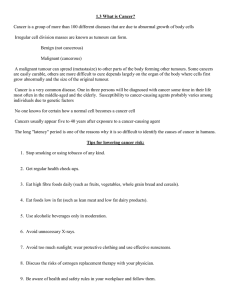
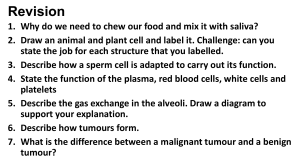
PERSPECTIVES OPINION Experimental mouse tumour models: what can be learnt about human cancer immunology? Glenn Dranoff Abstract | The recent demonstration that cancer immunotherapy extends patient survival has reinvigorated interest in elucidating the role of immunity in tumour pathogenesis. Experimental mouse tumour models have provided key mechanistic insights into host antitumour immune responses, and these have guided the development of novel treatment strategies. To accelerate the translation of these findings into clinical benefits, investigators need to gain a better understanding of the strengths and limitations of mouse model systems as tools for deciphering human antitumour immune responses. Immunotherapy has recently emerged as a viable, and potentially transformative, approach to cancer treatment. Within the past 15 months, the US Food and Drug Administration has approved two ‘firstinto-class’ immunotherapies, based on their abilities to prolong patient survival. These therapies are sipuleucel‑T (Provenge; Dendreon), a cellular vaccine for prostate cancer, and ipilimumab (Yervoy; BristolMyers Squibb), a blocking antibody specific for cytotoxic T lymphocyte antigen 4 (CTLA4) that is used for treating advanced melanoma (BOX 1). The clinical success of these immuno­ therapies has motivated increasing numbers of academic investigators and biotechnology and pharmaceutical companies to reconsider the role of immunotherapy in cancer treatment. Several new agents are already undergoing clinical examination, with promising early signs of activity. The most compelling candidates may be blocking antibodies specific for the T cell co-inhibitory receptor programmed cell death protein 1 (PD1) or its ligand, PDL1, which can be expressed at high levels on tumour cells as a consequence of oncogenic signalling or local interferon‑γ (IFNγ) production1. Furthermore, ‘offthe-shelf ’ cancer vaccines that combine molecularly defined tumour antigens with novel delivery systems and adjuvants are being tested in large, randomized Phase III clinical trials for efficacy against common tumour types, including lung, prostate and breast carcinomas, for which there are large unmet treatment needs2,3. Beyond these relatively advanced programmes, a range of antibodies that target other immune regulatory molecules, bispecific antibodies that induce adaptive immune responses and engineered adoptive T cell strategies are in, or about to enter, testing in patients4. The new cancer immunotherapies arise, in large part, from mechanistic insights obtained from experimental studies in mice, which have also served as the most common system for obtaining ‘proof of principle’ for therapeutic antitumour activity. Given the expense of the clinical development of immunotherapies and the risk for inflammatory toxicity, model systems are widely considered to be a required prelude to investigation in humans. However, many model systems are available, including transplantable tumour models, models in which tumours arise owing to transgenes or gene knockouts, and models in which humanized mice (which are immunodeficient mice that have been reconstituted with various components of a human immune system) NATURE REVIEWS | IMMUNOLOGY are inoculated with human tumour xenografts. This diversity of mouse model systems raises challenges for both newcomers to the field and experienced workers. How does one choose which system or systems to study? Can the lessons derived from one model system be generalized to others? Does any system faithfully recapitulate tumour development in patients? How informative are comparative studies of different therapies in the same model? Can the experimental systems be used to prioritize particular combinations of immunotherapies? These difficult questions acquire some urgency given the growing number of potential targets and strategies for immuno­ therapy. Moreover, although the recent clinical trials validate the overall approach of immunotherapy and hint at a greater potential, most patients still need more effective treatments, underscoring the heterogeneity of human antitumour immune responses. Unfortunately, our understanding of human cancer immunology is currently too limited to allow definitive answers to the questions posed above. Ironically, an intensification of the breadth and depth of clinical research may be required to generate a sufficiently rich framework to more effectively evaluate, develop and apply experimental systems. However, mouse tumour models remain an almost obligatory stepping stone to undertaking studies in patients with cancer. In this Opinion article, I discuss some of the strengths and limitations of three of the most commonly used experimental mouse model systems, juxtaposing relevant clinical data in an effort to evaluate the predictability of current models. Because of space constraints, this short commentary is not meant to be exhaustive, but rather to highlight a few central principles. Particular attention is directed to studies of immune-checkpoint blockade in light of the recent exciting clinical data. Transplantable tumours Transplantable tumours have been the workhorse of cancer