")
SECTION 5
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
ASSESSMENT OF
AUTONOMIC FUNCTION
The autonomic nervous system controls many of our “automatic” functions, including heart rate
and blood pressure, sweating, urinary functions, and gastric motility. It regulates visceral functioning and the internal environment of the body through its effects on the heart, gut, and other
internal organs, peripheral blood vessels, and sweat glands (Chapter 35). Autonomic dysfunction
has important implications for health and disease, yet it is clinically under-recognized. Clinical
signs of autonomic dysfunction are easily overlooked, and neural activity in the autonomic nervous
system is difficult to record directly. Involvement of the autonomic nervous system may occur in
various neurological diseases involving the central nervous system (e.g., multiple system atrophy)
or peripheral nervous system (e.g., diabetic polyneuropathy). Assessment of autonomic function
depends primarily on measuring the response of the autonomic nervous system to external stimuli,
which can be accomplished with several neurophysiological tests.
The measurements of sweating (Chapters 36 and 38), cardiovascular activity and peripheral
blood flow (Chapters 37 and 39), and central autonomic-mediated reflexes provide insight into
the broad range of disorders that affect the central and peripheral components of the autonomic
nervous system—from the hypothalamus to the autonomic axons in the trunk and limbs. With better understanding of the clinical importance of measuring autonomic function and with increasing use of newly available tests of cardiovagal function, segmental sympathetic reflexes, postural
hemodynamics, and power spectral analysis, the tests and measurements of autonomic function
will continue to be of benefit in patient care.
Pain is mediated mainly through small nerve fibers, particularly in the autonomic nervous system. Measurements of their function can help elucidate the mechanisms underlying pain, especially
peripheral pain. The emerging modalities for assessment of pain pathways include quantitative
sensory tests, autonomic tests, microneurography, and laser-evoked potentials (Chapter 40).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Chapter 35
Autonomic Physiology
William P. Cheshire, Jr.
INTRODUCTION
MUSCLE SYMPATHETIC ACTIVITY
SYMPTOMS AND DISEASES
AUTONOMIC CONTROL
OF HEART RATE
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
GENERAL ORGANIZATION OF
THE AUTONOMIC SYSTEM
Visceral Afferents
Visceral Efferents
SYMPATHETIC FUNCTION
Functional Anatomy of the Sympathetic
Outflow
Assessment of Sympathetic Function
in Humans
CARDIOVASCULAR
REFLEXES
Arterial Baroreflexes
Cardiopulmonary Reflexes
Venoarteriolar Reflexes
Ergoreflexes
MAINTENANCE OF POSTURAL
NORMOTENSION
SYMPATHETIC INNERVATION
OF THE SKIN
SUMMARY
INTRODUCTION
various forms of stress the body experiences.
It consists of sympathetic (thoracolumbar) and
parasympathetic (craniosacral) divisions. Both
divisions contain general visceral afferent and
efferent fibers. The enteric nervous system,
located in the wall of the gut, is considered a
third division of the autonomic nervous system.
The autonomic nervous system thus regulates
and coordinates such physiological functions as
The autonomic nervous system is essential to
maintaining physiological homeostasis in health
and responding to illness. Its integrative functions coordinate input from peripheral and visceral afferent nerves to orchestrate a dynamic
balance among organ systems. Its adaptive
functions react moment by moment to the
617
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
618
Section 5: Assessment of Autonomic Function
blood pressure and heart rate, respiration, body
temperature, sweating, lacrimation, nasal secretion, pupillary size, gastrointestinal motility, urinary bladder contraction, sexual physiology, and
blood flow to the skin and many organs.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
SYMPTOMS AND DISEASES
Disorders affecting the autonomic nervous system may be manifested by failure or hyperactivity of one or many of the visceral effector organs.
Autonomic neuropathies that disconnect central autonomic centers and autonomic ganglia from their peripheral effectors may result
in deficits in autonomic function. Examples
include orthostatic hypotension due to adrenergic failure, heat intolerance due to sudomotor
failure, gastroparesis, colonic inertia, hypotonic
bladder, and male erectile failure. Some autonomic neuropathies result in localized deficits;
for example, Horner’s syndrome from oculosympathetic denervation, Adie’s tonic pupil
from oculoparasympathetic denervation, and
neurogenic bladder from sacral anterior horn
cell involvement in poliomyelitis. In other
cases, autonomic centers disconnected from
inhibitory influences may give rise to episodic
autonomic hyperfunction. Examples include
autonomic dysreflexia and hypertonic bladder
following spinal cord trauma, diencephalic syndrome following severe head injury, hypertensive surges in the baroreflex failure that follows
irradiation to the carotid sinuses, facial sweating
in auriculotemporal syndrome, and catecholamine storms in pheochromocytoma.
Autonomic disturbances frequently accompany neurological illnesses affecting motor or
sensory systems or may occur in isolation. The
presence of autonomic failure is sometimes
clinically obvious. More frequently, accurate
characterization, localization, and grading of
autonomic dysfunction require a careful history to elicit subtle symptoms, a neurological
examination attentive to autonomic signs, and
testing in a clinical autonomic laboratory.
The differential diagnosis of autonomic
failure includes the peripheral neuropathies
(many of which involve autonomic fibers), central degenerative disorders, and medical disorders that affect the autonomic nervous system.
