneddon-WIIklnson disease), and pustular vasculitis.
• Acneiform pustular eruptions (see Section 1) are associated with iodides, bromides, adrenocorticotropic hormone (ACTH), glucocorticoids, isoniazid, androgens, lithium, actinomycin 0, and phe·
nytoin. The EGFR tyrosine kinase inhibitors erlotinib, gefitinib, cetuximab, and panitumumab produce
pustules that are acneiform but without comedos and erupt in the face {Fig. 23-4) but can erupt
also In atypical areas, such as on the arms and legs. and are most often monomorphous.
FIGURE 23·2 Pustular drug eruption: amte ,enerallzed exanthematous pustulosis (AGEP)
Multiple tiny nonfolllcular pustules against the background of diffuse erythema that tlrst appeared In the
large folds and then covered the entire trunk and the face.
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
FIGURE 23·3 Pustular drug eruption:
AGEP Multiple sterile pustules surrounded by fiery-red erythema in a
S~ear~ld female who had fever and
leukocytosis. In contrast to the disseminated pustules In Fig. 23·2, here the pustules show a tendency for grouping and
confluence. Differential diagnosis of von
Zumbusch pustular psoriasis {compare
with Fig. 3-12).
FIGURE 23-4 Pustular drug eruption:
erlotinlb This pustular eruption
occurred in a patient who had received
an anti-EGR monoclonal antibody for
cancer of the colon localfzed to face. Differential diagnosis to acne and rosacea.
PART II DERMATOLOGY AND INTERNAL MEDICINE
DRUG·INDUCED ACUTE URTICARIA, ANGIOEDEMA,
EDEMA, AND ANAPHYLAXIS (see also sectlon 14)
• Drug-Induced urticaria and angioedema occur, caused by a variety of mechanisms (see lllble 23·1)
and are characterized dinically by transient wheals (see Fig. 1~) and angioedema causing extensive tissue swelling with involvement of deep dermal and subcutaneous tissues. Angioedema is
often pronounced on the face (Fig. 23-SA) or mucous membranes (tongue, Fig. 23-SB).
• In some cases, cutaneous urticaria/angioedema Is associated with systemic anaphylaxis, which Is
manifested by respiratory distress, vascular collapse, and/or shock.
• Drugs causing urticaria/angioedema and anaphylaxis are listed in Table 23·5.
• lima from Initial Drug Exposure to Appearance of Urticaria
• lgE-Mediated. Initial sensitization, usually 7 to 14 days. In previously sensitized individuals, usually
within minutes or hours.
• Immune Complex-Mediated. Initial sensitization, usually 7 to 10 days, but as long as 28 days; in previously sensitized individuals, 12 to 36 h.
• Analgesics/Anti-Inflammatory Drugs. 20 to 30 min (up to 4 h).
• Prior Drug Exposure. Radiographic Controst Media. 25 to 35% probability of repeat reaction in
Individuals w!th history of prior reaction to contrast media.
• Skln Symptoms. Pruritus, burning of palms, and soles with airway edema difficulties breathing.
• Constitutional Symptoms.lgE-mediated: Flushing, sudden fatigue, yawning, headache, weakness,
and dizziness; numbness of tongue, sneezing, bronchospasm, substernal pressure, and palpitations;
nausea, vomiting, crampy abdominal pain, diarrhea, and possibly arthralgia.
Drug-induced urticaria/angioedema usually
resolves within hours, days, or weeks after the
causative drug is withdraWIL
MANAGEMENT Identify and withdraw o1fendillg drugs. Antihistaminea. H1 blockers
or H,_ blockers or combination. Systemic
Gluc:ocortlcoidslntravmotU. Hydrocortisone or methylprednisolone for severe
symptoms. OraL Prednisone, 70 mg, tapering
by 10 or S mg daily over 1 to 2 weeks, is
A
usually adequate. In A£ute Severe Urticarial
Anaplryluls Bpinephrlne. 0.3 to 0.5 mL of
a 1:1000 dilution subcutaneously, repeated
in 15 to 20 min. Maintain airway. Intravenous access. RIUiiograpldc Contfalt Media.
Avoid use of contrast media known to have
caused prior reaction. If not possible, pretreat
patient with antihistamine and prednisone
(1 mglkg) 30 to 60 min before contrast media
exposure.
B
FIGURE 23·5 Drug-inducad angioaclema: pll'llclllln (A) Angioedema has led to closure of right eye.
(8) Sublingual angioedema in another patient interfered with breathing, talking, and eating and caused
great concern.
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
TABLE 23-5 Drugs Causing Urticaria/Angioedema/Anaphylaxis
Drug Type
Specific Drugs
Antibiotics
Penicillins: ampicillin, amoxicillin, dicloxacillin,
mezlocillin, penicillin G, penicillin V, ticarcillin.
Cephalosporins, third-generation sulfonamides
and derivatives
Cardiovascular drugs
Amiodarone, procainamide
lmmunotherapeutics, vaccines
Antilymphocyte serum, levamisole, horse serum,
monoclonal antibodies
Cytostatic agents
L-Asparaginase, bleomycin, cisplatin, daunorubicin,
5-fluorouracll, procarbazine, thiotepa
Angiotensin-converting enzyme Inhibitors
Captoprll, enalaprll,llslnoprll
Calcium-channel blockers
Nlfedlplne, dlltlazem, verapamll
Drugs releasing histamine
Morphine, meperidine, atropine, codeine,
papaverine, propanidid, alfaxalone, o-tubocurarine,
succinylcholine, amphetamine, tyramine,
hydralazine, tolazoline, trimethaphan camsylate,
pentamidine, propamidine, stilbamidine, quinine,
vancomycin, radiographic contrast media, and
others
FIXED DRUG ERUPTION ICD-10:T88.7
• A fixed drug eruption (FDE) is an adverse cutaneous reaction to an ingested drug, characterized by
the formation of a solitary (but at times multiple) erythematous patch or plaque. The most commonly implicated agents are listed in Table 23-6.
• If the patient is rechallenged with the offending drug, the FDE occurs repeatedly at the identical skin
site (i.e., fixed) within hours of ingestion.
• Skin symptoms: Usually asymptomatic. May be pruritic, painful, or burning.
• Skin Lesions. A sharply demarcated macule, round or oval in shape. Initially erythema, then dusky
red to violaceous (Fig. 23-6A). Most commonly, lesions are solitary and can spread to become quite
large, but they may be multiple (Fig. 23-7) with random distribution. Lesions may evolve to become
a bulla (Fig. 23-68) and then an erosion. Eroded lesions, especially on genitals or oral mucosa, are
quite painful. After healing, dark brown with violet hue postinflammatory hyperpigmentation. Genital skin (see Section 34) is frequently involved site, but any site may be involved; perioral or periorbital (Fig. 23-6A). They occur in conjunctivae or oropharynx.
• Dermatopathology. Similar to findings in erythema multiforme and/or TEN.
• Patch Test. An inflammatory response occurs in only 30% of cases.
• FDE resolves within a few weeks of withdrawing the drug. Recurs within hours after ingestion of a
single dose of the drug.
• Management. Withhold offending drug. Noneroded lesions: Potent topical glucocorticoid ointment. Eroded lesions: Antimicrobial ointment. For widespread, generalized, and highly painful
mucosal lesions, oral prednisone 1 mg/kg body weight tapered over a course of 2 weeks.
PART II DERMATOLOGY AND INTERNAL MEDICINE
FIGURE 23-6 Fixed dnag eruption (A) Tetracycline. Two well-defined periorbital plaques with edema.
This was the second such episode following ingestion of a tetracycline. No other lesions were present.
(8) Tylenol. A large oval violaceous lesion with blistering In the center. Erosive mouth lesions were also
present
TABLE 23-6 Most Commonly Implicated
Agents In Fixed Drug Eruptions
Tetracyclines {tetracycline, minccycline,
doxycycline}
SUifonamldes, other sulfa drugs
Metronidazole. nystatin, sallcyfates, NSAIDs,
phenylbutazone, phenacetin
Barbiturates
Oral conlJaceptlves
Quinine (lndudlng quinine In tonic water),
quinidine
Phenolphthalein
Food coloring (yellow}: in food or medications
FIGURE 23·7 Fixed drug eruption Doxycycline. Multiple lesions. Similar violaceous plaques
were also on the anterior and poster1or trunk.
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
DRUG HYPERSENSITIVITY SYNDROME ICD.O: 188.7
• Drug hypersensitivity syndrome is an idiosyncratic adverse drug reaction that begins acutely in the
first 2 months after initiation of the drug and is characterized by fever, malaise, and facial edema with
lymphadenopathy or an exfoliative dermatitis. Synonym: Drug rash with eosinophilia and systemic
symptoms (DRESS}.
• Etiology. Most commonly: Antiepileptic drugs (phenytoin, carbamazepine, or phenobarbital; crosssensitivity among the three drugs is common) and sulfonamides {antimicrobial agents, dapsone,
or sulfasalazine). Less commonly: Allopurinol, gold salts, sorbinil, minocycline, zalcitabine, calciumchannel blockers, ranitidine, thalidomide, or mexiletine.
• Some patients have a genetically determined inability to detoxify the toxic arene oxide metabolic
products of anticonvulsant agents. Slow N-acetylation of sulfonamide and increased susceptibility
of leukocytes to toxic hydroxylamine metabolites are associated with a higher risk of hypersensitivity
syndrome.
• Skin Lesions. Early: Morbilliform eruption (Fig. 23-8) on the face, upper trunk, and the upper
extremities; cannot be distinguished from an exanthematous drug eruption. May progress to
generalized exfoliative dermatitis/erythroderma, especially if the drug is not discontinued. Eruption
becomes infiltrated with edematous follicular accentuation. Facial edema (especially periorbitally) is
characteristic and may result in blister formation. Sterile pustules may occur. Eruption may become
purpuric on legs. Scaling and/or desquamation may occur with healing.
• Distribution. Symmetric. Almost always on the trunk and extremities. Lesions may become confluent and generalized.
• Mucous Membranes. Cheilitis, erosions, erythematous pharynx, and enlarged tonsils.
• General Examination. Involvement of the liver, kindeys, lymph nodes, heart, lungs, joints, muscles,
thyroid, and brain also occurs.
• Eosinophilia {30% of cases). Leukocytosis. Mononucleosis-like atypical lymphocytes. Histology
Skin. Lymphocytic infiltrate, dense and diffuse or superficial and perivascular.± Eosinophils or
dermal edema. In some cases, band like infiltrate of atypical lymphocytes with epidermotropism,
simulating cutaneousT cell lymphoma.
• Proposed Diagnostic Criteria. (1) Cutaneous drug eruption, (2) hematologic abnormalities (eosinophilia ~1 SOO/J.LL or atypical lymphocytes}, and {3) systemic involvement [adenopathies ~2 em in
diameter or hepatitis (SGOT ~2 N) or interstitial nephritis, or interstitial pneumonitis or carditis].
Diagnosis is confirmed if three criteria are present.
• Course and prognosis: Rash and hepatitis may persist for weeks after the drug is discontinued. In
patients treated with systemic glucocorticoids, rash and hepatitis may recur as glucocorticoids are
tapered. Lymphadenopathy usually resolves when the drug is withdrawn; however, rare progression to lymphoma has been reported. Patients may die from systemic hypersensitivity such as with
eosinophilic myocarditis (1 0%). Clinical findings recur if the drug is given again.
• Management. Identify and discontinue the offending drug. Systemic. Prednisone (0.5 mg/kg per
day) usually results in rapid improvement of symptoms and laboratory parameters.
• Prevention. The individual must be aware of his or her specific drug hypersensitivity and that other
drugs of the same class can cross-react. These drugs must never be readministered. Patient should
wear a medical alert bracelet.
PART II DERMATOLOGY AND INTERNAL MEDICINE
FIGURE 23-8 Drug hnM~rsenslllvtty SJlldrorne: phenytoin Symmetric, bright red, exanthematous
eruption, confluent in some sites; the patient had associated lymphadenopathy and fever.
DRUG-INDUCED PIGMENTATION ICD-1 0: T88.7
• Drug-induced pigmentation is common and results from the deposition of a variety of endogenous
and exogenous pigments in the skin.
• Drugs most commonly causing hyperpigmentation:
Antiarrhythmetic amiodarone.
Antimalarial: Chloroquine, hydroxychloroqulne, quinacrine, and quinine.
Antimicrobial: Minocycline, clofazimine, and zidovudine.
Antiseizure: Hydantoins.
Cytostatic: Bleomycin, cyclophosphamide, doxorubicin, daunorubicin, busulfan, 5-fluorouracil, and
dactinomycin.
• Metals: silver; gold, and Iron.
• Hormones: ACTH, estrogen or progesterone.
• Psychiatric: Chlorpromazine.
• Dietary: ~rotene.
SECTION 23 ADVERSE CUTANEOUS DRUG REAcnONS
CLINICAL MANIFESTATION
AMIODARONE More than 7596 ofpatients after
40-g cumulative dose after >4 months of
therapy. More common in skin phototypes I
and n. and may be limited to the light-exposed
areas in a small proportion (896) ofpatients.
Dusky-red erythema and later, blue-gray
dermal melanosis (Fig.13-9) in e:xposed area&
(the face and hands). Upofusc.ln-type pigment
deposited In macrophages and endothelial cells.
Cloroquine, hydroxychloroquine. Occurs in 2596 of individuals who
MTIMAWIIALS
take the drug for >4 months. Brownish,
FIGURE 2H Drug-Induced pigmentation: amlodarone A striking mix of a
slate gray and brown pigmentation in the face. The bluish color is caused by the
deposition of melanin and lipofuscin contained in macrophages and endothelial
cells in the dermis. The brown color is caused by melanin. The pigmentation is
reversible, but It may take up to a year or more to complete resolution.
PART II DERMATOLOGY AND INTERNAL MEDICINE
gray-brown, and/or blue-black discoloration
resulting from melanin or hemosiderin. Over
shins; the f.u:e and nape of neck; hard palate;
under finger- and toenails (see Section 32); may
also occ:ur in the comea and retina. Quinacrine:
Yellow, ycllow-green skin, and sclerae (resembling icterus}; yellow-green flu.orescen.ce of the
nail bed with Wood lamp.
MINOCYCLINE Onset delayed. usually after total
dose of >50 g, but may occur after a small
dose. Not melanin but an iron-containing
brown pigment. Blue-gray or slate-gray
pigmentation (Fig. 2.3-10). Distributed on
extensor legs. ankles, do.rsa of the feet. the
face, especially around eyes; sites of trauma or
Inflammation such as acne scars, contusions,
abrasions; hard palate, teeth; nails.
CLDFAZIMINE Orange, reddish brown (range,
pink to blaclc:) discoloration, ill-defined on
light-exposed areas; conjunctivae; accompanied
by red sweat. urine. feces. Subcutaneous fat is
orange.
ZIDOVUDINE Brown macules on lips or oral
mucosa; longitudinal brown bands in nails.
PHENYTOIN High dose ow:r a long period of
time(> l year). Discoloration is spctt:y, resembling melasma. in .llgbt-c:xposed areas and is
caused by melanin.
II:EOMYCIN Tan to brown to black and results
from an increase in epidermal melanin at
sites of minor inflammation, i.e., parallel
linear streab at sites of exoriations caused by
scratching (•flagellate" pjgmentation), most
commonly on the back. elbows, small joints.
and nails.
CYCLDPHOSPHAMID£ Brown. Dl1fuse or discrete
macules on elbows; palms with Addisonianlike pigmentation (see Fig. 15-tO and macule.s.
FIGURE 23·10 Drug-indua.cl pigmentation: minocyclln. Striking, blue-gray
pigmentation on the lower legs. This 75-year-old woman had been treated with
m!nocycllne for > 1 year because of nontuberculous mycobacterial Infection.
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
BUSULFAN Occurs in 5% of treated patients.
Addisonian-like pigmentation. Face, uillae,
chest, abdomen, and oral mucous membranes.
ACTH Addisonian pigmentation of skin and
oral mucosa. First 13 amino acids of ACTH
are identical to a.-melanocyte-stimulating
hormone (MSH) (see FiG- 15-11).
Caused by endogenous and exogenous estrogen combined with
progesterone. i.e., during pregnancy or with
oral contraceptive therapy. Sunlight causes
marked darkening of pigmentation. Tan/
ES1ROGENSI·PROGESTERONE
brown. Mcla8ma (sec Fig. 13-9).
SILVER (ARGYRIA OR ARGYROSIS) Source: Silver
nitrate nose drops; silver sul.mdie.zine applied
as an ointment. SUver sul1ide (photographic
Dim.). Blue-gray discoloration. Prlmarily areas
a:posed to light, Le., the face. dorsa of the
hands. nails, and conjunctiva; also diffuse.
IRON Source: IM iron injections; multiple blood
trlm!!fusions. Brown or blue-gray discoloration. Generalized; also local deposits at site of
injection.
CAROTENE Ingestion oflarge quantities of
~-carotene-containing vegetables; ~-carotene
tablets. Yellow-orange discoloration. Most
apparent on the palms and soles.
PSEUDOPORPHYRIA ICD-10: E80.25
• Pseudoporphyria is a condition that clinically presents with cutaneous manifestations of porphyria
cutanea tarda (PCr) (see Section 1O) without the characteristic abnormal porphyrin excretion.
• Drugs causing pseudoporphyria are naproxen, nabumetone, oxaprozin, diflunisal, celecoxib, tetracyclines, ketoprofen, mefenamic acid, tiaprofenic acid, nalidixic acid, amiodarone, and furosemide.
• Develops on the dorsa of hands and feet with characteristic tense bullae that rupture and leave
erosions (Fig. 23-11) and heal with scars and milia formation.
• It Is characterized by subepidermal blistering with little or no dermal Inflammation and, In contrast to
true PCT, little or no deposition of immunoreactants around upper dermal blood vessels and capillary walls.
• A bullous dermatosis that is morphologically and histologically indistinguishable from pseudoporphyrla also occurs In patients with chronic renal failure receiving maintenance hemodialysis (see
Section 18).
FIGURE D-11 PMudoporphyrfa: nonsWrolclll•ntl-fn&mmatory •s•rrts In this 2(}-year-old male,
blisters appeared on the dorsa of both hands that led to erosions, crusting, and were dinically indistinguishable from porphyria cutanea tarda. However, there was no urinary fluorescence, and porphyrin studIes were negative. The patient had taken an NSAID for arthritis and had Impaired kidney function.
PART II DERMATOLOGY AND INTERNAL MEDICINE
ACOR-RELATEO NECROSIS IC0-1 0: T88.7
• Drugs can cause cutaneous necrosis when given orally or at InJection sites.
• warfarin-Induced cutaneous neaos/s Is a rare reaction with onset between the third and fifth days of
anticoagulation therapy with the warfarin derivatives, manifested by cutaneous infarction.
• Risk factors: Higher initial dosing, obesity, female sex; individuals with hereditary deficiency of protein
C, protein S, or antithrombin Ill deficiency.
• Lesions vary with severity of reaction: Petechiae to ecchymoses to tender hemorrhagic Infarcts to
extensive necrosis, which can be well demarcated, deep purple to black (Fig. 22-1 2). Distribution:
Areas of abundant subcutaneous fat breasts (Fig. 23-1 2), buttocks, abdomen, thighs, and calves;
acral areas are spared.
• Differential diagnosis: Purpura fulminans (disseminated intravascular coagulation), hematoma/
ecchymosis/necrotizing soft tissue Infection, vasculitis, or brown recluse spider bite.
• Heparin can cause cutaneous necrosis, usually at the site of the subcutaneous injection (Rg. 23-13}.
• Jnterferon-o. can cause necrosis and ulceration at injection sites, often in the lower abdominal panniculus or thighs (Fig.l3-14).
• Ergotamine-containing medications lead to acral gangrene; ergotamine-containing suppositories
after prolonged use cause extremely painful anal and perianal black eschars which, after having
been shed, leave deep painful ulcers (Fig. 23-1 5).
• Embolia cutis medicomentoso: Deep necrosis developing at the site of intramuscular injection of oily
drugs inadvertently injected into an artery (rtg. 23-16}.
• Necrosis also develops in obtunded or deeply sedated patients at pressure sites (Fig.l3-17).
FIGURE 23-12 ACDR-related cutaneous nec:rosls:warfarrn Bilateral areas of cutaneous Infarction
with purple-to-black coloration of the breast surrounded by an area of el)'thema occurred on the fifth
day of warfarin therapy.
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
FIGURE 23-13 ACDR·rellrted c:utaneoYJ neaosls: heJH&rfn Two lesions of irreg·
ular dark·red erythema with central hemorrhagic necrosis on the abdomen occurring
postoperatively in a female injected with heparin.
FIGURE 23·14 ACDR·NIIrted cutaneous niKI'OSis: irrterferon-o. An ulcer on
the thigh at the site of Interferon InJection.
PART II DERMATOLOGY AND INTERNAL MEDICINE
FIGURE 23·15 ACDR-relatecl cutanaous nacrosls: ergotamine This ~ear-old male had used
ergot<ontaining suppositories for pain relief over many months. Painful black necrosis followed by ulceration developed on the anus and perlanally and extended Into the rectum.
FIGURE 23-16 ACDR-relatecl neaoJIJ following Intramuscular lnjacllon Embolia cutis medicamentosa. The drug (an oily preparation of testosterone) had been Inadvertently administered Intraarterially.
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
FIGURE 23-17 ACDR·related neaosls wtth hemorrhagic blistering after an overdose ofbarbl·
tt.lrates This patient had attempted suicide.
ACDR-RELATEDTOCHEMOTHERAPY IC0-10:T88.7
• Chemotherapy may Induce local and systemic skin toxicity with a wide range of cutaneous manifestations from benign to life threatening.
• The ACDR can be related to overdose, pharmacologic side effects, cumulative toxicity, delayed toxicity, or drug-drug interactions.
• Clinical manifestations range from alopecia (see Section 31) and nail changes (see Section 32}
to mucositis and acral erythema, often with sensory abnormalities: Palmoplantar dysesthesia
(capecitabine, cytarabine, doxorubicin, fluorouracil).
• Chemotherapeutic agents are also responsible for inflammation and ulceration at sites of extravasation of intravenous medications, such as doxorubidn or taxol, which can be followed by skin necrosis
with ulceration.
• Other reactions are radiation recall or enhancement (as with methotrexate), eros!on or ulceration of
psoriasis caused by an overdose of methotrexate, inflammation and sloughing of actinic keratcr
sis resulting from 5-fluorouracil or fludarabine, or erosions caused by cisplatin plus 5-fluorourocil
(Fig. 23-18A}.
• Table 23-7 1ists newer chemotherapeutics induding •biologicals" and their ACDR
PART II DERMATOLOGY AND INTERNAL MEDICINE
FIGURE 23·18 ACDR-related cellultt1s Erosions resulting from cisplatin
and 5-fluorouraci/ (SFU). This patient
had received chemotherapy with dsplatin and 5FU. Painful erosive lesions
appeared on the scrotum and there was
also erosive mucositis.
TABLE 23·7 Newer Chemotherapeutic Agents and Their ACDR
Cllu
Agarrts
Spindle inhibitor
Taxanes: docetaxel,
paclltaxel
Anti metabolites
ACDR'
Hand-root skin reaction"; combined with sensory
abnormalities: erythrodysesltlesla; radiation
recall urticaria,. exanthems, mucositis.. alopecia,
nail changes (see Secdon 32); sderodermalike changes on lower extremities; subacute
cutaneous lupus ef)'thematosus (SCI..£), AGEP
and fixed drug reaction {paclltaxef)
VInca alkaloids: vincristine, Phlebitis. alopecia,. acral erythema, extravasation
vinblastine, vlnorelb!ne
reactions (Including necrosis)
F1udarabine
Serpentine supravenous hyperpigmetnatlon,
macular, papular exanthem, mucositis,. acral
erythema, para neoplastic pemphigus, drugInduced SCLE
Oadrlbine
Exanltlem,TEN(?)
Capecitabine
Hand-root skin reaction" acral hyperpigmentation,
palmoplantar keratoderma, pyogenic
granuloma, Inflammation ofactinic keratoses
SECTION 23 ADVERSE CUTANEOUS DRUG REACTIONS
TABLE 23-7 Newer Chemotherapeutic Agents and Their ACDR (Continued)
Class
Agents
ACD~
Tegafur
Hand-foot skin reactionb acral hyperpigmentation;
pityriasis lichenoides et varioliformis acuta,
phototoxlc reactions
Mucositis, alopecia, maculopapular exanthem,
radiation recall, linear lgA bullous dermatosis,
pseudoscleroderma, lipodermatosclerosis,
erysipelas-like plaques, pseudolymphoma,
lymphomatoid papulosis
Exanthema, radiation recall, urticarial vasculitis
Gemcitabine
Pemetrexed
Genotoxic agents
Carboplatin
Oxallplatln
Llposomal doxorublcln
Liposomal daunorubicin
ldarubicin
Topotecan
lrinotecan
Alopecia, hypersensitivity reaction (erythema,
facial swelling, dyspnea, tachycardia, wheezing),
palmoplantar erythema, facial flushing
Hypersensitivity reaction (see preceding); Irritant
extravasation reaction; radiation recall
Acral erythema, palmoplantar erythrodysesthesla
neutrophilic eccrine hidradenitis,
hyperpigmentation (blue-gray), mucositis,
alopecia, exanthems, radiation recall, ultraviolet
light recall
Alopecia, mucositis, extravasation reactions
Radiation recall; alopecia, acral erythema,
mucositis, nail changes (transverse pigmented
bands), extravasation reactions
Maculopapular exanthem, alopecia, neutrophi lie
hidradenitis
Mucositis, alopecia, lichenoid reactions
Papulopustular eruptions in seborrheic areas,
Signal transduction EGFR antagonists:
inhibitors
gefitinib, cetuximab,
erythematous plaques, telangiectasias; xerosis,
paronychia; hair abnormalities (trlchomegaly,
erlotlnlb, panltumumab
curling, fragility, see Section 31)
Usually start a week after initiation of drug. Can
treat with topical antibiotics, retinoids (topical
or systemic). Can also lead to paronychia,
trlchomega ly, leu kocytocalstlc vasculitis,
urticaria, anaphylaxis and necrolytic migratory
erythema.
