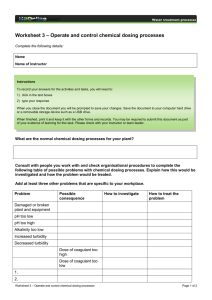
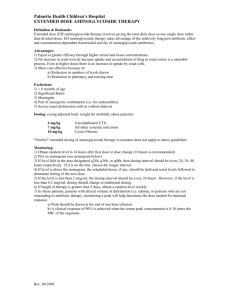
Consider adjunctive prn Benzodiazepine: Clonazepam or Lorazepam; ideally <4 weeks Severe anxiety Generalized Anxiety Disorder Comorbid depression? (Bus pirone offers m ore be nign SE profile; le ss effective w ith hx of Benzodiazepine us e ) Buspirone/SSRI/SNRI No Yes Combination Cognitive-behavioral therapy, acceptance and commitment therapy (if available in community) SSRI or SNRI Follow up and titrate dose as appropriate q 1-2 weeks for active medication management Inadequate response (< 50% improvement) Max dose NOT achieved due to side effects Partial Response Max dose achieved with inadequate response (<50% improvement) Partial Response On SSRI/SNRI? Buspirone montherapy? Switch to SSRI/SNRI Yes No Adequate response (≥ 50% decrease in symptoms) Continue SSRI/SNRI; augment with Buspirone On buspirone monotherapy? Continue Buspirone; add SSRI/SNRI First time failing an SSRI or SNRI? Yes Trial of different medication No Discontinue current medication Follow up and titrate dose as appropriate q 1-2 weeks for active medication management Partial response Continue SSRI/SNRI and Buspirone Begin Mirtazapine Inadequate response Stop Mirtazapine and start either: Quetiapine Pregabalin/Gabapentin Inadequate response Try other agent Inadequate response after trying both agents Stop above agent and start either: TCA Maintain effective pharmacotherapy for minimum of 12 months; if asymptomatic for 4-6 months, consider slow taper Consider TCA prior to chronic benzodiazepines Imipramine most studied, other TCAs reasonable Benzodiazepine Clonazepam Lorazepam Adequate response (≥ 50% decrease in symptoms) GENERALIZED ANXIETY DISORDER Anxiolytic SSRI Antidepressants Buspirone BuSpar DOSING: Start 7.5mg BID or 5mg TID, increase by increments of 5mg/day every 2-3 days to target dose 20mg-30mg/ day divided BID or TID; max dose 20mg TID. May also be used as a prn. SIDE EFFECTS: (common) dizziness, nausea, headache, jitteriness DOSING: See agent descriptions. SIDE EFFECTS: (common) nausea, headache, weight gain, sexual side effects; (rare, serious) hyponatrema, GI bleeding, serotonin syndrome Escitalopram Lexapro Fluoxetine Prozac DOSING: Start 10mg in AM, wait a few weeks to assess response before increasing, max dose 80mg/day. NOTE: Off-label for GAD. Paroxetine Paxil DOSING: Start 10mg/day, wait a few weeks to assess response before increasing, can increase by 10mg/day once/week; max dose 60mg/day. Sertraline Zoloft Citalopram Celexa SNRI Antidepressants DOSING: See agent descriptions. SIDE EFFECTS: (common) nausea, dry mouth, dizziness, headache, sexual side effects DOSING: Start 5 mg/day, increase slowly up to 20mg/day if necessary, once daily dosing. DOSING: Start 25mg/day, increase to 50mg/day after one week if necessary, thereafter wait a few weeks to assess response before increasing; max dose 200mg/day, single dose. NOTE: Off-label for GAD. DOSING: Start 10mg/day, may increase to 20mg/day after one week if necessary; max dose 40mg/day. Do not exceed 40mg/day due to reports of QTc prolongation. NOTE: Off-label for GAD. Duloxetine Cymbalta DOSING: Start 20mg/day, divided or in a single dose, increase slowly; max dose 60mg/day. SIDE EFFECTS: (rare, serious) hepatic failure, orthostatic hypotension, syncope Venlafaxine Effexor XR DOSING: Start 37.5mg/day, increase by 37.5mg/day at weekly or longer intervals; max dose 225mg/day. SIDE EFFECTS: (rare, serious) hypertension, SIADH Other Antidepressant Mirtazapine Remeron Atypical (SGA) Antipsychotics Quetiapine Seroquel ER DOSING: Start 12.5mg-25mg/day, increase by 12.5mg-25mg at weekly intervals as necessary, max dose 150mg/day. SIDE EFFECTS: (common) hypotension, dry mouth, weight gain/ hyperlipidemia/ diabetes, dizziness; (rare, serious) orthostatic hypotension, NMS, TD NOTE: Off-label for GAD. Novel Anticonvulsants Pregabalin Lyrica DOSING: Start 75mg BID and increase as tolerated; max dose 300mg BID. SIDE EFFECTS: (common) peripheral edema, dizziness, weight gain; (rare, serious) hypersensitivity reactions, angioedema NOTE: Off-label for GAD. Tricyclic Antidepressant Benzodiazepines DOSING: Start 7.5mg QHS, increase by 7.5mg every 1-2 weeks as necessary and as tolerated; max dose 45mg/day. SIDE EFFECTS: (common) weight gain, somnolence; (rare, serious) agranulocytosis, severe neutropenia NOTE: Off-label for GAD. Gabapentin Neurontin DOSING: Start 100mg QHS, increase as tolerated to 300mg TID; max dose 3600mg/day. SIDE EFFECTS: (common) dizziness, weight gain, somnolence; (rare, serious) DRESS NOTE: Off-label for GAD. Imipramine Tofranil DOSING: Start 25mg QHS, increase as tolerated by 25mg/day; max dose 150mg-200mg/day. SIDE EFFECTS: (common) sedation, dry mouth, constipation, weight gain, sexual side effects; (rare, serious) seizures, cardiac effects, fatal in overdose NOTE: Off-label for GAD. DOSING: See agent descriptions. SIDE EFFECTS: (common) somnolence, grogginess, ataxia, abuse potential; (rare, serious) anterograde amnesia, fall risk, respiratory depression, paradoxical reaction Clonazepam Klonopin DOSING: Start 0.25mg BID; increase to 1mg/day after 3 days. Dose either BID or once at HS. Use the lowest possible effective dose for the shortest possible period of time. NOTE: FDA indicated for panic disorder. Lorazepam Ativan DOSING: Start 0.25-0.5mg BID, increase by 0.25mg-0.5mg increments every few days to max 6mg/day divided BID or TID. Use the lowest possible effective dose for the shortest possible period of time.