Peripheral autonomic failure frequently occurs
in small-
fiber neuropathies, particularly in
diabetes mellitus and amyloidosis. Additionally,
prominent autonomic dysfunction can occur
in autoimmune diseases, such as autoimmune
autonomic ganglionopathy associated with
antibodies to the α-3 ganglionic acetylcholine
receptor, Guillain–
Barré syndrome, Sjögren’s
syndrome, Lambert–
Eaton myasthenic syndrome associated with antibodies to voltage-
gated calcium channels, and paraneoplastic
disorders such as lung carcinoma associated
with antineuronal nuclear antibody (ANNA-1
or anti-Hu). Autonomic disturbances are common also in botulism, diphtheritic neuropathy,
and Chagas disease. Central neurodegenerative disorders associated with autonomic failure include multiple system atrophy (MSA),
dementia with Lewy bodies, and Parkinson’s
disease. Isolated autonomic failure may occur
acutely or subacutely (e.g., in inflammatory or
paraneoplastic pandysautonomia), or as a slowly
progressive disease (pure autonomic failure).
The presence of autonomic failure has important implications for clinical management as well
as for prognosis. Disruption of autonomic function can influence the long-term risks of morbidity, mortality, and intraoperative mortality
(Sandroni et al. 1991; Vinik et al. 2003; Ewing,
Campbell, and Clarke 1980; Bellavere et al. 1984;
Chambers et al. 1990; Knuttgen, Weidemann,
and Doehn 1990; Burgos et al. 1989).
Autonomic testing is indicated in patients
(1) with any of the aforementioned symptoms
suggesting autonomic failure, (2) with peripheral neuropathies (particularly small-
fiber
neuropathies in which nerve conduction and
electromyographic findings may be normal),
or (3) with Parkinsonism or cerebellar dysfunction in which MSA is suspected. Unlike the
easily reproducible functions of somatic motor
or sensory nerves, autonomic nerve function
is difficult to evaluate precisely in humans. In
general, evaluation of autonomic function has
been restricted to noninvasive recordings of
heart rate, blood pressure, blood flow, or sweat
production. The interpretation of the results
of these tests may be difficult, because (1) the
effector organs react slowly to variations in neural input, (2) the interactions of sympathetic
and parasympathetic outputs at a single target
level are complex, and (3) autonomic responses
are affected by pharmacological, hormonal,
local chemical, and mechanical influences.
This chapter provides an overview of some
aspects of autonomic function that may help
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
35 Autonomic Physiology
with interpreting the results of noninvasive autonomic tests commonly used clinically. Therefore, the focus is on sudomotor,
cardiovascular, and adrenergic functions.
Gastrointestinal, bladder, and sexual functions
are not discussed.
Purpose and Role
of Autonomic Testing
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Autonomic testing serves several goals; among
them, to:
• Recognize the presence, distribution, and
severity of autonomic dysfunction
• Recognize patterns of autonomic failure that
can be related to specific syndromes; for
example:
• Generalized autonomic failure
• Orthostatic hypotension
• Orthostatic intolerance
• Reflex syncope
• Distal small-fiber neuropathy
• Peripheral neuropathies that may have an
autonomic component
• Neurodegenerative disorders that may
have an autonomic component
• Organ-specific autonomic syndromes such
as gastroparesis that may have a more
widespread autonomic component
• Recognize potentially treatable autonomic
disorders
• Recognize disorders that warrant further
evaluation
• Diagnose benign autonomic disorders that
may mimic life-threatening conditions
• Quantitatively evaluate autonomic dysfunction over time:
• To define the progression or remission of
autonomic disease
• To assess the response to therapy
GENERAL ORGANIZATION
OF THE AUTONOMIC SYSTEM
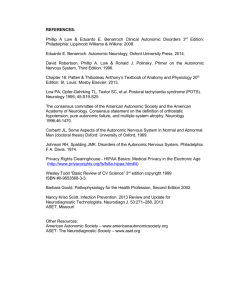
The general organization of the autonomic nervous system is composed of visceral afferent
and efferent nerves (Figure 35–1).
619
Visceral Afferents
Visceral receptors generally are slowly adapting mechanoreceptors or chemoreceptors
that have a low level of spontaneous activity
and are innervated by small myelinated and
unmyelinated fibers (Cervero and Foreman
1990). Visceral afferent signals may mediate
local reflexes in peripheral organs or provide
collateral input to autonomic ganglion cells.
Most visceral afferent fibers enter the central
nervous system at a spinal or, in the case of
cranial nerves (CN), the medullary level to
initiate segmental or suprasegmental viscerovisceral reflexes or to relay visceral information to higher centers (Cervero and Foreman
1990; Loewy 1990; Dampney 1994). Spinal
sympathetic afferents mediate visceral pain
and initiate segmental and suprasegmental
viscerovisceral reflexes. Visceral afferents
that enter at the medullary level are in the
vagus (CN X) and glossopharyngeal (CN IX)
nerves and synapse in the nucleus of the tractus solitarius (NTS) (Loewy 1990; Dampney
1994). This nucleus is critically involved
in respiratory and cardiovascular reflexes
through its extensive connections with neurons in the so-called intermediate reticular
zone of the medulla (Dampney 1994; Jänig
and Häbler 1999).
Visceral Efferents
Sympathetic and parasympathetic autonomic
outflow systems produce responses that are
longer in latency and duration and more continuous and generalized than those mediated
by the somatic motor system. This reflects
important differences in the functional organization of autonomic and somatic efferents.
Autonomic output involves a two-
neuron
pathway that has at least one synapse in an
autonomic ganglion (Jänig and Häbler 1999).
