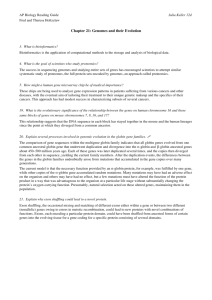
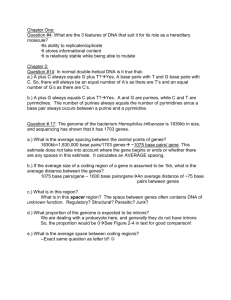
Questions for further study and thinking 1. How does g gene expression protect against b-thalassemia? 2. What is the most likely phenotype of a child with a genotype / , b/-? How about a child having the genotype / , b/-? 3. (Optional!!) Describe mechanisms that could account for the high frequencies of -thal and b-thal mutations in local population. (Hints: selection, genetic drift and founder effects) Ref: Thompson and Thompson Genetics in Medicine, 6th ed., 2004, chapter 7 (Genetic variation in populations) 4. Suppose the incidence of b-thalassemia major is 0.01% in the local population. What is the carrier rate of b-thalassemia mutation? (Hint: Hardy-Weinberg equilibrium: p2 + 2pq + q2 = 1) (See slide 48 for answer.) 39 Suggested textbooks: • Nussbaum, R.L. et al.: Thompson & Thompson Genetics in Medicine, 6th ed. Saunders, 2004 (chap. 11: Principles of Molecular Disease: Lesson from the Hemoglobinopathies) • Gelehrter, T.D. et al.: The Principles of Medical Genetics, 2nd ed. Williams and Wilkins,1998 (chap. 6: Molecular Genetics of Human Disease: Hemoglobinopathies) • NCBI Books: GeneReviews ( and b thalassemia); Human Molecular Genetics 2 (chap. 16) Go back to basic (NCBI Books have earlier version): Lewin’s Gene XI 2014 Molecular Biology of the Cell 2014 Stryer Biochemistry 7th ed 2012 (chaps. 7 and 29) Molecular Cell Biology 7th ed 2013 40 References and further reading • 1) 2) 3) 4) Recent review articles N. Eng. J. Med. 353:1135-1146, 2005 (“b-thalassemia”) N. Eng. J. Med. 371:1908-1916, 2014 (“ -thalassemia”) Lancet 391:155-167 2018 (“Thalassaemia”) Blood 112:3927-3938, 2008 (“Hemoglobin research and the origins of molecular medicine”) • 1) Books for specialists (extended reading for your own interest only) Stamatoyannopoulos G et al.: The Molecular Basis of Blood Diseases, 3rd ed., Saunders, 2001 2) Weatherall, D.J. and Clegg, J.B.: The Thalassaemia Syndromes, 4th ed., Blackwell, 2001 3) Steinberg M.H. et al.: Disorders of Hemoglobin: Genetics, Pathophysiology and Clinical Management, Cambridge, 2001 • Websites Globin Gene Server: http://globin.cse.psu.edu/ NCBI OMIM: http://www.ncbi.nlm.nih.gov/ Bloodline: http://www.bloodline.net/ 41 Learning Outcomes By the end of the lecture (and after the Biochemistry Practical, PBL and your study), you should be able to: • Define the organisation of the α- and β- globin gene clusters • Outline the molecular and genetic basis of α- and βthalassemia • Correlate genotypes with phenotypes in α- and βthalassemia Discuss the molecular mechanisms of β-thalassemia Understand the scientific basis of its diagnosis and treatment • • - and b-globin gene clusters The genomic structure of the clusters of -like and β-like globin genes, on chromosomes 16 and 11, in human beings. The functional -like genes are shown in dark blue and the pseudogenes are in light blue; 2 of these (µ and -1) code for small amounts of RNA. The functional β-like genes are shown in light green. The important control elements, HS-40 and the LCR, are also shown at their approximate locations. The -gene cluster is approximately two thirds of the length of the β-gene cluster; it is transcribed from telomere toward centromere, the opposite of the β cluster. The various hemoglobin species that are formed from these genes, with their prime developmental stages, are shown in the lower part of the figure. Illustration by Alice Y. Chen. (Legend to slide 5) - thalassemias: genotypes and phenotypes Genotype-phenotype relationships in -thalassemias: In rare cases, hemoglobin H (HbH) disease or hemoglobin Bart's hydrops fetalis can result from homozygosity for nondeletional forms of α-thalassemia. Although HbH disease is usually symptomatic, some patients, particularly those with deletional variants of α-thalassemia, are asymptomatic. Furthermore, three α-globin gene deletions involving severe nondeletional mutations (e.g., hemoglobin Constant Spring) can also cause the hemoglobin Bart's hydrops fetalis syndrome. With regard to the lethality of hemoglobin Bart's hydrops fetalis, four α-globin gene deletions with persistence of an intact embryonic ζ-globin gene — for example, –(α)20.5 in the Mediterranean area — may be associated with neonatal survival. (NEJM 2014; Legend to slide 8) 43 Developmental switches of globin expression The timeline of the expression of the human globin genes from early stages of fetal development to the changes that occur at birth and in the first year of life. Also shown are the major sites of erythropoiesis and the types of hemoglobin-containing cells during these periods. These analyses are largely based on observations of clinical samples made by Huehns et al. in the 1960s; the figure is reprinted from Wood (Br Med Bull. 1976;32:282) with permission. Illustration by Alice Y. Chen. (Legend to slide 6) Normal developmental switches in