Multikinase inhibitors:
lmatinib
Maculopapular exanthem (face, forearms,
ankles), exfoliative dermatitis, graft-versus-host
reaction-like reaction, erythema nodosum,
vasculitis, SJS, AGEP; hypoplgmentatlon,
hyperpigmentation, darkening of hair, nail
hyperpigmentation, lichen planus-like eruption
(skin and oral mucosa), follicular mucinosis,
pityriasis rosea-like eruption, Sweet syndrome,
exacerbation of psoriasis, palmoplantar
hyperkeratosis, porphyria cutanea tarda,
primary cutaneous EBV-related B cell lymphoma
(continued)
PART II DERMATOLOGY AND INTERNAL MEDICINE
TABLE 23-7 Newer Chemotherapeutic Agents and Their ACDR (Continued)
Class
Agents
ACD~
Dasatlnlband nllotlnlb
Localized and generalized erythema,
maculopapular exanthem, mucositis, pruritus,
exfoliation, alopecia, xerosis •acne: urticaria,
panniculitis, Sweet' syndrome.
Rash/desquamation, hand-foot skin reactionb pain,
alopecia, mucositis, xerosis, flushing edema,
seborrheic dermatitis, yellow skin coloration
(sunitinib, one week after starting drug),
subungual splinter hemorrhages, pyoderma
gangrenosum, sec (KA-type) and eruptive
melanocytlc lesions (sorafenlb)
Sorafenib and sunitinib
Proteasome
inhibitor
Bortezomib
Immune
Modulators
lpilimumab (CTLA-4 AB)
Pembrolizumab and
Nivoluman (PD-1
receptor antibody)
BRAF inhibitors
Vemurafinib
Dabrafenib
Erythematous nodules and plaques, morbllllfurm
exanthem, ulceration, vasculitis and Sweet'
syndrome
Immune-mediated side effects: macular and
papular eruption, pruritis, hepatitis, vitiligo,
hypothyroidism, enterocolitis, hepatitis, SJS/TEN
Immune-mediated side effects: macular
and papular eruption, pruritus, vitiligo,
hypothyroidism, enterocolitis, hepatitis,
mucositis
Rash (68%), arthralglas, photosensitivity (42%),
sec (23%, most occur in first few months)
Pyrexia, headaches, rash
"'n ly cutaneous adverse reactions are listed here.
bHand-foot skin reaction: erythema, hyperkeratotic with halo of erythema, tender, localized to areas of
pressure on fingertips, toes, and heels.
Source: Collated from N Haidary et al. JAm Acad Dermatol. 2008;58:545. Please note that this table has
also been supplemented by the authors.
BACTERIAL COLONIZATIONS AND
INFECTIONS OF SKIN AND
SOFT TISSUES
The human miaobiome or microbiota represents diverse viral, bacterial, fungal, and other
species that live on and within us. They are part
of us and we are part of thJs complex ecosystem. ':Ute hwuan body contains > 10 times
more microbial cells than human cells. Skin
supports a range of microbial communities that
live in distinct niches. Microbial colonization
of skin is more dense in humid intertriginous
and occluded sites such as axillae. anogenital
regions, and webspaces offeet. An lntart stratum corneum is the most important defense
against invasion of pathogenic bacteria.
Coagulase-negative staphylococci normally
colonize skin shortly after birth and are not considered to be pathogens when cultured from. skin.
Overgrowth offlora in occluded areas often
results in clinical syndromes oferythrrwna,
pitted kn'atolysis, and trichomycosis.
Pyoderma is an ar<:haic term, literally "pus
in the skin:" Skin and soft-tissue infections,
commonly caused by Staphylococcus aunus
and group A streptococcus (GAS), have
been .referred to as "pyodenua:" Pyodenua
gangrenosum is a noninfectious inflammatory
process, often associated with a systemic disorder such as inflammatory bowel disease.
S. aureus colonizes the nares and intertriginous skin intermittently. can penetrate the stratum corn.eum, and cause skin infections, e.g.,
impetigo, folliculitis. Deeper infection results
in soft-tissue infections. Methicillin-resistant
S. aureus (.MRSA) is an important pathogen for
community-acquJred (CA-MRSA) and healthcare-acquired (HA-MRSA) infediOilS. .MRSA
strain USA300 is the major cause of skin and
soft tissue as well as more invasive infections in
community and health-care settings.
GAS usually colonizes the skin tim and
th.en the nasoph.arynx. Group B streptococcus
(GBS; Streptococcus agaJaalae) and group G
(3-hemolytic streptococci. (GGS) colonize the
perineum ofsome individuals and may cause
superficial and invasive infections.
Cutaneous production of toxins by bacte:ria
(S. aureus and GAS) causes systemic intolicat!.ons such as toxic shock syndrome (TSS) and
scarlet fever.
ERYTHRASMA ICD-10: L08.1
• Etiology. Cotynebocterium minutissimum, gram-positive (diphtheroid) bacillus; normally in human
mlcroblome. Growth favored by humid cutaneous microclimate.
CLINICAL MANIFESTAnON
Asymptomatic except for subtle dlscolo:ratfo:n.
Patches, sharply marginated (Fig. 25-1 ). Tan
or pinkish; postinflammatory hyperpigmentation in more heavily pigmented individuals.
522
In webspaces of the feet. it may be macerated
(Fig. 25-2). Dtstrllndion: Intertriginous skin.
i.e.. toe webs (Fig. 25-2), inguinal folds, axillae.
and other occluded sites.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-1 Er,thre1ma: groin• Sharply marginated, tan patches in the genit<r
crural fold. Wood lamps demonstrates bright coral-red fluorescence differentiating
erythrasma from Intertriginous psoriasis. KOH preparation was negative for hyphae.
DIAGNOSIS
Wood's lamp examination demonstrates
corral-red fluorescence. KOH negative; rules
out epidermal dermatophytosis.
DIFFERENTIAL DIAGNOSIS
Intertriginous psoriasis. epidermal dermatophytosis, pityriasis Vt:l'Sicolor, and HaileyHailey disease.
COURSE
FIGURE 25·2 Er,thrasma: w81:11pace This
macerated interdigital webspace appeared bright
coral-red when examined with Wood's lamp; KOH
preparation was negative for hyphae. The we~
space is the most common site for erythrasma
in temperate climates. In some cases, interdigital
tfnea pedis and/or pseudomonallntertrfgo may
coexist.
Persl.sts and reaus unless microclimate Is
altered.
TREATMENT
Usually controlled with benzoyl peroxide wash
or sa.nitlzing alcohol geL Clindamycinlotion
and erythrom~iD. ue beneficiaL
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
PITIED KERATOLYSIS
• Etiology. Kytococcus sedentorlus. One of human mlcroblome on plantar feet In the setting of hyperhidrosis; produces two extracellular proteases that can digest keratin.
CLINICAL MANIFESTAnON
Punched out pita in at:ratum comeum, 1 to
8 mm in diameter (Fli- 25-3). P.lts can remain
discrete or become con11uent. forming large
both feet. Distribution: Pressure-bearing areas,
ventral aspect of toe. ball offoot, heel; interface
of toes.
DIAGNOSIS
areas of eroded stratum comeum. Lesions are
more apparent with hyperhidrosis and macera-
Clinical diagnosis. KOH to rule out tinea
tion. Symmetric or asymmetric involvement of
pedis.
FIGURE 25-3 Plttad lalntolysb: plantar The stratum corneum of the plantar skin shows confluent
multiple, confluent 'pits' (defects In the stratum corneum).
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
DIFFERENTIAL DIAGNOSIS
TREATMENT
ConcomitaDt tinea pedis. erythrasma. candida!
intertrigo, and pseudomonal webspace infec-
Usually controlled with benzoyl peroldde wash
or llallitizing alcohol gel. Topical antibiotIcs. such as erythromycin and clindam:ycln.
and aluminum chloride solution can also be
tion may be present
COURSE
helpful.
Persists and .teCUIS unless ml.croclimate Is altered.
TRICHOMYCOSIS ICD-1 0: A48.8/LOB.B
• Superficial colonization on hair shafts in sweaty regions, axillary and pubic.
• Etiology. Corynebacw/um tenuls and other corynebacterial spedes; gram-positive diphtheroid. Not
fungus.
• Malodorous granular concretions (yellow, black, or red) on hair shaft (Fig. 25-4). Hair appears thickened, beaded, and firmly adherent.
• Treatment. Usually controlled with benzoyl peroxide wash or sanitizing alcohol gel. Antiperspirants.
Shaving area.
FIGURE 25-4 TrkhomJCOifs ulllarfs
40-year-old obese male. Axillary hairs
have cream-color encrustation. Some
skin tags are also seen.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
INTERTRIGO ICD-10: L30A
• Intertrigo (latin /nrer, •between•; rrlgo, •rubbing").
• Inflammation of opposed skin Onframammary regions, axillae, groins, gluteal folds, and redundant
skin folds of obese persons). May represent inflammatory dermatosis or superficial colonization or
infection.
• Dermatoses occurring in intertr1ginous skin include intertriginous psor1asis, seborrheic dermatitis,
Halley-Halley disease, and Langerhans cell histiocytosis. S. aureus and streptococcus can cause
secondary Infection of these dermatoses.
INFECTIOUS INTERTRIGO
CLINICAL MANIFESTATION
BACTERIAL
Usually asymptomatic. Discomfort usually
indicates lDfectton rather than colonizatl.on.
Soft-tissue .Infection can gain entry inS. aureus
or streptococcal intertrigo.
• Beta-hemolytic st.reptococcL Group
A (Fig. 2S-5), group B, and group G
(Fig. 2S-6). Streptococcal intertrigo can
progress to soft-ti~&ue infection (Fig. 25-6).
• S. aumu. Ofu:.n galn8 entry into the skin
via hair follicles. causing folliculitls and
furuncles.
• Pser.uWmonas aeruginosa (Fig. 25-7).
• C. minutissimum (erythrasma) (Pigs. 25-1
and 25-2).
• K. sedentarius (pitted keratolysis) (Fig. 2S-3).
DIAGNOSIS
Identify pathogen by bacterial culture, Wood's
lamp examination. or KOH preparation.
TREATMENT
Identify and treat pathogen.
FIGURE 25-5 lntargluteal irrtertrigo:
group A streptococcus A painful moist
erythematous plaque In a male with Intertriginous psoriasis, with foul odor. Infection
resolved with penicillin VK.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-6 Erysipelas: group G streptoc:oc:c:us 65-year-old male with
sharply marginated erythematous plaque on buttocks. Portal of entry of infection was intergluteal intertrigo.
FIGURE 25-7 Webspecelnt....go: P. Cl«:f"U-
glnosc Erosion of a webspace of the foot with a
bright red base and surrounding erythema. Tinea
pedis Onterdlgltal and moccasin patterns) and
hyperhidrosis were also present which facilitated
growth of Pseudomonas.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
IMPETIGO ICD-10: B08.0
• Etiology. 5. aureus; GAS.
• Portal of Entry. Impetigo occurs adjacent to the site of S. aureus colonization such as the nares.
Secondary infection of (1) minor breaks in the epidermis (impetiginization), (2) preexisting
dermatoses, (3) other infections such as eczema herpeticum, or (4) wounds.
• Clinical Manifestation. Honey-colored crusted erosions.
• Treatment
• Reduced colonization.
• Topical antibiotic to infected and colonized sites; systemic antibiotic.
EPIDEMIOLOGY AND ETIOLOGY
• S. aureus: Methicillin-sensitive (MSSA)
and methicillin-resistant (MRSA). Bullous
impetigo: Local production of epidermolytic
toxin A-producing S. aureus, which
also causes staphylococcal scalded skin
syndrome.
• Beta-hemolytic streptococcus: group A.
S. aureus and GAS are not members of human
skin microbiome. They may transiently colonize
skin and cause superficial infections.
DEMOGRAPHY Secondary infections, any age.
Primary infections most often occur in children.
PORTALS OF ENTRY OF INFECTION Minor breaks
in the skin most commonly. Facial lesions
usually associated with S. aureus colonization
of nares. Dermatoses such as atopic dermatitis
or Hailey-Hailey disease. 'fraumatic wounds.
Bacterial infections occur in other cutaneous
infections.
CLINICAL MANIFESTATION
Superficial infections often asymptomatic.
Ecthyma may be painful and tender.
IMPETIGO Erosions with crusts (Figs. 25-8 and
25-9). Golden-yellow crusts are often seen in
impetigo but are hardly pathognomonic; 1- to
>3-cm lesions; central healing often apparent
if lesions present for several weeks (Fig. 25-9).
Arrangement: Scattered, discrete lesions;
without therapy, lesions may become confluent; satellite lesions occur by autoinoculation.
Secondary infection of various dermatoses is
common (Figs. 25-10 and 25-11).
BULLOUS IMPETIGO Superficial blisters containing clear yellow or slightly turbid fluid
with erythematous halo, arising on normalappearing skin. Bullous lesions rupture easily,
revealing shallow moist erosions (Figs. 25-12
and 25-13). Distribution: More common in
intertriginous sites.
ECTHYMA Ulceration with a thick adherent
crust (Fig. 25-14). Lesions may be tender,
indurated Usually occurs at occluded sites
(common in homeless or soldiers in trenches
during combat who do not or cannot change
boots).
DIFFERENTIAL DIAGNOSIS
Excoriation, contact dermatitis,
herpes simplex, epidermal dermatophytosis,
and scabies.
INTACT BULLAE Acute contact dermatitis, insect
bites, thermal burns, and porphyria cutanea
tarda (PCT) {dorsa of hands).
ECTHYMA Excoriations, insect bites.
IMPETIGO
DIAGNOSIS
Clinical findings confirmed by culture: S.
aureus, commonly; failure of oral antibiotic
suggests MRSA. GAS.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-8 Impetigo: MSSA Crusted eryttlematous erosions becoming confluent on the nose,
cheek. lips, and chin in a child with nasal carriage of S. aureus.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-9 lmpttlgo: MSSA Crusted, erythematous erosions becoming confluent in the antecubital fossa, uppef' and lower arm in a child with atopic dermatitis.
COURSE
Untrea.ted.le.sions of impetigo become more
ex:te:nsi.ve and develop into ecthyma. With
adequate treatment, prompt resolution. Lellions
can progress to deeper skiD. and soft-tissue
infections. Nonsuppurative complications of
GAS infection include guttate psoriasis, scarlet
fever. and glomerulonephritis. Ecthyma may
heal with scarring. ReCUITe:nt S. aum.IS or GAS
Infections can occur beau8e of the failure to
eradicate pathogen or by recolonization. Undiagnosed MRSA lnfedion does not respond
to usual oral antibiotics given for methicillinsensitiveS. aureus.
TREATMENT
PRlVENTION Benzoyl peroxide wash. Check
famlly members for signs of impetigo. Ethanol
FIGURE 25-10 Sec:ond•ry lnhctlon ofH•IIey-H•IIey dl..ua: MRSA 51-year-old female
with Hailey-Hailey disease has chronic MRSA
Infection of cutaneous erosions on thigh.
or Isopropyl gel for hands and/or in:volved
sites.
TOPICAl TREATMENT Mupirocin and retapamulin oin1ment is highly effective in eliminating
S. aln'l!us from the nares and cutaneous lesiollll.
SYSTEMIC AN11MICROIIIAL TREATMENT
to se.nsltivityof!solated organism.
According
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-11 Secondary lnfectlon of mild atopic dermatltfs: MRSA 11-yearold boy has yellowish crusted lesions on left cheek and chin.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-1:1 Bullous impatlgo Scattered, discrete, intact, and ruptured thin-walled
blisters on the inguinal area and adjacent thigh of a child; lesions in the groin have ruptured, resulting In superficial erosions.
FIGURE 25-13 Bullous lmpatfgo with blistering cladJIItb: $, GCUWUS A large, single
bulla with surrounding erythema and edema on the thumb of a child; the bulla has ruptured and clear serum exudes.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
EcthJm•: MSSA Thickly crusted ulcer on the leg that had been present on the lower
leg of a homeless who had not taken off his boots for weeks. The crust was adherent and the site bled
wlth debridement
FIGURE 25-14
ABSCESS, FOLLICULITIS, FURUNCLE, AND CARBUNCLE ICD-1 0: L02
• Deeper skin infections can follow traumatic inoculation into skin or the extension of infection into
hair follicles.
• Abscess: Acute or chronic localized inflammation. associated with a collection of pus accumulated in
a tissue. Inflammatory response to an infectious process or foreign material.
• Folliculiris: Infection of hair follicle with ± pus in the ostium of follicle.
• Furunde: Acute, deep-seated, red, hot, tender nodule or abscess {boil) that evolves from a staphylococcal folliculitis.
• Carbunde: Deeper infection composed of interconnecting abscesses usually arising in several
contiguous hair follicles.
EPIDEMIOLOGY AND ETIOLOGY
CLINICAL MANIFESTATION
S. aureus (MSSA. MRSA).
osass May arise in any organ or tissue.
Abscesses that present on the skin arise in the
dermis, subcutaneous fat, muscle. or a variety
Other O.rganlsm8. Less common.
Sterile abscess can oo:ur as a foreign-body
response (splinter, ruptured inclusion cyst.
injection site&). Cutaneous odontogenic slnu8
can appear anywhere on the lower face, even
at sites distant from the origin (see Cutaneous
Odontogenic (Dental) Abscess. Section 33).
Folliculitis. furuncles. and carbuncles
represent a continuum ofseverity ofS. aureus
infccticm. Portal of entry: Ostium of hair
follicle.
of deeper structure&. Initially. a tender red
nodule forms. In time (days to weeks), pus
collcctll within a central space (Fig.15-15). A
well-fo.nued abscess Js characterized by fluctuance of the central portion of the lesion. Arise
at sites of trauma. Ruptured inclusion cyst
on the back often presents as painful absce65.
When~ from S. aumu folliculitis, it may
be soUtary or multiple.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-15 Abscau: MSSA A very tender abscess with surrounding erythema on the heel. The
patient was a diabetic patient with sensory neuropathy; puncture by a sewing needle that was imbedded
In the heel had provided a portal of entry. The foreign body was removed surgically.
FOUICUUTIS Begins In the upper portion of
the hair follicle. Can arise from bacteria, fungi.
virus and mites. Follicular papule, pustule,
erosion or crust at the follicular infundibulum,
and can extend deeper into the entire length
of the follicle (sycosis). Usually nontender or
slightly tender; may be pruritl.c. (Flg. 25-16).
Predisposing factors include shav.lng hairy
regions, occlusion ofhair-bearJ.ng areas, topical
corticosteroid preparations, systemic antibiotic
promotes growth of gram-negative bacteria,
diabetes mellitus, and immunosuppression.
Elrte.n!l.on of.Infection can progress to abscess
or furuncle formation.
Bacterial agent&: S. aweus (Bockhart impetigo);
Pseudomonas aerugtnosa (hot-tub); gramnegative folll.cull:tis.
Viral: Herpetic, molluscum contagiosum (see
Section 27).
Fungal: Candida, Malassu:ia, de.rmatophyte&
(see Section 26).
Other: Syphilitic (see Section 30), Demcdex
(see Section 28).
Varllnts
S. auretU Folliculitis can be either superficial
folliculitis (infundibular) (Pig. 25-16} or deep
(sycosis) (exteosion beneath infundibulum)
(Fig. 25-17) with abscess formation.ln severe
cases (lupoid sycosis), the pilosebaOO>us units
may be destroyed and replaced by fibrous scar
tissue.
GRAM-NEGA11VE FOUICULins Occurs In individuals with acne vulgaris treated with oral antibiotics. •Acne.. typically worsens, having been in
good controL Chamcterized by small fullicular
pustules and/or larger abscesses on the check&.
(Pseudomonas Auuginosa). Occurs on the trunk following immer-
HOT'·TUB FOWCULrTIS
sion in spa water (Flg. 25-18).
MANAGEMENT
FURUNCLE Initially, a firm tender nodule, up
to 1 to 2 em In diameter. In many individuals,
furuncles occur in the setting of staphylococ-
cal folliculitis. Nodule becomes fluctuant.
with abscess formation ± central pustule.
Nodule with cavitation remains after drainage
of abscess. A variable zone of cellulitis may
surround the furuncle. Distrilnmon: Any hairbearing region-Beard area, posterior neck
and occipital scalp, axillae. buttocks. Solitary or
multiple lesions (Fip. 25-19 to 25-23).
CARBUNCLE Evolution is s!mllar to that of
furuncle. Composed of several to multiple,
adjacent. and coalescing furuncles (Fig. 25-24).
Characterized by multiple loculated dermal
and subcutaneous abscesses, superficial pu&tules, necrotic plugs, and sieve-like openings
draining pus.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-16 lnfectrous folliculitis,
superftdllln axilla: MRSA A 25-year-old
male with pruritic and tender axillary lesions
for several weeks. Multiple follicular pustules and papules are seen in the vault of
the shaved axilla. Sha\llng facilitates entry of
5. aureus into the superficial hair follicle. The
lesions resolved witt. minocycline.
FIGURE 25-17 Infectious folliculitis A male patient with HIV/AIDS and persistent pruritic pustular and
ruptured lesions on the cheek/beard for several months.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-18 lnhctlous folliculitis ("'hot tub"): P. dfi'Ugi:rtOIII A
31-year-old male with multiple painful follicular pustules 3 days after
bathing In a hot tub. P. aeruglnosa was Isolated on culture from a
lesion.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-19 Furunde:
MSSA Abscess on the
upper lip of a 35-year-old
male. The lesion is crusted
on the top and solid and
extremely painful. The
furuncle was incised and
drained and treated with
antibiotics.
FIGURE25-20 Fur.~ndes
and cellulitis: MRSA A
64-year-old male developed furuncles on the
dorsum of the left hand
(A) and forearm (1). Infection was spreading from
the abscess with cellulitis.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-21 Multipl• furundac on tll•lowar chett: MRSA 60-year-old diabetic nurse with multfple painful nodules. MRSA was Isolated on culture of the nares and from an abscess. She was treated
wlth cllndamycln and muplrocln to nares. She was restricted from returning to work until culture sites
were negative for S. aureus colonization.
FIGURE 25-22 Multipl•
furundes: MRSA Multiple painful nodules on
ttle buttocks of a 52-yearold female wittl diabetes.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-D Chronic abKess, bot·
ryornycosfs:MRSA 41-yearold with HIV
disease had an extensive abscess for months.
(A) R-buttock abscess. (B) The abscess was
drained and treated with llnezolld. (C) The
white grains noted In the drainage represent
colonies of S. aureus.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25·24 Carbuncle: MSSA
A very large, inflammatory plaque studded with pustules and draining pus on
the nape of the neck. Infection extends
down to the fascia and has formed from
a confluence of many furuncles.
DIFFERENTIAL DIAGNOSIS
TREATMENT
FOUICUUTIS Acneiform disorders (acne
vulguis, rosacea. or perioral dermatitis), HIVassoctated eosinophlli' follic:ulitl.s. chemical
irritants (cliloracne), acneiform adw:rse artaneous drug reactions [epidermal growth factor
receptor iDhibitom (e.g.• erlotiDib), halogens.
Correct underlyingpredisposing
condition. Washing with antibacterial soap or
benzoyl pero.lide preparation or isopropyl/
ethanol geL
ANTIMICROBIAL THERAPY Bacterial Follfadltis.
Most will respond to natural penicillins but
can coDSider dicloxadlli.n. amoxi.cillin. primary
(:Cphalosporlns and clindamydn, usually for
7 to 10 days. Consider culture for resistant
organisms. Minoqclin.e, trimethoprim-sulfamethoxazole and quinolones may be necessary.
There may be higher resistance to the erythromycin family.
Gram-Negative Follfc:ulltie. Associated with
systemic antibiotic therapy of acne vulgaris.
Discontinue current antibiotics. Wash with
benzoyl peroxide. In some cases. ampicillin
(250 mg fuur times daily) or trimeth.oprim.sulfamethOiaZOle four times daily.lsotretl-
glucocorticolds,llth.lum.], keloidal folliculitis,
and pseudofolliculitJs barbae.
PAINFUL DERMAUSUBCUTANEOUS NODULE
Ruptured epidermoid or pilar cyst, hidradenitis
suppurativa.