immunology for several decades5 (FIG. 1). Studies using these systems have uncovered many important mechanistic features, including the existence of shared and tumour-specific antigens, the intrinsic VOLUME 12 | JANUARY 2012 | 61 © 2012 Macmillan Publishers Limited. All rights reserved PERSPECTIVES Box 1 | Clinical advances in immunotherapy Sipuleucel‑T is an autologous cellular vaccine consisting of peripheral blood mononuclear cells that have been exposed ex vivo to a recombinant fusion protein composed of prostatic acid phosphatase (PAP; a prostate cancer differentiation antigen) linked to granulocyte–macrophage colony-stimulating factor (GM-CSF; a cytokine that enhances antigen-presenting cell function)58. Repetitive intravenous infusions of sipuleucel‑T to patients with metastatic, castrate-resistant prostate carcinoma increased median overall survival by approximately 4 months, although no tumour regressions or impact on time to disease progression were observed59. This clinical improvement, albeit modest, was achieved with minimal toxicity and in a disease setting with few therapeutic options — factors that collectively translate into meaningful benefits. Ipilimumab is a fully human monoclonal antibody that blocks the T cell co-inhibitory molecule cytotoxic T lymphocyte antigen 4 (CTLA4)22. In two large randomized clinical trials in patients with advanced melanoma, ipilimumab augmented median overall survival to a greater extent than dacarbazine (a cytotoxic chemotherapy considered as a standard of care) or vaccination with a short peptide derived from GP100 (also known as PMEL; a melanocyte differentiation antigen), which showed minimal, if any, efficacy60,61. Ipilimumab is the first agent that enhances survival in patients with advanced melanoma and, most notably, treatment yielded long-term disease control in approximately 20% of the subjects, with a follow-up of more than 4 years. Although treatment is associated with a substantial (~15%) incidence of inflammatory toxicities (such as colitis and hypophysitis), these conditions are usually straightforward to manage and considered acceptable risks, given the clear likelihood for sustained antitumour activity. immunogenicity of dying tumour cells and the generation of antitumour immune responses by the host. Moreover, they have enabled the therapeutic manipulation of tumour cells and/or the host to enhance or diminish tumour resistance6–10. The commonly used cell lines in this model either originated spontaneously or were induced by carcinogens in inbred mouse strains, and they have been selected for efficient propagation in vitro and in vivo. Among the most thoroughly characterized are the B16 melan­ oma, CT26 colon carcinoma, 4T1 breast carcinoma, EL4 T lymphoma, Lewis lung carcinoma and methylcholanthrene-induced fibrosarcoma cell lines. When syngeneic mice are injected with these cell lines, they must be sacrificed within a few weeks owing to the rapid formation of large tumours. Subcutaneous implantations are frequently used because of the ease of monitoring tumour growth, but bioluminescent imaging is a powerful tool for observing visceral disease11. This technique allows tumour cells that have been engineered to emit visible light (owing to expression of a luminescent protein) to be detected within live animals using a specialized imaging system. Surgical resection of subcutaneous lesions may allow for spontaneous metastases in some cases, whereas intravenous inoculation is an alternative approach to evaluate disease dissemination to the lung, liver or spleen. Another option is orthotopic injection of the tumour cells, for example the intra­ cranial implantation of glioma cell lines. This approach is advantageous over subcutaneous injection, as it mimics the growth of tumours within a relevant microenvironment. Strengths and limitations. The speed and reproducibility of tumour growth render transplantable cell lines attractive for treatment studies. However, a single bolus of large numbers of tumour cells and the tissue damage associated with injection induce a local inflammatory response that may affect therapeutic responses. Indeed, the intrinsic immunogenicity of transplantable tumour cell lines varies widely, and is perhaps related to differences in the uptake of dying tumour cells by phagocytes and/or in the release of endogenous moieties that activate innate immune receptors12,13. Poorly immunogenic tumours (such as B16 melanomas) thus constitute a more stringent test for intervention than moderately immunogenic lines (such as EL4 T lymphomas)14, although the precise basis for these differences remains to be clarified. Furthermore, immunosuppressive mechanisms may also vary between transplantable tumour cell lines, and again this could potentially affect the outcome of a given intervention. The enforced expression of model antigens (such as ovalbumin) or viral gene products in tumour cell lines provides some advantages over the standard transplantable tumour models. These advantages include the induction of enhanced immuno­ monitoring by T cells and the availability of mice expressing transgenic T cell receptors (TCRs) specific for the model antigen15. However, the increased immunogenicity of foreign antigens