")
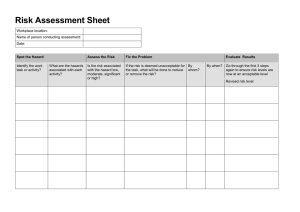
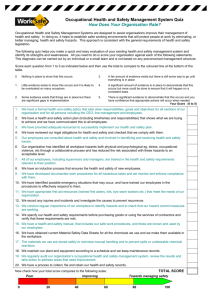
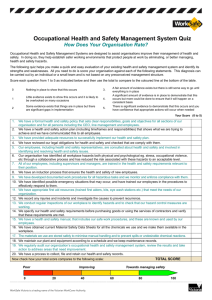
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/231315785 Workplace Risk Assessment Chapter · January 2010 CITATIONS READS 0 3,376 4 authors, including: Elisaveta Stikova Neda Milevska-Kostova Ss. Cyril and Methodius University in Skopje Center for Regional Policy Research and Cooperation - Studiorum 100 PUBLICATIONS 377 CITATIONS 65 PUBLICATIONS 219 CITATIONS SEE PROFILE Doncho Donev Ss. Cyril and Methodius University in Skopje 282 PUBLICATIONS 655 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Millennium Development Goals in R. Macedonia View project Development of new Schools of Public health in SEE"" View project All content following this page was uploaded by Doncho Donev on 19 January 2015. The user has requested enhancement of the downloaded file. SEE PROFILE METHODS AND TOOLS IN PUBLIC HEALTH A Handbook for Teachers, Researchers and Health Professionals Title Workplace Risk Assessment (WRA) Module: ECTS (suggested): 0,5 Elisaveta Stikova, MD, PhD, Professor Author(s), degrees, National Public Health Institute, Faculty of Medicine, institution(s) University “Ss. Cyril and Methodius”, Skopje, R. Macedonia Neda Milevska-Kostova, MSc, MCPPM, Program Director Centre for Regional Policy Research and Cooperation “Studiorum”, Skopje, R. Macedonia Petar Bulat, MD, PhD, Professor University of Belgrade, School of Medicine, Occupational Health Department, Belgrade, Serbia Doncho Donev, MD, PhD, Professor Institute of Social Medicine, Institutes, Faculty of Medicine, University “Ss Cyril and Methodius”, Skopje, R. Macedonia Elisaveta Stikova, MD, PhD, Professor Address for Faculty of Medicine, University “Ss. Cyril and Methodius”, Correspondence Skopje, R. Macedonia 50 divizija 6, 1000 Skopje, R. Macedonia Tel: +389 70 230 183 e-mail: estikova@ukim.edu.mk or estikova@gmail.com Workplace, risk assessment, risk analysisis, risk Keywords management After completing this module students and public health Learning objectives professionals should be able to: understand and define the terms risk, risk analysis - risk assessment, risk communication and risk management; understand the concept and elements of workplace risk assessment; understand the team work for workplace risk assessment; perform workplace risk assessment using elaborated techniques. Workplace risk assessment is a new approach in the Abstract traditionally oriented occupational health, practiced to date in the SEE countries. Current techniques for recognising and managing occupational safety and health risks were mainly oriented and defined as “workplace analysis” and they lack a risk management and risk quantification component. This module introduces a modern approach to risk quantification that incorporates recent scientific and legal advances in occupational safety and health, consistent with the Framework Directive 89/391/EEC, the ILO conventions and other relevant binding documents that are part of the International and EU regulations. In the introductory lecture the students will be introduced Teaching methods with the concept of risk assessment at the workplace, with special focus on the four key steps of the risk assessment: hazard identification, exposure assessment, dose-response assessment and risk characterization. The theoretical knowledge will be supported by a presentation of a case study. After the theoretical lecture, the students will be required to assess the risk at a given workplace, while referring to the recommended readings. The findings will be presented and shared with other students in the class. 1 Specific recommendations for teachers Assessment of students ECTS: 0,5; work under teacher supervision/individual students’ work proportion: 30%/70%; facilities: lecture room; equipment: LCD projection equipment, flip chart; training materials: recommended readings and matrices/chart tables; target audience: undergraduate and master degree students according to the Bologna process. Multiple choice questionnaire, seminar paper, oral exam. 2 WORKPLACE RISK ASSESSMENT (WRA) Elisaveta Stikova, Neda Milevska-Kostova, Petar Bulat, Doncho Donev THEORETICAL BACKGROUND Introduction – Workplace risks According to the estimations of the International Labour Organization (ILO), every year there are approximately 2.2 million deaths, or on average 6,000 die every day as a result of work-related accidents or diseases. Also, every year, there are about 270 million reported injuries at the workplace that lead to absences from work for 3 days or more, and about 160 million incidents of work-related disease, as a result of exposure to hazardous physical, chemical or biological agents, as well as improper working conditions. About 30-40% of them become chronic and irreversible conditions, and 10% lead to complete and permanent loss of working ability (1,2,3). Hazardous substances kill about 438,000 workers annually, and 10% of all skin cancers are estimated to be attributable to workplace exposure to hazardous substances. There are more than 150 registered physical and chemical agents, classified as occupational cancerogens, and to which about 20-30% of the male and 520% of the female professionally active population are exposed (4). Occupational malignant diseases are cause of about 146,000 deaths or 1,4 million disability adjusted life years (DALYs). Occupational exposure is cause of death for 10% of all cases of malignant diseases of the lungs, bronchi and trachea, and to 24% of all cases of leukaemia. Asbestos alone claims about 100,000 deaths every year and the figure is rising annually. Although global production of asbestos has fallen since the 1970s, increasing numbers of workers are now dying from past exposure to asbestos dust (5). Another occupational disease, silicosis - a fatal lung disease caused by exposure to silica dust – still affects tens of millions of workers around the world. There are 35 million health workers in the world. Significant occupational risk for them represents the percutaneous injury with sharp objects with which they work, such as needles, scalpels, peans, etc. The analyses show that every year nearly 3 million injuries at work are registered, where health professionals have come in contact with contaminated blood. In 2 million of the cases, they have been exposed to Hepatitis B, in 0,9 million of the cases with Hepatitis C, and in 170,000 cases they have been exposed to the HIV virus. As a consequence, every year, there are 85,000 cases of professionally contracted infectious diseases in the health professionals’ community (6). The analysis of the influence of the professional exposure in the total burden of disease shows that 5 18% of all cases of asthma