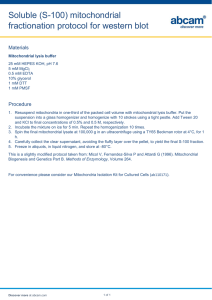
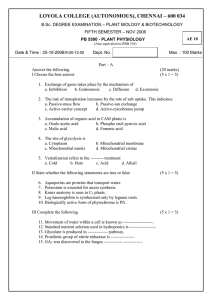
The Role of Mitochondria Dynamic in bone healing Abstract The regeneration capacity of tissues can best be monitored after injury; therefore, bone healing was in the focus of several studies as a model system of regeneration. Bone is a living tissue that not only mechanically supports the body and protects vital organs, but also produces blood cells and stores minerals. As a result of aging, hormonal imbalances, nutrient deficiencies, or the frequent use of certain medications, the bone remodeling cycle process may become unbalanced. Like many other European societies, the German population is an aging society. Recently the population development department of the Federal Statistics Office predict that by the year 2040, one in two of German population will be older than 50 and one in three older than 60 years old. One in every seven will be over the age of 80 years old.In aged patients, the capacity of such regeneration is limited. Many studies have addressed several factors that correlate with aging along and with the energy metabolism, however, rarely were mitochondria the target of investigations. Mitochondria are powerhouses of the cell, generating chemical energy in the form of ATP. Several agerelated pathologies like neurodegenerative or metabolic diseases and cancer have been linked to mitochondria. Today we know that the initial phases of healing turn from proinflammatory state into anti-inflammatory state. Our knowledge also revealed that inflammation induce mitochondrial dysfunction. Recent studies even showed promising results by utilizing fission inhibitors to encounter mitochondrial dysfunction. Simply put, balancing the dynamic of mitochondrial morphology is possible and have potential in understanding the limited regenerative capacity at aging. However, little is known in this specific regard. The project will deepen our knowledge of mitochondrial dynamic differences between cells from old and young donors, and can offer answers to the continuous downregulation of mitochondrial genes throughout the healing process. The project will also unravel the effects of pro- and anti-inflammatory stimulants on stromal cells and their differentiation. Furthermore, the crosstalk between mitochondrial dynamics and strontium as a prophylactic drug will be investigated. We hypothesized that treatment with non-steroidal anti-inflammatory drugs (NSAID) and Strontium will both contribute to the balance in mitochondrial dynamics. Furthermore, we also hypothesized that fission inhibitors will reflect favorably on osteogenic and chondrogenic differentiation of stromal cells from aged donors. Keywords Bone, Mitochondria (Mt), Mitochondrion Dynamics, Mesenchymal Cells (MSC), Osteogenesis, Age related diseases Introduction One important neglected factor is the weakness of tissue regeneration in later ages. The ability of the bone to restore its structure and function after injury declines, even in healthy old individuals. To best understand the process of bone healing firstly we must be able to understand the molecular mechanisms by which the bone is generated from its precursors stem cells. This can be explained by focusing in the mesenchymal stem cells (MSCs) differentiation towards bone tissue [1, 2]. Furthermore, this will enhance not only our understanding of aging but also most importantly the possible therapy for old patient. Bone fractures like and other body injury, once its occur, it will directly stimulate the immune system, since the bone is highly vascularized tissue. At the early stages of healing, bone hematoma moves from the pro-inflammatory into an anti-inflammatory state[9]. Furthermore, low levels of oxygen and glucose as well as high concentrations of lactate and reductive metabolites. We know that the inflammation caused by the immune response and the bioenergetics situation together have a considerable relationship with the mitochondrial activity in bone healing process. Mitochondria does not only produce energy as ATP units, but also play a critical role in the regulation of inflammation, metabolism and energy supply [11]. One more feature about the mitochondria is called the mitochondrial dynamic which characterized by the ability to fission (Divide) and or fuse (Merge) as a quality control process to maintain the intracellular homeostasis environment surrounding the nucleus. Aging disrupts fusion and fission cycles leading to changing the normal behavior inside the cell [13]. Taken together, understanding the correlation of mitochondria dynamics to the changing pro- and anti-inflammatory state of hematoma might be a key to understand the differences between cell behaviors in aged and young patients. New findings by our collaborator PD. Dr. med, Matthias Hecker of the department of internal medicine II at the