owing to decreasing T cell tolerance tempers some of these gains. By contrast, the characterization of endogenous tumour antigens that are recognized by 62 | JANUARY 2012 | VOLUME 12 CD4+ and CD8+ T cells, and the development of experimental tools for investigating these responses against transplantable tumours are important advances for immunotherapy research16–18. Transplantable tumours may be used to evaluate both prophylactic and curative therapies, and ideally the effects of the therapy should be evaluated in multiple models. When testing strategies aimed at cancer prevention, transplantable tumour models provide flexibility in the time at which antitumour immunity is initiated and allow the immune response to be optimized in the absence of tumour-induced immunosuppression19. These advantages facilitate the careful dissection of the cell­ ular and molecular interactions necessary for protective immunity, and allow for the comparison of different therapies that might be applied in settings of minimal residual disease. The therapeutic eradication of well-established transplantable tumours presents complementary challenges20,21. Among these is the requirement for the extremely rapid induction of antitumour effector immune cells that can navigate the tumour vasculature and stroma, infiltrate the growing lesion and overcome a myriad of tumour-derived tolerizing and suppressive factors. Few therapeutic strategies accomplish all of these requirements, and effectuating the regression of advanced lesions typically requires combinatorial approaches that have a substantial risk of toxicity. Clinical correlates. The clinical success of immune-checkpoint blockade (as exemplified by CTLA4 blockade) allows the predictive value of transplantable tumour models for immunotherapy to be examined. First, the ability of ipilimumab, as a monotherapy, to prolong the survival of patients with advanced melanoma affirms the finding that transient, antibody-mediated blockade of CTLA4 potentiates antitumour immunity 22. This result was initially obtained using moderately immunogenic transplantable cell lines, such as TRAMPC1 (also known as pTC1) prostate carcinoma, ovalbumin-expressing EL4 T lymphoma and Sa1N fibrosarcoma cells. This concord­ ance of preclinical and patient data is profound in its implication, as earlier failures of immunotherapy were frequently attributed, at least in part, to a purported inability of transplantable tumour systems to accurately model human antitumour immune responses5. The recent clinical www.nature.com/reviews/immunol © 2012 Macmillan Publishers Limited. All rights reserved PERSPECTIVES Tumour cell Intracranial injection Culture dish Subcutaneous tumour Tail vein injection Metastatic tumour growth in lungs Figure 1 | Transplantable tumour models. A variety of cell lines that represent a range of tumour types are available for study. These lines are easy to grow in culture and rapidly form tumours after Nature Reviews | Immunology inoculation into syngeneic mice. The cells may be inoculated subcutaneously, intravenously or orthotopically to induce tumours in different microenvironments. Therapeutic strategies may be evaluated for protection against subsequent tumour challenge or for eradication of established tumours. results suggest that the earlier failures may have instead primarily reflected a lack of sufficient immunogenicity. In addition, some mechanistic aspects of CTLA4 blockade appear to be conserved between transplantable tumour models and humans. These aspects include the importance of the intratumoural balance of effector and regulatory T cells, and the upregulation of T cell co-stimulatory molecules, such as inducible T cell co-stimulator (ICOS)23–26. This suggests that these parameters could have potential as biomarkers. Notwithstanding the clinical data, CTLA4‑specific monoclonal antibodies administered as a monotherapy displayed minimal efficacy against B16 cells, which are a widely used transplantable model of melanoma22. These findings are in contrast with those obtained using the more immunogenic cell lines mentioned above, and they raise the possibility that the B16 transplantable tumour model might correspond to a subset of more refractory human melanomas. Indeed, most patients with advanced melanoma do not benefit from ipilimumab. Thus, the poorly immunogenic B16 cell line might prove useful for identifying combinatorial strategies that improve the activity of CTLA4 blockade. One such strategy that could be advanced to testing in patients is the combination of CTLA4 blockade with vaccines containing tumour cells that secrete granulocyte–macrophage colony-stimulating factor (GM-CSF), as synergy has been observed between these two therapies27. Albeit less clinically mature than ipilimumab, PD1‑specific blocking anti­ bodies have been shown to stimulate tumour regression in diverse human malignancies, including melanoma, lymphoma and carcin­ omas of the kidney, colon and lung 28,29. Surprisingly, these patient benefits appear to exceed the impact of PD1‑specific blocking antibodies as a monotherapy in a variety of transplantable models. However, coupling PD1‑specific blocking antibodies with tumour vaccines, with adoptive T cell therapy or with other