The preganglionic axons are small myelinated
(type B) cholinergic fibers that emerge from
neurons of the general visceral efferent column in the brain stem or spinal cord and pass
through peripheral nerves to the autonomic
ganglia (Gibbins 1990). Postganglionic autonomic neurons send varicose, unmyelinated
(type C) axons to innervate peripheral organs.
Autonomic terminals contain varicosities.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
620
Section 5: Assessment of Autonomic Function
Visceral
effectors
Cranial
preganglionic
parasympathetic
neurons
Parasympathetic
ganglion
ACh
NE
Sympathetic
ganglia
Preganglionic
sympathetic
neurons
(T1–L3)
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Sacral
preganglionic
parasympathetic
neurons
(S2–S4)
Parasympathetic
ganglion
Figure 35–1. Organization of the sympathetic and parasympathetic outputs of the autonomic nervous system. ACh, acetylcholine; NE, norepinephrine. Mayo Scientific Publications. Permission to reproduce Figure 9.3 from Benarroch EE,
Daube JR, Flemming KD, Westmoreland BF. Mayo Clinic Medical Neurosciences. 5th edition. Mayo Clinic Scientific
Press and Informa Healthcare; c2008.
At most sympathetic neuroeffector junctions, the primary postganglionic neurotransmitter is norepinephrine, which acts on the
various subtypes of α- and β-adrenergic receptors. In the sweat glands, sympathetic effects
are mediated principally by acetylcholine. The
primary postganglionic neurotransmitter at
all parasympathetic neuroeffector junctions is
acetylcholine, which acts on the various subtypes of muscarinic receptors. Whereas the
main consequences of denervation in the striated muscle are paralysis and atrophy, postganglionic efferent denervation produces an
exaggerated response of the target when it is
exposed to the neurotransmitter. This phenomenon, called denervation supersensitivity,
is evidence of a lesion involving postganglionic
neurons in which the remaining neuroeffector
receptors are upregulated.
Activity of most autonomic effectors is modulated by dual, continuous sympathetic, and
parasympathetic influences (Jänig and Häbler
1999; Gibbins 1990). Sympathetic control originates from preganglionic neurons in segments
T1–L3 of the spinal cord and predominates in
blood vessels, sweat glands, and cardiac muscle.
Parasympathetic outflow originates from preganglionic neurons in nuclei of CNs III, VII,
IX, and X and in segments S2–S4 of the spinal
cord. It predominates in control of the salivary
glands, sinoatrial node, gastrointestinal tract,
and bladder (Jänig and Häbler 1999; Gibbins
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
35 Autonomic Physiology
1990). Sympathetic–
parasympathetic interactions are not simply antagonistic but are functionally complementary. The sympathetic and
parasympathetic systems may interact at several levels, including that of the central nervous
system, autonomic ganglia, neuroeffector junction, and target organ (Cervero and Foreman
1990; Loewy 1990; Dampney 1994; Jänig and
Häbler 1999; Gibbins 1990).
SYMPATHETIC FUNCTION
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Functional Anatomy of the
Sympathetic Outflow
Preganglionic sympathetic neurons have a
slow, irregular, tonic activity that depends
mainly on multiple segmental afferent and
descending inputs (Cabot 1996; Jänig 1996).
Preganglionic sympathetic neurons are organized into specialized spinal sympathetic functional units that control specific target organs
and are differentially influenced by input from
the hypothalamus and brain stem. Sympathetic
functional units include skin vasomotor, muscle
vasomotor, visceromotor, pilomotor, and sudomotor units (Cabot 1996; Jänig 1996; Cheshire
2000b). There are, for example, clear differences between the patterns of sympathetic
outflow to skin and to muscle, but sympathetic
activity patterns recorded simultaneously from
different muscles at rest or from skin sympathetic nerves innervating the palms and the
feet are remarkably similar (Jänig 1996; Wallin
and Fagius 1988; Walling and Elam 1994).
Preganglionic sympathetic output has a segmental organization, but the segmental distribution of preganglionic fibers does not follow
the dermatomal pattern of somatic nerves
(Cabot 1996; Wallin and Fagius 1988). For
example, sudomotor functional units in segments T1 and T2 innervate the head and neck,
units in T3–T6 innervate the upper extremities
and thoracic viscera, those in T7–T11 innervate the abdominal viscera, and ones in T12–
L2 innervate the lower extremities and pelvic
and perineal organs (Wallin and Fagius 1988).
Preganglionic sympathetic axons exit through
ventral roots and pass through the white ramus
communicans of the corresponding spinal
nerve to reach the paravertebral sympathetic
chain and to synapse on neurons located in
621
the paravertebral or prevertebral ganglia.
Paravertebral ganglia innervate all tissues and
organs except those in the abdomen, pelvis,
and perineum.
Their postganglionic fibers destined for the
trunk and limbs follow the course of spinal
nerves or blood vessels or both. Spinal fibers
join the peripheral spinal (somatic) nerve
through the gray ramus communicans. These
fibers provide vasomotor, sudomotor, and
pilomotor input to the extremities and trunk.
Sympathetic fibers are intermingled with
somatic motor and sensory fibers, and their
distribution is similar to that of the corresponding somatic nerve. Most sympathetic fibers are
destined for the hand and foot and are carried
mainly by the median, peroneal, and tibial
nerves, and, to a lesser extent, the ulnar nerve.