DIAGNOSIS
Clinical fin~ confu:med by findings on
Gram stainlng and cul.tun:.
COURSE
Most cases offolliculitis and abscesses resolve
with efi'ectlw treatment. If diagnosis and treatment are delayed, furunculosis c:an be (:Om-
plicated by soft-tissue infection, bacteremia.
and hematogenous seeding of viscera. Some
individuals an: subject to recw::rent furwu:ulosls, particularly diabetics.
PROPHYLAXIS
noln.
'Ihe treatment of an absceee, !urunde. or
aubund.e is incision and drainage. with oonsideration of systemic antimicrobial therapy in
immunocompromised patients or when there
an: signs ofsystemic Infection.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
SOFT-TISSUE INFECTION
• Characterized by inflammation of skin and adjacent subcutaneous tissues. Soft tissue refers to tissues
that connect, support, or surround other structures and organs: skin, adipose tissue, fibrous tissues,
fascia, tendon, ligaments.
• Syndromes. Cellulitis, erysipelas, lymphangitis, necrotizing fasciitis, or wound infection.
• Soft-tissue inflammation. Although often infectious, soft-tissue inflammation can be a manifestation
of a noninfectious reaction pattern such as with neutrophilic dermatoses, erythema nodosum, and
eosinophilic cellulitis.
• Cellulitis. Usually begins at a portal of entry in the skin, spreading proximally as an expanding solitary
lesion. Uncommonly, soft-tissue infection can follow hematogenous dissemination with multiple
sites of infection. Cellulitis is most often acute, caused by S. aureus.
• Acute Inflammation. Resulting from cytokines and bacterial superantigens rather than to overwhelming tissue infection.
• Chronic Soft-llssue Infection. Nocardiosis, sporotrichosis, and phaeohyphomycosis.
CELLULITIS ICD-10: A46.0
• Acute, spreading infection of dermal and subcutaneous tissues. Characterized by a red, hot, and
tender area of skin. Portal of entry of infection is usually apparent. Most common pathogen is
S. aureus. Erysipelas is a variant of cellulitis involving cutaneous lymphatics, and is usually caused
by beta-hemolytic streptococci.
EPIDEMIOLOGY AND ETIOLOGY
Adults: S. aureus, GAS.
Less commonly beta-homolytic streptococcus: Group B, C, or G. Erysipelothrix rhusiopathiae (erysipeloid); P. aeruginosa, Pasteurella
ETIOLOGY
multocida, Vibrio vulnificus; Mycobacterium
fortuitum complex. In children: Pneumococci,
Neisseria meningitidis group B (periorbital).
Haemophilus influenzae type b (Hib) infections much less common because of Hib
immunization.
Chronic Soft-Twue Infections. Nocardia
brasiliensis, Sporothrix schenckii, Madurella species, Scedosporium species, and nontuberculous
mycobacteria (NTM).
Dog and Cat Saliva and Bites: P. multocida
and other Pasteurella species. Capnocytophaga
canimorsus (see Septic shock: ischemic necrosis
of acral sites, p. 566).
PORTAL OF INFECTION Pathogens gain entry via
any break in the skin or mucosa. Tinea pedis
and leg and foot ulcers are common portals.
Infections follow bacteremia/sepsis with cutaneous seeding.
RISK FACTORS Host defense defects, diabetes
mellitus, drug and alcohol abuse, cancer and
cancer chemotherapy; chronic lymphedema
[postmastectomy, previous episode of cellulitis/
erysipelas].
After entry, infection spreads to tissue spaces
and cleavage planes {Fig. 25-25) as hyaluronidases break down polysaccharide ground
substances, fibrinolysins digest fibrin barriers,
and lecithinases destroy cell membranes. Local
tissue devitalization is usually required to allow
for significant anaerobic bacterial infection.
The number of infecting organisms is usually
small, suggesting that cellulitis may be more of
a reaction to cytokines and bacterial superantigens than to overwhelming tissue infection.
CLINICAL MANIFESTATION
Symptoms of fever and chills can develop
before cellulitis is clinically apparent. Higher
fever (38.5"C) and chills usually associated
with GAS infection. Local pain and tenderness.
Necrotizing infections associated with severe
pain and systemic symptoms.
Red, hot, edematous, and shiny plaque
originating at the portal of entry. Enlarges with
proximal extension (Figs. 25-26 and 25-27);
borders usually sharply defined, irregular, and
slightly elevated. Vesicles, bullae, erosions,
abscesses, hemorrhage, and necrosis may form
in plaque (Fig. 25-27). Lymphangitis. Lymph
nodes can be enlarged and tender regionally.
DISTRIBUTION Adults. Lower leg most common
site (Fig. 25-27). Arm: In young male, consider
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
}.-Cellulitis
. . :~1. - -Necrotlzlng
fuel Ills
FIGURE 25-25 Structural components of the skin and soft tissu•,superficial infections, and
Infections of dte deeper structures The rich capillary network beneath the dermal papillae plays
a key role In the localization of Infection and In the development of the acute Inflammatory reaction.
(Reproduced with pennission fi"om Stevens DL Infections of the skin, muscles, and soft tissues. In: Longo
DL., Fauci AS, Kasper DL., et al, eds. Harrison's Principles ofInternal Medidne. 18th ed. New York, NY: McGrawHill; 2012.)
FIGURE 25-26 Cellulitis at portal of •ntry; MSSA 51-year-old male wi\tl interdigital tinea pedis
noted pain on the dorsum of his foot. KOH preparation was positive for demtatophytic hyphae.
Methicillin-sensitive 5. aureus was Isolated on culture of the webspace.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-27 Cellulitis lower leg:
MRSA 70-year-old male with increasing
erythema and edema of the lower leg
associated with fever.
FIGURE 25-28 Recurrent cellulitis of the arm with
chronic IJmphedema: MSSA Right breast cancer
had been treated with mastectomy and lymph node
excision 10 years previously. Lymphedema of the right
arm followed. Hand dermatitis was secondarily infected
wlth MSSA. Cellulitis occurred repeatedly In the setting
of chronic lymphedema.
IV drug we; in female, postmastectomy
(Fig. 15-28). Thmk: Operative wound site.
Pace: Following .rhi.nitia. conjunctivitis, pharyn-
gitis; associated with colonization of.nares by
S. aureus and of pharynx by GAS.
VARIANTS OF CELLULITIS BY PATHOGEN
S. aureus: Portal of entry 18 U8ually apparent;
cellulltis is an extension offocal lnfectio:n.
Tolin syndromes: Scalded-skin syndrome. TSS.
Endocarditis may follow bacteremia.
Beta-hemolytic streptococci GAS (Streptocoaus pyogenes) colonize skin and oropharynx.
GBS and GGS colo.nize anoge:nital regio:n.
Beta-hemolytic streptococc:al soft-tissue infections spread rapidly along superfidal cutaneous lymphatic vessels. presenting tender red
expanding plaques, i.e., erysipelu (Figl.lS-29
and 25-30). Following childbirth, known as
puerperal sepsis; infection can extend into
pelvia. GBS cellulltis occurs in neonates; :tugh.
morbidity and mortality. GAS iD.fectl.on with
necrotizing fasciitl.s and streptococcal TSS has
high morbidity and mortality.
E. rlausiopathiae: :Erysipeloid occW"S in
individuals who handle swine, sheep. poultry.
or fish. Painful, inflamed plaque with sharply
defined irregular raised border occurring at
the site of inoculation, i.e., the fingers or hand
(Fig. 2S..31), spreading to the wrist but not to
forearm. Color: Purplish red acutely; brownish with resolution. Bnlargei peripherally with
central fading. Usually DO systemic: symptoms.
Ecthyma gangrenosum: Rare variant of necrotizlng soft-tissue lnfectlon caused by P. aeruginosa in iU pmients. Clinically characterized
by infarcted center with erythematous halo,
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-29 EryslpiNs of thigh: group B streptococcus 52-year-old female
with fever. Portal of entry was an insect bite in the popliteal fold. Lesion was very
painful.
expanding rapidly without effective treatment
(Fig. 25-32). Distribution: Most commonly
in the axilla. groin, or perineum. Prognosis
depends on prompt diagnosis. treatmeut, and
restoration of host defense defects. usually
corredion of neutropenia.
H. inftuenzae: Occurs mainly 1n children
<2 years. Cheek. periorbital area. head, and
neck are most common sites. Clinically. swelling, characteristic violaceous erythema hue.
Use ofHlb vaccine bas dramatically reduced
inddence.
V. vulnificu.s, V. dwlerae non-01 and non0 139. Underlying disorders: Cirrhosis, diabetes,
immunosuppression, hemochromatosis, and
thalassemia. Follows ingestion of raw/undercooked seafood, gastroente.ritls, bactetemJa
with seeding of sk1n; also expomre of skin to
seawater. Characterized by bulla formation,
necrotizing vasculitis (Fig. 25-33). Usually on
the extremities; often bilateral.
Aeromonas hydrophila: Water-assodated.
trawn.a; preexisting wound. Immunocompro-
mised host Lower leg. Necrotizing soft-tissue
Infection.
C. canimorsus. Immunosuppression or
asplenta; exposure to dog saliva or bite. Causes
fulminant sepsis and disseminated intravascular coagulation (see Septic shock: ischemic
necrosis of acral sites, p. 567).
P. multocida: Most common cause ofinfection following animal bite; soft-tissue infection.
Clostridium specles •.Associated with trauma;
contamination by soil or feces; malignant
intestinal tumor. Infection characterized by gas
production (crepitation on palpation), marked
systemic toxicity. NecrotWng infection.
Nontuberculous mycobacteria. History of
recent surgery, iDJectl.on, penetrating wound,
systemic corticosteroid therapy. Low-grade
cellulitis. Multiple sites ofinfection. Systemic
findings lacking.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-30 Erplpllu of face: group A streptococaJs Painful, well~efined, shiny, erythematous,
edematous plaques Involving the central face of an otherwise healthy male. On palpation, the skin Is hot
and tender. There is fever (395").
FIGURE 25-31 Erplpllold of hand A well
demarcated, violaceous, cellulltfc plaque (Without
epidermal changes of scale or vesiculation) on the
dorsa of the hand and fingers, occurred following
cleaning fish; the site was somewhat painful,
tender, and warm.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-S2 EdfaytrNI gattglWIIOS4lm of buttock: P. fHiruginos(J A 30.year"()ld male with HIV disease and neutropenia. (A) An extremely painful, infarcted area with surrounding erythema present for
5 days. This primary cutaneous Infection was associated with bacteremia. (B) Two weeks later, the lesion
had progressed to a large ulceration. The patient died 3 months later of P. oeruglnosa pneumonitis associated with chronic neutropenia.
FIGURE 25-33 Bllataral cellulitis of legs: V. wlnllfcus Bilateral hemorrhagic plaques and bullae on
the legs, ankles, and feet of an older diabetic with cirrhosis. Unlike other types of cellulitis In which microorganisms enter the skin locally, which is caused by V. vulnificus, usually follows a primary enteritis with
bacteremia and dissemination to the skin. Most cases initially diagnosed as bilateral cellulitis are inflammatory (eczema, stasis dermatitis, psoriasis) rather than infectious.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
Cryptococcus neoformans: Immunocompromised. Red, hot, tender, edematous plaque on
extremity. Rarely multiple noncontiguous sites.
Mucormycoais: Usually occurring in individuals with uncontrolled diabetes.
Nocardiosis: See Cutaneous Nocardia Infections, p. 559.
Eumycetoma: See Section 26.
Chromoblastomycosis: See Section 26.
DIFFERENTIAL DIAGNOSIS
ERYSIPELASJCELWLITIS Deep vein thrombophlebitis, urticaria, insect bite (hypersensitivity
response), fixed drug eruption, erythema nodoswn. acute gout, and erythema migrans (EM).
NECROTIZING STIS Vasculitis, occlusive vasculopathy, peripheral vascular disease, calciphylaxis, warfarin necrosis, traumatic injury,
cryoglobulinemia, pyoderma gangrenosum,
and brown recluse spider bite.
underlying diseases, travel history, animal
exposure, history of bite, and age. Confirmed
by culture in only 29% of cases in immunocompetent patients. Suspicion of necrotizing
fasciitis (see below) requires immediate deep
biopsy and tissue culture.
COURSE
With timely diagnosis and treatment, softtissue infection resolves with oral or parenteral
antibiotic treatment.
Dissemination of infection (lymphatics,
hematogenously), with metastatic sites of
infection occurring, if effective treatment is
delayed In immunocompromised patients,
prognosis depends on prompt restoration of
altered immunity, usually on correction of
neutropenia.
TREATMENT
DIAGNOSIS
Clinical diagnosis is based on morphologic
features oflesion and the clinical setting, ie.,
Systemic high dose antibiotic treatment
according to type and sensitivity of microbial
organism.
NECROTIZING SOFT-TISSUE INFECTIONS ICD-10: M72.510
• Characterized by rapid progression of infection with extensive necrosis of soft tissues and overlying
skin. Necrotizing fasciitis.
• Etiology. Usually polymicrobial, historically beta-hemolytic GAS. Necrotizing soft-tissue infections also
caused by P. aeruginosa and Clostridium species.
• Portal of Entry. May begin deep at site of non penetrating minor trauma {bruise, muscle, or strain).
Minor trauma, laceration, needle puncture, or surgical incision on an extremity.
Clinical variants of necrotizing soft-tissue infection differ with causative organism, anatomic location
of infection, or underlying conditions. Streptococcal necrotizing myositis occurs as a primary myositis.
StreptococcaiTSS may occur with necrotizing fasciitis. GBS causes necrotizing fasciitis in episiotomy
incisions.
• Diagnosis. Imperative in understanding pathogenesis and deciding on the appropriate antimicrobial
and surgical therapies.
• When skin necrosis is not obvious, diagnosis must be suspected if there are signs of sepsis and/or some
of the following local symptoms/signs: severe pain, indurated edema, bullae, cyanosis, skin pallor,
skin hypesthesia, crepitation, muscle weakness, or foul smelling exudates.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-34 Necrotizing hsditis of buttock Black eschar within an erythematous, edematous
plaque involving the entire buttock with rapidly progressive area of necrosis.
CLINICAL MANIFESTAnON
Local redness, edema. wmmth, pain in the
involved site, typic::ally on an extremity.
Characteristic findinp appear within 36 to
72 h after onset Involved soft ti&su.e becomes
dusky blue in color; vesicles or bullae appear.
Infection spreads rapidly along :6tsdal planes
(Fig. 25-34). Extenslve, cu.tan~us soft-tissue
necrosis develops. Involved tissue may be
bacte.rem.l.a. Secondary thrombophlebitis
occurs. Without surgical debridement necrotizing fasciitis is fatal
DIFFERENTIAL DIAGNOSIS
Pyoderma gangrenosum. cak.lphylaxis. purpura fulminans. warfarin neaosis, pressure
ulcer, and brown recluse spider bite.
anesthetic. Necrosis manifests as a black esc:Mr
with S\UTOUDding irregular border of erythema.
TREATMENT
Fever and other conatitutional symptoms an:
prominent as the in1lamm.atory process extends
rapidly over the next few days. Metastatic
abscesses may occur as a consequence of
SURGICAL DEBRIDEMENT
Requires early and
complete surgical debridement of necrotic
tissue in combination with high-dose antimiaobial. agents.
LYMPHANGITIS IC0-10: 189-1
• An Inflammatory process Involving the subcutaneous lymphatic channels.
• Etiology.
• Acute lymphangitis: GAS; S. aureus; other bacteria. Herpes simplex virus.
• Subacute to chronic nodular lymphangitis: Mycobacterium marinum, other NTM. Sporotrix schenkii,
and N. brasiliensis.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
CLINICAL MANIFESTATION
ACUTE LYMPHANGITIS Portal of entry: Break in
akin, WUUild, S. aumu paronychia. and primary andherpes simplex infectiOil. Pain and/or
erythema proximal to break in skin. Red linear
streaks and palpable lymphatic cords, up to
sevaal centimeters in width, extend from the
local lesion toward the regional lymph nodes
(Fig. lS-35), which are usually enlarged and
tender.
Subacute and chronic lymphangitis; nodular
lymphangitis; see discussion on Nocardiosis
(p. 559), NTM infection (p. 583), and sporotrichosia (see Section 26).
DIFFERENTIAL DIAGNOSIS
UNEAR LESIONS ON EXTIIEMITIES Phyto-all.ergic
contact dcrmatilia (polson ivy or oak),
phytophotode:rmatltis, and superficial thrombophlebitis.
NODULARLYMPHANGmS M. marinum, N. Pmuiliensis, and S. scheru:kii infectiOil.
DIAGNOSIS
The combination of an acute peripheral lesion
with pnmm.J. tender/painful red linear atn:w
leading toward regional lymph nodes Ia diagnostic oflymphaDgitls. IsolateS. aumu or GAS
from portal of entry.
COURSE
Reaolves with correct diagnosis and treatment
Bacteremia with metastatic infection uncommon with adequate trealment
TREATMENT
Systemic antibiotic depending on causative
organiml.
FIGURE 2S.J5 Acute !rmPhangltll Gf forurm .S: aureus A small
area of1he cellulitis on the volar wrist
with a tender linear streak extending
proximally up the arm; the Infection
spreads from the portal of enny within
the superfidallymphatic vessels.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
WOUND INFECTION
• Wound.lnjury In which skin Is surgically lndsed or traumatically Injured (open wound) or In which
blunt force trauma causes a contusion (closed wound). Wound infection: Skin and all wounds are
colonized by bacteria and other microbes, i.e.. cutaneous microbiome. Infection is characterized by
pain, tenderness, purulence, erythema, warmth, and must be diagnosed on clinical as well as culture
findings.
ETIOLOGY AND EPIDEMIOLOGY
CLASSIFICATION
'&aumatic wounds: Open or
closed wounds (Pig. 25-36). Surgictll wounds:
lnfect:lonln surg!.callncWo:ns (Fig. 25-37).
Burn wounds: Burn wound may become super-
tidally colonized with S. aureus; open burnrelated surgical wound infection; burn wound
cellulitis; invasive infection in debrided burn
wounds (Fig. 25-38). Chronic u1cer.s: Arterial
insuffidency; venous lnsuflidency; neuropathic
ulcers/diabetes mellitus; pressure ulcers (bedsores) (Pip. 25-39 to 25-41). Bites: Animal;
human; insect.
EPIDEMIOLOGY S. aureusln the most common
pathogen in wound iDCections. MSSA. and
increasingly MRSA. Surgical wound infection
is up to 10 times more likely among patients
who harborS. aureus in nares. Hospitalacquired (nosocomial) or health-care-
associated infections (most commonly 81l.J:81cal
wound infections) are the most common
complication affecting hospitalized patients.
PATHOGENESIS Wounds are initially colonized
by skin flora or introduced organisms. In some
cases. these organisms proliferate. causing a
host inflammatory response.
FIGURE 25-36 Lec:eratlon Infection In renal
transplant rec:ipiant; MRSA 6o-year-old male
immunosuppressed renal transplant recipient was
unaware of a laceration on the calf. Erythema and
induration are seen around the crusted wound.
MRSA was isolated on culture. Two circled invasive squamous cell carcinomas are also seen on
the calf.
FIGURE 25·37 Surgical excision wound
Infection: MSSA Surgical wound became painful and tender 7 days after excision of squamous
cell carcinoma; soft tissue (cellulitis) is seen adjacent to the wound margin. Necrotic tissue is seen
in the base.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-SI Bum wound Infection: MSSA 1(}-year-old male with extensive third degree thermal
bum treated with autologous skin grafting has extensive new crusted erosions. MSSA was cultured from
the infected site.
FIGURE 25-Jt Wound Infection of stasis ulcer 75-year-old female with varicose veins and enlarging
stasis ulcer infected with MRSA and Pseudomonas aeruginosa. IV antibiotics were administered. lncomp~
tent veins were treated with endovascular laser ablation. The ulcer healed with minimal scar.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-40 Infection of diabetic ulcer:
MRSA S&year-<!ld male with diabetes mellitus
type 2 had a chronic neuropathic ulcer on the
R-lateral foot. The ulcer rapidly enlarged associated with fever and glucose of 450 mg/dL MSSA
was isolated from the wound. He was hospitalized
and treated with IV antibiotics. He died 3 months
later.
CLINICAL MANIFESTATION
LOCAL INFECTION Tendemess of wound area,
erythema. hot. purulent drainage. and induration. Invasive infection: Mal.a!se, anorexia,
sweats, fever, or chills. Sepsis syndrome: Fever
compulsive disorder excoriates extremities In the
evening. MRSA inrection has occurred repeatedly.
Ulcers resolved with doxycycline, doxepin, and
unna boots applied weekly.
DIAGNOSIS
Because all open wounds are colonized with
and hypotension.
TYPESOFSURGICALINFEC110N5
FIGURE 25-41 Wound infection and cal·
lulltls: MRSA 53-year-old male with obsessive-
Superficial infec-
tion of wound. wound infection with soft-tissue
infection, Le., cellulitis and erysipelas. softtissue abscess, necrotlz.lng soft-tissue infectl.on.
and tetanus.
DIFFERENTIAL DIAGNOSIS
Allergic contact dermatitis (e.g., neomycin),
pyoderma sangrenosum, and vasculitis.
microorganislll.S, diagnO&is of infection relies
on the dinl.cal characte.rlstic& of the wound.
Wound culture identllies the potential
pathogen(s).
TREATMENT
Although all wounds require treatment.
only infected lesions require antimicrobial
therapy.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
DISORDERS CAUSED BY TOXIN-PRODUCING BACTERIA
• Bacteria colonize skin and mucosa (mucocutaneous microbiome), replicate locally, and elaborate
toxins that cause local mucocutaneous and systemic disorders.
• Clinical syndromes caused by these toxins:
• S.aureus.
Bullous impetigo (see Figs. 25-1 2 and 25-1 3).
Staphylococcal scalded-skin syndrome. Generalized form with extensive epidermolysis,
followed by desquamation.
TSS. Abortive form, staphylococcal scarlet fever.
• GAS.
Scarlet fever.
Streptococcal TSS.
Bacillus anthracis: Anthrax.
Corynebacterium diphtheriae: Diphtheria.
• Clostridium tetani:Tetanus.
STAPHYLOCOCCAL SCALDED-SKIN SYNDROME ICD-10: LOO
• Etiology. 5. aureus producing exfoliative toxins. Occurs in neonates and young children.
• Pathogenesis. Illness develops after toxin synthesis and the subsequent toxin-initiated host response.
Exotoxins (Exfoliatin) cleave desmoglein-1 in epidermal granular cell-layer, resulting in its separation.
CLINICAL MANIFESTATION
LOCALIZED FORM See "Bullous ImpetigoD in
Figures 25-12 and 25-13. Intact flaccid purulent
bullae, clustered. Rupture of the bullae results in
moist red and/or crusted erosive lesions. Lesions
are often clustered in an intertriginous area.
GENERALIZED FORM Exfoliative toxin-induced
changes: macular scarlatin!fimn rash (staphylococcal scarlet fever syndrome) or diffuse, illdefined erythema and a fine, stippled, sandpaper
appearance occur initially. In 24 h, erythema
deepens and involved skin becomes tender. Initially, periorifid.ally on face, neck, axillae, groins;
becoming more widespread in 24 to 48 h.
Superficial epidermis is most pronounced periorificially on face; in flexural areas on neck, axillae, groins, and antecubital areas; back (pressure
points). With epidermolysis, epidermis appears
wrinkled and can be removed by gentle pressure
(skin resembles wet tissue paper) (Nikolsky sign)
(Fig. 25-42). In some infants, flacci.d bullae
occur. Unroofed epidermis forms erosions with
red, moist base (Fig. 25-43A). Desquamation
occurs with healing (Fig. 25-43B).
Mucous membrane, uninvolved. TSS, in
comparison, manifests with mucosal erythema.
DIFFERENTIAL DIAGNOSIS
Kawasaki syndrome, adverse cutaneous drug
eruption, or scarlet fever.
DIAGNOSIS
Clinical findings confirmed by bacterial
cultures from bullous impetigo or nares. Erosions
from epidermolytic toxin may not yield bacteria.
COURSE
With adequate antibiotic treatment, superficially denuded areas heal in 3 to 5 days associated with generalized desquamation; there is
no scarring.
TREATMENT
S)15temic antibiotic to treat infection and stop
toxin production.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-42 Suph,toCOC'GII sc:~ldeckldn JJndromr. Nlkolsky sfgn The skin of this infant is diffusely erythematous; gentle pressure to the skin of the arm has sheared off the epidermis, which folds like
tissue paper.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-43 Staphylococcal saldad-slcln
SJildrome: sloughing and desquamation In this
infant, painful, tender, diffuse erythema was followed by generalized epidermal sloughing and erosions. S. aureus had colonized the nares with perioral
impetigo, the site of exotoxin production. (A) Extensive desquamation is seen on buttocks and legs {B).
TOXIC SHOCK SYNDROME ICD-10: A48.3
• Etiology. Exotoxin (TSST-1 )-producing S. aureus; less commonly GAS.
• Staphylococcal TSS.
• Menstrual TSS (MTSS).