immunoregulatory antibodies has been shown to enhance their activity in several model systems, and this should help to guide further development of these therapies in patients30,31. Overall, investigations of checkpoint blockade in mouse models and humans indicate that transplantable tumours may provide valuable information for clinical translation. A better understanding of the differential activities of therapies in poorly versus moderately immunogenic cell lines may help to identify new approaches to increase patient survival. However, important limitations of these models include the failure to fully recapitulate the toxicities observed in patients treated with checkpoint-blocking therapies and the potential pharmacokinetic and pharmacodynamic differences between mice and humans. NATURE REVIEWS | IMMUNOLOGY Genetically engineered tumour models Studies of tumour formation in immuno­ deficient mice have elucidated many aspects of the endogenous response to tumour growth (FIG. 2), resulting in the concept of immunoediting 32. In this concept, the dynamic interplay between the tumour and the immune response influences disease development, while shaping characteristics of the evolving transformed cells. Diverse outcomes may arise from this interplay, including tumour inhibition, promotion, equilibrium and escape, but the key factors that dictate the overall impact on the disease course remain to be defined. A large number of mouse strains that harbour mutations in immune response genes have been used to investigate the mechanisms associated with immunoediting. In one approach, gene-knockout mice are exposed to carcinogens, and then the frequency of tumour formation and the kinetics of tumour development in these mice are measured. These experiments have underscored a central role in tumour inhibition for T helper 1 (TH1)-type immune responses and cytotoxic T cells, as evidenced by the enhanced tumour susceptibility of mice lacking IFNγ, interleukin‑12 (IL‑12), components of the MHC class I antigen processing and presentation pathways, CD8+ T cells, perforin or granzymes33. In a complementary approach, spontaneous tumour development is assessed in mice as they age, and experiments using this approach have revealed an elevated frequency of haematological malignancies and solid tumours in several knockout mouse strains. Excessive immune responses, however, may increase cancer incidence, in part through the deleterious consequences of unresolved inflammation34. However, crucial, tumour-promoting contributions have been delineated in these models for persistent microbial agents, nuclear factor-κB (NF-κB) and signal transducer and activator of transcription 3 (STAT3) signalling, pro-inflammatory cytokines and chemokines (such as IL‑1, IL‑6, IL‑23, tumour necrosis factor (TNF) and CC‑chemokine ligand 2 (CCL2)), and various immune cell types, including macrophages, mast cells, B cells, forkhead box P3 (FOXP3)+ regulatory T cells and myeloid-derived suppressor cells35–41. Advances in cancer genetics have also given rise to a wealth of new mouse tumour systems that recapitulate the genetic lesions that are characteristic of human cancers. These models capitalize on transgenic technologies that allow for the enforced VOLUME 12 | JANUARY 2012 | 63 © 2012 Macmillan Publishers Limited. All rights reserved PERSPECTIVES a Immunodeficient mouse models MCA-induced fibrosarcoma Inflammationassociated colon carcinoma Spontaneous lung carcinoma b Oncogene-driven models Lung cancer driven by KRAS and a lack of p53 function SV40 large T antigen-driven prostate cancer ERBB2-driven breast cancer Commonly used immunodeficient mice include mice deficient in RAG, IFNγ, NF-κB or STAT3 Figure 2 | Genetically engineered mouse tumour models. a | Immunodeficient mice can have enhanced tumour susceptibility, which may reflect a loss of protective immune responses and/or the development of tumour-promoting inflammation. The figure shows examples of methylcholanthrene (MCA)-induced fibrosarcoma, inflammation-associated colon carcinomaNature and spontaneous lung carcin­ Reviews | Immunology oma. b | The tissue-specific and/or temporally controlled expression of oncogenes or the loss of tumour suppressors can give rise to tumours that recapitulate genetic lesions found in human cancers. The figure shows examples of breast cancer driven by ERBB2, prostate cancer driven by simian virus 40 (SV40) large T antigen (which antagonizes the function of the host p53 and RB proteins), and lung cancer driven by mutations in Kras and Tp53. These systems can be used to evaluate both endogenous and therapy-induced antitumour immune responses. IFNγ, interferon‑γ; NF-κB, nuclear factor-κB; RAG, recombination-activating gene; STAT3, signal transducer and activator of transcription 3. expression of oncogenes and/or the loss of function of tumour suppressors, often in a tissue-specific and/or temporally controlled manner. In this context, the ability to characterize how immune responses to tumours vary in relation to specific cancer genotypes is a significant advance towards deconvoluting the heterogeneity in the crosstalk between the tumour and the host immune system. A recent study used adenoviral vectors encoding Cre recombinase to