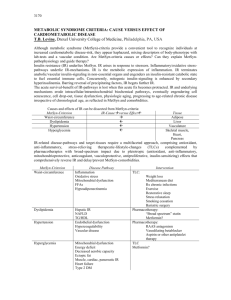
Optimal Lab Interpretation - Blood Chemistry The ranges and information contained within this sheet are for informational and educational purposes only. Please see a licensed healthcare practitioner before making any changes to your current lifestyle. The ranges contained within this sheet are nutritional ranges, they are not designed to diagnose, treat, or cure any disease. Acceptance of these ranges varies among practitioners. Lab CBC w/Differential HGB Optimal F=Female M=Male F: 13.5-14.5g /dL M: 14-15 g/dL High Levels Low Levels Cardiac dysfunction, excessive RBC, immune suppression, lung dysfunction, hemoglobin production abnormality, bleeding, hemolysis, liver dysfunction, kidney dysfunction Shock, immune suppression, excessive RBC Decreased levels of RBC, RBC abnormality, hemoglobin production abnormality, bleeding, hemolysis, liver dysfunction, kidney dysfunction, bone marrow dysfunction HCT F:37-44 M:40-48 RBC F:3.9-4.5 Excessive RBC, dehydration, M:4.2-4.9 renal dysfunction, high altitude, lung dysfunction, immune suppression, cardiovascular dysfunction MCV 85-92 fL/red cell MCH 27-32 pg/cell B12/folate need, high altitude, increased methylmalonic acid and homocysteine B12/folate need, new born infants, RBC abnormality MCHC 32-35 g/dL B12/folate need, new born infants, RBC abnormality Decreased levels of RBC, abnormal breakdown of RBC, immune suppression, increased levels of WBC, adrenal dysfuntion, acute blood loss Decreased levels of RBC, immune suppression, hemorrhage, adrenal dysfunction & cortisol production dysfunction, chronic bacterial infections B6 need, bleeding, decreased levels of RBC, free radicals, parasites B6 need, RBC abnormality Decreased levels of RBC, B6 need, abnormal hemoglobin production 1 Lab RDW Optimal High Levels Neut. B12 and iron need, immune suppression, abdnormal hemoglobin 150,000- Over production of platelets, 450,000 excessive RBC production, increased immature WBC, splenectomy 5.0-8.0 billion /L 40%-60% Bacteria Lymph. 25%-40% Virus Mono. <7 Infections, heavy metals Eos. <3% Allerigies, parasites Baso. 0%-1% Platelets WBC Low Levels <13 Use sesame seed oil Adrenal dysfunction Thyroid TSH 1.8-3.0 uU/mL Total T4 6-12 mcg/Dl Free T4 1.0 - 1.5 ng/dL 100-180 ng/dL Total T3 FTI 1.2-4.9 Free T3 3.0-4.0 pg/ml T3 Uptake 28-38 % Rev. T3 9-35ng/ mL 20+ T3:RT3 Ratio Decreased thyroid hormone levels Pituitary dysfunction, gut infections, excessive production of thyroid hormone Increased thyroid hormone Overly high protein levels in levels, increase in thyroid the blood, decreased thyroid binding globulin, hormone levels, decreased hepatitis/liver, acute thyroid binding globulin, thyroditis, thyroid medication thyroid medication Increased thyroid hormone levels High cortisol levels, inflammation, third trimester pregnancy, pituitary dysfunction Decreased thyroid hormone levels, need selenium High cortisol levels, inflammation, third trimester pregnancy, pituitary dysfunction TSI TPO AB 0 Autoimmune / GI TGB AB 0 Autoimmune / GI 2 Lab Optimal High Levels Low Levels CMP Glucose 85-100 mg/dL Sodium 135-140 mEq/L Potasium 4-4.5 mEq/L Chloride 100-106 mmol/L 25-30 mmol/L Co2 Calcium 9.2-10.1 mg/dL Excess glucose in the low blood glucose levels, bloodstream, blood sugar adrenal dysfunction & cortisol issues, pituitary dysfunction, production dysfunction, liver pregnancy, increased blood dysfunction, pituitary iron levels, inflammation of dysfunction, decreased levels the pancreas, thiamin need of thyroid hormone dehydration, renal Low salt diet, diarrhea, dysfunction, water softners, cardiac