• Nonmenstrual TSS {NMTSS) occurs secondary to a wide variety of primary and secondary S. aureus
infections of underlying dermatoses.
• StreptoCOccal TSS. Skin or soft-tissue Infection with toxin production.
• Clinical manifestations. Rapid onset of fever, hypotension, and multisystem failure. Rash.
Generalized and blanching scarlatiniform erythroderma •painless sunburn: most intense around
infected areas. Fades within 3 days of appearance. Edema. Mucosal erythema/ulcers. Desquamation
one week after onset of rash. Begins with the torso, face and extremities, followed by the hands and
feet.
• Course. StreptoCOccal TSS 25 to 50% mortality. NMTSS 6.49& mortality; MTSS 259& mortality.
• Treatment Systemic antibiotic to treat infection and stop toxin production. Supportive.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
SCARLET FEVER IC0-10:A38
•
•
•
•
•
•
•
•
Etiology.
Group A ~-hemolytic streptococcus (GAS) (5. pyogenes), erythrogenic toxin-producing strains.
Exfoliative toxin (ET)-producing S. aureus.
Clini01l Manifestation. Infection: pharyngitis, tonsillitis, infected wound, or dermatoses.
Taxln Syndrome (Scarlet Fever). Acutely ill with high fever, fatigue, sore throat. headache, nausea,
vomiting, and tachycardia. Anterior cervical lymphadenitis associated with pharyngitis/tonsillitis.
Scarlatiniform exanthema occurs in nonimmune persons.
Exanthem. Face flushed with perioral pallor. Rnely punctate erythema is first noted on the upper
part of the trunk (rtg. 25-44); may be accentuated in skin folds such as the neck, axillae, groin,
antecubital, and popliteal fossae; linear petechiae (Pastia sign) occur in body folds. The palms and
soles are usually spared. Inltlal punctate lesions become confluently erythematous, I.e., scarlatiniform.
Exanthem fades within 4 to 5 days, followed by desquamation on the body and extremities and by
sheet-like exfoliation on the palms and fingers as well as the soles and toes. 1n subclinical or mild
infections, exanthem and pharyngitis may pass unnoticed.
Enanthem. Pharynx beefy red. Forchheime~ spots: Small red macules on soft palate. Punctate
petechiae may occur In the palate. White tongue: Initially Is white with scattered red, swollen papillae
(white strawberry tongue) (Flg. 25-45). Red strawberry tongue: By the fourth or fifth day, the hyperkeratotic membrane is sloughed, and the lingular mucosa appears bright red (Fig. 25-45).
Complications. Acute rheumatic fever 1 to 4 weeks after onset of pharyngitis Oncidence markedly
decreased over past five decades), acute glomerulonephritis more common after Impetigo with
nephrltogenlc strain ofGAS (types 2, 4, 12, 49 and 60), guttate psoriasis (see Section 3) and erythema
nodosum (see Section 7).
Differential Diagnosis. Viral exanthema, adverse cutaneous drug eruption, Kawasaki syndrome, and
infectious mononucleosis.
Diagnosis. Rapid direct antigen tests: Used to detect GAS antigens In throat swab specimens. Isolate
GAS on culture of specimen from throat or wound. Blood cultures are rarely positive. Centor criteria
for diagnosis of acute streptococcal pharyngitis: History of fever; tonsillar exudates; tender anterior
cervi01l adenopathy; absence of cough.
Treatment Systemic penicillin is the drug of choice; alternatives are erythromycin, clindamycin,
clarlthromycln, or cephalosporlns.
FIGURE 25-44 Scarlet fever: exanthem Finely
punctated erythema has become confluent (scarlatiniform); petechiae can occur and have a linear
configuration within the exanthem in body folds
(Pastia line}.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-45 Scllrlet fever: white and red strew-
berry tongue The white patches at the back of the
tongue represent residua of the initial white strawberry
tongue.
CUTANEOUSANTHRAX ICD-10:A22.000
• Etiology. B. onthrocis, a nonmotile, gra~positive, aerobic rod. Zoonosis. Spores can remain dormant
In the soli for decades. Low-level germination occurs at the primary site, resulting In local edema and
necrosis. Primary Infection: Skin, pulmonary, and Gl. Pathogenesis: Toxin mediated.
• Transmission. Zoonosis of mammals, especially herbivores. Human infections result from contact
with contaminated wild and domestic animals or animal products. Human-to-human transmission
does not occur. At risk: Farmers, herders; slaughterhouse, textile workers.
• Cutaneous anthrax. Accounts for 9596 of anthrax cases In the United States.
• Cut or abrasion on exposed sites of head, neck, extremities. Nondescript, painless, pruritic papule
(resembling insect bite) appears 3 to 5 days after introduction of endospores. In 1 to 2 days,
evolves to vesicle(s) ± hemorrhage + necrosis. Vesicles rupture to form ulrers with extensive local
edema (Fig. 25-46}, ultimately forming dry eschars (1 to 3 em). Satellite lesions can form in a nodular lymphangiTis proximally on edematous extremity (Fig.lS-46).
• Differential Diagnosis, Ecthyma, brown recluse spider bite, ulceroglandular tularemia, orf, or glanders.
• Diagnosis. Isolation of B. onthrods from skin lesions, blood, or respiratory secretions, or by measuring
specific antibodies in blood of persons with suspected symptoms.
• Course and Treatment. Mortality rate in untreated persons with cutaneous anthrax is about 2096.
Systemic penicillin Is the drug of choice; alternatives are erythromycin, azathloprln, clarlthromycln, or
cephalosporins.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-46 A cutaneous anthrax A 4o-year-old farmer wfth anthrax. (A) A black eschar at the site
of inoculation with a central hemorrhagic ulceration on the thumb associated with massive edema of the
hand. (B) A nodular lymphangitis extending proximally from the primary lesion on the thumb.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
CUTANEOUS DIPHTHERIA IC0-10: A30
• Etiology. Corynebocretlum diphtheria. Cases In Industrialized countries extremely rare.
• Pathogenesis. Localized Infection caused by toxigenic and nontoxlgenlc strains. Acute Infection may
involve any mucous membrane or skin wound. Toxin causes myocarditis and peripheral neuropathy.
• Clinical Manill!stations. Cutaneous: Nonspecific wound. Thick gray membrane in the pharynx. Mycard~
tis, arrhythmias. Polyneuritis involving cranial nerves: Diplopia, slurred speech, or difficulty swallowing.
• Diagnosis. Made by Isolation of C diphtheria on the culture of the wound.
• Treatment Penicillin, erythromycin, or antitoxin.
Vacclnlltfon. Immunity to vaccine wanes over time. Decennial boosters are recommended.
CUTANEOUS NOCARDIA INFECTIONS
• Etiology. Nocardia species of bacteria. Saprophytic gram-positive anaerobic actinomycetes living in
soli. Actinomyces were mistakenly classified as fungi. N. brasiliensis Is usually associated with disease
limited to the skin. Infection follows traumatic inoculation into the skin on extremity.
• Clinical Manill!station. Cellulitis. Inflammation 1 to 3 weeks following traumatic inoculation. Expanding
erythema, induration; firm, nonfluctuant Untreated, infection can progress to involve adjacent muscles,
tendons, bones. and joints. Dissemination is rare, and occurs in people with host defense defects.
Nodular Lymphangitis. Begins as a nodule at the Inoculation site. Untreated, Infection extends Into
lymphatic vessels with linear subcutaneous nodules.
Cutaneous Nocardiosis. Nodule occurs at the site of inoculation (Fig. 25-47), most commonly at
the feet or hands. Untreated, infection expands forming plaques with Sinus tracts and fistula form;r
tlon (Fig.lS-48). As with eumycetOma, grains (dense masses of bacterial filaments extending radially
from a central core) may be seen In discharging pus and tissue. After years, deformity of extremity
may occur with involvement of adjacent anatomical structure.
• Diagnosis. Grains and organism in purulent discharge. Isolate and speciate Nocardia in pus. exudate,
or tissue. Sensitivities determined on isolated organism.
• Differential Diagnosis. Nodular Lymphangitis. Sporotrichosis, NTM Infection.
Acdnomycetoma. Eumycetoma.
• Course. Tends to relapse, especially with defective host defenses.
• Treatment Trimethoprim/sulfamethoxazole is the preferred antimicrobial agent. Minocycline or
linezolid. Surgical excision/debridement.
FIGURE 25-47 Cut.neous noe~~rdlosls A
23-year-old female from Central America with a
painful lesion for 6 months. Confluent erythematous
violaceous nodules on the right prepatellar area arising in an abrasion. Nocardia brasiliensis isolated on
culture of biopsy specimen. The lesion resolved with
trimethoprim-sulfamethoxazole.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-48 Chronic cutaneous nocardlasts Swelling, multiple sinus tracts, and Involvement of
the foot (Used with permission fi'om Amor Khachemoune, MD and The Ronald 0. Perelman Department
of Dermatology, NYU School of Medicine.)
RICKEn'SIAL DISORDERS
• Rickettsiae. Gram-negative bacteria. Coccobacilli/short bacilli; obligate intracellular.
• Transmitted to humans by arthropods; tick, mite, flea, louse; mammalian reservoirs; humans are
Incidental hosts.
• Rickettsial Disorders. Spotted fever group, typhus group, and scrub typhus group.
CLINICAL MANIFESTAnON
E:r:posure to vectors or animal reservoirs, travel
to or residence in endemic locations (http://
www.cdc.grJVIncidodldiseases/submenusl
sub_typhus.htm).
'flJche noire (black. spot or stain). Co:ln-llkc
lesion with ce:nttal eschar and a :red halo at the
site of the vector-feeding bite site.
EXANTHEM Macules-papules. Exception: Rickettsialpox with papules-~es.
LATER FINDINGS VARYING WITH PATHOGEN May
become: hemorrhagic with vasculitis.
produce vasculltis with necros:ls and thrombosis.
COURSE
Rickettsiae can cause Ufe-threatening infections. Order of decreasing case-fatality rate:
R. rickettsii [Rocky Mountain spotted fever
(RMSF)]; R. prowazelai (epidemic louseborne typhus); Oricmtia tmtsugamwhi (scrub
typhus); R. conorll (Mediterranean spotted
fever); R. typhl (endemic murine typhus);
in rare cases, other spotted fever group
organisms.
DIAGNOSIS
Confirmed by paired serum samples after con-
valescence or demonstration of rickettsiae.
DERMATOPATHOLOGY Riclcettsi.ae multiply
in endothelial cells of small blood vessels and
TREATMENT
Doxycycline is the drug of choice, 100 mg BlD
orally. Alternates: Ciproftoxacin or chloramplu:nicoL
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
TICKSPOTTEDFEVERS IC0-10:A77.0
• Characteristic exanthema: macules and papules.
• RMSF R. rickettsia.
• Boutonneuse fever R. conorii. Siberian tick typhus R. sibirico, Australian tick typhus R. autralis, oriental
spotted fever R.japonico, African tick bite fever R. africae, etc.
• Rickettsialpox R. alcori.
• Transmission. Vector. Dermarocenror andersonVvorlablls (American dog tick), Amblyomma amerlamnum (lone star tick), Rhipicephalus sanguineus (Brown dog tick), b«xJes holocydus/tasmani. Worldwide
distribution. Attachment often unnoticed.
• Inoculation. Bite; contact vector feces with open wound. Travel history: Recent travel to or living in
endemic region.
CLINICAL MANIFESTATION
Incubation period: Average 7 days after tick
bite. Onset sudden of symptoms In 5096 of
patients. Most common: Headache, fever;
also chills, myalgias, arthralgias. malaise, or
anorexia.
Tlche noire at inoc:ulation site. An inoculation eschar: papule forms at the bite site and
evolves to a painless. blac:k.-austed ulcer with
red halo (Fig. 25-49) in 3 to 7 days. Occurs in
all spotted fevers e:xcept RMSF.
EXANTHEM About 3 to 4 days after appearance
of Mche noire, an erythematous mac:ul.es and
papules appear on trunk; may subsequently
disseminate, involving fac:e, extremities,
and the palms or soles. Density oferuption
heightens during next few days. In severe cases,.
l.esiob8 may become hemonhagic.
FIGURE 25-49 African spotted tev.r: tach• nolr 65-year-old female, who had recently returned
from trip to South Africa, noted a lesion on the thigh and reported flu-like symptOms. A central dark crust
(tache nolr) with halo of erythema Is seen at the site of tick bite. Paired serologies confirmed the diagnosis of African spotted fever. Symptoms resolved with doxycycline.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
DISTAIBII110N Similar pattern of spread and distribution in all spotted fuvers-trwik. extremities. face (centrlfugal)-exctpt RMSF, which
tirst appears at wrists and ankles and spreads
centripetally.
DIAGNOSIS
Clinical, epidemiologic, and convalescent serologic data establish the diagnosis ofa spotted
fever-group rickettsiosis.
SYSTEMIC FINDINGS Conjunctivitis. pharyngitis.
photophobia. Central nervous system (CNS)
symptoms: Confusion, stupor, dellrlum, seizures, coma; common in RMSF but not seen in
other spotted fevers.
DIFFERENTIAL DIAGNOSIS
VIral a:anthems, drug eruption, vasculitl.s.
COURSE
In France and Spain, mortality rate is similar
to that of RMSF. Spotted fevers are usually
m.Uder in children. Morbidity and mortallty
rates are higher (up to 5096) in individuals
with diabeteo mellitus. cardiac insufficiency,
and alcoholism.
ROCKY MOUNTAIN SPOTTED FEVER ICD-10: A77
• Etiology. Rickettsia rickettsii.
• Transmission. Bite of Infected tick; only 60% of patients are aware prior tick bite. Most common In
springtime in the southeastern United States; >2000 reported cases of RMSF in the United States
annually.
CLINICAL MANIFESTATION
Abrupt onset ofsymptoms. Fever, chills, shaking rlgor. Anorc:Jia. nausea. vomiting. Malaise.
lrrltabllity. Severe headache. Mya1g1a. Can
mimic acute abdomen, acute cholecystitis. and
acute appendicitis. Dche noire uncommon in
RMSF.
Early exanthem: 2 to 6 mm, pink. blanchable
macules (Figs. 25-50 and 25-51).111 1 to 3 days.
evolves to deep red papules (Fig. 25-52). Cb.aracteristically. rash begins on wrists, forearms,
and ankles and somewhat later on the palms
and soles. Within 6 to 18 h, the rash spreads
centripetally to the arms. thighs. trunk. and
tick exposure in endemic areas. Diagnosis
made clinically and confirmed later. Only 3%
of patients with RMSP present with the triad of
rash. fever, and history of tick. bite during the
tirst 3 days of illness.
face.
Later ennthem: In 2 to 4 days, become hemonbagi.c, no longer blanchable. Loc:al edema.
Petechiae may occur on the palms and soles.
Necrosis occurs in aaaJ. extremities following
prolonged hypotension. Pedal edema.
Spotless fever: SlO% of cases. Associated
with higher mortaUty rate because of the delay
in dlagnosls.
DIAGNOSIS
Clinical and epidemiologic con.sl.derations are
more important than a laboratory diagnosis
in early RMSF. Su&pect in febrile children,
adolescents,. and men >60 years of age with
FIGURE 25·50 Rocky Mourrtain spotted
fever: early Erythematous macules and papules
appeared Initially on the wrists of a young child.
The lesions are not completely blanchable with
pressure, indicating early hemorrhage of dermal
blood vessels.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-52 Rocky Mountain spottacll
fever: late Disseminated hemorrhagic macules
FIGURE 25-51 Rocky Mountain spotted
fev•r: HrfJ Erythematous and hemorrhagic
macules and papules appeared initially on the
ankles of an adolescent
COURSE
Severe course is associated with older age,
delay in diagnosis, delay in or no treatment
and is more common in men, darker-skinned
individuals, and those with alcoholism or G6PD
defideru:y. Fatality rate: 0.5%. Fulminant RMSF
defined as a fatal disease whose COU1'1le is unusually rapid (Le., 5 days from onset to death) and
and papules on the face, neck, trunk. and arms on
the fourth day of febrile illness in an older child.
The initial lesions were noted on the wrists and
ankles, subsequently extending centripetally.
usually characterlzed by early onset of neurologic signs and late or absent rash. In uncomplicated cases, defervescence usually occurs within
48 to 72 h after initiation of therapy.
TREATMENT
Doxycycline is preferred treatment. Chloramphenicol
RICKETTSIALPOX ICir10: A79.1
• Epidemiology. R. okari. Vector: Mice mite (Liponyssoides sanguineus), other mites; transovarian transmission. Geography: United States, Europe, Russia, South Africa, Korea, and Europe.
CLINICAL MANIFESTAnON
COURSE
Uche noire (Fig. 25-53). At tick bite site.
EXANTHEM 2 to 6 days after the onset of non-
Fever resolves In 6 to 10 days without treatment
with doxycycline.
specific symptoms, red macules and papules
appear. May evolve to characteristic vesicles
(pox); austed erosions occur. Lesions usually
heal without scarring.
DIFFERENTIAL DIAGNOSIS
V1I8l. exanthems, varicella, and pityriasi&
llchenoldes et varloUformls a.cuta.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-53 Rickettsialpox: tache noire A crusted, ulcerated papule (eschar) wlth a red halo
resembling a cigarette burn at the site of a tick bite.
INFECTIVE ENDOCARDITIS IC0-10: 133
• Inflammation of endocardium. Infective and nonInfective. Usually of hean valve. Characterized by
vegetations that are made up of fibrin, platelets, and inflammatory cells (also microcolonies of microorganism if infective endocarditis).
• Infective endocarditis. Occurs at sites on altered endothelium or endocardium. The primary event is
bacterial adherence to damaged valves during transient bacteremia. Bacteria grow within the cardiac
leslon{s), I.e~ vegetattons, with local extension and cardiac damage. Subsequently, septic embolization
occurs to skin, kidney, spleen, brain, etc. arculating immune complexes may result in glomerulonephritis, anhritis, or various mucocutaneous manifestations of vasculitis. Embolization of vegetative
fragments results in infection/infarction ofremote tissues.
• Acute bacterial endocarditis rapidly damages cardiac structures, hematogenously seeds extracardlac sites, and may progress to death In a few weeks.
• Subacute bacterial endocarditis (SBE) causes structural damage slowly, rarely causes metastatic
infection, and is gradually progressive unless complicated by a major embolic event or ruptured
mycotic aneurysm.
• Nonlnfectlve endocarditis: Occurs on previously undamaged valves. Hypercoagulable state. Marantic
endocarditis. Libman-Sacks endocarditis.
• Diagnosis: Based on clinical features. echocardiogram, and blood cultures.
CLINICAL MANIFESTAnON
Common with acute S.
aureus endocarditis. Hematogenously seeded
SEPTIC ART'EIUAL EMBOLI
focal infection (Pig. 25·54). Apparent in up to
50% of patients.
OStiA NODES Painful. erythematous nodules
mo&t commonly found on the pads of the
fingers and toes of some patients with iDfective
endocarditis.
JANEWAY LESIONS Nontender. erythematous.
and nodular lesiom most commonly found
on the palms and soles (Fig. Z5-55) ofsome
patients with infective en.doc:arditls.
SPLINTER HEMORRHAGES A small linear longitudinal subungual hemorr
initially red then
brown. Middle third of
d in SBE.
PETECHIAL LESIONS Small. no:nblanching.
reddish-brown macules. Occur on extremities.
upper chest. mucous membranes [conjunctivae
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-54 Septic vasculitis assoc:1ated
wtth becteremlll Dermal nodule with hemorrhage and necrosis on the dorsum of a finger.
This type of lesion occurs with bacteremia (e.g.,
S. aureus, gonococcus) and fungemia (e.g.,
Candida troplcalls).
FIGURE 25-55 lnfactiv• •ndocarditis, acutr. JaMWay lasions Hemorrhagic,
Infarcted papules on the volar fingers In a patient w1th S. aureus endocarditis.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-56 lnfectlve endocardtt1s, acute: subc:onjunc:tlnl hem·
orrflage Submucosal hemorrhage of
the lower eyelid in an elderly diabetic
with enterococcal endocarditis; splinter hemorrhages In the mldportlon of
the nail bed and Janeway lesions were
also present on the volar fingers. Infection followed urosepsis.
(Fig. 25·56), palate]. Occur in crops. Fade after
a few days (20 to 40%).
ROTH SPOTS White spot in the retina close to
the optic disk. often surrounded by hemorrhages; also seen in peml.dous anemia and
leukemia.
SEPTIC EMBOLISM Painful, hemorrhagic macules,. papules, or nodules,. wually aaal.location.
COURSE AND TREATMENT
Varies with underlying cardiac disease and
baseline health of the patient, as well as with
the c:ompllcatiollS that occur. Complications:
Congestive heart failure, stroke, other systemic
embolizati.ons. or septic pulmonary embolization. Aortic val~ involvement has a higher risk
of death or need fur sw:gery. Anb"biatia.
SEPSIS lCD: A40
• Sepsis is a whole-body inflammatory state. in response to infection. Can be complicated by multiple
organ dysfunction.
• Characterized by fever or hypothermia, tachypnea, tachycardia, and, in severe cases, multiple organ
dysfunction syndrome.
• Epidemiology.> 1 million cases In the United States annually; >200,000 deaths. Two-thirds of cases
occur in persons hospitalized for other illnesses. Incidence is increasing. Risk factors: Chronic disease
and immunosuppression.
CLINICAL MANIFESTAnON
Cutaneoua infedions as eource of tepds:
Superficial skin infections, soft-tissue infections, wounds. B. gangnmosum (Fig. 25-32):
P. aeruginosa mo8t commonly.
EXANTifEM Su menlngococcem.l.a and RMSF
(Fig. 25-50).
PETEQtiA£ Oltaneousloropharyngeal location
suggem meningococ:cal infection; leas commonly,
H. influenzae.ln patient wid!. tick bite living in
endemic area, RMSF (Pip. 25-51 and 25-52).
HEMORRHAGIC BULLOUS LESIONS V. vulnffo:us
in patient (diabetes mellitus. liver disease)
with history ofeating raw oysters or clams
(Fig. 2S..33).
Disseminated intravascular coagulation. See
Section20.
Severe prolonged hypote:ns:ion with
aaal necrosis ofthefingers, hands, andfeet
(Fig. 2S..57).
COURSE AND TREATMENT
Early sepsis is revemble; septic shock has high
mortality/morbidity. High dose antibiotics
plus treatment of disseminated intravascular
coagulation.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-57 Septic shodc
Jsdtemlc necrosis of aaal
sites Capnocytophaga canimo~us sepsis {dog bite) with
prolonged hypotension and
hypoperfusion resulted in
Infarction offlngers and nose.
MENINGOCOCCAL INFECTION ICD-10: A39
• Etiology. N. meningitidis. colonizes nasopharynx. Infects only humans; no animal reservoirs. Spread by
persons-t«rperson contact through respiratory droplets.
• Demography. The disease occurs sporadically throughout the world. The highest burden of the
disease Is caused by the cyclic epidemics occurring In the African •meningitis belt~
CLINICAL MANIFESTAnONS
Small pink blanchahle rruu:ults and papules oo:ur
soon after onset ofdisease (Pig.15-58). Wrth
vascular fi:iability and he:monbage. petechiae and
ecchymoses occur; first seen on the an:kks. wrists.
u:illae, mucosal rurfaces. and conjunctivae.
A duster ofpete<:h1ae may be seen at pressure
points. e.g.. where a blood pressure cuffhas been
inflatai. Bcchymoses and pu.rpu:rt~. may progress to hemOIThagic bullae, unde:rgo necrosis,
and ulcerate. Confluent necrotic hemorrhagic
lesions may haw b!zarre..sh.aped. grayish to bl.aclt
necrosis, Le., pu.tpu:rt1.julminans) associated with
disseminated intrmlscular coagulation (DIC) in
fulminant disease (Pig. 15-59).
MENINGOCOCCEMIA SEPTICEMIA Meningococci
enter the bloodstream and multiply, damagl.ng
the walls of the blood vessels and causing
bleeding into the skin and organs. Characterized by development of shock and multiorgan
failure. Peripheral gangrene may occur, requiring amputation In those who survive.
WATERHOUSI.·FRIDERICHSEN SYNDROME Fulmi-
nant menlngoc.occal. septl.cemla characterized
by high fever, shock. widespread purpura, disseminated intravascular coagulation, thrombocytopenia, and adrenal insufficiency.
MENINGOCOCCAL MENINGITIS Bacteremia can
result In the seeding of man:y organs. espedally
the meninges. 'Ihe symptoms of meningoo>ecal meningitis are those of typical bacterial
meningitis. namely. fever, headache, stiff' neck.
and polymorphonuclear neu1rophils (PMNs) in
spinal fluid.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25·58 Acute meningococ-
cemia: early exanthem Discrete,
pink-to-purple macules and papules
as well as purpura on the face of this
young child. These lesions represent
early disseminated Intravascular coagulation with its cutaneous manifestation, purpura fulminans.
FIGURE 25·59 Acute meningococcemia: purpura fulmlnans Maplfke, grayto-black areas of cutaneous infarction of the leg in a child with NM meningitis and
disseminated intravascular coagulation with purpura fulminans.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
Intermittent bacteremia. Slow replication seeds various organs:
meninges, pericardium, large joints, and skin.