and 14% of cases of Chronic Obstructive Pulmonary Disease (COPD) are related to work. Every year, 234,000 deaths are reported due to COPD with occupational ethiology, which represents 0.4% of the total number of deaths from this cause. This is related to 3 million disability adjusted life years (DALYs). Occupational exposure to noise is a cause for hearing loss of 16% of those that have hearing impairment. In the total burden of disease, the professionally acquired deafness accounts for 0.3% or 4.2 millions of DALYs (7). Although these figures represent basis for serious concern, the problem is additionally aggravated, if we take into account the large number of occupational diseases that remain undiagnosed or unaccounted for. The direct costs for diagnosis, treatment and rehabilitation of the work-related injuries and occupational diseases represent a significant burden to the healthcare system. The indirect costs related to the absence from work, loss of working ability or decreased productivity represents a further burden to the national budgets of each country. Occupational safety and health is one of the European Union's most important social policy areas: every three and a half minutes, somebody in the EU dies from work-related causes; this means almost 167,000 deaths a year as a result of either work-related accidents (7500) or occupational diseases (159,500). According to European Statistics on Accidents at Work (ESAW), about 4 million accidents at work resulting in more than three days off work occurred in EU-15 in 2004. If accidents causing no absence from work or an absence of up to 3 days are added, the estimated total number rises to more than 7 million every year. It means that every four-and-a-half seconds, a worker in the EU is involved in an accident that causes three or more days absence from work (8,9). 3 According to the data from the European Agency for Safety and Health at Work (EU-OSHA), occupational diseases and work-related injuries that are consequence of improperly organized system for protection at work cost each country between 2.6-3.8% of GDP. In the EU about 1 250 million working days are lost each year due to health problems in general. Within the structure by causes (Fig. 1) about 210 million days are lost due to accidents at work and 340 million due to work-related diseases (10,11). Figure 1. Causes for the sickness absence in EU The consequences of accidents at work and of work-related ill health are multiple and complex. The total costs of accidents at work and work-related ill health are not equally divided between the different players. The total labour costs attributable to accidents at work in EU-15 in the year 2000 were estimated at around 48 billion euros. Other costs were estimated at around 6.6 bilion euros (12). Thus, the safety and health of workers represents not only a legal requirement and obligation , but also substantial need for improvement of the productivity and economic progress of each country. At the same time, that means a possibility for establishing a balance between the economic interest, productivity and the health and working ability of the working population. The occupational safety and health is economically oriented category, which is aimed at protection of the interests of the workers, companies, health insurance companies, health workers, and finally of the country and European community as a whole (13). Workers’ safety and health is protected in Europe by an approach based on assessing and managing the risk. In order to carry out effective workplace risk assessement, all those involved require a clear understanding of the legal context, the roles of the main actors involved in the process, as well as the concepts and the process of assessing the risk (14, 15). Legal Context and the role of the main players The legal context of the risk assessment is set out in the EU Framework directive and other related so-called sisters’ directives (16). All European Union countries have legislation that set out measures to protect worker safety and health in order to improve quality in safety and security in the workplace. These laws are based on European Directives that lay down minimum obligations for employers and workers, covering the prevention of all types of risks and each activity or sector where risks exist. This legislation is in place to protect workers against occupational accidents and diseases and to assist in the prevention of occupational hazards (17). Employers have a general duty to ensure the occupational safety and health in every aspect related to work and carry out a risk assessment. The EU framework directive highlights the key role played by risk assessment and sets out basic provision and measures that must be followed by every employer. Every employer is responsible for taking the appropriate measures such as ensuring the availability of sufficient resources, carrying out a risk assessment, preventing occupational risk, informing, training and consulting workers. The employer has a duty to: 4 Organise risk assessment Select the person (s) to carry out risk assessment and ensure they are competent Assess the risk and implement protective measures Consult the employees or their representatives about the organisation of the risk assessment Ensure all affected workers are informed of any hazard and any harm to which they may be at risk and the all protective measures taken to prevent such harm. The employer has a duty and responsibility to make a final decision and to designate the people who carry out risk assessment. They can be: The employer Employees designated by the employer External assessor and/or services if there is a lack of competent person within the company (16). Among the most important characteristics of designated or nominated person/company should be competence. They don’t need to be occupational safety or health experts, but they should demonstrate their competencies. They should have competencies to understand the general approach to the risk assessment and capabilities to apply this understanding, knowledge and skills to the workplace. But, they should have ability to identify the situations that overwhelmed their competencies in terms to ask for proper help and further assistance .They should demonstrate their competencies by showing they would be able to: Identify safety and health problems, Assess and prioritise the need for action, Suggest options available to eliminate or minimise risk, Evaluate their effectiveness and Promote safety and health good practices. The last but not the least point in the risk’s chain are workers and their representatives. They have a right to be consulted for organisation of the risk assessment, to participate in the risk assessment, to alert the designated