university hospital Giessen showed that 18R-HEPE and Resolvin E1 (RvE1) possess anti-inflammatory and anti-apoptotic properties. They can restore inflammation-induced mitochondrial dysfunction by decrease in mitochondrial respiration and membrane potential, furthermore, imbalance of mitochondrial fission and fusion [14]. Fission is controlled by dynamin related protein 1 (Drp1) [15]. Furthermore, inhibition of mitochondrial fission by Mdivi-1 and Dynasore reduces levels of the pro-inflammatory cytokines IL-6 and IL-8. That means we can control the mitochondrial dynamic (fission/fusion) in vitro proportional to inflammation. Furthermore, this is indicative of the potential that lies in investigating the mitochondrial dynamic in aging. In this project, we will collaborate closely with PD. Dr. Hecker as an expert in the field. Furthermore, osteoporosis is one of the most common age-related disease, were fractures are considered a major cause of increased mortality. Therefore, aging patients are encouraged to take prophylactic drugs capable of promoting bone formation and, simultaneously inhibiting bone resorption. Long-term studies showed that Strontium ranelate is an effective compound for chronic treatment of osteoporosis-mediated bone loss [16]. Several studies also showed the efficacy of locally applied strontium on healing of osteoporotic fractures [17-24]. Intriguingly, reports about strontium interaction with mitochondria without exerting a damaging effect as seen with calcium ions [25]. MMMMMMMMMMMMMMMMMMMM Therefore, we will examine the mitochondrial dynamics in mesenchymal stromal cells from aged and young donors under following hypotheses: 1- Young mesenchymal stromal cells show enhanced fission dynamics than old cells. 2- Pro-inflammatory treatment (with tumor necrosis factor (TNF-α)) will induce mitochondrial fission and reduced fusion, which is not favorable for cellular function. 3- Anti-inflammatory treatment (with nonsteroidal anti-inflammatory drugs, Diclofenac sodium), will induce mitochondrial fusion, which is favorable for the cell function. 4- Stimulating aged cells using Strontium ranelate, will rejuvenate cells from old patients by shifting mitochondrial dynamics towards fusion and promote genes regulating energy metabolism. 5- Fission inhibitors (Mdivi-1 and Dynasore) will reverse the effects of pro-inflammatory treatment and reflect upregulation osteogenesis genes. Preparatory work done: The success of fracture healing relies on coordinated overlapping cellular and molecular events. Bone healing is considered as a model system to understand tissue regeneration [25]. Thereby, we first retreated to our microarray data to pinpoint mitochondrial irregular gene expression, whether chronological, temporal or functional changes arises in the course of pathological bone healing. Therefore, we analyzed the healing progression of standard closed femoral fracture in C57BL/6N (age = 8 weeks) wild type male mice model. Fracture callus was assessed at days (D) 3, 7, 10, 14, 21, and 28 post fracture by microarray and histological analysis. Interestingly, microarray analysis of the essential role of mitochondrial genes in the success of bone healing showed a significant downregulation of mitochondrial genes most prominent during the early inflammatory phase. Out of 39 differentially expressed mitochondrial genes, only one single gene was significantly upregulated at onetime point. Crucial genes like Gpx1, Peroxidase 2 (Prdx2) and Peroxidase 3 (Prdx3), that play role against oxidative stress condition were downregulated at D3 and D7. 3-Oxoacid CoA transferase 1 (Oxct1), which plays a central role in ketone body catabolism was significantly downregulated at D3 and D7. Genes like Solute carrier family 25 member 11 (Slc25a11), Solute Carrier Family 25 member 20 (Slc25a20), and Branched chain ketoacid dehydrogenase kinase (Bckdk) that play role in mineral transport and exchange were significantly downregulated at D3 and D7. Other important genes for mitochondrial transport and electron transport chain like Transmembrane proteome 14C (Tmem14c), Atp5b, ATP synthase H+ transporting mitochondrial f1complex (Atp5f1) and Translocase of outer mitochondrial membrane 7 (Tomm7) were significantly downregulated at D3 and D7. Genes like Citrate Synthase (Cs), Fumarate Hydratase 1 (Fh1), Succinyl CoA ligase (Suclg1), Ubiquinol-Cytochrome C Reductase Core Protein 2 (Uqcrc2), and Cytochrome c1 (Cyc1) that are important for energy producing signaling pathways were significantly downregulated at D3 and D7. Coenzyme Q9 (Coq9) which involves lipid biosynthesis for electron transport chain was significantly downregulated during the early phase. Another downregulated gene was Cytochrome P450 family 27 subfamily A member 1 (Cyp27a1) which plays a role in keeping cholesterol homeostasis. Cyp27a1 was significantly downregulated