SYMPATHETIC REFLEXES
Unlike somatic motor neurons, sympathetic
preganglionic neurons are not monosynaptically driven by visceral, muscle, or cutaneous
sensory input. These afferents converge on
second-order neurons located in laminae I, V,
VII, and X of the spinal cord that project to the
sympathetic preganglionic neurons to initiate
segmental somatosympathetic and viscerosympathetic reflexes (Cabot 1996). Segmental
reflex pathways arising from somatic or visceral
afferents activate ipsilateral local interneuronal networks in laminae I, V, and VII, which
may directly activate or inhibit the sympathetic
preganglionic neurons. With the exception of
Ia muscle spindle and Ib Golgi tendon organ
afferents, activation of all other groups of primary sensory fibers arising from skin (Aβ, Aδ
and C), muscle (groups II, III, and IV), and
viscera (groups Aδ and C) can modulate preganglionic neuron activity through segmental
pathways (Cabot 1996; Jänig 1996). Segmental
sympathetic reflexes are segmentally biased,
predominantly uncrossed, and exhibit ipsilateral, function-
specific, reciprocal, and non-
reciprocal patterns of response. For example,
nociceptive stimuli reflexively activate segmental circuitry that generates excitation of
vasoconstrictor outflow to skeletal muscle
and inhibition of vasoconstrictor outflow to
the skin (Jänig 1996). Unlike somatic reflexes
(e.g., the flexor reflex), segmental sympathetic
reflexes do not exhibit reciprocal contralateral
response patterns, but they may exhibit crossed,
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
622
Section 5: Assessment of Autonomic Function
non-reciprocal responses. For example, during
execution of the cold pressor test, decreases
in cutaneous blood flow in an arm exposed to
ice-cold water are accompanied by cutaneous
vasoconstriction in the contralateral forearm.
All segmental spinal reflexes are subject to
supraspinal modulation through several parallel pathways arising in the hypothalamus, pons,
and medulla and innervating the sympathetic
preganglionic neurons (Loewy 1990; Dampney
1994; Jänig and Häbler 1999).
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Assessment of Sympathetic Function
in Humans
Sympathetic function in humans can be
assessed, directly or indirectly, with various
noninvasive or invasive techniques. Indirect
methods include noninvasive tests of sudomotor and cardiovascular function described in
Chapters 36–39; measurement of plasma norepinephrine concentration in forearm veins
with the subject first supine and then standing;
assessment of splanchnic and cerebral blood
flow using Doppler techniques; and assessment of sympathetic innervation of the heart
using radioisotope methods (Garland et al.
2007; Thieben et al. 2007; Fujimura et al.
1997; Purewal et al. 1995; Zhang, Crandall, and
Levine 2004; Horowitz and Kaufmann 2001;
Yamashina and Yamazaki 2007; Goldstein
2004). In comparison, microneurographic
technique allows direct recording of postganglionic sympathetic nerve activity in humans
(Wallin and Fagius 1988; Wallin and Elam
1994). Nerve recordings are made with tungsten microelectrodes inserted percutaneously
into a nerve, especially the median, peroneal, or tibial nerves. This technique allows
multi-
unit recordings of two different types
of outflow: skin sympathetic nerve activity and
muscle sympathetic nerve activity (Wallin and
Fagius 1988; Wallin and Elam 1994).
SYMPATHETIC INNERVATION
OF THE SKIN
Sympathetic vasomotor, pilomotor, and sudomotor innervation of skin effectors has a primarily thermoregulatory function (Gibbins
1990; Johnson 1986; Cheshire and Low 2007).
Skin sympathetic activity is a mixture of sudomotor and vasoconstrictor impulses and may
sometimes include pilomotor and vasodilator
impulses. The average conduction velocity for
skin sudomotor and vasomotor fibers is 1.3 m/
second and 0.8 m/second, respectively (Wallin
and Fagius 1988; Wallin and Elam 1994).
The intensity of the skin sympathetic activity
is determined mainly by environmental temperature and the emotional state of the subject. Decreased or increased environmental
temperature can produce selective activation
of the vasoconstrictor or sudomotor system,
respectively, with suppression of activity in the
other system. Emotional stimuli or inspiratory
gasp also increases spontaneous skin sympathetic activity, but in this case the bursts are
caused by simultaneous activation of sudomotor and vasomotor impulses (Wallin and Fagius
1988; Wallin and Elam 1994). Cutaneous arteries and veins have a prominent noradrenergic
innervation that regulates both nutritive and
arteriovenous skin blood flow (Gibbins 1990;
Johnson 1986). Nutritive skin flow is carried
by capillaries and is regulated by sympathetic
(α- and β-adrenergic) and local nonadrenergic
mediators. Arteriovenous skin blood flow is
carried by low-resistance arteriovenous shunts,
which receive abundant sympathetic vasoconstrictor input and play a key role in thermoregulation (Gibbins 1990; Johnson 1986). Skin
vasoconstrictor neurons may coordinate their
activity with vasomotor neurons in other vascular beds to maintain cardiac output, but they
are not sensitive to baroreflex input.
Skin blood flow is also controlled by somatosympathetic reflexes and three local axon
reflexes: (1) the axon flare response, (2) the
sudomotor axon reflex, and (3) the venoarteriolar reflex (Cabot 1996; Jänig 1996). The
axon flare response is mediated by nociceptive C-fiber terminals (Low and Sletten 2008).
Activation by noxious chemical or mechanical
stimuli produces antidromic release of neuropeptides (substance P and others) that cause
skin vasodilatation directly and through stimulation of histamine release by mast cells. The
sudomotor axon reflex is mediated by sympathetic sudomotor C fibers. The venoarteriolar
reflex is mediated by sympathetic vasomotor
axons innervating small veins and arterioles.
Skin vasomotor activity has been studied
clinically by using several noninvasive methods for measuring skin blood flow, including
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
35 Autonomic Physiology
plethysmography and laser Doppler flowmetry
(Low and Sletten 2008).