person for perceived risk and to be informed about the risk on the work place and their safety and health. What is risk? According to WHO (1993) risk represents a likelihood of an occurrence of hazardous event and the likelihood of an occurence of injury or damage to the health of people caused by this event. Risk is a combination of the likelihood of an occurrence of a hazardous event and the severity of injuries or damage to the health of people that might be caused by this event. Thus, the term professional risk embeds the probability of occurrence of negative effects on the workers' health and life, as a result of presence of certain hazards at work or exposure of the workers to hazardous agents in the working environment (17, 18). Occupational risk is expected frequency of occurrence of occupational diseases and work-related injuries or death, that are consequential to the exposure to different hazardous events or substances, and physical, chemical or biological factors of the working environment. A risk is a chance, higher or low, that somebody may be harmed by the hazard. A hazard can be anything –work materials, equipment, work methods or practices that have potential to cause harm. Bearing in mind that it is practically impossible to eliminate the probability of occurrence of hazardous agents in the working environment, it is clear that the risk is always present. From expert point of view, it is inevitable to assess the actual and real level of risk, and furthermore important – to define the acceptable levels of risk (19). Acceptable risk level means that the likelihood of occurrence of hazardous health effects can justifiably be considered as insignificant, and that the occurring effects are so minimal that can not be further minimized, neither through increased regulatory mechanisms nor through further investment for risk elimination. Usually, acceptable risk level is agreed between all participants in the decision-making process – scientists, public health professionals, policy makers, administrative and legislative structures. Risk analysis is a process that enables insight into the correlation between the exposure, dose and effects from one side, and the measures for mitigation and elimination of the risk and the ways of informing the stakeholders. Risk analysis consists of 3 consecutive and interrelated processes, i.e. procedures: risk assessment, risk management and risk communication. 5 Phases of risk analysis and interrelatedness of its segments are presented in the Figure 2 below. Figure 2. Interrelatedness of the phases of risk analysis The starting key point in the risk analysis is the risk assessment. Risk assessment is quantitive measure of the likelihood of occurrence of hazardous health effects as a result of existing hazards at the workplace (20,21). Workplace risk assessment is the process of evaluating risk to workers’ safety and health from occupational hazards. It is a systematic examination and evaluation of all aspects of work that consider: What could cause injury or harm, Whether the hazards could be eliminated, and if not What preventive or protective measures are, or should be, in place to minimise and control the risk. Workplace risk assessment means quantification of the likehood of an occurrence of hazardous event at the workplace and related negative effects (injuries at work or work related diseases) Next phase in the risk analysis process is the risk management. The risk management represents assessment of the successfulness of the preventive and mitigation measures (22). Risk management includes the following activities: control of the decision made during the risk assessment, determination of the acceptable risk level, implementation of mitigation (corrective) measures and monitoring of the management. Risk management is a process in which direct responsibility falls with those that participate in the decision-making process and creating policies for safety and health – from the level in the company where the risk assessment is made to the highest national structures (15). The elements for decision making are taken from the scientific research and expert opinions, standards and good practices established on national or international level (23, 24). Risk communication represents interactive exchange of information and opinions/forecasts related to the confirmed risk. The information is exchanged between those that participate in the risk assessment and risk evaluation, those that manage the risk and those responsible for making the decisions related to the whole process (25). Information obtained through monitoring of the working environment in the process of health professional risk assessment are combined with the information from other sources, such as epidemiological studies for the impact of a certain professional exposure, referent values for the maximum allowed concentrations in the workplace, etc. The strategy for risk communication should be determined, established and agreed at the beginning of each risk analysis. That should be a continuous process in which at first, the stakeholders as well as key 6 responsible persons and methods of communication are identified. At the same time, the most appropriate ways of communication should be defined. The most often used ways of risk communication are: public gatherings, technical and expert meetings, written and published documents, written and published results of related research and establishment of website. Risk communication represents a legal obligation for the employers to inform the employees about the identified and confirmed level of risk to which they are exposed during their work as well as about the measures and procedures that they, both employer and employees, have to comply with in order to achieve successful risk management. The interrelatedness of the processes and activities of risk analysis and risk assessment, as well as risk management are shown on the Figure 2. What is risk assessment? As already shown, the starting and key point of the risk analysis is the risk assessment. Risk assessment is an important step in the overall process for protecting the workers and business as well as complying with the low. It should be focused on the level of risk with potential to cause harm (17, 26). In addition, risk assessment is quantitive measure of the likelihood of occurrence of hazardous health effects as a result of existing hazards at the workplace. Risk assessment is based on the quantification of the probability that the hazardous event will occur during the working process and on the assessment of the severity of the hazardous effects that those events will have on the health of the exposed workers (27). Risk assessment represents obligation of the employers, and