at D3 and D7. Further, there were erythropoiesis regulatory gene like Heat shock protein family a member 9 (Hspa9) and metal binding gene like Iron-Sulfur Cluster Assembly 1 (Isca1). Hspa9 and Isca1 were significantly downregulated at D3 and D7. Cold Shock domain containing protein E1 (Csde1) which acts as RNA binding protein during transcription and translation was significantly downregulated at D3 and D7. Further, glucose and fatty acid metabolism is important for bone homeostasis regulated by gene like Pyruvate Dehydrogenase Kinase 4 (Pdk4), which was significantly downregulated at D3 and D7. Another important gene is Electron transfer flavoprotein alpha subunit (Etfa) which is needed for amino acid metabolism. Etfa was significantly downregulated at D3 and D7. Further, Glutathione S transferase P1 (Gstp1) which links stress kinase and cell apoptotic pathway was significantly downregulated at D3 and D7. Another downregulated gene was Translocase of inner mitochondrial membrane 8 homolog B (Timm8b) which acts as chaperone for protein transport. Timm8b was significantly downregulated at D3 and D7. Genes like Vdac1 and Voltage Dependent Anion Channel 3 (Vdac3) that perform role in diffusion and binding of molecules were also downregulated. Vdac1 was significantly downregulated at D7 and Vdac3 was significantly downregulated at D3, D7, and D21. Further, Carnitine O-palmitoyltransferase 1 (Cpt1b) which acts as a unit for fatty acid beta oxidation was significantly downregulated at D10 and D14. Another downregulated genes were Cytochrome c oxidase subunit 8B (Cox8b), Cytochrome C oxidase subunit 7A1 (Cox7a1), and Cytochrome C oxidase subunit 6A2 (Cox6a2) that are involved in electron transport activity. Cox8b and Cox7a1 were significantly downregulated at D10 and D14. Cox6a2 was significantly downregulated at D10. Another important gene was Creatine kinase S-type (Cktm2) which serves as energy transducer was significantly downregulated from D3 through D7, D10 until D14. Further, carbohydrate metabolism gene like Succinate dehydrogenase cytochrome b560 subunit (Sdhc) was significantly downregulated at D14. Lyr motif containing protein 5 (Lyrm5) which acts as electron transfer flavoprotein regulator was significantly downregulated at D14. Another important gene was Dual Specificity Phosphatase 26 (Dusp26) which acts as an inhibitor of Mapk1 and Mapk3. Dusp26 was significantly downregulated at D14. Heme biosynthesis gene like Solute carrier family 25 member 37 (Slc25a37) was significantly downregulated at D21 and D28. Among upregulated genes, there was molecule exchange factor like Solute carrier family 25 member 5 (Slc25a5), which was significantly upregulated at D10. The drastic downregulation of mitochondrial genes during early inflammatory phase urged the examination of mitochondrial activity at cellular level. Therefore, an antioxidant protein (GPX1) was localized using IHC (Figure 1). The positive signal of GPX1 was examined throughout the fractured callus and specifically in the osteocyte vicinity. Descriptively, GPX1 positive signal was seen in small patches within bone marrow and in callus region (Figure 1A). Histomorphometry showed lower GPX1 positive area at D7 when compared with other time points (Figure 1E). D28 showed higher GPX1 stained area when compared with other time points (Figure 1E). But no significant differences were noted. On the other side, Silver nitrate counter-stained sections showed GPX1 signal within osteocytes and around blood vessels (Figure 1C). GPX1 signal was seen around blood vessels rather than osteocytes at D7. Further, GPX1 positive signal was seen around blood vessels and some patches within osteocytes vicinity at D10. Interestingly, D14 showed higher number of GPX1 signal within osteocytes vicinity than blood vessels (Figure 1C). GPX1 signal was seen in osteocytes vicinity and around blood vessels at D21. GPX1 signal was not seen within osteocytes at D28. Figure 1: Histological analysis of GPX1 and UBB activity during fracture healing showed active positive signal within bone matrix and bone marrow. (A, A´) D28 showed GPX1 stained region around the newly formed bone and bone marrow. (B, B´) D7 showed UBB stained region near to periosteal region and bone marrow. (C) Active osteocyte signals visualized via Silver Nitrate counter-stain within GPX1 positive areas. (D) Positive signal of UBB visualized around blood vessels in the fractured callus via Silver Nitrate counter-stain. (E) GPX1 stained area was higher at D28 compared with other time points. (F) UBB stained area was significantly higher at D7, D10, and D14 when compared with D21. (N = 4 (D7), N = 6 (D10), N = 3 (D14), N = 5 (D21, D28), Ot: osteocytes). These results encouraged us to investigate the major fusion genes of mammalian mitochondria (Mfn1 and Mfn2; Mfn is mitofusin). Intriguingly both genes were down