The eccrine sweat glands in humans have a
major role in thermoregulation. The segmental
pattern of distribution of sudomotor fibers to
the trunk and limbs is irregular and varies substantially among individuals and even between
the right and the left sides of an individual
(Gibbins 1990). Sympathetic inputs to the
sweat glands are mediated by acetylcholine,
acting via M3 muscarinic receptors.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
MUSCLE SYMPATHETIC ACTIVITY
Muscle sympathetic activity is composed of
vasoconstrictor impulses that are strongly
modulated by arterial baroreceptors (Jänig
1996; Wallin and Fagius 1988; Wallin and
Elam 1994). Conduction velocity of the postganglionic C fibers has been estimated to be
0.7 m/second in the median nerve and 1.1
m/second in the peroneal nerve (Wallin and
Fagius 1988). At rest, there is a striking similarity between muscle sympathetic activity
recorded in different extremities. However,
this activity in the arm and leg can be dissociated during mental stress and during forearm ischemia after isometric exercise (Wallin,
Victor, and Mark 1989). Muscle sympathetic
activity is important for buffering acute
changes of blood pressure and decreases in
response to moment-to-moment baroreceptor
influence (Wallin and Fagius 1988; Wallin and
Elam 1994; Somers et al. 1993). It has much
less importance, however, for long-term control of blood pressure (Wallin and Elam 1994).
At rest, muscle sympathetic activity correlates
positively with antecubital venous plasma
norepinephrine levels (Eckberg, Nerhed, and
Wallin 1985). Muscle sympathetic activity is
also inhibited by cardiopulmonary receptors.
The respiratory cycle, changes of posture,
or the Valsalva maneuver may modulate the
muscle sympathetic activity caused by changes
in arterial pressure. However, hypercapnia, hypoxia, isometric hand-grip, emotional
stress, or the cold pressor test increase muscle sympathetic activity despite unchanged
or increased arterial pressure (Wallin and
Fagius 1988; Wallin and Elam 1994; Eckberg,
Nerhed, and Wallin 1985).
623
AUTONOMIC CONTROL
OF HEART RATE
Heart rate depends on the effects of parasympathetic and sympathetic modulation
of the intrinsic firing rate of the sinus node.
Parasympathetic control is provided by cardiovagal neurons in the nucleus ambiguus
and dorsal motor nucleus in the medulla
(Gibbins 1990; Spyer, Brooks, and Izzo 1994).
Sympathetic noradrenergic control derives
mainly from the cervical and upper thoracic
ganglia (Gibbins 1990). In humans at rest,
parasympathetic tone predominates over the
excitatory sympathetic β-adrenergic influence.
Effects mediated by the vagus nerve have a
shorter latency and duration than those mediated by the sympathetic nerves. Heart rate has
spontaneous fluctuations, which reflect changing levels of autonomic activity modulating
sinus node discharge (van Ravenswaaij-
Arts
et al. 1993).
Use of power spectral analysis of heart rate
fluctuations allows a noninvasive quantitative assessment of beat-to-beat modulation of
neuronal activity affecting the heart (Baillard
et al. 2001; Bernardi et al. 2001; Mancia et al.
1985). Fluctuations of heart rate at respiratory
frequencies (approximately 0.15 Hz) are mediated almost exclusively by the vagus nerve (van
Ravenswaaij-
Arts et al. 1993; Baillard et al.
2001; Bernardi et al. 2001). Vagal influences on
the heart are associated directly with respiratory activity and are minimal during inspiration
and maximal at the end of inspiration and in
early expiration. This is the basis of the respiratory sinus arrhythmia (Low and Sletten 2008;
van Ravenswaaij-Arts et al. 1993; Baillard et al.
2001). Spontaneous and baroreflex-
induced
firing of central cardiovagal neurons is inhibited during inspiration and is maximal during
early expiration (Eckberg, Nerhed, and Wallin
1985). Increased tidal volume increases respiratory sinus arrhythmia, whereas increased
respiratory frequency decreases it. Heart rate
variability is correlated inversely with age in
normal subjects at rest (Low and Sletten 2008).
Spontaneous lower frequency fluctuations
(those less than 0.15 Hz) of heart rate are
mediated by both the vagus and the sympathetic nerves and may be related to baroreflex activity, temperature regulation, and
other factors. Upright posture in humans
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
624
Section 5: Assessment of Autonomic Function
dramatically increases sympathetic nerve
activity and produces a large increase in low-
frequency heart rate power (van Ravenswaaij-
Arts et al. 1993; Baillard et al. 2001; Bernardi
et al. 2001).
CARDIOVASCULAR REFLEXES
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Arterial Baroreflexes
In normal subjects, control of arterial pressure depends primarily on the sympathetic
innervation of the blood vessels, particularly
in the splanchnic bed (Mancia et al. 1985;
Abboud 1986; Cowley 1992; Dampney 2008;
Wieling and Wesseling 1993). The number of
splanchnic sympathetic preganglionic neurons progressively decreases with age, and
orthostatic hypotension occurs after more
than 50% of them have been lost (Low and
Sletten 2008). Changes in sympathetic outflow are regulated by arterial baroreceptors
and chemoreceptors, cardiopulmonary receptors, and receptors in skeletal muscles (i.e.,
ergoreceptors) (Mancia et al. 1985; Abboud
1986; Cowley 1992; Dampney 2008; Wieling
and Wesseling 1993; Iellamo 2001). In addition, these reflexes are modulated by central
commands, particularly from the amygdala,
hypothalamus, and periaqueductal gray
(Loewy 1990; Dampney 1994; Green et al.