selectively introduce mutations in the oncogene Kras and the tumour suppressor gene Tp53 in the pulmonary epithelia42. An important role for T cells in attenuating lung tumour formation was established in this system, consistent with other experiments using immunodeficient mouse strains43. The concordance of interactions between the tumour and host immune system in models that traditionally are the workhorses of cancer biologists and cancer immunologists should help to identify common ground for study and to promote broader interactions between these disciplines. Strengths and limitations. Compared with transplantable tumours, genetically engineered mice more faithfully model the multistage pathogenesis of cancer and the intimate interplay between neoplastic cells and tissue microenvironments. However, tumour formation in the transgenic animals is somewhat more variable than the formation of transplantable tumours and requires a longer period of time. Moreover, the continuous expression of transforming genes may restrict the ability of the host to eradicate all malignant cells and could perpetuate inflammatory responses. Despite these limitations, genetically engineered systems have been used to help guide immunotherapy development. For example, antibody-mediated blockade of CTLA4 prolongs survival in a transgenic model of prostate cancer (induced by simian virus 40 (SV40) large T antigen)44, and cancer vaccines and the inhibition of regulatory T cells mediate tumour destruction in breast cancers driven by the kinase ERBB2 (also known as HER2 and neu)45. Such results are qualitatively similar to those obtained using transplantable tumours, but the therapeutic activities of treatment strategies are generally diminished in the genetically modified animals. The basis for this decreased efficacy is not fully understood, but it might include an increased level of tumour tolerance that arises from early and/or persistent transgene expression. In addition, antitumour effector mechanisms may differ between the models; for example, 64 | JANUARY 2012 | VOLUME 12 antibodies have a substantial role in inhibiting breast cancer progression in ERBB2‑transgenic mice, whereas both cell­ ular and humoral immunity is required to confer protection in wild-type, syngeneic animals challenged with ERBB2‑expressing transplantable cell lines46,47. Lastly, mice that are transgenic or deficient for key immunoregulatory molecules provide important systems for deciphering the impact of therapeutic manipulation of these pathways. Clinical correlates. A renewed interest in characterizing the human tumour microenvironment has underscored the importance of intratumoural immune infiltrates. Several clinical pathological studies have delineated a tight association between a high density of CD8+ cytotoxic T cells (and an accompanying TH1‑type gene signature) and favourable patient outcomes in diverse solid and haematological malignancies48–50. Conversely, the presence of mast cells, proinflammatory cytokines and pro-angiogenic myeloid cell populations and the constitutive activation of NF‑κB and STAT3 signalling are linked with many progressive human cancers, which supports the clinical exploration of novel therapeutic strategies targeting these pathways51–53. The conservation of protective and tumour-promoting immune parameters between mouse model systems and clinical samples highlights the predictive value of genetically engineered models for deciphering human antitumour immune responses. Humanized mouse models of cancer Human tumour xenografts that are implanted in immunodeficient mice are widely used in studies of cancer biology and targeted or cytotoxic therapy. However, a meaningful analysis of immuno­therapy is precluded by the impaired or absent adaptive immune responses in the immunodeficient mouse models, which include athymic nude mice, recombination-activating gene-deficient (Rag–/–) mice and NOD-scid Il2rg–/– (NSG) mice. In this regard, substantial effort is currently directed towards reconstituting these mice with a human immune system, and evidence for functional interactions among dendritic cells, B cells and T cells has been obtained54 (FIG. 3). Using such an approach, a recent study demonstrated that human breast carcinomas generate a tumour-promoting microenvironment that involves crosstalk between plasmacytoid dendritic cells and CD4+ TH2 cells, with a www.nature.com/reviews/immunol © 2012 Macmillan Publishers Limited. All rights reserved PERSPECTIVES Human tumour cells Immunodeficient mouse reconstituted with human DCs, B cells and T cells Human tumour xenograft (for example, a human breast tumour) Figure 3 | Humanized mouse tumour models. Human tumour xenografts can be implanted in immuno­deficient mice that have been reconstituted with human immune cells, including dendritic cells Nature immune Reviewsresponse | Immunology (DCs), B cells and T cells. This system can be used to characterize the human that is directed against a human cancer. Potential applications include the optimization of immunotherapy and the identification of crucial immune pathways that promote tumour growth. pro-tumorigenic role for thymic stromal lymphopoietin, OX40 and IL‑13 (REF. 55). In a second example, human T cells