has the aim to enable them to: make easier identification of the dangers and hazards at the workplace, determine measures for occupational safety and health,, check the efficiency of the measures undertaken and manifest responsibility in front of the authorities and workers in undertaking necessary preventive measures. Risk assessment consists of several groups of consecutive activities (Figure 3) that have to be undertaken in the proper order, in magnitude and timeframe that are consistent with the determined objectives (28,29). Those are: hazard identification, exposure assessment, dose-response assessment, and risk characterization. Hazard identification Hazard identification is a procedure of recognition of hazardous factor in the working environment and defining its physical, chemical and other properties. In the course of hazard identification, the "fate" of hazardous agent is determined, either in the external environment or in the organism, but also its properties to cause negative health effects or disease. Exposure assessment The assessment of the exposure means determination of the level of hazardous substances that are present in the working environment and their internalization/intake into the organism of the professionally exposed workers. According to the intake route of the substance into the human organism, the exposure can be: direct and indirect. Dose-response assessment Dose response assessment is process of making a conection between the data of the exposure assessment and occurence of the work-related diseasses and other harm of the health of the exposed workers. Risk characterization The last step in the risk assessment process means characterisation of the actual risk on the examined workplace. It is essential and most visible phase of the quantification of the percived risk. It means establismnet 7 of the interrelation among all information, data and results obtained from the previous steps. For practical use of the whole risk assessment proces in this phase the quantification of the probability of the occurence of the hazard and the severity of the harm caused by respective hazard is made. Figure 3. Group of activities that form the risk assessment Methodological approach to risk assessment Preconditions for commencement of risk assessment are: Existence of appropriate legal framework (obligation, responsibility and conditions), Existence of national standards, guidelines, technical guides, agreed best practices, determined levels of maximum allowed concentrations (levels), manufacturer's guidelines, professional associations' standards, etc. and Existence of legally and professinally defined hierarchy for risk prevention: o avoidance of hazards (modernization and automatization of the technology process), o replacement of hazardous with harmless or less hazardous substances (substitution), o combating hazards at their source (separation, hermetization), o applying collective protection measures, o adjustment to the new technological knowledge and their appliance into practice and continuous promotion of the care for safety and health at work. Workplace risk assessment begins with the decision of the employer for commencement of the procedure and appointment of expert person from the pool of employees that will be responsible for the overall process of risk assessment (30,31). At the same time, depending on the size of the company, the employer appoints representative or representatives of the workers that are participating in the process of risk assessment, or the Committee for safety and health at work might be established. The flow chart of the risk assessment and control consists of several procedures, as follows: Preparation of Action Plan and monitoring of its implementation, Data collection about the working environment and workplace (access, safety of working surfaces, safety of equipment and tools, microclimate conditions, lighting, chemical and biological hazards, etc.), Identification of working processes and operations with description and/or identification of hazards and dangers, 8 Data collection on occurence of hazards and/or dangers during the working process, Data collection on the employees, Analysis of the recorded effects and/or diseases related to the working conditions, Quantification of the likelihood of occurence of hazardous effects, Quantification of the severity of the expected hazardous effects and/or diseases and injuries at workplace, Defining priorities for prevention, reduction and elimination of workplace-related hazards, Implementation of the control measures and assessment of their effectiveness, Review of the risk assessment in pre-determined conditions (change of the technological process, occurence of severe, death or group injuries, etc.). Starting point in the risk assessment is preparation of the action plan, which preparation, implementation and monitoring is under the responsibility of the employer. The action plan should include: Organization and coordination of the risk assessment, Appointment of competent persons that will work on the risk assessment, Appointment of representatives of the workers that will be involved in the risk assessment process, Defining the flow of information and conditions under which the necessary data for risk assessment will be used (confidentiality), Defining the monitoring of the preventive and/or corrective measures and undertaking responsibility for their implementation by signing written act, Informing the employees about the identified conditions during the risk assessment and the preventive and corrective measures undertaken. According to the European directives, and depending on the conditions in one company, the risk assessment can be made by (16): The employer, Employed expert personnel appointed by the employer or External professional services. The defining criterion regarding the selection of the responsible party that will undertake the risk assessment is the size of the company, working conditions and the competence of the appointed person for risk assessment in the company. In practice, very often a need is imposed for engaging a team of different specialties from various fields (outsourcing). The persons involved in the risk assessment process are confirming their competencies by showing evidence of formal education in the field (if they have such education), as well as by showing competency and capability to: Understand and be familiar with the general concept of risk assessment; Have and apply their professional knowledge in particular conditions and workplaces for which the risk assessment is conducted. Such approach requires that the persons involved in the risk assessment have knowledge and information based on which they will be able to: Recognize the problems related