2007). In humans, arterial pressure is regulated primarily by the carotid sinus and aortic
baroreceptors, innervated by branches of CNs
IX and X, respectively, and by cardiopulmonary mechanoreceptors, innervated by vagal
and sympathetic afferents. The primary role
of arterial baroreflexes is the rapid adjustment of arterial pressure around the existing
mean arterial pressure (Mancia et al. 1985;
Abboud 1986; Cowley 1992; Dampney 2008;
Wieling and Wesseling 1993). The baroreceptor reflexes provide a negative feedback that
buffers the magnitude of arterial pressure
oscillations throughout the day.
Baroreflexes induce short-term changes in
heart rate opposite in direction to the changes
in arterial pressure, thus increasing heart rate
variability. The carotid baroreflex has been
studied by applying negative and positive pressures to the neck, which increase and decrease,
respectively, carotid sinus transmural pressure
(Eckberg and Fritsch 1993). The combined
influence of carotid and aortic baroreceptors
in the control of heart rate has been studied
by measuring heart rate responses to changes
in arterial pressure induced by intravenous
infusion of vasoconstrictor or vasodilator
agents (Eckberg and Fritsch 1993). Despite
their major influence on heart rate, the buffering effects of the carotid baroreflex depend
predominantly on changes in total peripheral
resistance (Mancia et al. 1985; Abboud 1986;
Cowley 1992; Dampney 2008; Wieling and
Wesseling 1993).
Baroreflex control of regional circulation is
heterogeneous and largely affects resistance
vessels in the splanchnic area (Mancia et al.
1985; Abboud 1986; Cowley 1992; Dampney
2008; Wieling and Wesseling 1993; Iellamo
2001). Sympathetic vasoconstriction in the
skeletal muscle is also strongly modulated
by the baroreflex; this control is dynamic
and more suitable for buffering short-
term
than long-term variations of arterial pressure
(Walling and Fagius 1988; Wallin and Elam
1994; Abboud 1986; Cowley 1992). During
orthostatic stress, baroreflex control over skeletal muscle sympathetic activity declines prior
to orthostatic syncope (Ichinose et al. 2006).
During exercise, carotid baroreceptor activity is rapidly adjusted to a higher level; this
allows increased arterial pressure to meet the
metabolic demands of the contracting muscles
(Mancia et al. 1985).
Cardiopulmonary Reflexes
Cardiopulmonary receptors are innervated by
vagal and sympathetic myelinated and unmyelinated afferent fibers. Atrial receptors innervated by vagal myelinated fibers are activated
by atrial distention or contraction and initiate
reflex tachycardia caused by selective increase
of sympathetic outflow to the sinus node.
Cardiopulmonary receptors with unmyelinated
vagal afferents, like arterial baroreceptors, tonically inhibit vasomotor activity. Unlike atrial
baroreceptors, cardiopulmonary receptors
provide sustained rather than phasic control in
sympathetic activity and vasomotor tone in the
muscle and have no major effect in controlling
heart rate (Mancia et al. 1985; Abboud 1986;
Cowley 1992; Dampney 2008; Wieling and
Wesseling 1993).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
35 Autonomic Physiology
Venoarteriolar Reflexes
The venoarteriolar reflex is a sympathetic
postganglionic C-fiber axon reflex, with receptors in small veins and effectors in muscle
arterioles. Venous pooling activates receptors
in small veins of the skin, muscle, and adipose tissue; the result is vasoconstriction in
the arterioles supplying these tissues. During
limb dependency, this local reflex vasoconstriction may decrease blood flow by 50%. The
main function of this reflex is to increase total
peripheral resistance (Low and Sletten 2008).
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Ergoreflexes
Static muscle contraction increases heart rate
and blood pressure. The mechanisms underlying these responses involve: (1) an exercise
pressor reflex initiated by the activation of chemosensitive endings of small myelinated and
unmyelinated afferent fibers by local metabolites in the contracting muscle and mediated
by group III and IV skeletal muscle afferent
fibers, (2) a pressor reflex initiated by muscle
mechanosensitive receptors, and (3) a central
command that influences descending autonomic pathways (Green et al. 2007; Leshnower
et al. 2001; Nakamoto and Matsukawa 2007).
Cardiovascular responses to moderately intense
static contraction may be produced primarily by
the motor command, which is solely responsible for increased heart rate. At higher intensity,
responses depend on both the motor command
and the muscle chemoreflexes (Mancia et al.
1985; Abboud 1986; Cowley 1992; Dampney
2008; Wieling and Wesseling 1993).
MAINTENANCE OF POSTURAL
NORMOTENSION
In healthy subjects, orthostatic stress such as
active standing, head-up tilt, or application of
lower-body negative pressure results in pooling of venous blood in the capacitance vessels
of the legs and abdomen. The bulk of venous
pooling occurs within the first 10 seconds. In
addition, central blood volume decreases following transcapillary filtration of fluid into the
interstitial space in the dependent tissues (Smit
et al. 1999). These combined effects lead to a
625
decrease in venous return to the heart, end-
diastolic filling of the right ventricle, and stroke
volume, resulting in approximately a 20%
decrease in cardiac output.