engineered to express a tumour-targeted chimeric antigen receptor incorporating CD137‑derived signalling domains were shown to mediate the regression of bulky human tumours propagated in NSG mice56. The potential clinical relevance of these findings was suggested by the striking antitumour effects observed in patients with advanced chronic lymphocytic leukaemia who were treated with autologous T cells expressing a chimeric antigen receptor incorporating CD137 co-stimulatory function (although the antibody-derived targeting moiety was different to that used in the mouse studies)57. Although these examples highlight the potential for humanized mouse models to inform clinical investigations, their role in prioritizing new therapeutic strategies for translation to patients will require additional study. The efficiency of dendritic cell-mediated stimulation of protective B and T cell responses and the extent to which tumour-induced tolerance and/or suppression are recapitulated in these systems are largely unknown. Moreover, the impact of mouse cytokines and cell-surface molecules on human immune cell populations may complicate the interpretation of some experimental results. Nonetheless, further improvements in humanized mice are likely to expand the application of these preclinical models. Perspectives In this brief commentary, I have illustrated how three classes of cancer models each provide crucial insights into the mechanisms of human antitumour immunity and the potential clinical efficacy of immunotherapy. The systems vary considerably in their recapitulation of selected aspects of human carcinogenesis, in the kinetics of tumour development and in the complexity and cost of experimentation (TABLE 1). The relative importance of these differences is likely to depend on the particular issue under investigation and the state of current knowledge. For example, a comparison of potential new checkpoint-blockade strategies might reasonably be initiated using several transplantable tumours of varying immunogenicity, given their convenience and the preclinical results that have been obtained to date using this system. However, the speed of tumour growth in these models might limit the evaluation of combinatorial strategies, especially if the sequence of administration were to prove decisive. In this case, a transgenic system might be preferred in a second stage of characterization, and this would also facilitate a preliminary assessment of the impact of tumour-induced tolerance and immuno­ suppression on treatment activity. Exploratory studies in a humanized mouse model might then follow to allow the confirmation of key experimental findings using clinical samples, as a prelude to subsequent patient testing. This progression, however, is predicated on the convincing evidence that CTLA4and PD1‑specific monoclonal antibodies offer meaningful benefits to patients with cancer. This information permits one to overlook, at least to some extent, the artificial Table 1 | Strengths and weaknesses of experimental tumour models used for cancer immunology research Experimental model Strengths Weaknesses Clinical validation Transplantable tumours • Simplicity of experimentation • Rapid tumour formation and evaluation of therapeutic responses • Limited recapitulation of tumour microenvironment • Checkpoint blockade (CTLA4- or PD1-specific monoclonal antibodies) Genetically engineered tumour models • Tumours harbour genetic lesions found in human cancers • Improved modelling of tumour progression and tumour microenvironment • Tumour-induced tolerance and immunosuppression show similarities to human cancers • Long time period for tumour development and evaluation of therapeutic response • Increased cost and complexity of generating and maintaining transgenic mice • Prognostic importance of intratumoural lymphocyte infiltrates • CTLA4-specific monoclonal antibodies Humanized mice • Human immune populations studied directly • Might be able to capture the heterogeneity of patient responses • Logistically difficult to obtain matched donor and tumour samples • Incomplete reconstitution of human immune response • Impact of mouse-derived factors on human immune cells not fully defined • Expensive • Chimeric antigen receptor T cell technology CTLA4, cytotoxic T lymphocyte antigen 4; PD1, programmed cell death protein 1. NATURE REVIEWS | IMMUNOLOGY VOLUME 12 | JANUARY 2012 | 65 © 2012 Macmillan Publishers Limited. All rights reserved PERSPECTIVES nature of each of these models, which cannot fully recapitulate the complexity of human disease, and to focus instead on lessons gained from these highly tractable platforms. Such a perspective implies that a fuller understanding of human antitumour immune responses will promote more effective application and interpretation of experimental systems. Indeed, the considerable heterogeneity in the human immune system suggests that many more models will need to be developed, and these in turn will inspire further clinical investigation. Glenn Dranoff is at the Department of Medical Oncology and the Cancer Vaccine Center, Dana-Farber Cancer Institute, and the Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts 02215, USA.e-mail: glenn_dranoff@dfci.harvard.edu doi:10.1038/nri3129 Published online 2 December 2011 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. Keir, M. E., Butte, M. J., Freeman, G. J. & Sharpe, A. H. PD‑1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 26, 677–704 (2008). Kantoff, P. W. et al. Overall survival analysis of a Phase II randomized controlled trial of a poxviralbased PSA-targeted immunotherapy in metastatic castration-resistant prostate cancer. J. Clin. Oncol. 