regulated at all time points in the inflammatory and reparative phase and started to upregulate by the beginning of the remodeling phase after bony consolidation at D21 and D28, where the healing process is close to the end (Figure 2). Figure 1: Mitochondrial fusion throughout the healing process in mouse model. The expression of the major mitochondria fusion genes Mfn1 (A) and Mfn2 (B). Both genes were downregulated from D3 to D14 when compared with D0. Upregulation of fusion genes came later after the bony consolidation. Nonetheless, quantification of mitochondria in histological sections is very important. Histological samples are fixed, processed, embedded, and sectioned before being stained; depending on these steps, the outcome of the study is affected. Cells are easily damaged during the long steps of chemical fixation, once analysis under Transmission electron microscope is envisaged. Therefore, we optimized the embedding process by the use of microwave assisted chemical fixation using a PELCO BioWave® Pro microwave (Figure 3). The low energy irradiation produced by the microwave during the fixation, dehydration and resin infiltration enhances the diffusion throughout the samples and improved the preservation quality tremendously [26]. These results showed that microwave technique increases the quality of sample, preserves and enhances ultrastructural microscopy analysis and the samples can also be used for further staining. Figure 3: Microwave Assisted Chemical Fixation (MWCF) improves sample quality. (A) MWCF is enhanced due to radiation, cooling plus vacuum and was used to fix samples. (B) Inferior subcellular structure of bone samples in chemical fixation, Osteocyte with less recognizable subcellular structure. (C) Enhanced ultrastructure in muscle cells. (D) MWCF fixation enhances mitochondrial visualization of osteocyte. Planned methodology: Immediately after approval of the funding, the experiments can be started, since a large part of the required samples is already available. Samples originate from volunteers who visited UKGM for fracture treatment or cruciate ligament graft will be analyzed (Figure 4). The ethics application is already approved. Other patient samples will be additionally acquired until the required number of Figure 4: Schematic illustration of the sample processing plan. samples is reached. Starting with isolated MSCs with pro-inflammatory stimulation (red arrows), anti-inflammatory stimulation (green arrows) and applied strontium (yellow arrows). Work Package I: Cell seeding, cultivation until confluency and cell profiling Mesenchymal stroma cells (MSCs) will be used in the present study. MSCs are not only able to differentiate into mesenchymal cells, such as osteoblasts, adipocytes and chondrocytes, but also into non-mesenchymal cells including endothelial cells and neural cells [27]. Cells will be transferred to expansion medium (DMEM, 10% FCS and 1% penicillin / streptomycin). They will be incubated at 37°C in a CO2 incubator to allow them to attach to the plastic flask. Cell splitting will take place as they became confluent in a 75-ml culture flask. Cell profiling will be performed using FACS Canto and the following markers CD13, CD45, CD73, CD105, CD166 to confirm that the isolated cells are MSCs. Work Package II: Cell stimulation and differentiation Firstly, we are planning to induce a pro- respectively ant-inflammatory state of the isolated MSCs. Inflammation will be induced with tumor necrosis factor (TNF)-α (10 ng/ml) 1 h before the experiment. Mitochondrial fission inhibitors Mdivi-1 or Dynasore will be added to cell culture 30 min prior to addition of TNF-α in the indicated experiments. Cytokines, growth factors and extracellular matrix (ECM) proteins will be present due to inflammation. These in turn stimulate proliferation of cells and healing [28; 29]. For example, Interleukin-1 (IL-1), an inflammation producer which is mainly secreted by macrophages in the innate immune response; Interleukin-6 (IL-6) an immune response stimulant which is secreted by T cells in the adaptive immune response; both are known to recruit mesenchymal cells [29]. Effects of non-steroidal anti-inflammatory drugs (NSAIDs): Pountos et al. [30] studied the effect of NSAID on MSCs proliferation and osteogenic and chondrogenic differentiation and evaluated both cyclooxygenase (COX)-1 and COX-2 specific drugs. They tested the effects of seven COX-1 and COX-2 inhibitors on MSC proliferation and osteogenic and chondrogenic differentiation. The MSC expression of COX1 and COX-2 and prostaglandin E2 (PGE-2) levels were evaluated by PCR and ELISA. They found that none of the NSAIDs significantly affected MSC proliferation. Only MSC chondrogenic was affected but not osteogenic differentiation [30]. To investigate the effect of NSAIDs on mitochondria fission. One of NSAIDs will be added to