to the occupational safety and health , Prioritize accordingly the activities related to the occupational safety and health, Predict the potential dangers and hazards, as well as consequences that can be expected in case of their occurence, based on relevant evidence, Identify conditions that surpass their competencies, in order to seek additional expert opinions and Know the methodologies for risk assessment, including as much as necessary the complex logic analyses and technical simulations. Key elements in risk assessment Risk assessment is in fact reconsideration of all aspects of the work and work process, in order to identify and quantify the hazards that can inflict injury, professional disease or injury at workplace, for the purpose of reducing or removing them, or if possible, to introduce as much as justifiable, preventive and protection measures with which the risk will be eliminated or decreased and controlled. The risk assessment should embed all predictable dangers and hazards at work in all aspects of work process. It is conducted with participation and consultation of all those involved in the work process – from workers to their employers. 9 Risk assessment is applicable to all workers and work positions that are in direct or indirect relation and interaction with the hazards present in the working environment, and special attention should be paid to the particularly vulnerable groups of workers – young people, pregnant and lactating women, disabled, etc. Risk assessment is a set of procedures during which an analysis of the available information is undertaken. During the risk analysis, the appointed person or team does not conduct any measurements, analyses or medical check-ups, but rather makes overview and analysis of the existing situation and available documentation (32,33). The information necessary for conducting risk assessment can be obtained through (but not limited to): Analysis of the work opreations and procedures, Filling stadndardized or adjusted check lists and questionnaires for workers, Consultation and conversation with workers and their representatives (interviews), Overview of the technical specifications and guidelines provided by the manufacturers or distributers of the equipment, tools and substances, Databases of relevent information for safety and health at work and other scientific and technical literature, Guidelines, directives and good practices given by national referent bodies in the field of standardization, scientific institutes or professional assocaitions, Data for recorded accidents and injuries at work, Data for the recorded morbidity (professional and other work-related diseases), Data from undertaken mesurements of the factors in the working environment and National standards, criteria and lists of maximum allowed concentrations and biological exposure tests, etc. The official and recorded data are used available from the records of the company, and, in the same way, all of the procedures would be recorded as part of the risk assessment. Methodology for risk assessment can be semi-quantitative or numerically quantitative, and that depends on the national legislation, as well as of the type of certain working process at the workplace. Regardless of the methodology chosen for undertaking risk assessment, each of the methodologies is based on defining the potential spectrum, i.e. severity of the potentially hazardous effects and the probability for their occurrence. The spectrum, i.e. the severity of potentially hazardous effects on the health of professionally exposed workers falls into the following categories: Insignificant consequences, Accedent without injury, Light injury, Severe injury, acute poisoning or chronic professional disease, Death, Death of more workers at the same time. The probability (likelihood) for occurrence of these hazardous effects as a result of professional exposure can be: Very unlikely (practically improbable) Likely (moderate probability) Very likely (high probability) In combination of these possibilities and with the use of risk assessment matrix, the result is semiquantitative risk assessment (20). In this case the result can be low, medium or high, or a numerical scale can be used (for example, scale with values from 1-10 with pre-defined criteria about the interpretation of the meaning of each of the values on the scale). Below is a sample for semi-quantitative matrix for risk quantification. This matrix is recommended by European Agency for safety and Health at Work (34). Table 1. Likelihood for severity of damage/level of risk in 3x3 matrix Severity of damage / level of risk Likelihood Very unlikely Likely Very likely Low Low risk (1) Low risk (1) Moderate risk (2) Moderate High Low risk (1) Moderate risk (2) High risk (3) Moderate risk (2) High risk (3) High risk (3) 10 Legend: Frequency of occurence Severity of the expected negative health effects Very unlikely: Not expected to occur during the whole working lifetime Low severity: injuries and diseases that do not cause prolonged/longterm health problems (e.g. small injuries, eye irritation, headache, etc.) Likely: IT can occur several times during the working lifetime Moderate severity: injuries or disease that cause moderate but prolonged/long-term and periodically repetitive health problems (e.g. wounds, simple fractures, burns of second degree to a limited part of the body, skin allergies, etc.) Very likely: It can occur repetitively during the working lifetime High severity: injuries or diseases that cause severe and permanent health problems or death (e.g. amputations, complex fractures with disability, cancer, burns of 3rd degree covering large part of the body, etc.) Below is a more complex quantification of the risk assessment by using the Risk matrix 5x5 (35). Table 2. Likelihood for severity of damage/level of risk in 5x5 matrix Consequences A- Likelihood BCDE- Almost certain to occur in most circumstances Likely to occur frequently Possible and likely to occur at some time Unlikely to occur but could happen May occur but only in rare and exceptional circumstances 1 – Insignificant Dealt with by inhouse first aid, etc 2 – Minor Medical help needed. Treatment by medical professional/hospital outpatient, etc 3 – Moderate Significant nonpermanent injury. Overnight hospitalisation (inpatient) 4 – Major Extensive permanent injury (eg loss of finger/s) Extended hospitalisation 5 – Catastrophic Death. Permanent disabling injury (eg blindness, loss of hand/s, quadriplegia) High (H) High (H) Extreme (X) Extreme (X) Extreme (X) Moderate (M) High (H) High (H) Extreme (X) Extreme (X) Low (L) Moderate (M) High (H) Extreme (X) Extreme (X) Low (L) Low (L) Moderate (M) High (H) Extreme (X) Low (L) Low (L) Moderate (M) High (H) High (H) How to