28, 1099–1105 (2010). Brichard, V. G. & Lejeune, D. GSK’s antigen-specific cancer immunotherapy programme: pilot results leading to Phase III clinical development. Vaccine 25 (Suppl. 2), B61–B71 (2007). Dougan, M. & Dranoff, G. Immune therapy for cancer. Annu. Rev. Immunol. 27, 83–117 (2009). Ostrand-Rosenberg, S. Animal models of tumor immunity, immunotherapy and cancer vaccines. Curr. Opin. Immunol. 16, 143–150 (2004). Prehn, R. T. & Main, J. M. Immunity to methylcholanthrene-induced sarcomas. J. Natl Cancer Inst. 18, 769–778 (1957). Klein, G., Sjogren, H. O., Klein, E. & Hellstrom, K. E. Demonstration of resistance against methylcholanthrene-induced sarcomas in the primary autochtonous host. Cancer Res. 20, 1561–1572 (1960). Old, L., Clarke, D. & Benacerraf, B. Effect of bacillus Calmette-Guerin (BCG) infection on transplanted tumors in the mouse. Nature 184, 291–292 (1959). Van Pel, A. & Boon, T. Protection against a nonimmunogenic mouse leukemia by an immunogenic variant obtained by mutagenesis. Proc. Natl Acad. Sci. USA 79, 4718–4722 (1982). Basombrio, M. A. Search for common antigenicity among twenty-five sarcomas induced by methylcholanthrene. Cancer Res. 30, 2458–2462 (1970). Craft, N. et al. Bioluminescent imaging of melanoma in live mice. J. Invest. Dermatol. 125, 159–165 (2005). Obeid, M. et al. Calreticulin exposure dictates the immunogenicity of cancer cell death. Nature Med. 13, 54–61 (2007). Apetoh, L. et al. Toll-like receptor 4‑dependent contribution of the immune system to anticancer chemotherapy and radiotherapy. Nature Med. 13, 1050–1059 (2007). Dranoff, G. et al. Vaccination with irradiated tumor cells engineered to secrete murine granulocytemacrophage colony-stimulating factor stimulates potent, specific, and long-lasting anti-tumor immunity. Proc. Natl Acad. Sci. USA 90, 3539–3543 (1993). Gilboa, E. The makings of a tumor rejection antigen. Immunity 11, 263–270 (1999). Hanson, H. L. et al. Eradication of established tumors by CD8+ T cell adoptive immunotherapy. Immunity 13, 265–276 (2000). Overwijk, W. W. et al. Tumor regression and autoimmunity after reversal of a functionally tolerant state of self-reactive CD8+ T cells. J. Exp. Med. 198, 569–580 (2003). 18. Xie, Y. et al. Naive tumor-specific CD4+ T cells differentiated in vivo eradicate established melanoma. J. Exp. Med. 207, 651–667 (2010). 19. Cavallo, F., Offringa, R., van der Burg, S. H., Forni, G. & Melief, C. J. Vaccination for treatment and prevention of cancer in animal models. Adv. Immunol. 90, 175–213 (2006). 20. Zhang, B., Karrison, T., Rowley, D. A. & Schreiber, H. IFN‑γ‑ and TNF-dependent bystander eradication of antigen-loss variants in established mouse cancers. J. Clin. Invest. 118, 1398–1404 (2008). 21. Klebanoff, C. A. et al. Determinants of successful CD8+ T‑cell adoptive immunotherapy for large established tumors in mice. Clin. Cancer Res. 17, 5343–5352 (2011). 22. Korman, A., Peggs, K. & Allison, J. P. Checkpoint blockade in cancer immunotherapy. Adv. Immunol. 90, 293–335 (2006). 23. Quezada, S. A., Peggs, K. S., Curran, M. A. & Allison, J. P. CTLA4 blockade and GM‑CSF combination immunotherapy alters the intratumor balance of effector and regulatory T cells. J. Clin. Invest. 116, 1935–1945 (2006). 24. Hodi, F. S. et al. Immunologic and clinical effects of antibody blockade of cytotoxic T lymphocyteassociated antigen 4 in previously vaccinated cancer patients. Proc. Natl Acad. Sci. USA 105, 3005–3010 (2008). 25. Fu, T., He, Q. & Sharma, P. The ICOS/ICOSL pathway is required for optimal antitumor responses mediated by anti‑CTLA‑4 therapy. Cancer Res. 71, 5445–5454 (2011). 26. Liakou, C. I. et al. CTLA‑4 blockade increases IFNγ-producing CD4+ICOShi cells to shift the ratio of effector to regulatory T cells in cancer patients. Proc. Natl Acad. Sci. USA 105, 14987–14992 (2008). 27. van Elsas, A., Hurwitz, A. & Allison, J. Combination immunotherapy of B16 melanoma using anti-cytotoxic T lymphocyte-associated antigen 4 (CTLA‑4) and granulocyte/macrophage colony-stimulating factor (GM-CSF)-producing vaccines induces rejection of subcutaneous and metastatic tumors accompanied by autoimmune depigmentation. J. Exp. Med. 190, 355–366 (1999). 28. Berger, R. et al. Phase I safety and pharmacokinetic study of CT‑011, a humanized antibody interacting with PD‑1, in patients with advanced hematologic malignancies. Clin. Cancer Res. 14, 3044–3051 (2008). 29. Brahmer, J. R. et al. Phase I study of single-agent anti-programmed death‑1 (MDX‑1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 28, 3167–3175 (2010). 30. Li, B. et al. Anti-programmed death‑1 synergizes with granulocyte macrophage colony-stimulating factorsecreting tumor cell immunotherapy providing therapeutic benefit to mice with established tumors. Clin. Cancer Res. 15, 1623–1634 (2009). 