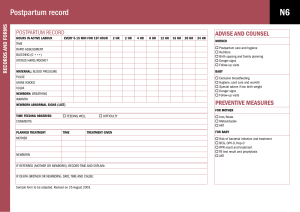
Unit 1 Objectives Quick book references & learning assignments: (Don't fill these out) Ricci, S. (2021) Essentials of maternity, newborn, and women’s health nursing (5th Ed): Philadelphia: Wolters Kluwer. ● Neonatal Assessment: Chapter 18, pp 582-620 ● Newborn Medications: Chapter 18 pp 588-590 o Completion of Newborn Medications Templates PRIOR to class ● Postpartum Adaptations: Chapter 15, pp 498-513 ● Nursing Assessment in the Postpartum Client: Chapter 16, pp 520-534 ● Assisting with screening tests: Chapter 18 pp 615-617 ● CCHD Screening: current recommendations ● Laboratory Tests in Pregnancy: Chapter 12, pp 376-377 and Table 12.1 ● Rh Status: Chapter 16, p 547-548 ● Blood Incompatibility: Chapter 19, pp 674-675 ● Resulting jaundice in the newborn with blood incompatibility: Chapter 24, pp 890895 ● Rubella: Chapter 20, pp 717-718 ● Hepatitis B Virus: Chapter 20 pp 719-720 ● Group B Beta Strep: Chapter 20, pp 721-722 ● Providing Immunizations: Chapter 16. P 547 Lesson 1: Nursing Assessment of the Well Newborn 1. Describe the sequence to follow in the assessment of the newborn. https://youtu.be/cracmPo3iYo https://youtu.be/pXrGIZOLz4k (registered nurse RN) Skin: general appearance, color, transient cutaneous lesions, birthmarks Cardiopulmonary: rate(110-160bpm, ALWAYS count 1 full minute at the apex), murmurs? Asses brachial and femoral pulses, assess cap refill Respiratory: rate(30-60 breaths/min. ALWAYS count 1 full min, shape(round+symmetric), movement(chest+abd move in synchrony), breathing patterns (periodic; irregular and varying depths along with the newborn having 5-10seconds w/o breathing IS NORMAL) Head assessment: 33-37 cm (13-14 in) -General appearance(size, shape, symmetry) -Sutures(sutures should be flat and FLEXIBLE) -Fontanelles: Shape is same on ALL, size may vary, bulging/tense are assoc. w/ illness, depressed= late sign of dehydration -Observe for abrasions, lacerations, bruising: typically related to labor procedure, rapid second stage, presentation, or birth trauma… facial+scalp bruising increase risk for hyperbilirubinemia due to RBC breakdown from bruise and immaturity of the liver, building up and creating a jaundice(yellow) look to the baby Face assessment: EYES: edema in eyelids is common, WHITE sclera, absent drainage, blink reflex EARS: where do the ears set?.. preauricular skin tags and dimples are common(may suggest renal malformations though).. hairy ears common in infants of diabetic mothers NOSE: patency(unlabored breathing, do not occluded nare) and sneeze reflex MOUTH/LIPS: lips are sense touch, baby should demonstrate "ROOT" reflex, lips+buccal mucosa are PINK, gloved finger to assess hard and soft palates for cleft palate AND to asses suck/swallow reflex… tongue(freely mobile).. cry (LOUD, LUSTY & moderate pitch) NECK: ROM (by stroking infants cheek), gently palpate masses, assess for webbing, clavicle intactness and straightness, assess nape of the neck for "stork bite" Chest assessment: breast enlargement is secondary to effects of maternal estrogen, may secrete "witches milk" and has no clinical significance inspect : Flat, concave? (Pectus excavatum) Convex? Pectus carinatum more common in some connective tissue and cardiac disorders cardiac Apical 110-160 newborn Circumference 30-33 cm (12-13 in newborn) Abdomen assessment: inspect(mildly protuberance and softly rounded), consistency is SOFT, bowel sounds present 30-60minutes after birth -umbilical assessment; assess for discharge, redness, odor, edema around the base of the cord for omphalitis (infection).. cord clamp is present or removed Genitalia: -female: fully enclosed within labia majors.. 