dysfunction, burns, excessive aldosterone adrenal dysfunction & cortisol production, pituitary production dysfunction, dysfunction, blood sugar malabsorption, edema issues Low adrenal function, renal Diurtetic use, excessive dysfunction, tissue adrenal function, renal destruction, dehydration, dysfunction, blood sugar blood sugar issues, acidosis issues, excessive alcohol use, starvation, alkalosis Alkalosis, excessive secretion Acidosis, asprin use, renal of aldosterone, lung & dysfunction, use of diuretics, alveolar dysfunction, starvation, diarrhea vomiting hyperthyroid/parathyroid, Pregnancy, bone weakening excessive Vit. D, bone cell issues, thyroid/parathyroid remodeling/deformity issues, dysfunction, magnesium immune suppression, need, Vit. D need, increased immature WBC, inflammation of the pancreas malabsorption, alcohol BUN Creatinine 0.7-1.1 mg/dL Alk Phos 27-90 iU/L Dehydration, renal dysfunction, enlarged prostate, uterine problems, increased growth hormone, neuromuskuloskeletal conditions, autoimmune issues Gut inflammation, liver dysfuntion, increased bone growth, gastric inflammation, cardiovascular issues, immune suppression, excessive production of Pregnancy, bone growth, protein need, liver dysfunction, glutathione need, methylation 3 thyroid hormone, lung dysfunction Lab Optimal SGOT (AST) 10-26 iU/L SGPT(ALT) 10-26 iU/L Albumin Globulin 4.0-5.0 g/dL 2.4-2.8 A/G Ratio 1.5-2.0 High Levels Low Levels Cardiac/muscle/liver B6 need dysfunction, virus, inflammation of the pancreas, parasitic activity, mushroom poisoning Liver dysfunction, bile duct Malnutrition, infections of the dysfunction, inflammation of urinary tract the pancreas Dehydration Liver dysfunction, Vit. C need, free radicals Increased need for HCL, Liver dysfunction, digestive Typhoid fever, parasites, inflammation, HCL Need, immune suppression, Severe hemorrhage, severe lymphatic infection decrease in RBC levels Dehydration Burns, kidney dysfunction, lung & alveolar dysfunction, viral infections, excessive production of thyroid hormone, inflammation of the peritoneum, intestial obstruction Lipid Panel Cholesterol 150-200 mg/dL Triglycerides 75-100 mg/dL LDL <120 HDL >55 Type 4 Diabetes, thyroid, carbs, chronic renal failure, Type 2 Diabetes, gallbladder dysfunction, liver/alcohol/pancreatic dysfunction Insulin resistance, alcohol, high carb intake, estrogen, defect/deficient LPL or APO-C2, blood sugar issues, thyroid dysfunction high carb intake, alcohol use, Type 2 Diabetes, high fat diet, blood sugar issues, eating disorders, renal dysfunction Vegetarianism, autoimmunity, free radicals, excessive production of thyroid hormone, abnormal RBC production, liver dysfunction Autoimmune issues, liver dysfunction, lung dysfunction, Cystic Fibrosis abnormally low levels of lipid in the blood, severe reduction in HDL in the blood, excessive production of thyroid hormone Autoimmunity, liver blood sugar issues, obesity, dysfunction, increased lipid high carb intake, lack of levels in the blood, long term exercise, high levels of exercise lipoproteins in the blood, Apo 4 C-3 dificency, cardiac dysfunction Lab Optimal Chol/HDL Ratio <3.1 HDL/LDL Ratio >.4 High Levels Low Levels Cardiovascular issues, Type 2 Liver dysfunction, excessive Diabetes, increased lipid in production of thyroid the blood, diabetes, renal hormone, long-term exercise, dysfunction inflammation, infections Additional Labs Homocysteine 5.5-8 umol/L HgBA1c <5.2 Uric Acid F:3.2-5.5 mg/dL M:3.7-6.0 mg/dl <1.0 mg/L Lab ranges HS-CRP RBC Folate MMA % Free Copper Lab ranges >6.0 mg/dl 80-100 ug/dl 25-40 mg/dL 100-140 ug/dL 