Prioritise the Risk Rating Once the level of risk has been determined the following table may be of use in determining when to act to institute the control measures. Table 3. Risk rating and prioritization of measures Risk rating Immediate measures Interim measures Extreme Act immediately to mitigate the risk. Either eliminate, substitute or implement engineering control measures. High Act immediately to mitigate the risk. Either eliminate, substitute or implement engineering control measures. If these controls are not immediately Remove the hazard at the source. An identified extreme risk does not allow scope for the use of administrative controls or PPE, even in the short term. An achievable timeframe must be established to ensure that elimination, substitution or engineering controls are implemented. NOTE: Risk (and not cost) must be the primary 11 accessible, set a timeframe for their consideration in determining the timeframe. A implementation and establish interim risk timeframe of greater than 6 months would reduction strategies for the period of the generally not be acceptable for any hazard set timeframe. identified as high risk. Medium Take reasonable steps to mitigate the risk. Until elimination, substitution or Interim measures until permanent solutions engineering controls can be can be implemented: implemented, institute administrative . Develop administrative controls to limit the …or personal protective Take reasonable steps to equipment mitigate and Low use or access. controls. These level” controls monitor the risk.“lower Institute permanent Provide supervision and specific training must notin bethe considered permanent controls long term. Permanent related to the issue of concern. solutions.may Thebetime for which they are controls administrative in nature (See Administrative Controls below) established be based on risk. At if the hazardmust has low frequency, rare the end of the if the risk has not likelihood andtime, insignificant consequence. been addressed by elimination, substitution or engineering controls a riskof assessment musttobeminimize occupational exposure Table 4.further Hierarchy control in order undertaken. Eliminate the hazard. Elimination Provide an alternative that is capable of performing the same task and is Substitution safer to use. Provide or construct a physical barrier or guard. Engineering Controls Develop policies, procedures practices and guidelines, in consultation Administrative Controls with employees, to mitigate the risk. Provide training, instruction and supervision about the hazard. Personal equipment designed to protect the individual from the hazard. Personal Protective Equipment There are many other methodologies for quantification of the likehood of occurrence of the hazardous event at the workplaces as well as a consequences of those events to the workers’ health (like AUVA’s or BG methodologies), but it seams that matrix’s approach is the most applicable one. The documentation which is a part of the process of risk assessment should be made available to: Experts responsible for implementing the measures for occupational safety and health Persons – representatives of workers, involved in the process of occupational safety and health. It is especially important to predict the time and conditions under which every employer is obliged to initiate the revision of the once undertaken risk assessment, but also there should be a legal obligation established for revision of risk assessment at any occasion when there are changes in the technological process or collective injury/death at work. Process of risk assessment - case study There are a lot of resources in which it is possible to find a case studies and examples for good practices (23,36). The usefulness and applicability of such case study or good practice depend of the sector, size of the company, age, gender and other characteristics of workforce in the company, technological improvement, management and organization of the work etc. Many case studies should be find on the web site of the EU-OSHA or other agencies. Process of risk assessment - exercise Theoretical approach to the risk assessment seems to be very complicate and inapplicable. But, it is so simple process if basic tools and essentials are accepted (34). According to the European Agency for Occupational Health and Safety, workplace risk assessment consists of 5 simple steps (Fig. 4): 12 Figure 4. Five steps to the workplace risk assessment (34) Step 1 – What information should be collected and how? What information are collected? For the workplace risk assessment it is necessary to have the following information at hand: location of the workplace, characteristics of the equipment, materials and processes, description of work operations, identified hazards and their sources, potential consequences, protection measures, number of exposed workers, number of workers from vulnerable groups (pregnant women, young workers, workers with disabilities), occurrence of professional diseases, work-related diseases and injuries at work (32,37). How information are collected? Possible sources of information are: technical data on the equipment, materials and substances that are used in the production process, technological procedures and work protocols, results of measurements about the hazards at the workplace (workplace analysis), specification of the properties of chemical substances (registry), legal framework and technical standards, scientific and technical literature, observing the working environment observing the task performed at workplace, Interviewing the workers, data on workplace injuries and professional diseases (registry), (33). Step 2 – How hazard can be identified? 1.1. The identification of the hazards in all aspects of work should be approached by: walking around the workplace and looking at what could cause harm 13 consulting workers and/or their representatives about any problems they have encountered. Often the quickest and surest way to identify the details of what really happens is to ask the workers involved in the activity being assessed. They will know what process steps they follow, whether there are any short cuts, or ways of getting over a difficult task, and what precautionary actions they take examining systematically all aspects of the work, considering long-term hazards to health, such as high levels of noise or exposure to harmful substances, as well as more complex or less obvious risks such as psychosocial or work organisational risk factors looking at company accident and ill-health records The hazard identification is usually performed by using hazard specific check lists. These are adjusted to the need and aim of the investigation/assessment itself. EU-OSHA on its website gives one