MSCs culture with and without fission inhibitors to study the effect on proliferation and osteogenic chondrogenic differentiation. Proliferation (using fluorescent dye or XTT assay, to measure the number of viable cells), osteogenic (measure the activity of alkaline phosphatase, ALP) and chondrogenic (measure the content of sGAG) differentiation will be analyzed. Prostaglandin E2 (PGE-2) will be measured in the media and compare it with cells without NSAIDs to check the activity of endogenous COX-1 and COX-2. Effect of strontium on aging process in bone regeneration and mitochondrial dynamics Because strontium has a stimulating effect on osteoblast and reduces osteoclast activity as well as a positive effect on the mitochondrial membrane structure, we want to evaluate the effect of strontium on isolated MSCs. Therefore, we will add 5%-10% strontium to the cell culture medium of MSCs from young and old patients. The strontium treated MSCs will not undergo a pro- or anti-inflammatory stimulation, but the osteo- respectively chondogenic differentiation will be performed as described in the next paragraph. Osteogenic differentiation assay Differentiation will be performed in 24 well plates in triplicates with a control. Starter cell density will be 2.4 x 104 cells in a 400 µl total volume of expansion medium per well, and cells will be allowed to adhere for 48 hours. The first day of adding the differentiation medium is considered day one. Osteogenic differentiation medium (ascorbic acid phosphate, β-glycerophosphate, water-soluble Dexamethasone) will be changed twice weekly. To test cell viability the 3-(4, 5-dimethylthiazol-2-yl)-5-(3-carboxymethoxyphenyl)2-(4-sulfophenyl)-2H-tetrazolium (MTS) test will be used. Osteogenic differentiation will be then evaluated visually by Von Kossa staining. Thereby, silver ions (one of the stain components) bind to the phosphate adsorbed in the extracellular matrix and form silver phosphate; which degrades to silver under light illumination. Calcium is measured by alizarin red, the stain is then extracted (bleached) using cetylpyridinium chloride. Subsequently dissolved color is measured at a wavelength of 405 nm by a microtiter platereader (TECAN, Genius – Maennedorf, Germany). Chondrogenic differentiation assay One million MSCs at passage 2 will be centrifuged at 200 g for 5 min and the pellets will be cultured in 15 ml conical tubes containing 1 ml of chondrogenic differentiation medium consisting of DMEM, 1× ITS, 100 nM dexamethasone, 50 mg/l ascorbic acid, and 5% PL. The medium will be changed twice a week. After 3 weeks, chondrogenic differentiation will be assessed via histochemical staining and RT-PCR. Pellets maintained in DMEM with 5% PL will be used as negative controls [31]. Under the described culture conditions, human MSCs undergo chondrogenic differentiation within 2–3 weeks, producing abundant extracellular matrix composed primarily of cartilage-specific molecules such as type II collagen and aggrecan. The expression of these cartilage markers can be used as evidence of the chondrogenic differentiation of MSCs. Chondrogenic differentiation can be assessed by toluidine blue staining of pellet sections. Effect of Mdivi-1 on mitochondrial fission as inflammatory signal. There are contradictory results regarding the use of Mdivi-1 to inhibit Drp-1 and prevent mitochondrial fission [32]. The review of Smith and Gallo (2017) stressed on further biochemical investigation and the use of stringent positive controls to proof the effect of Mdivi-1 on fission. Work Package III: Histology and TEM Following the MSC stimulation and differentiation, histological examination will be performed to verify the regenerative state of bone and mitochondrial state as a reaction to the pro- and anti-inflammatory treatment. Therefore, the cells will be transferred onto glass slides using the Cytospin system: MSCs will be trypsinized and collected in 15 ml conical tubes. Cell number will be determined, centrifuged and resuspended in PBS at a concentration of 5 x 105/ml. Subsequently, 200 µl of cell suspension will be centrifuged on glass microscope slides using a cytospin centrifuge. Afterwards, the cells will be fixed with 4% paraformaldehyde in NaPo 4 buffer and dried overnight to be ready for histological staining [33]. Immunohistology Immunohistochlogy will be performed to detect osteo-anabolic (BMP2, OCN) and osteocatabolic markers (OPG, RANKL). Chondrogenic differentiation can be evaluated using Immunohistochemical staining of serial sections of pellet sections such as Type I collagen, type II collagen, type X collagen, TNF-a, DRP1, Fis1, Mfn1 and Mfn2. Transmission Electron Microscopy (TEM) For the TEM analysis samples will be collected directly and fixed in 2% (wt/v) paraformaldehyde and 2% (w/v) glutaraldehyde in 0.05 M cacodylate buffer in a laboratory microwave assisted