2 types of discharge common(pseudomenstruation; slightly bloody r/t increased estrogen levels in intrauterine environment…. Smegma; white mucus discharge that is the result of leukocytosis of pregnancy) -male: glans completely covered by foreskin.. scrotum(length+rugae).. palpate for testes Anus: assess for imperforate anus.. definitive assessment of anal latency is the first stool Extremities: ARMS: ROM(full +uncoordinated), color (pink), muscle tone("strong" is infant resists abduction of arms), position: flexed HANDS: position(clenched), # of digits (abnormal: polydactyly, syndactyly), # of creases (3 distinct creases), color (PINK, however may have acrocyanosis), reflexes(palmer grasp), nail length(at or past fingertips) LEGS: ROM(full, uncoordinated), color(pink), muscle tone( "strong" if infant resists abduction), position (flexed) FEET: # of toes, creases, color(pink, however, may have acrocyanosis), reflexes(plantar grasp, babinski) Back: observe for abnormal spine curvature, gross defects, evidence of spina bifida… assess the pilonidal sinus (dermal sinus) for complete closure.. assess gluteal folds for symmetry.. NURSES DO NOT PERFORM BARLOW MANEUVER OR ORTOLANI MANEUVER Neonatal neurological exam: behavioral state assessment (deep sleep, light sleep, drowsy, quiet alert, active alert, crying…. Normal term newborns move from one state to the next with a smooth transition in response to appropriate stimuli) 2. Perform the assessments needed during the immediate newborn period. APGAR- https://youtu.be/cQKaTCMFjwc Perform 1minute immediately after birth, then again at 5 minutes and may require a recheck at 10 minutes(if 5 min score is less than 7) to determine which infant resuscitation intervention is needed depending on score of assessment Score of 8-10 normal no intervention 4-7 moderate difficulty 3 below distress APGAR 1 &5 min 0 - poor response 1- 2- normal response Appearance - color cyanotic /pale Acrocyanosis (blue extremities) Pink all over Pulse heart rate most impt absent Less 100 Higher 100 Grimace - reflex irritability No response Grimace or frown when irritated Sneeze, cough, vigorous cry Activity (muscle tone) Limp flaccid Some flexion Limited resistance to extension Tight flexion, good resistance to extension; good return to flexed position Respiratory(effort) apneci Slow irregular shallow Regular 30-60 breath per min Strong / good cry 3. Describe the normal physical and behavioral characteristics of the newborn. Normal Physical: ● skin: soft, smooth, opaque and warm color consistent with genetic background … normal variants ○ vernix caseosa - thick white film that protects skin of fetus, found first 2-3 days, leave ○ petechiae of head and neck, ○ dry/peeling skin transient cutaneous lesions: ○ benign variants; ■ Milia - white heads, unopened sebaceous gland dissapear in 2-4 weeks ■ Epstein pearls - milia in mouth and gums ■ hyperplasia, ■ erythema toxicumnewborn rash resembling flea bites late gray, macular hemangioma, petechiae ● skin color: all newborns are PINK with some variations of plethora, jaundice, pallor,cyanosis, bruising ● common birthmarks: Port wine stain(does not disappear), Hemangioma (2 types: cavernous and strawberry…. Many regress on own, others require laser therapy) Birthmarks are not common/expected on the face. ● Face ○ Full cheeks, features symmetrical ● Eyes ○ Same as adult (symmetrical, PERRL, tract objects to midline) ■ Birth may cause eyelid edema, subconjunctival hemorrhages ● Ears ● ● ● ● ● ○ Soft, pliable, quick recoil when folded & released, patent. Nose ○ Small & narrow, Midline, patent, intact septum Mouth ○ Symmetrical, midline, intact hard and soft palate Neck ○ Short, creased, moves freely, baby holds head midline. Chest ○ Round “barrel chest”, symmetrical, smaller than