globin expression. (A) The structure of the α-like and β-like globin gene clusters. IVS=intervening segments (or introns). (B) The sites of hemopoiesis at different stages of development and the levels of expression of the embryonic, fetal, and adult globin chains at various gestational ages are shown. ψ designates non-expressing pseudogenes. The three exons of the globin genes are shown in pale blue. (Lancet 2018; 391:155-167; Legend to slide 17) 44 Genetic basis of the phenotypic diversity of b-thal Primary and secondary modifiers of the b thalassemia phenotype include variable output from the b globin (b genotype), variable output from the globin genes ( genotype) and variable HbF response (co-inheritance of different QTLs (quantitative trait loci) controlling HbF and Fcell levels). The consequences of these factors is the degree of chain imbalance ( / nonglobin ratio) and severity of ineffective erythropoiesis. bsilent: have minimal effect on b globin production. bN: Normal. (Legend to slide 21) The primary cause lies in the -, b- and g-globin genes, as shown at the top of the figure, and they affect the magnitude of the excess of -chains. The secondary modifiers such as AHSP ( hemoglobin stabilizing protein; a chaperone that binds and stabilizes globin, thereby reducing 4 precipitation) are shown in the middle. HPFH: hereditary persistence of fetal hemoglobin. Tertiary modifiers are shown at the bottom of the figure: VDR, vitamin D receptor; ESR1, estrogen receptor; collagen, several genes determined in collagen synthesis; HFE, the locus for hereditary hemochromatosis; HAMP, hepcidin antimicrobial peptide (a peptide hormone that is the master regulator of iron homeostasis); UGT1, UGT glucuronyltransferase involved in bilirubin glucuronidation; HLA-DR, major histocompatibility complex locus; TNF, tumour-necrosis factor- ; ICAM1, intercellular adhesion molecule 1; GDF11, growth differentiation factor 11 (a member of transforming growth factor β superfamily); JAK2, Janus kinase 2 (disease gene of myeloproliferative disorders); TMPRSS6, transmembrane protease serine 6 (a metalloprotease governing hepcidin expression) (Legend to slide 23) From SNP to mechanism and potential therapy. Hemoglobin genes on human chromosome 11 are differentially expressed in the embryo, fetus, and adult. A SNP in the BCL11A gene is associated with varying amounts of fetal hemoglobin in human populations. Because there is an inverse correlation between BCL11A and fetal hemoglobin expression, inhibiting BCL11A is a potential therapy for adult hemoglobinopathies. LCR HSS: locus control region hypersensitive sites. The asterisk indicates a DNA region that, when deleted, is associated with increased fetal hemoglobin production. (Legend to slide 24) 45 Nonsense-mediated mRNA decay (NMD) Genes contain exons and introns. Genes are transcribed into a precursor mRNA, called pre-mRNA. Pre-mRNA is processed co- and post-transcriptionally in a series of temporally and mechanistically connected steps. One such step is 5′-end capping (m7Gppp). The presence of a 5′ cap enables the association of the cap binding protein (CBP) heterodimer. Another step is 3′-end polyadenylation. A third step is splicing, which results in intron removal and concomitant ligation of exons. Introns are recognized in part because they begin with a 5′-splice site and end with a 3′-splice site. Translation will terminate at the normal termination codon and the mRNA will not be targeted for NMD. However, if intron 1 contains a nonsense codon that resides in frame with the AUG initiation codon or if it lacks such a nonsense codon but is not a multiple of 3 nt and, thus, shifts the reading frame, then translation could terminate prematurely and elicit NMD. NMD involves three distinct processes. In the first, NMD substrates are detected by the NMD machinery. In the case of 3′ untranslated region (UTR) exon junction complex (EJC)-mediated NMD, if translation terminates, for example, at a premature termination codon (PTC), more than ∼50–55-nt upstream of an exon–exon junction (depicted as “^”), then termination is detected as aberrant. This is because a proteinaceous EJC, situated ∼20–24-nt upstream of the exon–exon junction, lies too far downstream from the PTC to be removed by the terminating ribosome. At the EJC, UPF2, anchored by UPF3X (also called UPF3B), interacts with UPF1 and SMG1 at the site of termination. Alternatively, on substrates with unusually long 3′UTRs, a large amount of UPF1 can promiscuously bind to the 3′UTR. The second phase of NMD is the commitment phase, where UPF1 is phosphorylated by its associated kinase, SMG1. This occurs efficiently during a series of regulated events on 3′UTR EJC-mediated NMD and less efficiently on 3′UTR EJC-independent NMD substrates. UPF1 phosphorylation represents a commitment to NMD. During the third phase of NMD, that is, mRNA degradation, phosphorylated UPF1 