chemical fixation (Ted Pella, Inc, Model PELCO BioWave® 34700230). Fixation will be done in four times under continuous vacuum of 15 mm Hg for 8 min, a radiation power of 150 Wattage will be alternately applied between the fixation steps. Then samples are washed with 50 mM cacodylate buffer four times using radiation power of 150 Wattage for 2 min each without vacuum. After washing samples are dehydrated in ascending series of ethanol: 30, 40, 50, 75, 90, 100% (vol/vol) ethanol in ddH2O with radiation power of 15 mm Hg for 2 min each then in propylene oxide for 2 min with radiation power of 15 mm Hg without vacuum. Sample infiltrate in ascending series of Spurr’s resin mixed with propylene oxide takes place before embedding in 100% Spurr’s resin for 24 hours. The process will achieve fixation and embedding in 36 hours therefore, saving 97% of the 6-8 weeks long embedded methyl methacrylate. Work Package IV: Molecular biology Molecular analysis will be performed to determine the bone regenerative capacity as well as the mitochondrial state as a response to the different treatments. Therefore, we will use different technics like PCRs and NGS. qRT-PCR: RNA will be isolated from cultured MSCs of all groups under different treatments and treatments combinations. It will be used as templet for cDNA synthesis. Quantitative realtime PCR will be used for expression analysis. The following genes will be analyzed: Anti-inflammation genes: COX-1, COX-2, to check if there is chondrogenesis inhibition. Anti-inflammation genes: IL-6, IL-8 to check the effect of TNF-α. Transcription factors: Runx2 and Sox-9 triggers of osteogenesis and chondrogenesis, respectively. Mitochondrial fission genes: Fis1 (promoter of mitochondrial fission), DRP1 (fission process). Under inflammation should be increased Mitochondrial fusion genes: OPA1, MFN1, MFN2. Under inflammation should be decreased. Effect Wnt signaling pathway: dKK, Sost House-keeping gene: GAPDH NGS: RNA isolation will be performed using NGS Tool Kit, Takara SMARTer® Ultra® Low Input RNA for Illumina® Sequencing – HV according to manufacturer’s protocol. Next generation sequencing will be performed at the university core facility after applying the prepared RNA on the NGS-chip according to manufacturer’s protocol. The NGS data are then analyzed using bioinformatics tools with focus on the coding components. The analysis will run using R packages such as Bioconductor for NGS data analysis. The main goal is to form enrichment maps to understand network analysis between the genes associated in bone, fat metabolism and mitochondria. ELISA: (collaboration) Concentrations of interleukin-6 (IL-6) and -8 (IL-8) in cell culture supernatants will be measured by ELISA. To correlate the presence of TNF-α with the level of IL-6 and IL-8 in presence and absence of strontium. Microarray, protein array and western blot: (collaboration) Microarray: The human mitochondrial genome is circular with 16,569 base pairs and encodes 37 genes coding for 22 transport RNAs, 2 ribosomal RNAs, and 13 messenger RNAs [34]. Microarray is used to study alterations of mitochondrial and nuclear gene expression in healthy and diseases samples. Commercially available mitochondrial array will be used. Protein array: Proteins will be extracted from different treatments with and without inflammatory conductions and will be applied on available protein arrays i.e. stress-related proteins and apoptosis-related proteins. Western blot: WB will be performed using specific antibodies to check the expression or repression for FIS1, DRP1, MFN2 and β-actin (house-keeping protein): with/without TNFα; with/without strontium; with/without Mdivi1. Work Package V: Bioinformatics Quantitative immunohistological evaluation will be done semi-automated using ImageJ software (1,52k) to quantify the mitochondrial and regenerative state after treatment and differentiation. The NGS raw data will be analyzed using the R project for Statistical Computing. Quality assessment of array data will be carried out by calculating Pearson’s correlation coefficient between arrays and fold Change (FC) will be calculated as the differences between each treatment. Clustering of genes will base on the expression pattern identifies co-regulated and functionally related genes. Hierarchical clustering method using R (version 3.0.3) and Bioconductor packages will be implemented to obtain set of differentially expressed genes with similar expression profile. An online server; Database for Annotation, Visualization and Integrated Discovery (DAVID) bioinformatics database (version 6.7, https://david.ncifcrf.gov/) provides an integrated and updated information about the involved molecular function, cellular component, and biological processes for gene of interest. Furthermore, DAVID provides an option of functional annotation clustering to cluster