general check list that can be used as model for design of own check lists for every particular company or workplace for which a risk assessment needs to be conducted. But, at the same time other additional check lists exist that are related to the most common hazards and dangers that occur at the workplace and for which a risk assessment is required and necessary. The check lists can be of a general type and specific type, where particular and specific professional hazards and very particular technological processes and workplace are assessed. In general, the check lists are aimed at fast and simple orientation in the process of hazard identification, frequency of its occurrence and severity of the damage that can be caused by it. Usually, the check lists are prepared in cooperation with all workers involved in the working process in question (38). Besides the general, there are also specific check lists for the hazards and sectors (Table 5). Table 5. Check lists for workplace hazards and related sectors Check lists – hazards 1) Uneven slippery surface; 2) Vehicles and moving machines; 3) Machines with movable parts; 4) Electric installations; 5) Fire; 6) Explosion; 7) Chemical substances; 8) Noise; 9) Vibrations; 10) Lighting. Check lists – sectors - administrative (office) work; - food production; - wood processing; - agriculture; - small and surface mining. *Additional info and specific check lists are available at: www.osha.europa.eu 1.2. The identification of all those who might be exposed to the hazards For each hazard it is important to be clear about who could be harmed; it will help in identifying the best way of managing the risk. Account should be taken of workers interacting with the hazards whether directly or indirectly, e.g. a worker painting a surface is directly exposed to solvents, while others workers in the vicinity, engaged in other activities, are inadvertently and indirectly exposed. This doesn’t mean listing everyone by name, but identifying groups of people such as ‘people working in the storeroom’ or ‘passers-by’. Cleaners, contractors and members of the public may also be at risk. Particular attention should be paid to groups of workers who may be at increased risk or have particular requirements: workers with disabilities, migrant workers, young and old workers, pregnant women and nursing mothers, untrained or inexperienced staff and temporary and part-time workers. Step 3 – How to assess the risk araising from identified hazard? The next step is evaluating the risk arising from each hazard. This can be done by considering: how likely it is that a hazard will cause harm; how serious that harm is likely to be; how often (and how many) workers are exposed. Based on the likelihood of the hazard or danger to occur and on the severity of the expected consequences on the health of professionally exposed workers, a decision on the level of professional risk should 14 be performed. As previously said in the part on methodology, the matrices 3x3 and 5x5 can be used for this purposes; or other semi quantitative or numerical matrices (for risk quantification). The next very important step is to decide whether risk arising from a hazard is acceptable or unacceptable. In general: high risk is unacceptable, small and medium risk is acceptable, If legal requirements are not complied with, risk is not acceptable! The risk assessment should always be carried out with the employees’ active involvement. When deciding on the acceptability of risk, bear in mind their input, and take into account gender, age, and also health of the employees for whom assessment is conducted. A straightforward process based on judgement and requiring no specialist skills or complicated techniques could be sufficient for many workplace hazards or activities. These include activities with hazards of low concern, or workplaces where risks are well known or readily identified and where a means of control is readily available. This is probably the case for most businesses (mainly small and medium-sized enterprises — SMEs). Risks should then be prioritised and tackled in that order. Step4 – How the actions to eliminate or reduce the risk arising from hazard can be planed? It is essential that any work to eliminate or prevent risks is prioritised. How should the activities for risk elimination or reduction be prioritised? The basic principles are: if the risk is high and assessed as unacceptable, the measures for its reduction should be undertaken immediately, if the risk is moderate and assessed as acceptable, it is recommended to plan the activities for reduction of the risk level, if the risk is low and assessed as acceptable, it is essential to ensure that it will be reduced or at least remain on the same level. When preventing and controlling risks, the following general principles of prevention have to be taken into account: avoiding risks (elimination of hazard/risk) by modernization and automatization of the technical process; substituting the dangerous by the non-dangerous or the less dangerous substances; combating or isolating the risks at source (separation, hermetization); minimization of the hazard/risk with organizational measures minimization of the hazard/risk with collective protection measures; minimization of the risk through appropriate personal protective means applying collective protective measures rather than individual protective measures (e.g. control exposure to fumes by local exhaust ventilation rather than personal respirators); adapting to technical progress and changes in information; seeking to improve the level of protection The next group of activities is to put in place the preventive and protective measures. It is important to involve the workers and their representatives in the process. Effective implementation involves the development of a plan specifying: the measures to be implemented; who does what and when; when it is to be completed. Step 5. How to document, monitor and review the process? The risk assessment for each workplace should be documented in the appropriate record for risk assessment. The record should contain the following sections of information: Basic information: name of the company and address, name of the workplace, number and names of workers on the assessed workplace, date of the assessment and name of the person conducting the assessment; Name of the hazard if identified; For every identified hazard should be noticed: Preventive/protection measures used for alleviation and limitation of the risk, Results of risk assessment/evaluation, Planned activities for reduction of the risk. 15 The risk assessment has to be reviewed regularly depending on the nature of the risks, the degree of change likely in work activity or as a result of the findings