recruits RNA degradation activities either directly, by recruiting the SMG6 endonuclease (solid line with arrow to the scissors, which represent SMG6 itself) and/or the SMG5–SMG7 heterodimer, which recruits (dotted lines with arrow to the scissors) decapping and deadenylation enzymes (scissors) that produce unstable RNAs that are targeted for further degradation by exonucleases (red pacmen). CBP, cap-binding protein(s); 5′ dot, 7-methylguanine 5′ cap; AUG, translation initiation codon; AA(A)n, 3′ poly(A) tail; P, phosphate. (Legend to slide 28) 46 RNA splicing: b-globin as an example The β-globin gene contains three protein-coding exons (red) and two intervening noncoding introns (blue). The introns interrupt the protein-coding sequence between the codons for amino acids 31 and 32 and 105 and 106. Transcription of this and many other genes starts slightly upstream of the 5′ exon and extends downstream of the 3′ exon, resulting in noncoding regions (gray) at the ends of the primary transcript. These regions, referred to as untranslated regions (UTRs), are retained during processing. The 5′ 7methylguanylate cap (m7Gppp; green dot) is added during formation of the primary RNA transcript, which extends beyond the poly(A) site. After cleavage at the poly(A) site and addition of multiple A residues to the 3′ end, splicing removes the introns and joins the exons. The small numbers refer to positions in the 147-aa sequence of β-globin. (Legend to slide 30) Abnormal processing of the b-globin primary RNA transcript in humans with the disease b thalassemia. In the examples shown, the disease is caused by splice-site mutations, denoted by black arrowheads. The dark blue boxes represent the three normal exon sequences; the red lines are used to indicate the 5 and 3 splice sites that are used in splicing the RNA transcript. The light blue boxes depict new nucleotide sequences included in the final mRNA molecule as a result of the mutation. Note that when a mutation leaves a normal splice site without a partner, an exon is skipped or one or more abnormal "cryptic" splice sites nearby is used as the partner site, as in (C) and (D). (Adapted in part from S.H. Orkin, in G. Stamatoyannopoulos et al., eds, The Molecular Basis of Blood Diseases, pp. 106-126. Philadelphia: Saunders, 1987.) (Legend to slide 31) 47 New strategies in the treatment of thalassemias • Hematopoietic stem cell transplantation • Cellular and molecular modifiers (5-azacytidine, hydroxyurea, etc) • Antioxidants • CRISPR/Cas9 (correcting mutations by targeted genome editing) • Gene therapy (lentiviral vectors: treatment succeeds, with a caveat) (Science 326:1468-1469, 2009; Nature Medicine 21:221-230, 2015) (http://asheducationbook.hematologylibrary.org/cgi/content/full/2009/1/690) (http://asheducationbook.hematologylibrary.org/content/2010/1/445) If the incidence of b-thalassemia major is 0.01% in the local population, the carrier rate of b-thalassemia mutation is 2 0.01 0.99 = 0.0198 = 1.98% 2%. 48 Hematopoietic stem/progenitor cells(HSPC) gene therapy Hematopoietic stem/progenitor cell (HSPC) gene therapy. HSPCs are isolated from the bone marrow (or mobilized peripheral blood) of a patient with b-thalassemia. Following culture ex vivo in conditions that stimulate cell proliferation, the cells are exposed to a retroviral vector expressing a functional copy of the defective gene and then infused back into the patient after a few days. Infusion usually takes place following administration of a pharmacological conditioning regimen that eliminates the endogenous bone marrow progenitors and favours engraftment of the transplanted cells. The engrafted gene-corrected progenitor cells generate functional progeny that reconstitute all lineages and restore red blood cell functions to the patient. If the genecorrected cells have a selective growth advantage compared to the unmodified cells, full reconstitution of the red blood cell compartments is obtained even from a few engrafted transduced progenitor cells, as depicted in the figure, and this may occur even without conditioning. If the engrafted progenitor cells have self-renewal capacity, they ensure long-term correction of the disease. If the engrafted cells are multipotent stem cells, they generate gene-marked cells in all haematopoietic lineages. NK, natural killer cells. (Legend to slide 34) Advantages of HSPCs: 1) Capacity to self renew and maintain specific functions over an individual’s lifetime: HSPCs are defined by their ability to regenerate all blood lineages (multipotency). Transfer and expression of genes added to a small number of cells result in gene correction of much greater numbers of cells by self-renewal and differentiation. 2) Accessibility: can be obtained easily. 3) Ability to survive and be manipulated in ex vivo cell culture. 4) Transplantability: HSPC transplantation provides the best chance for a cure for many diseases. 49