The adaptation to orthostatic stress consists
of several mechanisms. The decrease in mean
arterial pressure is prevented by a compensatory vasoconstriction of the resistance and
capacitance vessels of the splanchnic, renal, and
muscle vascular beds. The initial adjustments
to orthostatic stress are mediated by baroreflexes and cardiopulmonary reflexes. During
prolonged orthostatic stress, additional adjustments are mediated by humoral mechanisms,
including the arginine-vasopressin and renin-
angiotensin-aldosterone systems (Cowley 1992;
Smit et al. 1999). Carotid sinus baroreceptors
are of primary importance during standing,
whereas cardiopulmonary receptors have a
small role. When venous filling in the dependent parts increases intravenous pressure to
25 mm Hg, it activates a local axon reflex, called
the venoarteriolar reflex, which further contributes to adaptation to orthostatic stress.
Patients with autonomic failure have disturbed neural reflex arterial vasoconstriction, and this is the primary mechanism of
orthostatic hypotension. The inability to
increase vascular resistance allows considerable venous pooling to occur in the skeletal
muscle, cutaneous, and splanchnic vascular
beds of the dependent parts. The abdominal compartment (splanchnic circulation)
and perhaps skin vasculature are the most
likely sites of venous pooling. The counter-
regulatory mechanism that reduces pooling
in the lower extremities is activation of the
skeletal muscle pump. Active muscle contraction increases intramuscular pressure, which
opposes the hydrostatic forces and reduces
venous pooling in the legs. This may explain
why some patients with orthostatic hypotension habitually fidget and contract their leg
muscles when upright (Cheshire 2000a). Such
physical countermaneuvers may be taught to
patients to help them compensate for orthostatic hypotension (Bouvette et al. 1996).
SUMMARY
The autonomic nervous system consists of three
divisions: the sympathetic (thoracolumbar),
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
626
Section 5: Assessment of Autonomic Function
parasympathetic (craniosacral), and enteric
nervous systems. The sympathetic and parasympathetic autonomic outflows involve a
two-
neuron pathway with a synapse in an
autonomic ganglion. Preganglionic sympathetic neurons are organized into various functional units that control specific targets and
include skin vasomotor, muscle vasomotor,
visceromotor, pilomotor, and sudomotor units.
Microneurographic techniques allow recording
of postganglionic sympathetic nerve activity in
humans. Skin sympathetic activity is a mixture
of sudomotor and vasoconstrictor impulses and
is regulated mainly by environmental temperature and emotional influences. Muscle sympathetic activity is composed of vasoconstrictor
impulses that are strongly modulated by arterial baroreceptors. Heart rate is controlled
by vagal parasympathetic and thoracic sympathetic inputs. Vagal influence on the heart
rate is strongly modulated by respiration; it is
more marked during expiration and is absent
during inspiration. This is the basis for the so-
called respiratory sinus arrhythmia, which is
an important index of vagal innervation of the
heart. Power spectral analysis of heart rate
fluctuations allows noninvasive assessment of
beat-
to-
beat modulation of neuronal activity
affecting the heart. Arterial baroreflex, cardiopulmonary reflexes, venoarteriolar reflex, and
ergoreflexes control sympathetic and parasympathetic influences on cardiovascular effectors. The main regulatory mechanism that
prevents orthostatic hypotension is reflex arterial vasoconstriction in the splanchnic, renal,
and muscular beds triggered by a decrease in
transmural pressure at the level of carotid sinus
baroreceptors.
REFERENCES
Abboud, F. M. 1986. “Interaction of cardiovascular reflexes
in humans.” In Neural mechanisms and cardiovascular
disease, eds. B. Lown, A. Malliani, and M. Prosdocimi,
73–84. Padova, Italy: Liviana Press.
Baillard, C., P. Goncalves, L. Mangin, B. Swynghedauw,
and P. Mansier. 2001. “Use of time frequency analysis to follow transitory modulation of the cardiac
autonomic system in clinical studies.” Autonomic
Neuroscience 90:24–28.
Bellavere, F., M. Ferri, C. Cardone, et al. 1984. “Analysis
of QT versus RR ECG interval variations in diabetic
patients shows a longer QT period in subjects with
autonomic neuropathy.” Diabetologia 27:255A.
Bernardi, L., C. Porta, A. Gabutti, L. Spicuzza, and P.
Sleight. 2001. “Modulatory effects of respiration.”
Autonomic Neuroscience 90:47–56.
Bouvette, C. M., B. R. McPhee, T. L. Opfer-Gehrking,
and P. A. Low. 1996. “Role of physical countermaneuvers in the management of orthostatic hypotension: Efficacy and biofeedback augmentation.” Mayo
Clinic Proceedings 71:847–53.
Burgos, L. G., T. J. Ebert, C. Asiddao, et al. 1989. “Increased
intraoperative cardiovascular morbidity in diabetics with
autonomic neuropathy.” Anesthesiology 70:591–97.
Cabot, J. B. 1996. “Some principles of the spinal organization of the sympathetic preganglionic outflow.”
Progress in Brain Research 107:29–42.
Cervero, F., and R. D. Foreman. 1990. “Sensory innervation of the viscera.” In Central regulation of autonomic
functions, eds. A. D. Loewy and K. M. Spyer, 104–25.
New York: Oxford University Press.
Chambers, J. B., M. J. Sampson, D. C. Sprigings,
G. Jackson. 1990. “QT prolongation on the electrocardiogram in diabetic autonomic neuropathy.” Diabetic
Medicine 7:105–10.
Cheshire, W. P. 2000a. “Hypotensive akathisia: Autonomic
failure associated with leg fidgeting while sitting.”
Neurology 55:1923–26.