functionally similar terms associated with gene list. Conclusion The aim of this research proposal is to unravel the mechanisms underlying modulation of endogenous regeneration due to aging, with a focus on mitochondrial network dynamic in vitro. Special attention is given to the response of mesenchymal stromal cells to pro- and antiinflammatory stimulants and in response to prophylactic drugs. Publications 1. El Khassawna T, Serra A, Bucher CH, Petersen A, Schlundt C, Könnecke I, Malhan D, Wendler S, Schell H, Volk H-D, Schmidt-Bleek K, Duda GN: T Lymphocytes Influence the Mineralization Process of Bone. Front Immunol 2017, 8. [doi: 10.3389/fimmu.2017.00562] 2. El Khassawna T, Bocker W, Brodsky K, Weisweiler D, Govindarajan P, Kampschulte M, Thormann U, Henss A, Rohnke M, Bauer N, Muller R, Deutsch A, Ignatius A, Durselen L, Langheinrich A, Lips KS, Schnettler R, Heiss C. Impaired extracellular matrix structure resulting from malnutrition in ovariectomized mature rats. Histochem Cell Biol. 2015 [doi: 10.1007/s00418-015-1356-9] 3. Schlundt C*, El Khassawna T*, Serra A, Dienelt A, Wendler S, Schell H, van Rooijen N, Radbruch A, Lucius R, Hartmann S, Duda GN, Schmidt-Bleek K. Macrophages in bone fracture healing: Their essential role in endochondral ossification. Bone. 2015. (Equal contribution) doi: 10.1016/j.bone.2015.10.019.] 4. El Khassawna T, Bocker W, Govindarajan P, Schliefke N, Hurter B, Kampschulte M, Schlewitz G, Alt V, Lips KS, Faulenbach M, Mollmann H, Zahner D, Durselen L, Ignatius A, Bauer N, Wenisch S, Langheinrich AC, Schnettler R, Heiss C. Effects of multideficiencies-diet on bone parameters of peripheral bone in ovariectomized mature rat. PLoS One. 2013. [doi: https://doi.org/10.1371/journal.pone.0071665] 5. El Khassawna T. Cellular and molecular analysis of fracture healing in a neurofibromatosis type 1 conditional knockout mice model [https://doi.org/10.18452/16781] Collaboration with other scholars: Prof. Klaus D Jandt Prof. Dr.-Ing. Peter Czermak Univ.-Prof. Dr. med. Christian Heiß Lehrstuhl für Materialwissenschaft, Otto-Schott-Institut für Materialforschung, Friedrich-Schiller-Universität Jena Technische Hochschule Mittelhessen Prof. Dr. Katrin Susanne Lips Univ. Prof. Dr. Ing. Georg Duda Klinik und Poliklinik für Unfall-, Handund Wiederherstellungschirurgie, Justus-Liebig-Universität Gießen Klinik und Poliklinik für Unfall-, Handund Wiederherstellungschirurgie, Justus-Liebig-Universität Gießen Justus Liebig Universität Gießen Julius Wolff Instiut, Universitätmedizin Charite, Berlin Prof. Kurosch Rezwan University Bremen, Department 4, Advanced Ceramics Prof. Michael Gelinsky Zentrum für Translationale Knochen-, Gelenk- und Weichgewebeforschung, TU Dresden Klinik und Poliklinik für Kinder- und Jugendmedizin, TU Dresden Physikalisch-Chemisches Institut, JLU Gießen Leibniz University Hannover, Institute for Multiphase Processes Medizinische Klinik V, Labor für Myelomforschung, UK Heidelberg Prof. Dr.med. Volker Alt Prof. Angela Rösen-Wolff Prof. Jürgen Janek Prof. Birgit Glasmacher Dr. Dirk Hose References: [1] Jakob F, Seefried L, Schwab M. [Age and osteoporosis. Effects of aging on osteoporosis, the diagnostics and therapy]. Internist (Berl). 2014;55:755-61. [2] Botolin S, McCabe LR. Bone loss and increased bone adiposity in spontaneous and pharmacologically induced diabetic mice. Endocrinology. 2007;148:198-205. [3] Opal SM. Phylogenetic and functional relationships between coagulation and the innate immune response. Crit Care Med. 2000;28:S77-80. [4] Park SH, Silva M, Bahk WJ, McKellop H, Lieberman JR. Effect of repeated irrigation and debridement on fracture healing in an animal model. J Orthop Res. 2002;20:1197204. [5] Mizuno K, Mineo K, Tachibana T, Sumi M, Matsubara T, Hirohata K. The osteogenetic potential of fracture haematoma. Subperiosteal and intramuscular transplantation of the haematoma. J Bone Joint Surg Br. 1990;72:822-9. [6] Street J, Winter D, Wang JH, Wakai A, McGuinness A, Redmond HP. Is human fracture hematoma inherently angiogenic? Clin Orthop Relat Res. 2000:224-37. [7] Xing Z, Lu C, Hu D, Miclau T, 3rd, Marcucio RS. Rejuvenation of the inflammatory system stimulates fracture repair in aged mice. J Orthop Res. 2010;28:1000-6. [8] Mountziaris PM, Mikos AG. Modulation of the inflammatory response for enhanced bone tissue regeneration. Tissue Eng Part B Rev. 2008;14:179-86. [9] Schmidt-Bleek K, Schell H, Lienau J, Schulz N, Hoff P, Pfaff M, Schmidt G, Martin C, Perka C, Buttgereit F, Volk HD, Duda G. Initial immune reaction and angiogenesis in bone healing. J Tissue Eng Regen Med. 2014;8:120-30. [10] Krauss S, Brand MD, Buttgereit F. Signaling takes a breath--new quantitative perspectives on bioenergetics and signal transduction. Immunity. 2001;15:497-502. [11] Harrois A, Huet O, Duranteau J. Alterations of mitochondrial function in sepsis and critical illness. Curr Opin Anaesthesiol. 