0.53-0.91 mg/L 9-14.7 mg/L 40-70 ng/mL <15 Zinc/CU ratio 1.3:1 Magnesium RBC Copper, Serum Ceruloplasmin Zinc, Serum Copper, RBC Zinc, RBC Histamine Cardiovascular issues, hypo-methylation, oxidative stress, mood dissorders, and numerous other issues. Blood sugar issues, insulin resistance Low glutathione and CoQ10 need. Low Glutathione, Toxic exposure, or SNP upregulation Inflammation/ gut/ infection/ poor diet MTHFR, FOL, SLC19A1 SNPs. Folate is unable to get into the cell. Adeno-B12 Need Magnesium need 5 Lab Vit. D 1,25 (OH) Vit. D 25(OH) Ratio 1,25D:25D Ionized Ca Optimal High Levels Low Levels 22-75 ng/mL 35-80 ng/mL 1.5-2.0 Lab Ranges Iron Ferritin TIBC % Sat Fibrinogen Galectin-3 20-50 ng/mL 250-350 mcg/dL 25%-30% 250-350 (mg/dl) <12.9 Inflammatory marker that, (ng/ml) when elevated, systemic enzymes (Vitalzym XE) and modified citrus pectin (MCP-Pectasol) often are needed until the root cause of elevation is found. Hormones IGF-1 220+ Estriol (E3) EQ (E3 / (E1+E2) Pregnenolone 130+ Progesterone (Pg) Pg/E2 Ratio Testosterone, Free Testosterone DHEA 300-500 DHEAS 200-400 LH FSH 6 Lab Optimal High Levels Low Levels Infectious / Autoimmune / Inflammatory Panels Immunoglobulin G Immunoglobulin M EBV VCA AB (IGM) EBV EA AB (IGG) EBV VCA AB (IGG) EBV EBNA AB (IGG) Complete Cytokine Assay Candida Antibodies Helicobacter IgG panel Hep A, B, and C titers Breakout of Cytokine panel ESR RA factor SLE screen T Lymphocite Helpter supporessor assay IL 8, IL1 B or TNF alpha analysis Cancer history of colon, breast and ovary CEA for colon cancer CA 125 for ovarian cancer CA 27.9 for breast cancer AFP blood test CA125, 15-2, 27.29, 19.9 BRCA 1 and 2 screen Previous Heart Disease Apo A-1 and B B Natriurietic Factor LpA status, Lp-PLA2 CIMT 7 Calcium Index Score Lab Optimal High Levels Low Levels Bonus: Optimal Hormone Levels from StopTheThyroidMadness.com This information comes from https://stopthethyroidmadness.com/lab-values/ Iron / Total Iron % Iron Saturation US: Close to 110 for women, upper 130s for men; UK / AU: lower to mid-20s for women; CAN: Mid-20s for women, higher for men close to 35% for women, 40-45% for men If you are considerably higher than optimal, you could have the MTHFR mutation which will need testing and treatment. The MTHFR mutation also drives the ferritin low with normal or high iron is many of us, we’ve noted. If all three iron labs are high (serum iron, % saturation, and ferritin, you may have the genetic hemochromatosis and you can ask your doctor for testing for that. Measures your serum iron divided by your TIBC. Like all iron labs, you should be off all iron for at least 12 hours before testing to see how your supplementation is doing, or up to 5 days to see what your natural levels are. The latter may be best. NOTE: % Saturation can look falsely good or high if your TIBC is too low!! 8 Lab TIBC Optimal High Levels Low 300s (ref range: 250-450) - for other ranges, a little more than 1/4th above the bottom number in the range provided. CAN: when range is umol/L >45-77=lo w 60s; range us 50-70 umol/L= bottom 1/4th above bottom of range TIBC measures whether a protein called transferrin, produced by the liver, is enough to carry iron in the blood. Used to determine anemia or low body iron. If your result is high in the range and in the absence of chronic disease, you may be anemic. NOTE we do NOT treat the TIBC. We treat the iron and % Sat. The TIBC just gives us interesting information as explained. Low Levels 9 Lab Optimal High Levels Low Levels 10 Ferritin Lab 70-90 for women; slightly above 100 for men Measures your levels of storage iron. NOTE