Host inflammatory reaction limited to seeded
site.
CHRONIC MENINGOCOCCEMIA
DIFFERENTIAL DIAGNOSIS
Adverse cutaneous drug eruptions, vasculitis,
RMSF, and infective endocarditis.
COURSE
Onset of symptoms is sudden and death can
follow within hours. In as many as 10 to 15%
of survivors, there are persistent neurological
defects, including hearing loss, speech disorders, loss oflimbs, mental retardation, and
paralysis.
TREATMENT
DIAGNOSIS
Definitive etiologic diagnosis requires isolation
of meningococci from blood or local site of
infection.
High dose antibiotic therapy and treatment of
DIC.
PROPHYLAXIS Several vaccines are available to
control the disease.
BARTONELLA INFECTIONS
• Etiology. Bartonella spp.; tiny gram-negative bacilli that can adhere to and invade mammalian cells
such as endothelial cells and erythrocytes.
• Transmission. Cat scratch or bite. Body louse or sandfly bite.
CLINICAL MANIFESTATION
Vary with the immune status of the host.
Bartonella henseloe. Immunocompetent
host: cat-scratch disease. HIV disease: bacillary
angiomatosis.
B. bacilliformu. Nonimmune, nonresidents
of endemic area: Oroya fever with severe febrile
illness, profound anemia. With immunity after
convalescence: verruga peruana with red-purple cutaneous lesions (peruvian warts; resemble
angiomatous lesions of bacillary angiomatosis).
B. quintmul. 'Irench fever presenting as a
febrile systemic illness with prolonged bacteremia; no cutaneous manifestations.
Diseases caused by Bartonella species:
• Cat-scratch disease: B. henselae.
• Bacillary angiomatosis: B. henselae,
B. quintana.
• Bacillary peliosis: B. henselae.
• 'french fever: B. quintana.
• Bartonellosis (Carri6n disease); Oroya fever
and verruga peruana: B. bacilliformis.
CAT-SCRATCH DISEASE (CSD) ICD-10:A28.1
• Etiology. B. hense/ae. Reservoir: Domestic cat.
• Transmission. Associated with exposure to young cats. Blood cultures of kittens are frequently
positive for B. hense/ae. Cat flea Ctenocephalides felis transmit infection between cats.
• Demography/Age of Onset. Majority of cases occur in children.
• Pathogenesis. B. henselae causes granulomatous inflammation In healthy individuals (CSD) and
angiogenesis in immunocompromised persons.
CLINICAL MANIFESTATION
INOCULATION SITE Innocuous-looking, small
(0.5 to 1 em) papule, vesicle, or pustule; may
ulcerate; skin color pink to red; firm, at times
tender (Fig. 25-60). Residual linear cat scratch.
Persists for 1 to 3 weeks. Distribution: Exposed
skin of the face and hands.
CONJUNCTIVAE If portal of entry is the conjunctiva, 3- to 5-mm whitish-yellow granulation on
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 2!Hi0 Barton•llosis: cat-scratch dis••• with primary IHion Erythematous nodule
of the cheek of a 9-year-<lld girl at the site of cat
scratch. Diagnosis was made on the histologic
findings of the excised specimen.
palpebral conjunctiva associated with tender
preauricular and!or cervical lymphadenopathy
(Parinaud oculoglandular syndrome).
Uncommonly urticaria, ttanaient maculopapular eruption. or erythema nodorum.
REGIONAL LYMPHAPf.NOI'ImtY (Fig. 25·61)
Evident within 2 to 3 weeks after inoculation
in 90% of cases; primary le.sion, ifpresent. may
have n:solved by the time lymphadenopathy
oc:curs. Nodes are often soUtaty, moderately
tender, and freely movable. Involved lymph
nodes: epitrochlear, u:illary. pectoral. and cervicaL Nodes may suppurate. U.sually re.solm:l
within 3 months. Generalized lymphadenopathy or Involvement of the lymph nodes of more
than one region is unusual
DIFFERENTIAL DIAGNOSIS
Chancriform syndrome. Suppurative bacterial
lymphadenitis, NTM infection, sporotrichosls,
and tularemia.
ontERCAT-ASSOCIATEDINFECTIONS Bite infections caused by P. multocida and C. canimorsus,
FIGURE 25-61 Bartonellosis: c:at-scntch
disuse with u:lll•ry •denopathy Acute, very
tender, axillary lymphadenopathy in a child; cat
scratches were present on the dorsum of the ipsilateral hand. (Used with permission from Howard
Heller, MD.)
sporotrichosis; Microsporum canis dermatophytosis.
DIAGNOSIS
Sugested by regional lymphadenopathy
developing am' 2 to 3 weeks in an individual
with cat comact and a primary lesion at the
site of contact; co:n1i.rm.ed by identification of
B. henselae from tlssue or serodiagnosis.
COURSE
Sel£-Umiting. usually within 1 to 2 months.
Uncommonly, prolonged morbidity with
persistent high fever, suppurative lymphadenitis, and severe systemic symptoms. May
be confused with lymphoma. Uncommonly.
cat-saatch encephalopathy occurs. Antibiotic
therapy has not bun very effective in altering
the course of the lnfectlon.
TREATMENT
In the lmmunocompromised, az.l.thromycin;
in immunocompetent. spontaneous resolution
occurs.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
BACILLARY ANGIOMATOSIS (BA) IC0-10:A44.8
• Etiology. B. henselae, B. qulntona. Both cause cutaneous angiomas. B. qulnrana causes subcutaneous
nodules and lytic bone lesion.
• Demography. Occurs in advanced HIV disease. 1ncidence decreased with antiretroviral therapy (ART)
and prophylaxis of opportunistic infections.
• Risk Factors. B. henseloe: contact with cats and/or cat fleas (C fe/is). B. quintana: row income, hom~
lessness. body louse fP. humonls corpoTis) Infestation.
CLINICAL MANIFESTAnON
Papules or nodules resembling angiomtl.5
(bright red. violaceous. or sld:n. colored)
(Fig. 25-62); up to 2 to 3 em. in diameter;
usually situated in dermis with thinning or
erosion of overlying epidermis. Larger lesions
may ulcerate. Subcutaneous nodules. 1 to 2 em
in diameter, resembling cysts. Uncommonly.
abscess !ormation. Papules/nodules .range from
solitary lesions to>100. Firm. nonblanchlng.
DtSTRJBimON Any site, but palms and soles are
usually spared. Occasionally. lesions occur at
the site ofa cat saatch. A solitary lesion may
pn:sent as dactyUtis.
MUCOUS MEMBRANES Angioma-like lesions of
lips and oral mucosa. Laryngeal involvement
with obstruction.
SYSTEMIC FINDINGS Infection may spread hematogenously or via lymphatics to be<:ome systemic. commonly involving the liver (pello&is
hepatitis) and spleen. Lesions may also occur in
infection c:au&e& significant morbidity and
mortality. With dfective antimicrobial therapy
(erythromycin 18 treatment of choice; altema-
tively. doxycycline),lesions resolve within 1 to
2 weeks. As with other .Infections occurring 1n
HJV disease, relapse may occur and require
lifclong secondary prophylaxis.
the heart. bone marrow; lymph nodes, muscles.
soft tissues. and CNS.
DIFFERENTIAL DIAGNOSIS
Kaposi sarcoma, pyogenic granuloma. and
cheJTY angioma.
DIAGNOSIS
Clinical findings confirmed by demonstration
of Barltmella bacilli on the Warthin-Starry
allver stain oflesional biopsy spec:lmc:n. culture.
or antibody studies.
COURSE AND TREATMENT
Rarely seen in pe.rsons with HIV disease successfully treated with ART. Untreated systeml.c
FIGURE 25·62 Bartonellosis: bacillar, anglomatosb 3- to 5-mm cherry hemangioma-like
papules and a larger pyogenic granuloma-like
nodule on the shin of a male with advanced HIV
disease. Sutx:utaneous nodular lesions were also
present. Lesion promptly resolved with oral erythromycin, but required secondary prophylaxis for
re<:urrent lesions.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
TULAREMIA ICD-10:A21
• Etiology: Franc/sella tularensls. types A and B. After Inoculation Into skin, mucous membrane, lung
(inhalation), or Gl tract F. tularensis reproduces and spreads through lymphatic channels to the
lymph nodes and bloodstream.
• Transmission. Bite ofinsect vector (ticks, deer flies, body lice, or other arthropods). Handling flesh of
infected animals; inoculation of conjunctiva; ingestion of infected food; inhalation. Most US cases
occur In June to September when arthropod transmission Is most common.
• Animal Reservoir. Rabbits, hares, muskrats, squirrels, voles, and beavers.
• lnddence. Rare; <200 cases reported in the United States per year; underdiagnosed, underreported.
CLINICAL MANIFESTAnON
COURSE
About 48 h after inoculation. pruritic papule
develops at the site of trauma or insect bite
followed by enlargement of the regional lymph
Untreated, mortality rate for ulcerogl.andular
form is 596; 1% If therapy is ln!tiated promptly.
nodes. Fever to 41•c.
Inoculation site: Erythematous tender
papule evolving to a vesl.copustule, enlarging to
crusted ulcer with raised, sharply demarcated
margins (96 h) (Fig. 2S.63). Depressed center
that is often covered by a black eschar (chancriform). Primary lesion on the finger or hand at
the site of trauma or insect b:lte; groin or axilla
after tick bite.
ontER CIITANEOUS FINDINGS Exanthem may
occur after bacteremia on the trunk and
e:rtremit.ies with macules,. papules, and
petechiae. Erythema multiforme. Erythema
nodoswn.
CONJUNCTIVAE In oculoglandular tulatemJ.a.
F. tularensts is inoculated Into conjunctiva,
causing a purulent conjunctivitis with pain,
edema, and congestion. Small yellow nodules
occur on conjunctivae and ulcerate.
REGIONAL LYMPH NODES As the ulcer develops,
nodes enlarge and become t:ende.t; Le., chancriform syndrome (Fig. 25-63). If untreated, they
become suppurating buboes.
TREATMENT
Streptomycin Is the treatment ofchoice. Also
gentamycin, chloramphenicol. dorycydine, and
ciprofloxa.cin.
DIFFERENTIAL DIAGNOSIS
Acute cutQneous ulcer; Furuncle, paronychia.
anthrax. P. multocida infection, sporotrichosis. and M. mo.rinum infection. Clumcriform
syndrome: Herpes simplex virus lymphade:nitis,
plague, and cat-scratch disease.
DIAGNOSIS
CUnical diagnosis in a patient with chancriform syndrome with appropriate animal or
insect exposure.
FIGURE 25-63 Tularemia: primary lesion and
regfonallldenopathy A crusted ulcer at the site
of inoculation is seen on the dorsum of the left
ring finger with associated axillary lymph node
enlargement (chancriform syndrome). The Infection occurred after the patient killed and skinned
a rabbit.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
CUTANEOUS PSEUDOMONAS AERUGINOSA INFECTIONS
• P. aeruginosa: Nonfastidious, motile; produce pyocyanin and pyoverdine, pigments that cause yellow
to dark green to bluish color.
• Ecology. Widespread In nature, inhabiting water, soil, plants, and animals, preferring moist environments. In healthy individuals, carriage rate of skin is low; pseudomonas is minimally invasive.
• Transmission. Most invasive infections are hospital acquired. Entry sites wounds, ulcers, and thermal
burns; foreign bodies (IV or urinary catheter), and aspiration/aerosolization into respiratory tract.
CLINICAL MANIFESTATIONS
P. aeruginosa grows as a bio:film
on ventral or dorsal surface of abnormal
nails. Onycholytic nails, e.g., psoriasis and
onychomycosis, create a moist environment
for Pseudomonas to colonize. Less commonly,
Pseudomonas can colonize the dorsal surface of
fingernails associated with chronic paronychia.
The onycholytic nail plate can be trimmed to
eliminate the abnormal space.
INTERTRIGO Gram-negative webspace intertrigo presents as macerated and eroded skin
on interdigital toes. Pseudomonas is the most
common cause. Usually occurs in the setting
of hyperhidrosis and hydration of stratum corneum. Interdigital tinea pedis and erythrasma
may also be present Superficial intertrigo can
progress with interdigital ulceration and softtissue infection.
EXTERNAL OTITIS Swimmers ear. Moist environment of external auditory canal provides
medium for superficial infection, presenting
as pruritus, pain, and discharge; usually selflimited. Malignant external otitis occurs in
elderly diabetic patients most commonly; may
progress to deeper invasive infection.
HOT TUB FOLLICULITIS P. aeruginosa can infect
multiple hair follicles during exposure in
GREEN NAILS
hot tubs or physiotherapy pools, presenting
as multiple follicular pustules on the trunk
(Fig. 25-18). Infection is self-limited.
COLONIZATION OF WOUNDS Thermal burns, stasis
ulcers, pressure ulcers, and surgical wounds are
more commonly colonized with Pseudomonas
(Fig. 25-39) after prior treatment of S. aureus
with systemic antibiotics, diabetes, and other
host defense defects. Soft-tissue infection can
occur in colonized wounds.
SOFT-TISSUE INFECTION AND E. GANGRENOSUM
Superficial infection can progress to cellulitis.
E. g'mgrenosum is a necrotizing soft-tissue
infection associated with blood vessel invasion, septic vasculitis, vascular occlusion, and
necrosis (Fig. 25-32).
PSEUDOMONAL BACTEREMIA Hematogenous
dissemination of P. aeruginosa can seed the
dermis, resulting in multiple tender subcutaneous nodules.
DIAGNOSIS
Clinical suspicion confirmed by culture of skin
lesion.
TREATMENT
Antibiotic according sensitivity of microbes.
Surgical debridement.
MYCOBACTERIAL INFECTIONS
Mycobacteria are rod-shaped or coccobacilli acid-fast bacilli (AFB). More than 120 species identified.
Relatively few associated with human disease:
•
•
•
•
Hansen disease (leprosy).
Tuberculosis.
Non Tuberculous Mycobacterium (NTM) infections.
Buruli or Bairnsdale ulcer disease is the third most common mycobacterial disease globally.
PART Ill
DISEASES CAUSED BY MICROBIAL AGENTS
HANSEN DISEASE (LEPROSY) ICD-1 0: A30
•
•
•
•
Etiology. Mycobacterium /eprae.
Chronic granulomatous disease principally acquired during childhood or young adulthood.
Sites of infection. Skin, peripheral nervous system, upper respiratory tract, eyes, and testes.
Clinical manifestations, natural history, and prognosis of leprosy are related to the host response: Various types of leprosy (tu bercu laid, lepromatous, etc.) represent the spectra ofthe host's immunologic
response (cell-mediated immunity).
Source: http//www.cdc.gov/nczved/divisions/dfbmd/diseases/hansens_disease/technical.html/.
CLASSIFICATION
Based on clinical, immunologic, and bacteriologic findings.
• Thben:uloid (TL): Localized skin involvement
and/or peripheral nerve involvement; few
organisms.
• Lepromatous (LL): Generalized involvement
including skin, upper respiratory mucous
membrane, reticuloendothelial system,
adrenal glands, and testes; many bacilli.
• Borderline (or ·dimorphic·) (BL): Has
features of both TI. and LL. Usually many
bacilli present, varied skin lesions: macules,
plaques; progresses to TL or regresses to LL.
• Indeterminate forms.
• 'fransitional forms: See "Pathogenesis; in the
following discussion.
ETIOLOGY AND EPIDEMIOLOGY
Mycobacterium leprae: Obligate intracellular
acid-fast bacillus; reproduces optimally at 27
to 30"C. Organism cannot be cultured in vitro.
Infects skin and cutaneous nerves (Schwann
cell basal lamina). In untreated patients, only
1% of organisms are viable. Grows best in
cooler tissues (skin, peripheral nerves, anterior
chamber of eye, upper respiratory tract, and
testes), sparing warmer areas of the skin (axilla,
groin, scalp, and mid-line of back). Humans are
main reservoirs of M. leprae. Wild armadillos
(southern United States) as well as mangabey monkeys and chimpanzees are naturally
infected with M. leprae; armadillos can develop
lepromatous lesions.
Incidence rate peaks at 10 to 20 years; prevalence peaks at 30 to 50 years. More common
in males than in females. Inverse relationship
between skin color and severity of disease; in
black Africans, susceptibility is high, but there
is predominance of milder forms of the disease,
ie., TI. vis-a-vis LL.
TRANSMISSION Uncertain. Likely spread from
person to person in respiratory droplets.
Disease of the developing
world. In 2010,228,474 new cases detected
worldwide; 294 in the United States. The vast
majority were from Angola, Bangladesh, Brazil,
China, Congo, Ethiopia, Indonesia, Madagascar, Mozambique, Myanmar, Nepal, Nigeria,
Phillipines, Sudan, and Sri Lanka. Risk groups:
Close contact with patients with untreated,
active, predominantly multibacillary disease,
and persons living in countries with highly
endemic disease. Most individuals have natural
immunity and do not develop disease.
PATHOGENESIS Clinical spectrum of leprosy
depends exclusively on variable limitations
in host's capability to develop effective cellmediated immunity toM. leprae. Organism
is capable of invading and multiplying in
peripheral nerves and infecting and surviving
in endothelial and phagocytic cells in many
organs. Subclinical infection with leprosy is
common among residents in endemic areas.
Clinical expression ofleprosy is development of
a granuloma; patient may develop a "reactional
state; which may occur in some form in >50%
of certain groups of patients.
DEMOGRAPHY
GRANULOMATOUS SPECTRUM OF LEPROSY
• High-resistance tuberculoid response (TT).
• Low- or absent-resistance lepromatous pole
(LL).
• Dimorphic or borderline region (BB).
• 1Wo intermediary regions.
• Borderline lepromatous (BL).
• Borderline tuberculoid (BT).
In order of decreasing resistance, the spectrum
is TT, BT, BB, BL, and LL.
IMMUNOLOGIC RESPONSES Immune responses
toM. leprae can produce several types of reactions associated with a sudden change in the
clinical status.
Lepra Type 1 Reactions. Acute or insidious
tenderness and pain along affected nerve(s),
associated with loss of function.
Lepra Type 2 Reactions. Erythema nodosum
leprosum (ENL). Seen in half ofLL patients,
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
w;ually occurring ~ initiation ofantilepro-
severe pain, and contractures of the hands and
matou& therapy, generally within the first
2 years of treatment. Massive in11ammatl.on
feet.
with erythema nodosum-llke lesions.
Luao Reaction. Individuals with diffuse l l
develop shallow, large polygonal sloughing
ulcerations on the legs. The reaction appears
to be either a varia.D.t of ENL or se<:ondary to
arteriolar occlusion.
CLINICAL MANIFESTAnON
Incubation period is 2 to 40 years (moot
comm.oDly S to 7 years). Onset is iDsidiow;
and paJ.D.lesa; first affeds peripheral nervous
S}'3tem with persistent or recurrent painful
parestheslas and numbness without any vislble
clinical signs. At this staF· there may be transient macular skin eruptions; blister, but lack
of awareness of tnuma. Neural involvement
leads to muscle weakness. muscle atrophy,
FIGURE 25-64 Leprosy:
tt.~bem~lold type
Well-
defined, hypopigmented,
slightly scaling, anesthetic
macules and plaques on the
posterior trunk.
Few well-defined
hypoptgmented hypesthetic macules (Fig. 25-64)
with raised edps and varyi.D.g in size from a few
TUBERCULOID WROSY (TT, BT)
millimeters to very large lesions covering the
entire trunk Erythematous or purple border
and hypopigmc::nted center. Sharply defi.D.ed,
raised; often annular; enlatge peripherally.
Central area becomes atrophic or depressed.
Advanced lesions are anesthetic::. devoid ofskin
appendap (sweat glands or hair follicles). Any
site including the face. IT: Le.sions may resolve
spontaneously; not associated with lepra reactions. BT: Does not heal spontaneoualy; type 1
lepra reactions ma;y occur.
Nerve Involvement May be a thickened nerve
on the edge of the lesion; large peripheral nerve
enlargement frequent (ulnar, posterior auricular, pcro:neal, and posterior tibial nerves). Skin
involvement is absent In neural leprosy. Nerve
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 2H5 Leprosy: borderllne-tJpe A 26-year-old Vietnamese male. (A) Well-demarcated, infiltrated, erythematous plaques on the face. (8) Identical red plaques on the lower back.
involvement is associated with hypesthesia (pinprick, temperature, or vibration) and myopathy.
BOIIDEALINEIB WROSY Lesions are intermediate between 1uberculoid and lepromatous and
are composed of maculea, papulea. and plaques
(Fig. 25-65). Anesthesia and decreased sweating are prominent In the lesions.
L£PROMM'OU$ LEPROSY (U.. BIJ Skin-colored
or slightly erythematous papules or nodules. LesioDS eularge; new lesions occur and
coalesce. Later, symmetr:lcally distributed
nodules, raised plaquea. dJ1fuse dermal in1iltrate, which on the face results In loss of halt
(lateral ~rows and eyclashes) and leonine
facies (lion's face; Pig. 2546). Diffu.se lepromatosis., occurring in western Mexico,. Can"bbean,
presents as dJ1fuse dermal in1iltration and
thickened dermis. Bllaterall:y symmetric involving the earlobes. face. arms. and buttoclcs, or
le.s.s frequently the trunk and lower atremities.
Tongue: Nodules, plaques, or fissures.
Nerve Involvement: More exteDSive than in TT.
Other Involvement: Upper respiratory tract.
anterior chamber of eye. and testes.
Reactfonal States
Immunologically mediated inflammatory
state5, occurring spontaneously or after initiation of therapy.
Lepra Type 1 ~tions: Skin lesions become
acutely inflamed. associated with edema and
pain; may ulcerate. Edema is most sevue on
the face, hands. and feet
Lepra 'I}'pe 2 Reactions (ENL): Present as
painful red skin nodules arising superficially
and deeply. In contrast the tru erythema nodoswn lesions form abscesses or ulcerate; they
occur most commonly on the face and extensor
limbs.
Ludo Reaction: Occurs in patients from
Meldco or Caribbean with dJ1fuse ll. Presents
as irregularly shaped erythematous plaques;
lesions may resolve spontaneously or undergo
necrosis with ulceration.
General Findings
Extremities: Sensory neuropathy. plantar ulcers,
secondary infection; ulnar and peroneal palstes
(Fig. 25-67), Charcot joints. Squamous cell
carcinoma can arise in chronic foot ulcers
(F.ig. 11-13).
Nose: Chronic nasal congestion, epistaxis;
destruction ofcartilage with saddle-nose deformity (Fig. 2547).
Byes: Cranial nerve palsies, lagophthalmos,
and corneal insensitivity. In LL. anterior chamber can be invaded with uveitis,. glaucoma, and
cataract fo.nuation. Corneal damage can occur
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 2!Hi6 Diffuse skin Infiltration, multiple nodular lesions, and sensory loss are the key hallmarks
of lepromatous leprosy (LL). This patient presented lesions on the upper part of the thorax, forehead,
ears, nose, lips, perilabial, and mentonian regions, as well as lax skin of the malar and palpebral superior
regions, with muscle force impairment on the left side. Superciliary and ciliary madarosis were also present. Ulnar and tibial posterior nerves were enlarged. A Zlehi-Neelsen stained skin smear had a 6+ bacterial index for acid-fast bacilli in clumps, and ELISA titration for anti-PGL-1 lgM was 3.445 (cutoff 0.295). The
12-month World Health Organization multidrug therapy regimen and prednisone were prescribed, with
significant improvement LL is the anergic form of leprosy; it generates an exacerbated but inefficient
humoral immune response, leading to highly infectious patients. Mycosis fungoides, neurofibromatosis,
sarcoidosis, amyloidosis, syphilis, anergic leishmaniasis, and lobomycosls are among diseases In the differential diagnosis. (Used with permission from Claudio G. Salgado, MD, PhD and Josaf.1 G. Barreto, PhD, Parti
Federal University, Brazil.)
secondary to trl.chiasls and sensory neuropathy,
secondary infection, and muscle paralysis.
Testes: May be involved in LL with resultant
hypogonadism.
Compllcatlo.ns of Leprosy: SqU4mous ci11
carcinoma can arise in chronic neurotrophic
ulcers on the lower extremities (see Fig. 11-13).
The tumors are usually low-grade malignancies
but can metastasize to regional lymph nodes
and cause death. Secondary amyloidosis with
hepatic and renal abnormalities.
DIFFERENTIAL DIAGNOSIS
Hypopigmented lesions with granulomas.
Sarcoidosis, leishmaniasis, NTM infection,
lymphoma. syphilis, and granuloma annulare.
I.ABORATORY EXAMINATIONS
A small skin incision is made;
the site is then scraped to obtain tissue tlu.ld
from which a smear is made and examined after
SUT-SIIIN SMEARS
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
Measure IgM antibodies to phenolic
glycolipid-! (PGL-1).
DERMATOPATHOLOGY Tl shows epit:helloid
cell granulomas forming around dermal
nerves; AFB are sparse or absent. LL shows an
atensive cellular infiltrate separated from the
epidermis by a narrow zone of normal collagen.