31. Melero, I. et al. Palettes of vaccines and immunostimulatory monoclonal antibodies for combination. Clin. Cancer Res. 15, 1507–1509 (2009). 32. Schreiber, R. D., Old, L. J. & Smyth, M. J. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science 331, 1565–1570 (2011). 33. Vesely, M. D., Kershaw, M. H., Schreiber, R. D. & Smyth, M. J. Natural innate and adaptive immunity to cancer. Annu. Rev. Immunol. 29, 235–271 (2011). 34. Mantovani, A., Allavena, P., Sica, A. & Balkwill, F. Cancer-related inflammation. Nature 454, 436–444 (2008). 35. Grivennikov, S. I., Greten, F. R. & Karin, M. Immunity, inflammation, and cancer. Cell 140, 883–899 (2010). 36. Qian, B. Z. et al. CCL2 recruits inflammatory monocytes to facilitate breast-tumour metastasis. Nature 475, 222–225 (2011). 37. Yu, H., Kortylewski, M. & Pardoll, D. Crosstalk between cancer and immune cells: role of STAT3 in the tumour microenvironment. Nature Rev. Immunol. 7, 41–51 (2007). 38. Marigo, I. et al. Tumor-induced tolerance and immune suppression depend on the C/EBPβ transcription factor. Immunity 32, 790–802 (2010). 39. Schioppa, T. et al. B regulatory cells and the tumorpromoting actions of TNF-α during squamous carcinogenesis. Proc. Natl Acad. Sci. USA 108, 10662–10667 (2011). 40. Rabinovich, G. A., Gabrilovich, D. & Sotomayor, E. M. Immunosuppressive strategies that are mediated by tumor cells. Annu. Rev. Immunol. 25, 267–296 (2007). 66 | JANUARY 2012 | VOLUME 12 41. Zou, W. Regulatory T cells, tumour immunity and immunotherapy. Nature Rev. Immunol. 6, 295–307 (2006). 42. DuPage, M. et al. Endogenous T cell responses to antigens expressed in lung adenocarcinomas delay malignant tumor progression. Cancer Cell 19, 72–85 (2011). 43. Dougan, M. et al. A dual role for the immune response in a mouse model of inflammation-associated lung cancer. J. Clin. Invest. 121, 2436–2446 (2011). 44. Hurwitz, A. A. et al. Combination immunotherapy of primary prostate cancer in a transgenic mouse model using CTLA‑4 blockade. Cancer Res. 60, 2444–2448 (2000). 45. Ercolini, A. M. et al. Recruitment of latent pools of high-avidity CD8+ T cells to the antitumor immune response. J. Exp. Med. 201, 1591–1602 (2005). 46. Rovero, S. et al. DNA vaccination against rat Her‑2/Neu p185 more effectively inhibits carcinogenesis than transplantable carcinomas in transgenic BALB/c mice. J. Immunol. 165, 5133–5142 (2000). 47. Reilly, R. et al. The collaboration of both humoral and cellular HER‑2/neu-targeted immune responses is required for the complete eradication of HER‑2/neuexpressing tumors. Cancer Res. 61, 880–883 (2001). 48. Zhang, L. et al. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N. Engl. J. Med. 348, 203–213 (2003). 49. Galon, J. et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 313, 1960–1964 (2006). 50. Wahlin, B. E. et al. A unifying microenvironment model in follicular lymphoma: outcome is predicted by programmed death‑1‑positive, regulatory, cytotoxic, and helper T cells and macrophages. Clin. Cancer Res. 16, 637–650 (2010). 51. Ruffell, B. et al. Leukocyte composition of human breast cancer. Proc. Natl Acad. Sci. USA 8 Aug 2011 (doi:10.1073/pnas.1104303108). 52. Qian, B. Z. & Pollard, J. W. Macrophage diversity enhances tumor progression and metastasis. Cell 141, 39–51 (2010). 53. Ferrone, C. & Dranoff, G. Dual roles for immunity in gastrointestinal cancers. J. Clin. Oncol. 28, 4045–4051 (2010). 54. Legrand, N. et al. Humanized mice for modeling human infectious disease: challenges, progress, and outlook. Cell Host Microbe 6, 5–9 (2009). 55. Pedroza-Gonzalez, A. et al. Thymic stromal lymphopoietin fosters human breast tumor growth by promoting type 2 inflammation. J. Exp. Med. 208, 479–490 (2011). 56. Carpenito, C. et al. Control of large, established tumor xenografts with genetically retargeted human T cells containing CD28 and CD137 domains. Proc. Natl Acad. Sci. USA 106, 3360–3365 (2009). 57. Kalos, M. et al. T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Sci. Transl. Med. 3, 95ra73 (2011). 58. Higano, C. S. et al. Integrated data from 2 randomized, double-blind, placebo-controlled, phase 3 trials of active cellular immunotherapy with sipuleucel‑T in advanced prostate cancer. Cancer 115, 3670–3679 (2009). 59. Kantoff, P. W. et al. Sipuleucel‑T immunotherapy for castration-resistant prostate cancer. N. Engl. J. Med. 363, 411–422 (2010). 60. Hodi, F. S. et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 363, 711–723 (2010). 61. Robert, C. et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N. Engl. J. Med. 364, 2517–2526 (2011). Acknowledgements Glenn Dranoff is supported by grants from the US National Cancer Institute, the Leukemia and Lymphoma Society, the Melanoma Research Alliance, the Alliance for Cancer Gene Therapy and the Research Foundation for the Treatment of Ovarian Cancer. Competing interests statement The author declares no competing financial interests. FURTHER INFORMATION Glenn Dranoff’s homepage: http://www.hms.harvard.edu/ dms/immunology/fac/Dranoff.php ALL LINKS ARE ACTIVE IN THE ONLINE PDF www.nature.com/reviews/immunol © 2012 Macmillan Publishers Limited. All rights reserved Copyright of Nature Reviews Immunology is the property of Nature Publishing Group and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.