THAT WE DO NOT TREAT the FERRITIN LEVEL. A mistake. We treat iron and % saturation and let ferritin follow in its own accord. But ferritin is interesting to watch, and can also point to INFLAMMATION if it goes high without serum iron being high. i.e. inflammation causes iron to be thrust into storage, and inflammation is common with certain thyroid patients for a variety of reasons. In less common cases, higher ferritin can be from liver disease, alcoholism, diabetes, asthma, or some types of cancer. But for most of us, it’s just about inflammation from hypothyroidism, or gluten issues, or unknown. So we need to lower the inflammation before taking iron supplements. If ferritin is high along with a high % Sat and Serum iron, you may have hemochromatosis, an inherited condition. Time to get tested in working with your doctor. If your ferritin is low along with inadequate/lower levels of iron and % saturation, that usually points to simply low iron, which is common with those on T4-only meds, or undiagnosed, or under-treated. But we do NOT treat that low ferritin. We treat the inadequate iron and % saturation, and over time, the ferritin moves up by itself if it’s too low. If your ferritin is low with very good or high iron, plus a TIBC in the middle 300s or higher, that usually points to having high heavy metals and an active MTHFR mutation. Optimal High Levels Low Levels 11 FEMALE HORMONES 20-22 Progesterone (Pg) ng/mL cycling women Progesterone (Pg) non-cycling women Lab (US) serum 64-70 nmol/L( UK) serum 250-300 pg/mL (US) saliva 1100-130 0 pmol/L (UK) saliva 8-10 ng/mL (US) serum 25-32 nmol/L (UK) serum 100-125 pg/mL (US) saliva 440-585 pmol/L (UK) saliva Optimal High Levels Low Levels 12 Estradiol - cycling women with normal SHBG 80-100 pg/mL (US) serum 294-367 pmol/L (UK) serum 1.30-1.50 pg/mL (US) saliva 3.70-6.50 pmol/L (UK) saliva 20-40 Estradiol non-cycling women pg/mL (US) with normal SHBG serum 73-147 pmol/L (UK) serum 0.40-0.60 pg/mL (US) saliva 1.50-3.00 pmol/L (UK) saliva NOTE: Women with high SHBG can have slightly higher estradiol. i.e. when SHBG is high (>160 or so), some need a level of 150-160 blood to feel well. As a noncycling woman with higher SHBG, some might need a level of 50-80. FSH LH <10 mIU/mL good/healthy egg reserve (nowhere close to meno–chance of conception, <3 excellent, 3-6 good, 6-9 fair) FSH/LH 10-15 conception difficult but not impossible FSH/LH 15-20 perimenopause (probably not ovulating every month) FSH/LH 20-30 menopause almost certainly in progress (ovulation rare if at all regardless of bleeding) FSH/LH > 30 noncycling/postmenopause 13 NOTE: FSH and LH for cycling women should be 1:1 ratio. If LH is higher, that typically means PCOS. Labs must be taken day 2-4 of the cycle while bleeding. 2.10-3.20 Free testosterone pg/mL (US) serum 7.30-11.00 pmol/L (UK) serum 108-149 pmol/L (UK) saliva 36-47 pg/mL (US) saliva 0.04-0.05 nmol/L serum 1.10-1.50 ng/dL serum 28-38 Total testosterone ng/dL (US) serum 1.00-1.32 nmol/L (UK) serum 36-47 pg/mL (US) saliva 108-149 pmol/L (UK) saliva 75-95 SHBG nmol/L Lab Optimal High Levels Low Levels 14 DHEA (in the absense of adrenal fatigue or PCOS) B-12 Serum 175-225 ug/dL Saliva > 13ng/mL upper quartile We noticed repeatedly that an optimal B12 lab result is in the upper quarter of the range. Mid-range can present symptoms of inadequate levels, such as legs falling asleep too easily, or the same with little fingers or other fingers. It has been shown in studies that patients with labs under 350 are likely to have symptoms, which means the deficiency is very serious and has gone on