Skin appendages are destroyed Macrophages
are 1illed with M. leprae, having abundant
foamy or vacuolated cytoplasm (lepra cells or
Vudl.ow cells).
SEROLOGY
DIAGNOSIS
Made if one or more of the cardinal findings
are detected: Patient from endemic area, skin
lesions characteristic of leprosy with diminished or loss of sensation. enlatged peripheral
nerves. finding ofM. leprae in skin or, less
commonly, other sites.
COURSE
FIGURE 25-67 Leprosy: lepromatous type
A 6<ryear-old Vietnamese female with treated
advanced disease. Ulnar palsy, loss of digits on
right hand, and saddle-nose deformity associated
with loss of nasal cartilage are seen.
Ziehl-Neelsen staining. Specim.e.rul are usually
obtained from multiple sites (both earlobes,
elbows, knees. and active lesions). High Bacterlal
Index (81) is seen in U..low/negative BI can be
seen in paucibacillary ca.se.s. treated cases. and
cues examined by an inexperienced tfdmician.
CUL1VRE M. leprae has not been cultured in
vitro; however, it does grow when inoculated
brto the mouse foot pad. Routine bacterial
cullUl'e.S to rule out seoondary infection.
PCR M. leprae DNA detected by this technique makes the diagnosis of early paucibacillary leprosy and identifies M. ll:prae after
therapy.
After the first few years of drug therapy. the
molt difficult problem is management of the
changes secondary to neurologic deficits;
contractures and trophic changes in the hands
and feet Uncommonly, secondary amyloidosis with renal failure can complicate longstanding leprosy. Lepra type 1 reactions lart
2 to 4 months in individuals with BT and up to
9 months in those with BL. Lepra type 2 reactions (ENL) occur in 5096 of individuals with
LL and 25% of those with BL within the first 2
years of treatment ENL may be complicated by
uveitis, dactyiitis, arthritis, neuritis, lymphadenitis, myositis, and orchitis. Lucio reaction
occurs secondary to vasculitis with subsequent
infarction.
TREATMENT
General principles of treatment:
• Thbetculold: Dapsone plus rifampin.
• Lepromatous: Dapsone plus clofazimJne plus
rlfampin.
• Eradicate infection with antilepromatous
therapy.
• Prevent and 17eat reactions (prednisone or
thalidomide).
• Reduce the risk of nerve damage.
• Educate patient to deal with neuropathy and
anesthesia.
• Treat complications of nerve damage.
• Rehabilitate patient into society.
Management involves a broad multidisciplinary approach including orthopedic swgery,
podiatry, ophthalmology, and physical therapy.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
CUTANEOUS TUBERCULOSIS ICD-1 0: A 18.4
• Etiology. Mycobacterium tuberculosis complex. Commonly infects lungs; rarely skin.
• Transmission. Airborne spread of droplet nuclei from those with infectious pulmonarylb to lungs.
• Cutaneous Infection. Exogenous inoculation into skin. Direct extension from deeper tissues such as
joint; lymphatic spread to skin; hematogenous spread to skin.
CLASSIFICATION
EXOGENOUS INOCULATION TO SKIN Primary
inoculation tuberculosis {PIT), ie., tuberculous
chancre: Occurs at inoculated site in nonimmune host. Tuberculosis verrucosa cutis (TVC):
Occurs at inoculated site in individual with
prior tuberculosis infection.
Tuberculosis may also result from bacille
Calmette-Guerin (BCG) immunization.
ENDOGENOUS SPREAD TO SKIN Lymphatics,
hematogenous, and bodily fluids (sputum,
feces, or urine). Lupus vulgaris. Scrofuloderma.
Metastatic tuberculosis abscess. Acute miliary
tuberculosis. Orificial tuberculosis.
PATHOGENESIS
Type of clinical lesion depends on route of
cutaneous inoculation and immunologic status
of the host
• Cutaneous inoculation results in a
tuberculous chancre in the nonimmune host
and TVC in the immune host
• Direct extension from underlying
tuberculous infection, i.e., lymphadenitis or
tuberculosis ofbones and joints, results in
scrofuloderma.
• Lymphatic spread to skin results in lupus
vulgaris.
• Hematogenous dissemination results in
acute miliary tuberculosis, lupus vulgaris, or
metastatic tuberculosis abscess.
• Autoinoculation from body fluids such as
sputum, urine, and feces results in orificial
tuberculosis.
Globally, the incidence of cutaneous tuberculosis is increasing, associated with HIV disease. Problem of multidrug resistance (MDR) is
also common in persons with HIV disease.
CLINICAL MANIFESTATION
PIT Initially, papule occurs at the inoculation site 2 to 4 weeks after inoculation. Lesion
enlarges to a painless ulcer, tuberculous chancre
(Fig. 25-68) with shallow granular base. Older
ulcers become indurated with thick crusts.
Deeper inoculation results in subcutaneous
abscess. Most common on exposed skin at sites
of minor injuries. Oral ulcers on gingiva or
palate occur after ingestion of bovine bacilli in
nonpasteurized milk. Regional lymphadenopathy occurs several weeks after appearance of the
ulcer (chancriform syndrome) (Fig. 25-68).
TVC Initial papule with violaceous halo.
Evolves to hyperkeratotic, warty, or firm plaque
(Fig. 25-69). Clefts and fissures occur from
which pus and keratinous material can be
expressed. Border often irregular. Lesions
are usually single, but multiple lesions occur.
Most commonly on the dorsolateral hands and
fingers. In children, on the lower extremities,
knees. No lymphadenopathy.
LUPUS VULGARIS Initial papule ill-defined and
soft, evolves into well-defined, irregular plaque
(Fig. 25-70). Reddish-brown. Diascopy (glass
slide pressed against skin) shows an "apple jelly'"
color (i.e., orange-tan). Lesions are characteristically soft and friable. Surface is initially
smooth or slightly scaly but may become
hyperkeratotic. Hypertrophic forms result in
soft tumorous nodules. Ulcerative forms present as punched-out, often serpiginous ulcers
surrounded by soft, brownish infiltrate. Usually
solitary, but several sites may occur. Most
lesions on the head and neck, most often on
nose, ears, or scalp. Lesions on ears or nose can
result in destruction of underlying cartilage.
Scarring is prominent. Characteristically new
brownish infiltrates occur within atrophic scars.
SCROFULODERMA Firm subcutaneous nodule
that initially is freely movable; lesion then
becomes doughy and evolves into irregular,
deep-seated node or plaque that liquefies and
perforates (Fig. 25-71). Ulcers and irregular
sinuses, usually of linear or serpiginous shape,
discharge pus or caseous material Edges are
undermined, inverted, with dissecting subcutaneous pockets alternating with soft, fluctuating
infiltrates and bridging scars. Most often occurs
in the parotid, submandibular, and supraclavicular regions; lateral neck; scrofuloderma
most often results from contiguous spread from
affected lymph nodes or tuberculous bones
(phalanges, sternum, or ribs) or joints.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE as-a Primary lnoa&lation tlllbem~losfs A large, ulcerated nodule at the site of Mycobacterium tuberculosis inoculation on the right thigh associated with inguinal lymphadenopathy. The erythematous papules on the left forearm occurred at the site of tuberculin testing.
FIGURE 25-8 Tubii'CUIosls verrucosa cutis A
~ear~ld male with warty
and crusted plaques on the
dorsum of the hand for
6 months. (Reproduced with
permission from Sethi A.
Tuberculosis and infections
with atypical Mycobacteria. In: Goldsmith LA, Katz
Sl, Gilchrest BA. et al, eds.
FltzpotrlcKs Dermatology In
General Medicine. 8th ed. New
York, NY: McGraw-Hill; 2012.)
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
METASTATIC TUBERCULOSIS ABSCESS Subcutaneous absce.ss, nontender, "cold." md fluctuant.
Coalescing with overlying skin, breaking
down and forming fistulas and ulcers. Slngle
or multiple lesions. often at sites of previous
trauma.
ACUTE.MIUARYTUBEACULDSIS Exanthem. Diss~m~inated lesions are minute macule& and pap-
ules or purpuric lesions. Sometimes vesicular
and crusted. Removal of crust reveals umbilication. Dl.sseminated on all parts of the body.
particularly the trunk.
ORIFICIAL TUBERCULOSIS Small yellowish nodule
on mu.co&a breaks down to form painful
ctrtular or irregular ulcer (Fig. 25-72) with
undermJned borde.rs. Surrounding mucosa
swoll.e.n. edematous. and inflamed. Since or11i-
cal tuberculosis results from autoinoculation of
mycobacteria from progressive tuberculosis of
internal orgam. it i& usually fuwtd on the oral.
pharyngeal (pulmonary tuberculosis), vulvar
(genitourinary tuberculosls), and anal (intestinal tuberculosiB) mucous membranes. Lesions
may be single or multiple. and in the mouth
most often occur on the tongue, soft and hard
palate, or lips.
FIGURE 25-70 Lupus vulgaris Reddish-brown
plaque, which on diascopy exhibits the diagnostic yellow-brown apple-jelly color. Note nodular
infiltration of the earlobe, scaling of the helix. and
atrophic scarring In the center of the plaque.
FIGURE 25-71 Scrofuloderma:
lataral c"-tt wall Two ulcers on
the chest wall and axilla are associated with underlying sinus tracts.
DIAGNOSIS
Oi:nical. findings. tuberculin skin testing
(Fig. 25-73), dermatopathology, confirmed by
isolation ofM. tuberculosis on culture or by
PCR.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25·72 Ortftc:lll
tuberculosis: lips A large,
very painful ulcer on the lips
of this patient with advanced
cavitary pulmonary tuberculosis.
COURSE
The course of cutaneous tubercul.o&i& is quite
variable, depending on the type of cutaneous
iDCectJ.on. amount ofinoculum. extent ofatracutaneous infection, age of the patient. immune
status. and therapy.
TREATMENT
ODly PIT and TVC are limited to the skin. .All
other patterns of cutaneous tubercul.osJs are
associated with systemic iDCedio.n that has disseminated secondarily to skin. AJ such. th.e.rapy
should be aimed at achieving a cure, avoiding
relapse, and preventing emergence of drugresistant mutants.
ANTITUBERCULOUS THERAPY Prolonged antituberculous the.rapy with at least two drugs is
indicated fur all cases of CTb except fur TVC
that can be excised.
• Standard antituberculous th.e.rapy:
FIGURE 25-7.1 Purlfled prot.In derlmlve or
Mantoux test: positive test A 31-year-old Taiwanese female with psoriasis, with a negative skin
test 1 year previously, was retested prior to beginning etanercept She had become infected while
visiting her father, who had pulmonary tuberculosis, in Taiwan. A red plaque with surrounding
erythema Is seen at the test site.
• Isoniazid (5 mgllcg daily) •
• Rifampin (600 mglkg daily).
• Supplemented in initial phases with:
• Ethambutol (25 mglkg daily) and/or
• Streptomycin (10 to 15 .m.gl.kg daily) and/or
• Pyrazinamide (15 to 30 mgllcg dally).
Isoniazid and rlfampin fur at least 9 months;
c;an be shortened to 6 months if four drugs are
given during the first 2 months.
MULTIDRIIG RESISTANT (MDR) TB Incidence is
increasing.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
NONTUBERCULOUS MYCOBACTERIAL INFECTIONS ICD-1 0: A31.1
• Nontuberculous mycobacteria (NTM) defined as mycobacteria other than M. tuberculosis complex
and M.leprae. Occur naturally in the environment: M. marinum, M. u/cerans, M. fortuitum complex,
M. abscessus, M. avium-intrace//ulare, and M. haemophilum.
• Infection. Capable of causing primary infections in otherwise healthy individuals and more serious
infection with host defense defects such as;
• Immunocompetent individuals: primary cutaneous infections at sites of inoculation. Nodules,
lymphocutaneous lesions, or nodular lymphangitis.
• lmmunocompromised host disseminated mucosal and cutaneous lesions.
• Diagnosis. Detection of mycobacteria histochemically or by culture on specific media. New
molecular techniques based on DNA amplification accelerate diagnosis, identify common sources of
infection, and revea I new types of NTM.
• Treatment. Clarithromycin, rifampicin, fluoroquinolones, and minocycline.
MYCOBACTERIUM MARINUM INFECTION
• Etiology. M. marinum, an environmental nontuberculous mycobacterium. Infection usually follows
traumatic Inoculation in aqueous environment, i.e., fish tank, unchlorinated water.
• Demography. Healthy adults. More invasive or disseminated infections with host defense defects.
CLINICAL MANIFESTATION
DIAGNOSIS
INCUBATION PERIOD Variable: Usually weeks
to months after inoculation. Lesions may be
asymptomatic or tender.
INOCULATION SITE Papule(s) enlarging to
inflammatory (Fig. 25-74), red to red-brown
nodule or plaque 1 to 4 ern in size on the
dominant hand. Surface of lesions may be
hyperkeratotic or verrucous (Fig. 25-75).
May become ulcerated with superficial crust,
granulation tissue base, ± serosanguineous, or
purulent discharge. In some cases, small satellite papules and draining sinuses may develop.
Usually solitary, over bony prominence. More
extensive soft-tissue infection may occur with
host defense defects. Atrophic scarring follows
spontaneous regression or successful therapy.
NODULAR LYMPHANGITIS Deep-seated nodules
in a linear configuration on hand and forearm
exhibit lyrnphocutaneous spread (Fig. 25-76).
Boggy inflammatory reaction may mimic
bursitis, synovitis, or arthritis about the elbow,
wrist, or interphalangeal joints. Tenosynovitis,
septic arthritis, and osteomyelitis. Host defense
defects.
DISSEMINATED INFECTION Rare. May occur with
host defense defects. Regional lymphadenopathy uncommon.
History of trauma in an aqueous environment,
clinical findings, confirmed by isolation of
M. marinum on culture. M. marinum grows
at 32•c (but not at 37•q in 2 to 4 weeks.
Early lesions yield numerous colonies. Lesions
3 months or older generally yield few colonies.
LABORATORY FINDINGS
LESIONAL BIOPSY Acid-fast stain demonstrates
M. marinum only in approximately 50% of
cases.
COURSE
Usually self-limited but can remain active for
a prolonged period. Single papulonodular
lesions resolve spontaneously within 3 months
to 3 years; nodular lymphangitis can persist for
years. With host defense defects, more extensive deep infection can occur.
TREATMENT
Drug of first choice: Clarithromycin and either
rifam.pin or ethambutol for 1 to 2 months after
lesions have resolved (3 to 4 months). Minceyeline alone may be effective.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25·74 M.mt1rlnum: lnoculatron sltelnfectlon on dMtfoot A 31-year-old male with painful
indurated plaque on the lateral dorsal foot The lesion arose at the site of a small blister 1 year ago while
in Afghanistan. Three previous biopsies and tissue cultures had been unsuccessful at making a diagnosis.
Mer intralesional injection of triamcinolone 1.5 mg/mL. acid-fast bacilli were identified in the biopsy specImen and M. marlnum Isolated on culture. He was successfully treated with four antimycobacterial agents.
FIGURE 25-75 M.mtltinum infection: verrucous plaque A red-violet. verrucous plaque on the dorsum of the right thumb of a fish tank hobblst at the site of an abrasion.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-76 M.mt~rinum: soft·tlssue Infection and l~phanghfs beginning on ftnger A
48-year~ld female with painful swelling of the right
middle finger for 4 months. She recalled cleaning
a fish tank several weeks before the distal digital
became red and tender. The flnger and hand
became progressively more inflamed and red nod·
ules appeared on the forearm. Slight enlargement
of axillary nodes was detected.
MYCOBACTERIUM ULCERANS INFECTION ICD-10: A31.1
• Synonyms: Buruli ulcer or Buruli ulcer disease in Africa. Bairnsdale or Daintree ulcer in Australia.
• Etiology. M. u/cerons. An environmental habitat for the organism has not been established. Incidence:
Third most common mycobacterial infection after tuberculosis and leprosy.
• Transmission. Inoculation probably via minor trauma occurring in wet, marshy, or swampy sites.
Bites of aquatic insects; M. ulcerons replicates in insect salivary glands; in endemic areas, 5 to 1096 of
aquatic insects have microbe in salivary gland.
• Demography. Occurs In >30 countries. Tropical regions of West Africa; Australia, Papua New Guinea;
Central Mexico.
• Pathogenesis. M. ulcerons produces polypeptide toxin (mycolactone), which suppresses immune
response to microbe.
CLINICAL MANIFESTATION
lncubation period apprwdmately 3 mon.tha.
The early nodule at the site of ttawna and subsequent ulceration are usually painless. Fever.
constitutional findings are usually absent
Painles.s subcutaneous swelling oa:w-s at the
site of inoculation. Papule(s), nodule(s), and
plaques are often overloob:d.. Les:lon enlarges
and ulcerates. The ulcer extench into the subcutaneous fat and ib margin is deeply undermined (Fig. 25-77). Uk:eratlo:ns may enlarge
to involve an entire enremity. Legs more commonly involved. sites of trauma. Any site may
be involved. Soft tissue and bony involvement
can occur• .AJi. ulcerations healed, scarring and
disabling deformities may occur. Osteomyelitis
may occur.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-77 M. ukfMJM: Bunlll ulcer A 15-year~ld Ugandan male with a huge ulcer with a
clean base and undermined margins extends into the subcutaneous tissue. (Used with permission from
Dr. ManfTed Dietrich.)
DIAGNOSIS
COURSE
Identification of microbe on culture or by PCR.
Because of delay in diagnosis and treatment.
lesions are often extensive. Ulcerations pe!Slst
fur months to years. Spontaneous healing
LABORATORY FINDINGS
DERMATOPATHOLOGY Necrosis originates in
interlobular septa ofsubcutis. Poor ln11ammatory response despite clusters ofextracellular
bacilli Granulation with giant cells but no caseation necrosis. AFB are alwaya demonstrable.
DIFFERENTIAL DIAGNOSIS
Sporotrichosis, nocardiosis, phaeohyphomyrosis. and aquamoua a:ll carcinoma.
occurs eventually in some patienfll; scarring,
conttactun: of the limb, and lymphedema.
Malnutrition and anemia delay heall:ng.
TREATMENT
ANTIMYCOBACTERIAL DRUG THERAPY Rifampicin and streptomycin combined with surgery.
Combination of rifampicin and ciprofloxacin
may be effective.
SURGERY Exciaion followed by grafting.
MYCOBACTERIUM FORTUITUM COMPLEX INFECTIONS ICD-10: A31.1
• Etiology. M. foltuitum, M. chelonoe. M. abscessus. Organisms are widely distributed in soil, dust and
water.
• Natural Reservoirs. Nosocomial environments: Municipal water supplies, moist areas in hospitals,
contaminated biological agents.
• Cutaneous infections account for 6096 of infections.
• Transmission. Inoculation via traumatic puncture wounds, percutaneous catheterizations or injections. Whirlpool footbaths in nail salons (M. fortuitum).
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
CLINICAL MANIFESTATION
LABORATORY EXAMINATIONS
Incubation period usually within 1 momh
DERMATOPATHOLOGY Necrosis is often present
(range 1 week to 2 years).
without caseation; AFB can be seen within
SKIN AND SOfT·TISSUE INFECT10NS Nodular
micro abscesses.
on lower legs following foot baths at nail
salons. Furunculosis (Fig. 25-78); shaving legs
COURSE
provides a portal ofentry. Wound infections
at surgical sites or sites of trauma. Multiple
nodules, abscessea. and auated ukers with host
defense defects (F.lp. 25-79 and 25-80).
lhe infection becomes chronic unless treated
with antl.mycobacterial therapy, ± surgical
debridement
TREATMENT
DIAGNOSIS
Lesional skin biopsy specimen or identify by
PCR.
FIGURE 25-78 M. fottultum
Infection A 45-year-old
female with erythematous tender nodules on the lower legs.
The lesions occurred several
weeks after a pedicure in a
foot care salon. Shaving of legs
may have facilitated the Infection. M. fortuitum was isolated
on culture oflesional biopsy
specimen.
Antimycobacterial chemotherapy. Surgical
debridement with delay00 closure for localized
infectioDS.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25·79 Multiple sites of soft-tissue
Infection lower leg: MycobGcterlum dlelonft
A 74-year-old female with chronic progressive lung
disease treated with prednisone and azathioprine
developed soft-tissue infections with multiple
abscesses on hands, lower legs, and feet. M. chelonae was isolated on culture of biopsy specimen.
FIGURE 25-80 M. c::IMioncrubsatss on L-dorsollltentl foot A 74-year-old
female treated with prednisone and azathioprine. M che/onae isolated on lesional
biopsy specimen.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
LYME DISEASE ICD-10: A69.2
• Etiologic agent: Borrelia spirochetes. Transmitted to humans by the bite of an infected Ixodes scapularis (US) or Ixodes ricinus (Europe) tick (deer tick).
• Stage 1early localized disease: Up to 30 days post tick bite. Erythematous plaque at th~ tick bite _site,
erythema migrans (EM), noted in 70 to 80% of cases. Acute illness syndrome (fever, chills, myalg1a,
headache, weakness, and photophobia). Lymphocytoma.
• Stage 2 early disseminated disease: Days to weeks post tick bite. Secondary lesions. Meningitis, cranial
neuritis (8%), radiculoneuritis (4%), peripheral neuritis. Carditis: AV nodal block (1 %). M1gratory musculoskeletal pain (33%), arthralgias.
• Stage 3late disseminated disease: Persistent infection, developing months or years later: Intermittent or
persistentarthritis, chronic encephalopathy or polyneuropathy, acrodermatitis chronica atrophicans (ACJ>V.
• Posttreatment Lyme disease syndrome: 10 to 20% of treated patients have persistent symptoms.
ETIOLOGY AND EPIDEMIOLOGY
ETIOLOGIC AGENT US: Borrelia burgdorferi,
recently Borrelia mayonii (Midwestern US).
Europe: B. afzelii, B. garinii
VECTOR Infected nymph Ixodes tick. Three
stages of tick development: larva, nymph, adult;
each stage requires blood meal. Preferred host
of adult Ixodes is the white-tailed deer.
SEASON In the Midwestern and Eastern United
States, most cases occur late May through early
autumn.
RISK FOR EXPOSURE Strongly associated with
prevalence of tick vectors and proportion of
those ticks that carry B. burgdorferi. In the
northeastern United States with endemic
disease, the infection rate of the nymph I.
scapularis tick with B. burgdorferi is 20 to 35%.
INCIDENCE LD is the most common vectorborne infection in the United States, with
25,359 cases reported in 2014. Cases reported
in all 50 states except Hawaii.
PATHOGENESIS After inoculation into the skin,
spirochetes replicate and migrate centrifugally,
producing the EM lesion, and invade vessels,
spreading hematogenously to other organs.
The spirochete has a particular trophism for
tissues of the skin, nervous system, and joints.
The organism persists in affected tissues during
all stages of the illness. The immune response
to the spirochete develops gradually. Specific
IgM antibodies peak between the third and
sixth weeks after disease onset. The specific
IgG response develops gradually over months.
Prointlammatory cytokines, 1NF-a, and IL-l
are produced in affected tissues.
CLINICAL MANIFESTATION
Incubation period for EM: 3 to 32 days after
tick bite. Cardiac manifestations 35 days
(3 weeks to >5 months after tick bite). Neurologic manifestations: Average 38 days (2 weeks
to months) after tick bite. Rheumatologic manifestations: 4 days to 2 years after bite.
PRODROME With disseminated infection (stage
2), malaise, fatigue, lethargy, headache, fever,
chills, stiff neck, arthralgia, myalgia, backache,
anorexia, sore throat, nausea, dysesthesia, vomiting, abdominal pain, and photophobia.
HISTORY Because of the small size (poppy seed)
of nymph tick, most patients are unaware
of tick bite; adults are sesame seed size. Bites
are asymptomatic. Removal of the nymphal
tick within 36 h of attachment may preclude
transmission. EM may be associated with
burning sensation, itching, or pain. Only 75%
of patients with Lyme disease exhibit EM. Joint
complaints more common in North America.
Neurologic involvement more common in
Europe. With persistent disease, chronic
fatigue.
STAGE 1 LOCALIZED INFECTION EM. Initial
erythematous macule or papule expanding centrifugally within days to form a lesion with a
distinct red border at the bite site (Fig. 25-81).
Maximum median diameter is 15 em. As EM
expands, site may remain uniformly erythematous, or several rings of varying shades of red
with concentric rings (targetoid or bulls eye
lesions). When occurring on the scalp, only a
linear streak may be evident on the face or neck
(Fig. 25-82). Multiple EM lesions are seen with
multiple bite sites. Most common sites: thigh,
groin, and axilla. Center may become indurated, vesicular, ecchymotic, or necrotic. As EM
evolves, postinflammatory hyperpigmentation,
transient alopecia, and desquamation may
occur.
Borrelial Lymphocytoma (BL). Mainly seen in
Europe. Usually arises at the site of tick bite.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
•r,them•
FIGURE 25-81 LJ!M borrellosls:
mlgrans (EM) on uppar
thigh (A). Attachment of Ixodes tick (B); oval erythema, slowly Increasing
(i.e., migrans). Will later resolve in the center, forminig a ring.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
FIGURE 25-82 Lyme borrellosls: erythema mfgr•ns on f•ce Serpiginous erythematous lesion on
the forehead represents the margin of a large lesion occurring on the scalp.