head. Extremities & spine ○ Symmetric, free movement, spine midline. Newborn Vitals: (This list assumes baby is full term) Temp 97.7 - 99.5 F (37 c +/- 0.5) axillary (rectal not used now due to perforation risk) Heart rate (pulse) 110-160bpm up to 180 while crying Respirations : 30-60 breaths per min at rest Blood pressure (Not normally performed, only done if clinical indication or low apgar score) ● 50-75 mm Hg systolic/ 30-45 mmHg diastolic crying, moving, delayed clamping will increase systolic pressure ● Full term newborn measurements: Usual findings ○ Head circumference - 33-37cm ○ Chest circumference - 30-33 cm ○ Weight - 2,500-4,000 g (5.5-8.5 lb) ○ Length - 45-55 cm (19-21 in) Head variants: molding, caput succedaneum, cephalhematoma, craniosynostosis ● Normal behavioral characteristics: ○ The newborn (initially) should be alert and not persistently lethargic. ■ Deep sleep, light sleep, drowsy, quiet alert, active alert, crying, self comforting skills (hand to mouth)… an infant should be able to demonstrate all 7 behavioral states in the hospital stay 4. Recognize deviations from normal physiologic and behavioral findings during the examination of the newborn. ● Abnormal physiological: ○ Skin: ■ Jaundice, acrocyanosis, milia, mongolian spots, stork bites, port wine stains, erythema toxicum, harlequin sign Cardiopulmonary: Respiratory: - "see-saw" breathing patterns indicate newborn is using intercostal muscles to breathe and is experiencing respiratory distress - Apnea: >20seconds w/o breathing infant goes cyanotic -Respiratory distress: Tachypnea, substernal or intercostal retraction, grunting on expiration, nostril flaring, cyanosis ● Head: ○ Microcephaly - head circumference below average/expected gestational age. ■ More serious/clinically significant than macrocephaly ○ Macrocephaly - Head circumference above average/expected gestational age ■ Often benign ● ● ○ Face: ○ Enlarged fontanelles Facial nerve paralysis, nevus flammeus (“Port wine stain” on face), nevus vasculosus (“strawberry” on face) Abdomen: ○ Infection signs in umbilicus, distended, only two vessels in umbilical cord (three is normal) ● Genitalia: ○ -males: hypospadias(incomplete formation of anterior urethra resulting in urethral meatus forming on ventral shaft of penis.. ¹/³⁰⁰ male infants)... Chordee (prescience of fibrotic tissue that causes ventral curvature of the erect penis… Cryptorchidism (undescended testicles, usually resulting in infertility... descent normally occurs 7th and 9th month of gestation). Impalpable testes. Any bulging, discoloration, edema. ○ Females - Discharge or pseudomenstruation (though its common) ● Anus: ○ Anal fissures/fistulas, no meconium passed within 24 hours of birth. ARMS: ○ Non-symmetrical, ROM issues HANDS: ○ polydactyly (6+), syndactyly(4 or less), simian crease (singular crease) is seen in infants w/ chromosomal + congenital abnormalities (three creases is considered normal) ○ LEGS & HIPS ○ Non-symmetrical, ROM issues ○ developmental dysplasia of the hip (use Ortolani and Barlow maneuvers to assess) FEET: ○ Club footing, unequal length or non-symmetrical skinfolds. Back: ○ Tuft or dimple on spine (tethered cord) ● ● ● ● ● 5. Discuss/describe the neurologic and neuromuscular characteristics of the newborn and describe normal newborn reflexes. https://youtu.be/rHYk1sYsge0 (reflexes Registered nurse RN) Newborn Reflexes Reflex Appearance Disappearance Stepping Birth 1-2 mo grasp nb 3-4 mo Tonic Neck (fencing) NB 3-4 Mo Moro (startle) NB 3-6 mo Rooting Birth 4-6 mo Babinski Sign NB 12 mo *Blinking NB persists *Sneeze NB persists *Gag Reflex nb persists *Cough Nb persists *protective reflexes 6. Describe the behavioral adaptations of the newborn, including periods of reactivity