for a few years undetected. Even mid-range has shown to be in adequate. Lab ranges are much too low for B12…in Japan the bottom of the range is 500. The urine test Urinary Methylmalonic Acid, also called the UMMA, can be added since it is a very sensitive detection and if high, will reveal a true B12 deficiency. NOTE: Measures an essential vitamin, B12, which can be low in hypothyroid patients due to low stomach acid. It is NOT optimal to simply be “in range”. For example, if your range is similar to 180-900, a healthy level appears to be 800 or higher. In the 500-800 range, you can benefit from taking B12 lozenges, specifically Methylcobalamin. The exception to the latter for some may be if they have both an MTHFR and COMT mutation–the methyl version of B12 can sometimes send out B12 levels way too high. Folate Top third of standard range (3-17); higher for MTHFR 15 Also sometimes called “folic acid”, this is a b-vitamin which can be low in hypothyroid patients. Folate is important for prenatal development, as well as your blood cell health. Folate works with B12 in the use and creation of proteins. It’s “folate” thats needed instead of “folic acid”, especially if you have MTHFR. We don’t start too high, as for some of us, it can start the methylation process too strongly. Lab Optimal ALT AST Magnesium teens Vit D (25 hydroxy) 60-80 High Levels Low Levels teens mid-rang e or higher Thyroid patients can be chronically low in the electrolyte magnesium, which causes a multitude of problems ranging from worsened Mitral Valve Prolapse, less cancer protection, poor muscle development, too much calcium, cramping, and many other chronic conditions. See Janie’s blog post on magnesium. Close to Sodium 142 Can also be strongly related to your adrenals and aldosterone: Measures the levels of the electrolyte sodium, which is outside cells, and has a balance with potassium, which is within cells. Sodium regulates bodily fluid and plays role in major bodily functions. This can be strongly related to whether you have low aldosterone or not. 4.2 or Potassium higher; upper 70-95% of the range Measures the electrolyte mineral Potassium, which is within cells, and has a balance with sodium, which is outside cells. Potassium plays a role in healthy kidney, heart and nervous system function. When potassium is too high, it’s called hyperkalemia; when too low, hypokalemia. It can rise in the presence of low aldosterone (see above under Adrenals), then fall. Best to do an RBC potassium–red blood cell—which measures it in your cells.Tell the lab tech NOT to use the tourniquet for drawing blood. It can falsely raise your potassium result. Measures the enzyme If both hormones are low in Renin hormone that regulates the the range, you ‘may’ a release of aldosterone and is pituitary problem. Always done in conjunction with the tested along with Aldosterone aldosterone test. If renin is to see if your problem is due high in the range along with a to the adrenals (primary low aldosterone, you have an adrenal insufficiency) or your adrenal cause. pituitary (secondary adrenal insufficiency). 16 Vitamin D plays a role in your immune system and other important actions. Many thyroid patients are low in D due to digestive issues from being undiagnosed or undertreated, plus problems with Celiac or gluten intolerance. When someone overreacts to Vit D supplementation, it seems to point to a parathyroid problem. Lab Optimal High Levels Low Levels Zinc Top third of the range Also important to test your RBC Zinc to see your cellular levels, because you have good-looking serum zinc and low RBC zinc! 17