Some patients have a history of EM; others
may show concomitant EM located around or
near the lymphocytoma. Usually presents as a
solitary bluish-red nodule (Fig. 2.5-83). Sites of
predilection: Earlobe (children), nipple/areola
(adults), areola, scrotum; 3 to 5 em Jn diameter.
Other Cutanetms Findings. Malar rash. diffuse urticaria. and subcutaneous nodules
(panniculitis).
STAGE :t DISSEMINATED INFEC110N
Secondary
B. afuiU infection in Europe and Asia. More
common In elderly women. In1tially. diffuse or lcc:aliud violaceous erythema, usually
on one extremity, accompanied by mild to
prominent edema. Extends centrifugally over
several months to years. leaving central areas of
atrophy, veins. and subcutaneous tissue become
prominent (Fig. 25-84). Loc:alized fibromas
and plaques are seen as subcutaneous nodules
around the knees and elbows.
Lesions. Secondary le&ioDB resemble EM but
are smaller, migrate less. and lack central
induration and ma;y be sca.J.y. Lesions occur
at any site except the palms and soles. A few
or dozens oflesions may occur; can become
confluent.
STAGE .S PERSISTENT INFEaiON At:rr:ldermt:ittis
chronica atrophicans (ACA) associated with
DIFFERENTIAL DIAGNOSIS
ERYTHEMAMIGRANS Insect bite (annular ery-
thema caused by ticks, mosquitoes. or Hymenoptera), epidermal dermatophytoses. allergic
contact dermatitis,. herald patch of pityriasis
rosea, and :fixed drug eruption.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 25-83 Lyme borrellosls: IJmph~
cytoma cutis Solitary, red-purple nodule on
the ear.
FIGURE 2.5-84 Lyme bornllosla: acnchrmatltls
dlronica atrophicans: end stage Advanced atrophy of the epidermis and dermis with associated vio-
laceous erythema of legs and feet; the visibility of the
superficial veins is striking.
SECTION 25 BACTERIAL COLONIZATIONS AND INFECTIONS OF SKIN AND SOFT TISSUES
Lyme disease-like illness with exposure in
Midwest and southern United States transmitted by Lone Star tick (Amblyomma americanum); referred to as southern tick-associated
rash illness.
SECONDARY LESIONS Secondary syphilis, pityriasis rosea, erythema multiforme, and urticaria.
LABORATORY EXAMINATIONS
Skin Biopsy of EM. Deep and superficial
perivascular and interstitial infiltrate containing lymphocytes and plasma cells with some
degree ofvascular damage (mild vasculitis
or hypervascular occlusion). Spirochetes can
be demonstrated in up to 40% of EM biopsy
specimens.
laboratory confinnation. Diagnosis of late LB
confirmed by specific serologic tests.
COURSE
After adequate treatment, early lesions resolve
within 2 weeks and late manifestations are
prevented. Late manifestations identified early
usually clear after adequate antibiotic therapy.
However, delay in diagnosis may result in
permanent joint or neurologic disabilities.
EM (short duration of infection) treated with
antimicrobial agents does not confer protective
immunity. H LB goes untreated for months,
immunity may develop that protects against
reinfection for years.
TREATMENT
DIAGNOSIS
Doxycycline 100 mg twice daily for 14 to
21 da)15 is the treatment of choice for early
The CDC recommends a two-step approach:
http://www.cdc.gov/lyme/diagnosis treatment/
LabTest/TwoStep/.
Diagnosis ofearly LB made on characteristic
clinical findings in a person living in or having visited an endemic area; does not require
localized and disseminated disease. Late stage
Lyme disease should be treated for 14 to
28 da)15. Amoxicillin, cefuroxime, ceftriaxone, cefotaxime, and penicillin can be used
in children under 8, pregnant woman, and
doxycycline-allergic patients.
ARTHROPOD BITES, STINGS,
AND CUTANEOUS INFESTATIONS
CUTANEOUS REACTIONS TO ARTHROPOD BITES
• Arthropods are defined by an exoskeleton, segmented body, and jointed appendages. Arthropods
causing local and systemic reactions associated with their bites; Arachnida, Chilopoda, Diplopoda,
and Insecta.
• Cutaneous reactions to arthropod bites are inflammatory and/or allergic reactions.
• Characterized by an intensely pruritic eruption at the bite sites. whether immediately or minutes to
hours to days after the bite, persisting for days to weeks, manifested by solitary or grouped: Urticarial
papules; papulovesicles; bullae. Persons are often unaware of having been bitten.
• Systemic symptoms may occur, ranging from mild to severe, with death occurring from anaphylactic
shock.
• Arthropods are vectors of many systemic infections.
ARTHROPODS THAT BITE,
STING, OR INFEST
Four of nine classes of arthropods cause local
or systemic reactions.
1. Andmlda (four pairs oflegs): Mites, ticks,
spiders, and scorpions.
a. Acarina. (mites and ticks) Sm-coptes scabiei (scabies). Demodexfolliculorum and
D. brevis (demodicidosis). Environmental
mites. Ticks (Fig. 28-1) that feed on humans and are vectors for disease include
blacklegged or Ixodes tick, Amblyomma
americanum (lone star) tick, and
Dermacentor (American dog or Wood)
tick.
b. An.neae. (spiders) Loxosceles reclusa or
brown recluse spider. Latrodectus or black
widow spiders. Tegmaria or hobo spiders
cause necrotic araclmidism in the Pacific
Northwest of United States. Tm-antula:
Mild inilammatory response to bite and
to shed hairs.
c. Scorpionlda. Venom contains a neurotoxin that can cause severe local and
systemic reactions.
2. Chilopoda or centipedes.
3. Diplopoda or millipedes.
4. ln&eda (three pairs of legs).
a. Anoplura. Phthirius pubis or crab lice.
Pediculus a~pitis or head lice. Pediculus
corporis or body lice.
720
b. Coleoptera. Beetles. B&ter beeili:s contain the chemical cantharidin, which produces a blister when the beetle iB crushed
on tlu: skin.
c. Diptera. Mosquitoes, black flies (bites
produce local reactions as well aa black
:fly fever with fever, headache, nausea,
genera]ized lymphadenitis), midges
(punkies, no-see-wns. sand fliea), Tabanidae (horseflies, deerflies, clegs. breeze
ilies, greenheada, mango ilies); botflies,
CaJlilroga americanQ,. Dermaiobt4 hominb, Phlebotomid sand :fl..!es. and tsetse
:flies.
cL Hemiptera. Bedbugs and kissing bugs.
e. Hymenoptera. Ants, bees, wasps, and
hornets.
f. Lepidoptera. Caterpillars, butterflles, and
moths.
g. Siphonaptera. Fleas, chigoe, or sand flea.
ARTHROPOD-BORNE INFECTIONS
• Lyme borreliosis, tularemia, and bubonic
plague.
• Scrub typhus, endemic (murine) typhus,
spotted fever groups, and Q fever.
• Human granulocytic anaplasmosis.
• Tick-borne meningoencephalitis.
• Leishmaniasis and trypanosomiasis (sleeping
sickness or Chagas disease).
• Malaria and babesiO&is.
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
1 Inch
Blacklegged tick
Qxocfes scapularis)
-~~~~
{
·.. ';111f'
I,
'
Adult
femaJ9
I
; ·.
Adult
rnaJ9
~'
I
nymph larva
Lone star tick
w~~Dog1fck
(Dermacentor vatfab//fs)
_2
- ·~~ ~
FIGURE 28·1 Comparison of bladdeggad, lone star, and dog ticks Blacklegged or fxodes nymphal ticks transmit Borrello burgdorferl (Lyme disease) and
other lnfe<:tlons. Lone star ticks or Amblyomma americanum Is the vector for anaplasmosis, tularemia, and Southern tick-associated rash illness. Dog or wood ticks,
De!macentor variabilis, transmit Rocky Mountain spotted fever and tularemia.
• Filariasis, onchocerciasis (river blindness).
and loiasis.
CLINICAL MANIFESTATION
ERYTHEMATOUS MACUW Occur at bite sites and
are usually transient.
PAJIULARUR11CARIA or urticarial papules
persistent for >48 h (Ffp. 28-2 and 28-3);
u.su.ally <1 em; vesicle may for on papule.
Large urticarial plaques may occur.
BULLOUS LESIONS Tense bullae with clear fluid
on a sllghtly inflamed base (F.ig. 28-4); excoriation results in ero&l.on.
Excoriations of urticarial.
papular; and vesicular lesions common. Painful erosion may be secondarily inf'ectM with
StnJihjlocoa:us aunus. Excoriated or secondarily
infeded lesions mayheal with hyper- or bypoplgmentation and/or raised or depressed scars.
especially in more d.arldy pigmented individu.als.
SYSTEMIC FINDING$ May~ associated with
toxin or allergy to the substance injected during the bite. Many varied systemic infections
can be injected during the bite.
SECONDARY I.I.SIONS
FIGURE 28-2 Pepul1r ul'tk.t1 A 21-year-old
male awoke with multiple pruritic erythematous
papules on his exposed face, neck, forearms, and
hands. Bedding was heavily colonized with bedbugs.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 2•3 Papular urticaria A6-year-old girl with multiple mosquito bites on face.
CLINICAL VARIATIONS BY ARTHROPOD
Mms Sarcoptes salhiei causes infestation
scabies (see Scabies). Demodex foUiculorum
and D. brevis live in human hair Colll.cles and
sebaceous glands. causing demodkidosis (see
Demodicidosis, p. 731).
Food. Cowl, grain. maw, harvest. and animal
mite bites cause papular urticaria.
FOOD MITES Cheese, grain. or mold mites
can cause mild contact dermatitis: Baker's or
grocets itch. Straw mites. Bites ocaa during
harvest season causing dermatitis; straw
itch. HtlrWllt mite: Chigger&. Bites can cause
dennatitis. One rpecics traniiDli.ts Rickettsia
tsutsugamushi. the cause of scrub typhus.
Dermatophagoides species of house dust
mites are implicated in the pathogenesis of
asthma and atopic dermatitis. Feed on desquamated human skin and other organic detrltua.
living in bedding. carpets, and furniture.
Bodies and excreta may have a role in asthma
and other allergies. Affected persons respond
with production oflgB antibodies. Fowl mites.
Chicken. pigeons. etc. Bites cause papular
urticarla on exposed sl.te8. Rat mites cause painful bites and dermatitis and transmit endemic/
murine typhus. House mouse mite Is the veaor
fur rickettsialpox. Cheyletiella spp. (dog and cat
mites) bite pet owners causing pruritic lesions
on fo.reanns, chest, and abdomen. Canine
sarroptlc mange (S. SC4biei var. canis) and £eliDe
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
FIGURE 28-4 Bullou Insect bite A 1(}year-old child with bullous lesions on the ventral wrist and
popular urticarial on the forearm.
mange (Notoedres cati) cause a pruritic dermatosis in pet owners.
TICKS Ticka attach and feed painlessly.
skin necrosis. Associated with a maculopapular
exanthem. fever, headache, malaise, arthralgia.
and nausea/vomiting. Most lc:sioll8 diagnosed
Sec.retions can produce local bite .reactions
(erythema), febrile illness, and paralys!B. Black-
as brown recluse spider bites are bite .reactions
to other arthropods. 'Widow spiders inJect a
neuroto.Jin (a-latrotoxin) that produces bite
legged or Ixodes tick, lone star tick, and dog
tick are vectors for diseases. Erythema migrans
(see Fig. 25-81), characteristic of primary Lyme
disease or borrellosis. occurs at the b:lte site of
an infected Ixodes tick that transmits Bom1ta
burgtkrrferi, B. mayonii (Midwestern US).
Lymphocytoma cutis (see Fig. 25·82) also
occurs at the site of bite of an infeded bt:.odi!s tick.
SPIDERS Brown reduse spider bites can result in
mild local urticarial reactions to full-thickness
site reactions as wcll u varying degrees of
S}'ltemic toxicity.
INSECTS Pubic lice, huui lice, body lice papular
urtic:aria. acoriations. and secondary infections (see pages 7~731).
Mosquitoes. Bites wually present as papular
urticaria (Fig. 2S..3) on exposed sites; reactions
can be urticaria. eczematous, or granulomatous.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
Black Flies. Anesthetic is injected. resulting in a
paiD!ess initial bite; may subseque:ntly be<:ome
palnful with itching. erythema. and edema.
Black fly fever Is characterized by Ceve.r; nausea,
and generalized lymphadenitis.
Midges. Bites produce immediate pain with
erythema at bite site with 2- to 3-mm papule
and vesicles, followed by indwated.nodules (up
to 1 em.) persisting for many months.
Tabanidae or horse flies. Bites pa!nful with
papular urtl.carla; rarely assodated with ana-
phyla:r:is.
Dermatobia hominis (human botfly) in tropical regions causes fururu:ular myiasis, painful
lesions that resemble pyogenic granuloma or
abscess. Female bottly captures a mosquito,
attaches its eggs to the mosquito body, and
then releases the mosquito. Eggs hat<:h on the
mosquito be<:oming larvae and are deposited
on human skin. Larvae use bite site as portal
of entry Into skin. A prurltlc papule develops
at the site. slowly enlarging over several weeks
into a domed nodule (resembles a furuncle)
with a central pore (FiJ. 28-5). Larvae drop out
after 8 weeks to pupate in soiL
House Flies. Larvae deposited iDto any exposed
skin site (ear. nose, paranasal sinuses. mouth.
eye, anus. and vagina) or at any wound site
Oeg uk.ers, ulcerated squamous and basal cell
carcinomas, hematomas, or umbilical stump)
and grow intD maggot&. which can be seen on
the surface of wound~ wound myiasis
(Fig. 28-6). Maggot debridement therapy is used
to selectively debride necrotic wound tissue.
Cimex lectularius or bedbugs bite exposed
skin (face. neck, arms, or hands) of sleeping humans. Feeding takes 5 to 10 minutes.
Grouped papular urticaria (Fig.18-2) occur at
bite sites, usually, but now always,ln groups of
three ("breakfast. lunch. and dinner"). Bedbug
hides in crevices of'Mills. mattresses. and
furniture. Reddish brown streaks may be seen
on mattre.ss; bedbugs defecate old blood meal
while ingesting a. new meal
Reduviid or kissing bugs bite usually present as
papular urticaria; severe reactions can produce
necrosis and ulceration. Subfamily of reduviid
bugs transmits Trypanosoma cruzi. the agent of
Chagas disease.
Fleas. Papular urtJ.carla at bite site. Dog ficas
often live in carpeting and bite exposed lower
legs. Secondary changes of excoriation, prurigo
nodularis, and S. au reus infection oc::cur.
Tunga Penetrans or Chigoe Flea. Papule,
nodule, or vesicle (6 to 8 mm in diameter) with
a central black dot (tungiasls) produced by
posterior part of the flea's abdomJnal segments.
AJ eggs .mature. papule becomes a black.
pea-sized nodule (Flg.18-7). With severe
infestation, nodules and plaques appear with a
FIGURE 28-5 Furuncular myiasis A pruritic papule at the site of deposition of a botfly larva, slowly
enlarging over several weeks into a domed nodule (resembles a furuncle). The lesion has a central pore
through which the posterior end of the larva (Inset) Intermittently protrudes and thus respires.
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
FIGURE 2H Wound rnyllsls
Multiple housefly larvae in a
chronic stasis ulcer on the ankle
after castellani paint and Unna
boot treatment for 1 week Upon
removal, the maggots were visible; and the base of the ulcer
was red and clean, having been
debrided by maggots.
honeycombed appearance. Ulceration, iDflammation. and secondary lnfeaio.n om occur.
Most common on feet. especially under the
toenails, webspace.s. plantar aspea of the feet,
and sparing weight-bearing area&; in sunbathers. any area of exposed skin.
Fnnale bee. hornet, or wasp sting producing immediate burnlng/paln. followed by
intense,loc:al, erythematous reaction with
swelling and urticaria. Severe systemic reactions occur in individuals who are sensitized.
with angioedema/generalized urticaria and/or
respiratory lnsuffidency from laryngeal edema
or bronchospasm and/or shock.
Fire and harvester ants produce local skin
necrosis and systemic reactions to sting; bite
reaction begins as an intense local inflammatory reaction that evolw:s to a sterile pustule.
Caterpillar/math contact can produce
bumiDgli.tching sen&ation, papular urticaria.
irritation caused by histamine release, all.erg1c
contact dermatitis (Fig. 28-8), and/or systemic
reactions. Wind-borne hairs can cause keratoconjunctivitis.
DIFFERENTIAL DIAGNOSIS
Papular urticaria. Allergic contact dermatitis, especially to plants such as poison ivy or
poison oak.
DIAGNOSIS
<linical. diagnosis, at times,. confu:med by
lesional biopsy.
TREATMENT
Apply insect repellent such as
diethyltoluamide (DEBT) to skin and permethrin spray to clothing. Use screeus. nets, and
clothing. Treat flea-infested cats and dogs;
spray household with insectiddes (e.g., malathion, 1 to 4% dust).
lARVAE IN SKIN Thngiasis. Remove ftea with
needle, scalpel, or curette; topical petrolatum to
suffocate fie as; topical ivermect:i.n; oral thiabendazole or metrifonate Cor heavy in.festatio.ns.
PREVENTION
FIGURE 28-7 Tungi1Sis Periungual papule
with surrounding erythema on the lateral margin
of the frfth toe; the larva is visualized by removing
the overlying crust.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 2•a Immunologic lgE-medlated contact urticaria: pin• pro cessionary catarplllar
Linear edematous papules and vesicles occurred on the exposed arm shortly after exposure to Thaumetopoea pityocampa in a pine forest.
FURUNC.VLAR MYIASIS Suffix:ate larvae by
covering with petrolatum and removing the
following day.
GLUCOCOR11COIDS Give potent topical giucocorticoids for a short duration for intense pruritus.
Oral glu.cocorticoids can be given for persistent
pruritus.
ANTIMICROBIAL AGENTS Secondary Jnfectlon
antibiotl' treatment with topical agents.
SYSTEMIC INFEcnONIINFESTATION Treat with
appropriate antimiaobial agent
PEDICULOSIS CAPITIS ICD-1 0: 885.0
• Infestation of the scalp by the head louse.
• Feeds on scalp and neck and deposits Its eggs on hair.
• Presence of head lice Is assodated with few symptoms but much consternation.
ETIOLOGY AND EPIDEMIOLOGY
Pediculus Hwnanus Capitis. Sesame seed size. 1 to 2 mm. Peed e"m'f 4 to 6 h.
Move by grasping hairs close to acalp; can
aawl up to 23 em./day. LU:e lay nita within 1 to
2 mm. of scalp. Nits ate ova within cbitlnous
ase. Young .Ike hau:b. within 1 wuk, passing
through nymphal staps and maturing to adults
on:r a period of 1 week. One female can lay
50 to 150 ova during a 16-day lifetime. Survive
SUBSPECIES
only for a few hours off scalp. 'ftansmillsion:
Head-to-head 'ontact shared hats, caps.
brushes. combs; theater seats; pillows. Head
louse is not a vec:tor of int'eaious disease.
DEMOGRAPHY In the United States. more
common in whites than blaclc:a; claws have
adapted to grip cylindrical hair; hair pomade
may inhlbit Infestation.ln Africa. pediculosis
Qpitis is relatively unoommon. Estimated that
6 to 12 million persons in the United States are
infested annually.
CLINICAL MANIFESTATION
SYMPTOMS P:rurl.tus of the back. and sides
ofscalp. Saatclling and secondary lnfKtlon assodated with ocxlpital and/or (:ervical
lymphadenopathy. Some individuals exhibit
obse.saive-compukive disorder or delusions of
parasitosis after eradiations ofli(:e and nits.
INFESTATION Head lice ate identified by eye or by
microscopy (hand lens or dermatoscope) but ate
ditlkult to find. Most patients have a population
of< 10 head li(:e. Nits ate the owl grayish-white
egg capsules (1 mm long) firmly cemented to
the hairs (Pig. 28-9); vary in number from anly
a few to thousands. Nits ate deposited by head
SI!CTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
FIGURE ZH Pedlwlosls CJipltls: nib (A) Arrows: Grayish-white egg capsules (nits) are firmly
attached to the hair shafts, visualized with a lens. (B) Magnified, an egg with a developing head louse
nymph attached to a hair shaft is seen.
Ucc on the: bair &haft aa it c:mcrgcs from the: follicle. With current infestation, nit& are near the
scalp; with lnfmatl.on oflong standing. nits may
be 10 to 15 an from the scalp. In that scalp hair
grows 05 mm daily. the presence ofnit. 15 an
from thc: acalp indicate& that thc: infestation il
apprclldmmly 9 .IUOilt.ba old. New viable eggs
have a creamy-yalow color; empty eggahel1s
are white. Sites ofprediJectkm: Head Ucc nearly
always confined to the scaJp, especially occipital
and postBuricular n:giona. Rarely. head lice
in&llt the beard or other hairy mea. Although
more common witb aab lice, head lice can alto
infest the eyela&hes (pediculosis palpebrarum).
SKIN LESIONS Bite m:u:tions: Papular urticaria
on the neck. Reactions related to immune
sensitivity/tolerance. Secondary lesions: Ecuma,
acoriation. ur litkn simpla chronicus on the:
ocdpital scalp and neck secondary to chronic
scratchlnglrubbing. Secondary infection with S.
aureus of eczema or acor:iations; may extend
onto the neck, forehead, face, or ears. Posterior
occipital lymphadenopathy.
.A1opic dermatitia, impetigo.
and lichen simplex chronic:us.
NO INFESTATION Delusions of parasitosis.
SCALP PRURITUS
LABORATORY EXAMINATIONS
MICROSCOPY Nits 0.5-mm oval. wbiWh eggt~
(FJg. 28-9B). Nonviable nits show an absence
ofan embryo or open:ulum. Lowe. Insect
with six legs, 1 to 2 mm in length, wingless,
translucent grayish-white body that iJ red when
engorged with blood.
DIAGNOSIS
Clin1cal. findings. confirmed by detection of
lice. Louse comb increases chances of finding lice. Nits alone are not diagnostic of active
infestation. Nits within 4 mm of scalp suggest
active infestation.
TREATMENT
Pmnethrin.
DIFFERENTIAL DIAGNOSIS
TOPICALLY APPLIED INSECTIODES
SmaU White Hair "'Bada'" Hair cuts (inner
root sheath I:CJDDallts), hair lacquer, hair gels.
dandruff (epidermal scales), and piedra.
SYSTEMIC Oral ivennectin.levamilole, and
malathion, pyrethrin, ivermectin, and spi-
nosad.
albendazole.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
PEDICULOSIS CORPORIS ICD-10:885.1
• Body lice reside and lay eggs In clothing. They occur In poor socioeconomic conditions.
• Lice leave clothing to feed on a human host Body louse survives more than a few hours away from
the human host.
• Body lice are vectors of many systemic infections.
EPIDEMIOLOGY AND ETIOLOGY
EnOLOGICAGENT
Pediculus HumattU$ Huma-
nus. Larger than head louse: 2 to 4 mm;
otherwise indistinguishable. Life span 18 days.
Female lays 270 to 300 ova. Nits: Ova within
chitinous case. Nlts incubate !or 8 to 10 days;
nymphs mature to adults In 14 daf5.
HABITAT Live in seams of clothing; can survive
without blood meal for up to 3 days. Attaches
to body hairs to feed. Risk &ctors mr i:rlttst:s.tion
include poverty; war. nat:w:al disasters, indigence.
hom.elessntss, and refugee-amp populations.
BODY Lla. AS Vf.CTORS OF DISEASE
Body lice
transmit many infectious agents while feeding.
BartoneUa quintana causes trench fever and
endocarditis. Rickettsia prowazekii causes epidemic typhus. BriU-Zinsser disease (louse-borne
relapsingfover) is recrudescence ofepidemic
typhus fever.
CLINICAL MANIFESTATION
INFESTATION Uce and nits are fowtd In clothing
seams (Fig. 28-10). Lice grab on to body hairs
to feed.
FIGURE 28-10 Pediculosis corporis A 6o-year-old homeless male. Multiple lesions
secondary to excoriations, prurigo nodularis, and lichen simplex chronicus. Lice and nits
are seen In the seams of clothing (Inset).
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
REACTIONS TO BITES
Bite reactions such as papu-
lar urticarial (Pig. 28-10) are similar to those of
head lh:e. Changes secondary to rubbing and
scratching Include excoriations, eczema,ll.chen
simplex, infectl.on with S. aureus, and postin-
ftammatoryhyperpigmentation (Fig. 28-10).
Scabies,. pediculosis capitis, and Pulex initans
(the human flea) can coexist.
DIAGNOSIS
Lice and eggs are found in clothing seams.
TREATMENT
DECONTAMINATION OF CLOTHING AND BEDDING
Hygiene measures.
DELOUSING Pyrethrin, pennethrin.
DIFFERENTIAL DIAGNOSIS
Atopic dennatitis, contact dennatitis,. scabies,
or adverse cutaneous drug reactl.on.