of an accident or ‘near miss’ investigation. Risk assessment is not a once-and-for-all activity. Risk assessment tools are available at the web-page of the EU-OSHA and they should be used and modified in accordance with specific condition and needs of the company. The translation and modification of the check list and final report is necessary (34). REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. ILO. Programme on Safety and health at Work and the Environment. Global Estimates of Fatal Work Related Diseases and Occupational Accidents, World Bank Regions 2005. Available from: http://www.ilo.org/public/english/bureau/inf/download/sh_background.pdf. (Accessed: 6.07.2008). International Labour Organization.Yearbook of Labour Statistics. Volume 59, Geneva, 2000. Hamalainen P, Takala J, Saarela KL. Global estimates of occupational accidents. Safety Science 2006; 44: 137–56. Leigh J, Macaskill P, Kuosma E, Mandryk J. Global Burden of Disease and Injury Due to Occupational Factors. Epidemiology 2005; 10 (5): 626-31. Driscoll T, Nelson DI, Steenland K, Leigh J et al. The global burden of disease due to occupational carcinogens. American Journal of Industrial Medicine 2005; 48(6): 463-71. Verschuren R, De Groot B, Nossent S. Working conditions in hospitals in the European Union. European Foundation for the Improvement of Living and Working Conditions. Luxembourg: Office for official publications of the European Communities.1995: 19-49 & 55-62. Schulte PA.Characterizing the Burden of Occupational Injury and Disease. Journal of Occupational & Environmental Medicine 2005; 47(6): 607-22. The European Statistics on Accident at Work. ESAW 2003 Databasa, Available from http://www.av.se/dokument/statistik/english/Accidents2003_EU15.pdf. (Accessed: 6.09.2008). Healthy Workplaces. Good for you. Good for business. A European Campaign on risk assessment. Campaign Summary. European Agency for safety and Health at work, 2008. Available from http://osha.europa.eu/en/campaigns/hw2008/campaign/campaignsummary. (Accessed: 6.09.2008). Falkdal AH, Edlund C, Dahlgren L. Experiences within the process of sick leave. Scand J Occup Ther 2006; 13(3):170-82. Hansen A, Edlund C, Branholm IB. Significant resources needed for return to work after sick leave. Work. 2005; 25(3):231-40. Eurostat. Statistical analysis of socio-economic costs of accidents at work in the European Union, Eurostat. Luxembourg: Office for Official Publications of the European Communities, 2004. Occupational Medicine in Europe: Scope of competencies. EUR/ICP?EHBI 02 02 04. Available from: http://www.who.int/occupational_health/publications/eurmedicine/en/index.html (Accessed: 24.10.2006). Kolluru RV, Bartell SM, Pitblado RM, Stricoff RS. Risk assessment and management handbook : For environmental, health, and safety professionals. McGraw-Hill, 1996. Eduljee GH. Trends in risk assessment and risk management. The Science of the Total Environment. 2000; 249 (13):13-23. European Council. Council Directive 89/391/EEC of 12 June 1989 on the introduction of the measures to encourage improvements in the safety and health of workers at work. European Legislation (occupational safety and health). Available from: http://osha.europa.eu/legislation (Accessed: 24.10.2006). Covello VT, Merkhofer MW. Risk Assessment Methods, Approaches to Assessing the health and environmental risk. New York: Plenum Publishing Corporation; 1993. Carrivick PJW, Lee A, Kelvin K. Effectiveness of a Workplace Risk Assessment Team in Reducing the Rate, Cost, and Duration of Occupational Injury. Journal of Occupational & Environmental Medicine 2002; 44(2):155-9. Hertz-Picciotto I. Epidemiology and quantitative risk assessment: A bridge from science to policy. American Journal of Public Health 1995; 85(4): 484-91. Kromhout H. Design of measurement strategies for workplace exposures. Education Occupational & Environmental Medicine. 2002; 59(5): 349-54. Jardine C, Hrudey S, Shorteed J. et all. Risk management frameworks for human health and environmental risks. J Toxicol Environ Health B Crit Rev. 2003; 6(6):569-720. WHO Regional Office for Europe. Towards good practice in health, environment and safety management in industrial and other enterprises. EUR/ICP/EHCO 02 03 04/13, WHO, 1999. Available from: http://www.who.int/occupational_health/publications/goodpractice/en/index.html (Accessed: 24.10.2006) Franco G: Evidence-based decision making in occupational health: Occup Med 2005; 55: 1-2 15. Cuny E, Jorgensen V, Galligan J. Comprehensive training for hazard communication. Compend Contin Educ Dent 2005; 26(3 Suppl):28-31. Scholz JT, Gray WB. OSHA enforcement and workplace injuries: A behavioral approach to risk assessment. Journal of Risk and Uncertainty 1990; 3(3):283-305. Concha-Barrientos M, Nelson DI, Driscoll T et all.: Comparative Quantification of Health Risks – Selected occupational risk factors. WHO, 2004. Stikova E. Risk and risk analysis [In Macedonian]. Republic Institute for Health Protection-Skopje; 2008. 16 29. Stikova E. Health Ecology [In Macedonian]. Univerzity »Ss. Cyril and Methodius, 2006. 30. Nelson DI, Concha-Barrientos M, Driscoll T et al. The global burden of selected occupational disease and injury risks: Methodology and summary. Am J Ind Med. 2005; 48(6): 400-18. 31. Maroni M, Faneti AC, Metruccio F. Risk assessment and management of occupational exposure to pesticides in agriculture. Med Lav 2006; 97(2):430-7. 32. Bugajska J. Occupational data cards as a source of information for health prevention purposes. Med Pr 2000; 51(6):551-61. 33. ILO. Recording and Notification of Occupational Accidents and Diseases. ILO code of practice, 1996. 34. European Agency for Safety and Health at Work. Safety and health at work is everyone's concern – checklists. Available from: http://osha.europa.eu/en/campaigns/hwi/ra_tools_checklists/ (Accessed: 7.07.2008). 35. Worcestershire, NHS. Future consequence or level of impact resulting from accident or incident. 5X5 scoring matrix. Available from: http://www.worcestershirehealth.nhs.uk/EXTRANET_Library/LINDAMARRIOTT/County%20Risk%20Matrix% 202.pdf (Accessed: 7.07.2008). 36. European Agency for Safety and Health at Work. Guidelines on the collection, evaluation and disemination of good practice information on the internet. Bilbao, 2002. Availavble from: http://osha.europa.eu/en/good_practice/. (Accessed: 7.07.2008). 37. Money C, Margary SA. Improved Use of Workplace Exposure Data in the Regulatory Risk Assessment of Chemicals within Europe. Annals of Occupational Hygiene 2002; 46(3):279-85. 38. European Agency for Safety and Health at Work. Safety and health at work is everyone's concern risk assessment essentials. Available from: http://osha.europa.eu/en/topics/riskassessment. (Accessed: 7.07.2008). 17 View publication stats