and sleep-wake states. Lesson 2: Postpartum Physical Assessment https://youtu.be/DzVhumIrqd0 1. Describe the sequence to follow in the assessment of the postpartum patient. BUBBLE-HE Breasts: Texture and consistency.. Redness/pain.. Nipple assessment Uterus: Fundus Location(midline or deviated to the right).. Fundus height(measured in fingerbreadths above/below umbilicus)..Fundus consistency(firm or boggy) Bowel: Rate..4 quad assessment..Provide pt. teaching to prevent/minimize constipation Bladder: is the pt. voiding adequately? Is there s/s of UTI? (pain/burning w/ voiding or normal/steady stream?) Lochia: Amount (scant,light,mod., heavy).. Color(Rubra, serosa, alba)// Odor?.. clots?.. Documentation of lochia Episiotomy: Evidence of infection?(REEDA).. Hemorrhoids?.. Pt. teaching regarding peri care Homan’s sign: ● Reflexes ● Edema ● Homan’s ● Clonus ● Capillary refill ● Pedal pulses Emotional: ● Mother’s general attitude, feelings of competence, supportive systems, and caregiving skill ● Evaluates fatigue and ability to accomplish developmental task ● Describe level of attachment to infant ● Determine mothers phase of adjustment to parenting Epidural: Assess epidural/spinal site for hematoma formation and S/S of infection and drainage Lesson 3: Newborn Screening 1. Explain the purposes for newborn metabolic screening. ● To identify NB who appears healthy but could be at risk of developing conditions with severe complications if left untreated. ● Most common screened below: ● ● ● ● PKU - inherited deficiency in enzyme necessary for metabolism of phenylalanine to tyrosine (amino acid found in most food) done 24-48 hours after protein feeding - Heel stick Congenital hypothyroidism - deficiency of thyroid hormone necessary for brain growth, calorie metabolism, done between 4-6 days, if untreated irreversible brain damage and intellectual disability before age 1 Galactosemia - absence of enzyme needed for the conversion of hte milk sugar galactose to glucose - done on discharge with followup test at 1 month Sickle cell anemia - recessively inherited abnormality in hemoglobin structure, most commonly found in African American newborns. Bloodspot obtained at same time of other nb screening tests or prior to 3 months of age. 2. Explain the purposes for a newborn hearing screening. (614-15) ● Most common birth disorder in US ● Delays in identifying hearing loss may affect language development, academic performance, and cognitive development ● Detection before 3 months greatly improves outcomes- can prevent severe psychosocial, educational, and language development delays ● 50% of infants with hearing loss have no known factors 3. Explain procedure and purposes for Critical Congenital Heart Disease Screening (CCHD). ● CCHD is a group of the 7 most severe congenital heart diseases ● Pulse oximetry screening will most likely detect the 7 critical CCHD ● Purpose of the screening is if an anomaly is identified prenatally, the parents can decide whether or not to continue the pregnancy. If after birth parents can be nformed promptly and given a realistic appraisal of the severity of the condition, the prognosis, and treatment options 4. Review procedures for performing a heel stick. ● Newborn Screening Blood Specimen Collection ● 5. Review procedures for atraumatic care of the newborn during invasive procedures. a. Lesson 4: Laboratory Values in the Pregnant/Postpartum Client 1. Explain the purposes for drawing critical lab values in the pregnant and postpartum client. a. Tests are generally ordered during the initial visit so that baseline data can be obtained, allowing for early detection and prompt intervention if any problems occur. Additional tests may be needed or suggested based on health status, exam findings, risk factors such as genetic diseases. Ultimately it is the choice of the patient. b. Ongoing/followup lab tests help achieve positive outcomes and identify potential issues such as gestational diabetes, anemia (hemoglobin/hematocrit) Rh-negative antibody titers in the mother (rhogam is given if indicated) c. Late pregnancy (37-40 weeks) group b streptococcus, gonorreia, chlamydia tests are performed due to infantile risks including newborn blindness. 