PEDICULOSIS PUBIS ICD-1 0: 885.2
• In infestation of hair-bearing regions by the crab or pubic lice.
• Most commonly inhabit the pubic area; hairy parts of the chest and axillae; upper eyelashes.
• Manifested clinically by mild-to-moderate pruritus, papular urticaria, and excoriations.
ETIOLOGY AND EPIDEMIOLOGY
CLINICAL MANIFESTATION
Phthirius pubis, the crab or pubic louse. Size 0.8
to 1.2 mm. First pair oflegs v..:stigial; other two
clawed (Fig.18-ll). Life span 14 days. Female
lays 25 ova. Nits .lncubatc for 7 days; .nymphs
mature over 14 days. Mobility: Adults can
crawl I 0 em/day. Prefer a hwnid environment;
tend not to wander. Infestation most common
in young males. 'lransmission during close
physical contact: Sharing bed. May coexist with
other sexually transmitted diseases.
OFTEN ASYMPTOMATIC Mild-to-moderate pruritus ror months. With excoriation and secondary infection. lesions may become tender and
be associated with enlarged regional
INFE.S'DlTION Uce appear as 1- to 2-mm.
brownl.sb.-gray speclcs (Fip.18-12 and 28-13) In
hairy areas involved. Remain stationary fOr days;
mouth pam embedded in skin; claws grasping a
hair on either side. Usually fi:w in number. Ntts
attached to hair appear as tiny white-gray speds
FIGURE 2•11 Crab louse Adult female with
FIGURE ~12 Crab louse Crab louse (arrow)
on the skin In the pubic region.
an egg developing within her body.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 28-13 Crab lice In eyelashes A
1~year-old child. Crab lice (arrows) and nits
on the upper eyelashes of a child; this was the
only site of infestation.
(Fig. 28-13). Few to numerous. Eggs at hairskin junction indicate active infestation. Inftstatum most common in pubic and axillary areas;
also, perineum, thighs. lower legs, trunk, and
periumbilical In children. eyelashes (Fig. 28-13)
and eyebrows maybe infested without pub:lc
involvement. Maculae coeruleae (see below)
most common on lower abdominal wall. buttocks, and upper thlghs.
SKIN LESION$ Papular urticaria (s.mall erythematous papules) at sites offeeding, especially
periumbilical (Fig. 28-14). Changes si!COndary
to rubbing lichenification and c:xcorlatiOllS.
Secondary S. aureus tnfoctton. Maculae c:oeruleae
FIGURE 28-14 Crab lice Infestation: papular urtle~~rfa A 25-year-old with pruritus. Multiple inflammatory papules at sites of crab lice bites on the abdomen and the inner aspects of the thighs.
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
(taches bleues) are shm:-gray or bluish-gray
maculea around 0.5 to 1 em in diameter. nonblancbing. Result from crab louse bites. With
eyelid infestation. serous crusts may be present
along with lice and nits; occasionally. edema of
eyelids with severe in&stati.on.
With se<:ondary impetiginization. regional
lymphadenopathy.
DIAGNOSIS
Demonsll'a1ion of live adult lice, nymphs, or nits
In the pubic an:a to diagnose active infestation.
COURSE
Tn:atment Is usually effective. Relnfestation can
occur. Retreatment may be necessary Iflice are
found or If eggs are observed at the hair-skin
DIFFERENTIAL DIAGNOSIS
junction.
Atopic dermatitis, seborrheic dermatitis, tinea
crur:i8, molluscum contagiosum. and scabiu.
TREATMENT
The&e disorders may coeJJst with aab louse
infestation..
PEDICUlOSIS Seep. 727. Decontaminate bedding and clothing. Tn:at sex partners.
DEMODICIDOSIS ICD-10: 888.0
Demodex species are human face mites, part of the human cutaneous microbiome. D. folliculorum
resides in hair follicles; D. brevis, infundibulum of sebaceous glands. Mites do not invade tissue. Site of
habitation usually symptomatic. In some cases, this causes an inflammatory reaction (demodicidosis)
that occurs with lesions resembling rosacea, suppurative folliculitis, or perioral dermatitis (Fig. 28-15).
• Treatment. Topical ivermectin, permethrin; in severe cases oral ivermectin 200 !JWkg.
B
FIGURE 28-15 Demodicklosls A 25-year-old female noted facial rash the day after a heavy workout
(A) Tender red papules on the face. Lesions look like papular rosacea. {B) Microscopic examination of
curetting of papule demonstrates Demodex mite. Lesions resolved w1th orallvermectln.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
SCABIES ICD-10: 886
• Superfidal epidermal Infestation by the mite Sarcoptes scob/el var. homlnls. 'INnsmlsslon: Usually
spread by skin-t<rskin contact and fomites.
• Oinlcal Manifestation. Pruritus often with minimal cutaneous findings. Burrows under stratum
corneum.
• Scabetic Nodules. Eczematous dermatitis. Hyperinfestation (crusted or hyperkeratotic or Norwegian
scabies).
• Diagnosis. Easily missed and should be considered in a patient of any age with persistent generalized severe pruritus.
ETIOLOGY AND EPIDEMIOLOGY
mOLOGICAGENT S. scabieivar. hominis. Obligate human paruite. Mites of all developmental
stages burrow into epiderm.ls shortly after
contact, no deeper than stratum gra.nulosu.rn;
deposlt feces in tunnels (Fig. 28-16). Female
life span 4 to 6 weeks; lays 40 to 50 eggs. Lays
3 eggs per day in burrows; eggs hatch in 4 days.
Leave bunow, usually at Digbt. and lay egg~
during the day. Hatched larvae migrate to
sldn surface and mature Into adults. Males
children with scabies exceeds that of children
with diarrheal and upper-respiratorydisease.
In countries where human T ce1lleukemial
lymphoma virus (HTLV-I) disease 18 common. hype.rlnfestatlon scabies is a marker of
this inCectl.on. Transmlasion by skin-to-skin
rontact and fomites. Mites can remain alive
for >2 days on clothing or in bedding. Persons
with hyperinfestation shed many mites into
their environment dally and pose a high risk of
inCecting those around them.
and females copulate. Gravid female burrows
back under stratum corneum; male falls off.
PATHOGENESIS
In classic scabies,. approximately 10 rema:Jes
Hypersenal.tivit ofboth immediate and delayed
types occurs In the development of lesions
other than burrows. Duringfim infestation.
pruritus occurs after sensitization to S. scabid
hu occurred. w;ually within 4 to 6 weeks. After
reinfesttmon. pruritus may occur within 24 h.
Wlth hyperlnfostatton. persons are often lmmu-
per patient are pre&ent. With hyperinfestati.on,
> 1 milllon mites may be present. Estimated at
300 milllon cases/year worldwide.
DEMOGRAPHY MaJor pubUc health problem in
many less-developed rountries. In some areas
of South and Central America, prevalence i&
about 100%. In Bangladesh, the number of
nocompromised or haw neurologic disorders.
FIGURE 28-16 Burrow with S•rcoptes scabiali (fem•le), eggs, •nd fee.. Female mite at the end
of a burrow with seven eggs and smaller fecal particles obtained from a papule on the webspace of the
hand.
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
CLINICAL MANIFESTATION
Symptoms
Patients are often aware ofsimilar symptoms
in family members or sc:maJ. partner&. Pruritus
is intense, widespread, but usually spares the
head and ned. Itdling often interferes with
or prevents sleep. Pnuitus may be absent with
byperinfe.station. Ra$h ranges from no rash to
generalized erythroderma. Patients with atopic
dlathes!a scratch. producing eaematous dermatit!a. Some individuals experience pruritus
for many months with no rash. Tenderness of
lesions suggests secondary bacterial infection.
Cutaneous Findings
(1) Lesions occurring at the sites ofmite .Infestation, (2) cutaneous manifestations of hypersensitivity to mJ.tes. (3) lesions secondary to
chronic rubbing and scratching. (4) secondary
infection, (5) hyperinfestation, and (6) variants
ofscabies in special hosts: those with an atopic
dlathes!a, nodular scabies, scabies in infants/
small clilldren, and scabies Jn the elderly.
INTRAEPIDE.RMAL JURROWS Skin-colored ridges,
o.s to 1 em in length (Figs. 28-17 to 28-19),
either linear or serpiginous, with minute vesicle
or papule at end of tunneL Bach infe&ting
female mite produces one burtow. Mites an:
about 0.5 mm in length. Burrows avuage 5 mm
in length but may be up to 10 em. Distribution: Areas with few or no hair follicles, usually
where stratwu comewu is thin and soft, Le.,
the lnterdlgital. webs of the hands (Fig. 28-17),
wrists, palms and soles in infants (Fig. 28-18),
shaft ofpenis. elbows. feet, buttocks. or u:illae
(Figs. 28-19 and 28-20). In infants, infestation
may also occur on head and neck.
Scabies with nodules 5 to 20 mm Jn diameter. red. pink. tan.. or brown Jn c:olo.r; smooth
(Fig. 28-ll); burrow sometimes sun on the
surface of a very early lesion. Distribution:
Scrotum, penis {Pig. 28-21), axillae. waist,
buttocks (Fig. 28-22), or areolae. Re&Olve with
post:lnflammatory hype.rpigmentation. May be
mo.re apparent after treatment, as eczematous
eruption resolves.
SCABIES WITH HYPERINFESTATION (FORMERLY
CAlLED NORWEGIAN SCABIES) May begin as
ordinary scabies. In others. clinical appearance
is ofchronic eczema, psorlaslfo.nu dermatl·
tis, seborrheic dermatlt!a, or erythroderma.
Lesions often markedly hyperkeratotic and/or
crusted (Pigs. 28-23 and 28-24). Warty dermatosis of the hands/feet with nail bed hyperb:ra·
to81s. Erythematous scaling eruptions occur
on the face, neck. scalp. and trunk. A1fected
persons have a characteristic odor. Distribution:
FIGURE 28-17 Scabies with burrows Papules and burrows in typical location on the finger web. Burrows are tan or skin-colored ridges with linear configuration with a minute vesicle or papule at the end of
the burrow; they are often difficult to deflne.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 28-18 Burrows of scabies on the palm of a 3-year-old infant. There are
many linear and even semi-circular lesions. The whole family was affected.
Generalized (even Involving head and neck Jn
adults) or localized. In patients with neurologl.c
deficit, hyperinfi:station may occur only in
an affected limb. May be localized only to the
scalp, face, finger, toenail bed, or sole.
"''d,. or autosensitization-type reactions
characterized by widespread small urticarial
edematous papules mainly on the anterior
trunk, thighs. buttocks, and forearms.
SECONDARY CHANGES Excoriations. lichen
simplex chronicus, and prurigo nodules.
Postin1lammatory hyper- and hypoplgmentation In more deeply pigmented Jndividuals.
Bullous scabies can mJmlc bullous pemphigoid.
Secondary infection by S. aumu.
DIFFERENTIAL DIAGNOSIS
Pruritus. localized or generalized, rash delusions of parasitosis, adverse cutaneous drug
reaction. atopic dermatitis. allergic contact
dennatitis, and met:abollc pruritus.
Nodular scabies. urticaria plgmentosa (in
young chil.d), papular urticaria (Insect bites),
prurigo nodularis, and pseudolymphoma.
SCABmC HYPERINFESTA110N Psoriasis. eczematous dennatitis, seborrheic dermatitis, and
erythroderma.
LABORATORY EXAMINATIONS
MICROSCOPY Higbelt yield in identifying a mite
Is in typical burrows on the finger webs, fiexor
aspects of wrists, and penis. A drop of mineral
oil is placed over a burrow, and the burrow is
scraped offwith a curette or no. 15 scalpel blade
and placed on a microscope slide. Three findings are diagnostic ofscabies: S. scabiei mites,.
eggs, and fecal pellets (scybala) (Fig. 28-24).
DERMATOPATHOLOGY Scabtet1c burrow: Located
within stratum comeum; female mite with
eggs situated in blind end of burrow. Spongiosis (epidermal edema) near mite with vesicle
formation common. Dermis shows infiltrate
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
FIGURE 28-19 Burrows on penis shaft and scrotum If you suspect scabies in a male,
always look at the penis.
FIGURE 28-20 Scabies: Predilection sites Burrows are
most easy to Identify on the
webs pace of the hands, wrists,
and lateral aspects of the
palms. Scabietic nodules occur
uncommonly, arising on the
genitalia, especially the penis
and scrotum, waist axillae, and
areolae.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
with eosinopbils. Nodules: Dense chronic
inflammatory infiltrate with e011inophils. In
some cases, persistent arthropod reaction
resembling lymphoma with atypical mono-
nuclear c:ells. Hyperinfestation: Thickened
stratum corneum riddled with innumerable
mites.
DIAGNOSIS
Clinical findings. confirmed by microscopy
(identification of mites, eggs, or mite feces).
COURSE
Pruritus often persi&ts up to several weeks
after successful eradication of mite infemti.on,
understandable in that the pruritus ls a hypersensitivity phenomenon to mite antigen(s).
If relnfestation oc.curs, pruritus becomes
symptomatic within a fuw days. Delusions of
parasitosis can occur in individuals who have
been successfully treated for scabies or have
never had scabies. Hyperl.n!e.statlon: May
FIGURE 2•:n Salbles with nodules R~
brown papules and nodules on the penis and scrotum; these lesions are pathognomonic for scabies,
occurring at sites of infestation In some lndMduals.
be impossible to eradicate; recurrence more
likdy to relapse than reinfestation. Nodules: In
treated patients, 8096 resolve in 3 months but
may persist up to 1 year.
FIGURE 2•22 SalbiH with nodules A 4-year-old infant with reddish brown nodules on thigh and
buttocks persisting after treatment with permethrln.
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
FIGURE 2•23 ScllbiH wtlh hyplffnfatatlon A60-year-old mal-
nourished female with hundreds of papular lesions and burrows on the
back and buttocks. Pruritus was excruciating.
MANAGEMENT
PIUNCIPUSOFTREATMENT Treat infested indlviduals and dose physical contacts (including
sexual partners) at the same time, whether or
not symptoms are present Application should
be to all skin sites.
RECOMMENDED REGIMENS Permethrln 5%.
Cream applied to all areas of the body. IJndane
(g-Benzene Hexachloride) 1% lotion or cream
applied thinly to all areas of the body from the
neck down; wash off thoroughly after 8 h. Note:
Ll.ndane should not be used after a bath or
shower, or by patients with atenaive dermatitis, pregnant or lactating women, or children
younger than 2 years. Mite reslstan.ce to lindane
exists. Low cost :m.akes lindane a key alternative
in many countries.
ALTERNAnVE REGIMENS TopiaiL Crotamiton
10%. sulfur2 to 1096inpetrolatum. ben~
benzoate 1096 and 25%. benzyl benzoate with
sulfiram, malathion 0.5%, sulfram 2596, and
ivennectin 0.896.
Systemic. Oral ivermectin, 200 mglkg; sing1e
dose reported very effective in 15 to 30 days.
Two to three doses, separated by 1 to 2 weeks.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 2•24 Scabies wtth hyperfnfestatlon A 79-year-old male with hyperkeratotic scabies for
4 years. The patient had been treated in his home with topical antiscabetic agents and oral ivermectin as
well as extensive decontamination of his home on multiple occasions. Confluent hyperkeratotic plaques
are seen on the back.. buttocks, and legs. As many as five scabetic mites were seen on one microscope
fleld {see Inset).
usually required for heavy Infestation or
in immunocompromised Individuals. May
effectively eradicate epidemic or endemic
scabies in institutions mch as nursing homes,
hospitals, and refugee camps. Not approved
by U.S. Food and Drug Administration
or European Drug Agency. Do not use in
ofscabies resolve after intralesional.
injeaion of triamcinolone acetonide.
PO$T$CABIE1'1( ITCHING Generalized itdrlng that
persists a w=k or more is probablycaused by
hypersensii:ivi to remaining dead mites and .mite
NODULES
CRUSTED SCABIES
products. Anlihlstamines, top.lcal steroids can be
used. For severe, pe.rs:lstent pruritus, espedall.yin
individuals with a historyofatopic disorders, a
14-daytapered course ofprednisone is indic:ated.
SECONDARYBACTERIALINFEC110N 'li'eat with
taml:nation of the environment.
agent.
infants, young children, or pregnant/lactating
women.
Oral ivermectin combined
with topical scalicides (not ivermectin). Decon-
mupirocin ointment or systemic antimic.robial
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
CUTANEOUS LARVA MIGRANS IC0-10: 876
• Creeping Eruption. Cutaneous Infestation following percutaneous penetration and epidermal
migration of hookworm larvae.
• Etiologic Agents. Cutaneous larva migrans: Hookworms larvae of Ancylostoma braziliense in the
United States. Ova of hookworms are deposited in sand and soil in warm shady areas, hatching into
larvae that penetrate human skin. Humans are aberrant. dead-end hosts who acquire the parasite
from an environment contaminated with animal feces. Larvae penetrate human skin, migrating
within the epidermis up to several centimeters a day. Most larvae are unable to develop further or
invade deeper tissues and die after days or months. Larva currens: Strongyloides stercora/is; filariform
larvae can penetrate skin (usually on buttocks), producing lesions similar to larva migrans.
CLINICAL MANIFESTAnON
LARVA CURRENS (CUTANEOUS STRONGYLOIDIASIS)
CIITANEOUS LARVA MIGRANS Serpiginous, thin,
urticaria, papulovesicles at the site of larval
penetration (Fig. 28-17). Allsociated with
Intense prurl.tus. Occurs on buttocks. thlgbs,
linear, raised. and tunnel-like lesion 2 to 3 mm
wide containing serous fiuid (Fig. 28-15).
Several or many lesl.ons may be present.
depending on the number of penetrating larvae
(Fig. 28-26). Larvae move a few to many millimeters daily, confined to an area of several
centimeters in diameter. Infe.station most
commonly occurs on the feet. lower legs. and
buttocks.
A distinctive form of larva migrans. Papules,
back. shoulders. and abdomen. P.ruritu.s and
eruption disappear when larvae enter blood
vessels and migrate to intestinal mucosa.
DIFFERENTIAL DIAGNOSIS
Migratory lesions from other parasites. photoallergic contact dermatitis, jellyfish sting. and
epidermal dermatophytosis.
LABORATORY FINDINGS
DERMATOPATHOJ.DGY Parasite& seen on biopsy
specimens from advancing point of the lesion.
DIAGNOSIS
Clinical findings.
COURSE
Self-llmlted; hUJDab8 are "dead-end" host&.
Most larvae die and the lesions resolve within
2to8weeks.
TREATMENT
FIGURE 2•25 Cutanaous larva mlgrans A
serpiginous, linear, raised, tunnel-like erythematous lesion outlining the path of migration of the
larva.
TOPICAL AGENTS 'Ihlabendazole, ivermectin,
and albendazole are effective.
SYSTEMIC AGENTS Thiabendazole, orally 50 myj
kg per day in two doses (maximum 3 gld) for
2 to 5 days; ivermectl:n. 6 mg twice dally, albendazole, 400 mgld for 3 days; highly effective.
REMOVAL OF PARASITE. Do not attempt; parasite
not in visible lesions.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
FIGURE 2•2t Cutanaous llrva migrans Multiple raised, tunnel-like, partially crusted and scaly
lesions on forefoot.
FIGURE 28·27 Larva curnns Multiple,
pruritic. serpiginous, inflammatory lines
on the buttocks at sites of penetration of
S. stercora/is larvae.
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
WATER·ASSOCIATED DISEASES
• various aquatic microorganisms can cause soft-tissue Infections after exposure.
• Bacteria. Aeromonas hydrophllo, Edwards/ella tordo, Erysipelothrix rhusiopathlae, Mycobacterium marlnum, Pfiesteria pisdddo, Pseudomonas species. Streptococcus iniae_ Vibrio vulnificus, and other Vibrio
species.
• Alga. Prototheco widcerhomii.
• Localized Cutaneous Infestations. Cercarlal dermatitis and seabather's eruption can occur after
exposure to microscopic marine animals.
• Cnidaria ijellyfish) and echinoderms (sea urchins, starfish) can cause envenomation.
SCHISTOSOME CERCARIAL DERMATITIS ICD-10: 865.3
• Swimmer's itch, clam digger's itch, schistosome dermatitis, and sedge pool itch.
• Acute pruritic papular eruption at the sites of cutaneous penetration by Schistosoma cercariae larvae
of schistosomes whose usual hosts are birds and small mammals.
• Schistosomes implicated: Trichobiiharzio, Gigantobiihorzia. Omithobilhorzia. Microbilhorzio, and Schistosomatium.
• Exposure can be to fresh, brackish, or saltwater. Eggs produced by adult schistosomes living in animals
are shed with animal feces Into the environment; on reaching water, schistosome eggs hatch, releasing fully developed larvae (miracidia). Snails are the appropriate hosts for miraddia, from which they
emerge as cercariae. These must penetrate the skin of a vertebrate host to continue development
• Transmission. Humans are dead-end hosts. Cercariae penetrate human skin, elicit an inflammatory
response_ and die without Invading other tissues. Occurs worldwide In areas with fresh and saltwater
Inhabited by appropriate molluscan hosts. Acquired by skin exposure to fresh/saltwater Infested by
cercariae.
CLINICAL MANIFESTAnON
Prutl.tus and rash begin wltbln hours after
exposure. A pruritic macular, papular,
papul<M:Si.cular, and/or urticarial eruption
develops at exposed site& with marked pruritus
(Fig. 28-28), sparing parts of the body covered
by clothing. (1n contrast. stabather's eruption
occurs on areas of the body covered by swimsuits.) Ptqmlm- urti<:arUJ oc:curs at each site of
penetration in previau.sly sensitized individuals.
In highly sensitized persons, lesions may progress to eaematous plaques, urtlcarlal wheals,
and/or vesicles, .reaching a peak 2 to 3 days after
exposure. Sc:histosomes capable ofcausing iD:vasive disease in humans (Sc:histosonu~ mansoni,
S. haematobium, and S. japonicum) may cause
a similar skin eruption shortly after penetration
as well as late visceral complications.
COURSE
Lc:s:lons usually resolve: within a week.
TREATMENT
Topical and/or systc:m.ic glucocorticolds may be:
mdlcated in more severe cases.
FIGURE 28-28 Schistosome cerarlal derma·
tltis A highly pruritic papulovesicular eruption
on the knees acquired after the patient waded
through a slow-flowing creek.
PART Ill DISEASES CAUSED BY MICROBIAL AGENTS
SEABATHER'S ERUPTION IC0-10; 865.3
• Etiology. caused by exposure to two marine animals: Larvae of the thimble jellyfish, Llnuche
unguiculata. in waters off the coast of Florida, caribbean, Mexico, and Brazil. Planula larvae of the sea
anemone, fdwardsielfa lineata_ Long Island, NY.
• Pathogenesis nematocysts of coelenterate larvae sting the skin of hairy areas or under swimwear,
presumably causing an allergic reaction. Some affected individuals recall a stinging or prickling
sensation while In the water.
CLINICAL MANIFESTAnON
Lesions present dinicaily as inllammatory
papules 4 to 24 h after aposure {Fig. 28-29). A
monomorphous eruption of erythematous papules or papulavcsicles i8 seen most commonly:
vesicles. pustules. and papular urticaria, wh1ch
may progress to crusted erosions. In comparison with cercarial dermatitis, which ocx:urs on
exposed sites. seabather's eruption oocurs at
sites covered by bathing apparel while bathing
in saltwater.
COURSE
On average.leslon8 per818t for 1 to 2 weeks. In
sensitized individuals, the eruption can become
progressively more severe with repeated
exposures and may be associated with systemic
symptoms.
TREATMENT
Topical or systemic glu.cocorticoids provide
symptomatic relief.
FIGURE 28-lt Seabdter's en~pdon This pa~
ulovesicular rash appeared on a swimmer while on
vacation in the caribbean. During swimming, the
patient experienced slight stinging in the regions
covered by her bikini; later that evening she
noticed the eruption. The rash is characteristically
confined to ttte areas covered by ttte swimwear.
CNIDARIA ENVENOMATION$ ICD-10: T63.6
• Etiology. There are > 10,000 Cnideria spp. that are swimming medusa or sessile polyps which inject
toxin/venom that has local and systemic effects. Members of ttte Cnidaria phylum that can affect
humans are jellyfish, Portuguese man-of~ar, sea anemones, and fire •coral:
• Pa'lhogenesls. Cnidarian stings elicit toxic rather than allergic reactions. Ranging from mild, selflimited Irritations to extremely painful and serious Injuries.
CLINICAL MANIFESTAnON
TREATMENT
Pruritic, burning, and painful papules in linear
arrangement (Figs. 28-30 and 28-31).
Wet dressings, topical corticosteroids.
COURSE
Stings from box: jellyfi&h. can be fatal
SECTION 28 ARTHROPOD BITES, STINGS, AND CUTANEOUS INFESTATIONS
FIGURE 28-30 Jelr,fllh envanomation Pruritic and painful papules in a linear arrangement on the
leg, appearing after contact with jellyfish.
FIGURE 28-31 Fire cor•l envenornatron A 47-year-old female with painful palms that
occurred after contact with fire coral. The palms and palmar fingers are red and edematous
at sites of envenomation.