2009;22:143-9. [12] Twig G, Elorza A, Molina AJ, Mohamed H, Wikstrom JD, Walzer G, Stiles L, Haigh SE, Katz S, Las G, Alroy J, Wu M, Py BF, Yuan J, Deeney JT, Corkey BE, Shirihai OS. Fission and selective fusion govern mitochondrial segregation and elimination by autophagy. EMBO J. 2008;27:433-46. [13] Seo AY, Joseph AM, Dutta D, Hwang JC, Aris JP, Leeuwenburgh C. New insights into the role of mitochondria in aging: mitochondrial dynamics and more. J Cell Sci. 2010;123:2533-42. [14] Hecker, M., Sommer, N., Foch, S., Hecker, A., Hackstein, H., Witzenrath, M., Weissmann, N., Seeger, E., Mayer, K. Resolvin E1 and its precursor 18R-HEPE restore mitochondrial function in inflammation. BBA Molecular and Cell Biology of Lipids. 2018; 1863: 1016-1028[15] Smith, G. and Gallo, G. To mdivi-1 or not to mdivi-1: is that the question? Dev Neurobiol. 2017; 77(11): 1260-1268. [15+1] Ray S, Thormann U, Sommer U, El Khassawna T, Hundgeburth M, Henß A, Rohnke M, Lips KS, Heiss C, Heinemann S. Effects of macroporous, strontium loaded xerogel-scaffolds on new bone formation in critical-size metaphyseal fracture defects in ovariectomized rats. Injury. 2016;47:S52-S61. [16] Thormann U, Ray S, Sommer U, ElKhassawna T, Rehling T, Hundgeburth M, Henß A, Rohnke M, Janek J, Lips KS. Bone formation induced by strontium modified calcium phosphate cement in critical-size metaphyseal fracture defects in ovariectomized rats. Biomaterials. 2013;34:8589-98. [17] Thormann U, Ray S, Sommer U, El Khassawna T, Heiss C, Schnettler R, Alt V. Biomaterials for enhancement of bone healing in osteoporotic fractures. BioNanoMaterials. 2013;14:135-42. [18] Marie PJ. Strontium ranelate: New insights into its dual mode of action. Bone. 2007;40:S5-S8. [19] Atkins GJ, Welldon KJ, Halbout P, Findlay DM. Strontium ranelate treatment of human primary osteoblasts promotes an osteocyte-like phenotype while eliciting an osteoprotegerin response. Osteoporos Int. 2009;20:653-64. [20] Caverzasio J. Strontium ranelate promotes osteoblastic cell replication through at least two different mechanisms. Bone. 2008;42:1131-6. [21] Maimoun L, Brennan TC, Badoud I, Dubois-Ferriere V, Rizzoli R, Ammann P. Strontium ranelate improves implant osseointegration. Bone. 2010;46:1436-41. [22] Ammann P, Shen V, Robin B, Mauras Y, Bonjour JP, Rizzoli R. Strontium ranelate improves bone resistance by increasing bone mass and improving architecture in intact female rats. J Bone Miner Res. 2004;19:2012-20. [23] Tashmukhamedov B, Gagel’gans A. Strontium and Animal Mitochondria: The Interaction of Strontium Ions with Mitochondria in Animal Tissues. Handbook of Stable Strontium: Springer; 1981. p. 213-37. [24] Schmidt-Bleek K, Petersen A, Dienelt A, Schwarz C, Duda GN. Initiation and early control of tissue regeneration – bone healing as a model system for tissue regeneration. Expert Opinion on Biological Therapy. 2014;14:247-59. [25] Daghma DES, Melzer M, Malhan D, Hassan F, Stoetzel S, Kojonazarov B, Schermuly RT, Heiss C. Enhanced ultrastructure preservation of undecalcified bone samples using non-ionized microwave radiation. Jornal of Bone Reports. 2019;accepted. [27] Kopen, G. C.; Prockop, D. J. and Phinney, D. G. Marrow stromal cells migrate throughout forebrain and cerebellum, and they differentiate into astrocytes after injection into neonatal mice brains, Proc Natl Acad Sci U S A. 1999; 19: 10711-6 [28] Probst, A. and Spiegel, H. U. (1997): Cellular mechanisms of bone repair, J Invest Surg. 1997;10(3): 77-86 [29] Pittenger, M. F.; Mackay, A. M.; Beck, S. C.; Jaiswal, R. K.; Douglas, R.; Mosca, J. D.; Moorman, M. A.; Simonetti, D. W.; Craig, S. and Marshak, D. R. (1999): Multilineage potential of adult human mesenchymal stem cells, Science. 1999; 284(5411): 143-7 [30] Pountos I, Giannoudis PV, Jones E, English A, Churchman S, Field S, Ponchel F, Bird H, Emery P, McGonagle D. NSAIDS inhibit in vitro MSC chondrogenesis but not osteogenesis: implications for mechanism of bone formation inhibition in man. J. Cell. Mol. Med. 2011; 15(3): 525-534 [31] Solchaga LA, Penick KJ, Welter JF. Chondrogenic Differentiation of Bone MarrowDerived Mesenchymal Stem Cells: Tips and Tricks. Methods Mol Biol. 2011; 698: 253– 278 [32] Bordt EA, Clerc P, Roelofs BA, Saladino AJ, Tretter L, Adam-Vizi V, Cherok E, Khalil A, Yadava N, Ge SX, Francis TC, Kennedy NW, Picton LK, Kumar T, Uppuluri S, Miller AM, Itoh K, Karbowski M, Sesaki H, Hill RB, Polster BM. The Putative Drp1 Inhibitor mdivi-1 Is a Reversible Mitochondrial Complex I Inhibitor that Modulates Reactive Oxygen Species. Dev Cell. 2017; 40:583–594 [33] Koh CM. Preparation of cells for microscopy using cytospin. Methods in Enzymology, 2013 [34] Voss JG, Raju R, Logun C, Danner LR, Munson PJ, Rangel Z and Dalakas MC. A Focused Microarray to Study Human Mitochondrial and Nuclear Gene Expression. Biol Res Nurs. 2008; 9(4): 272–279.