2. Explain the variations of acceptable lab values for the pregnant and postpartum client. (**)CBC VALUES TO KNOW!!!.... (--)Other important labs to know Non pregnant Pregnant **Hemoglobin (Hgb) 12-16g/dl 11.5-14g/dl **Hematocrit (Htc) 37-47% 32-42% **WBC 4500-10,000 mm3 5000-15,000 (Postpartum WBC can be 25,000-30,000 and be normal) **Platelets 150,000-350,000 mm3 150,000-350,000 mm3 STAYS THE SAME (Increases 3-5 days after delivery before gradually dropping.) **Plasma volume Increases in pregnancy 12-13 U 4-32 U -- ALT(SGPT) 7-41 2-25 -- 24hr Urine protein/creatinine <300 g of protein <0.3 -- Serum creatinine 0.5-0.9 0.4-0.9 Aspartate Aminotransferase aka (-- AST(SGOT) (Liver enzyme) 3. Explain the ABO blood group in determining ABO incompatibility and the impact on the neonate. ABO incompatibility increases the risk of hyperbilirubinemia in the newborn.. It is less severe than Rh incompatibility Usually occurs with an incompatibility, mother is type O with an anti-A and Anti-B antibodies in her blood, infant will be blood type A, B or AB 4. Explain the Rh sensitization process and the impact on the neonate. a. Simple explanation: Mom is Rh - and has a Rh + baby and there is an incompatibility issue with the blood between the mom and baby.. Mom typically has to take a medication so she does not miscarry. i. The risk is significantly higher in the second pregnancy. 5. Explain the purpose of determining rubella immunity in the prenatal period and the implications of the newborn with rubella exposure in non-immune mothers. Determine prevention strategies for future pregnancies. Risk of congenital rubella syndrome in pregnancy, greatest risk in the first trimester which can lead to hearing loss, eye defects, CNS abnormalities such as microcephaly, heart defects such as PDA and pulmonary artery stenosis. -Women who are rubella non immune should receive the vaccine after delivery and before DC from hospital Newborn Medicaitons: Phytonadione (Vitamin K) ((Aqua-Mephyton, Konakion, Mephyton)) ● Action: Provides NB with Vitamin K (necessary for production of adequate clotting factor II, VII, IX, X by liver) during the first week of birth until NB can manufacture it. - deficiency might lead to delayed clotting and hemmorhage ● Action Prevents Vitamin K deficiency bleeding (VKDB) of NB ● Nursing Implications: ○ Aminister within 1-2 hr of birth ○ Admin im injection outer middle third vastus lateralis ○ 25 guage , 5/8 in needle ○ Hold firmly inject slowly - std precautions- assess for bleeding after Erythromycin opthalmic ointment 0.5% ● Action : provides bactericidal and bateriostatic actions to prevent Neisseria gonorrhoeae and chlamydia trachomatis conjunctivitis, prevents ophthalmia neonatorum (which can cause neonatal blindness) ● Nursing implications ○ Administer ASAP ○ Be alert for chemical conjunctivitis for 1-2 days ○ Wear gloves, and open eyes by placing tumb and finger above and below eye ○ Gently squeeze the tube or ampule to apply medication into conjunctival sac from the inner canthus to outer ○ Do not touch tip of eye ○ Close eye to make sure med permeates ○ Wipe off excess ointment after 1 min Vitamin D ● 400 IU of vit D starting within the first few days of life to prevent rickets and Vitamin D difficiency ●