Cheshire, W. P. 2000b. “Peripheral autonomic function
and dysfunction.” In The autonomic nervous system,
O. Appenzeller, section editor, Handbook of clinical
neurology, eds. P. J. Vinken, and G. W. Bruyn, Vol. 75,
105–42. Amsterdam: Elsevier.
Cheshire, W. P., and P. A. Low. 2007. “Disorders of sweating and thermoregulation.” Continuum: Lifelong
Learning in Neurology 13(6):143–64.
Cowley, A. W., Jr. 1992. “Long-term control of arterial
blood pressure.” Physiological Reviews 72:231–300.
Dampney, R. A. 1994. “Functional organization of central pathways regulating the cardiovascular system.”
Physiological Reviews 74:323–64.
Dampney, R. A. L. 2008. “Cardiovascular and respiratory
reflexes: Physiology and pharmacology.” In Clinical
autonomic disorders: Evaluation and management,
eds. P. A. Low and E. E. Benarroch, 3rd ed., 43–56.
Philadelphia: Wolters Kluwer–Lippincott Williams &
Wilkins Publishers.
Eckberg, D. L., and J. M. Fritsch. 1993. “How should
human baroreflexes be tested?” News in Physiological
Sciences 8:7–12.
Eckberg, D. L., C. Nerhed, and B. G. Wallin. 1985.
“Respiratory modulation of muscle sympathetic
and vagal cardiac outflow in man.” The Journal of
Physiology (London) 365:181–96.
Ewing, D. J., I. W. Campbell, and B. F. Clarke. 1980.
“Assessment of cardiovascular effects in diabetic
autonomic neuropathy and prognostic implications.”
Annals of Internal Medicine 92:308–11.
Fujimura, J., M. Camilleri, P. A. Low, et al. 1997. “Effect of
perturbations and a meal on superior mesenteric artery
flow in patients with orthostatic hypotension.” Journal
of the Autonomic Nervous System 67(1–2):15–23.
Garland, E. M., S. R. Raj, B. K. Black, et al. 2007. “The
hemodynamic and neurohumoral phenotype of postural tachycardia syndrome.” Neurology 69(8):790–98.
Gibbins, I. 1990. “Peripheral autonomic nervous system.”
In The human nervous system, ed. G. Paxinos, 93–123.
San Diego: Academic Press.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
35 Autonomic Physiology
Goldstein, D. S. 2004. “Functional neuroimaging of
sympathetic innervation of the heart.” Annals of the
New York Academy of Sciences 1018:231–43.
Green, A. L., S. Wang, S. Purvis, et al. 2007. “Identifying
cardiorespiratory neurocircuitry involved in central
command during exercise in humans.” The Journal of
Physiology 578:605–12.
Horowitz, D. R., and H. Kaufmann. 2001. “Autoregulatory
cerebral vasodilation occurs during orthostatic hypotension in patients with primary autonomic failure.”
Clinical Autonomic Research 11(6): 363–67.
Ichinose, M., M. Saito, N. Fujii, et al. 2006. “Modulation
of the control of muscle sympathetic nerve activity during severe orthostatic stress.” The Journal of
Physiology 576:947–58.
Iellamo, F. 2001. “Neural mechanisms of cardiovascular
regulation during exercise.” Autonomic Neuroscience
90:66–75.
Jänig, W. 1996. “Spinal cord reflex organization of sympathetic systems.” Progress in Brain Research 107:43–77.
Jänig, W., and H.-J. Häbler. 1999. “Organization of the
autonomic nervous system: Structure and function.”
In Handbook of clinical neurology, Vol. 74; series
30: The autonomic nervous system. Part I. Normal
functions, eds. P. J. Vinken and G. W. Bruyn, 1–52.
Amsterdam: Elsevier Science Publishers.
Johnson, J. M. 1986. “Nonthermoregulatory control of
human skin blood flow.” Journal of Applied Physiology
61:1613–22.
Knuttgen, D., D. Weidemann, M. Doehn. 1990. “Diabetic
autonomic neuropathy: Abnormal cardiovascular reactions under general anesthesia.” Klinische Wochen-
schrift 68:1168–72.
Leshnower, B. G., J. T. Potts, M. G. Garry, and J.
H. Mitchell. 2001. “Reflex cardiovascular responses
evoked by selective activation of skeletal muscle ergoreceptors.” Journal of Applied Physiology 90:308–16.
Loewy, A. D. 1990. “Anatomy of the autonomic nervous
system: An overview.” In Central regulation of autonomic functions, eds. A. D. Loewy and K. M. Spyer,
3–16. New York: Oxford University Press.
Low, P. A., and D. M. Sletten. 2008. “Laboratory evaluation
of autonomic failure.” In Clinical autonomic disorders:
evaluation and management, eds. P. A. Low and E.
E. Benarroch, 3rd ed., 130–63. Philadelphia: Wolters
Kluwer–Lippincott Williams & Wilkins Publishers.
Mancia, G., G. Grassi, A. Ferrari, and A. Zanchetti.
1985. “Reflex cardiovascular regulation in humans.”
Journal of Cardiovascular Pharmacology 7(Suppl
3):S152–59.
Nakamoto, T., and K. Matsukawa. 2007. “Muscle mechanosensitive receptors close to the myotendinous junction of the Achilles tendon elicit a pressor reflex.”
Journal of Applied Physiology 102:2112–20.
627
Purewal, T. S., D. E. Goss, M. M. Zanone, et al. 1995.
“The splanchnic circulation and postural hypotension
in diabetic autonomic neuropathy.” Diabetic Medicine
12(6):513–22.
Sandroni, P., J. E. Ahlskog, R. D. Fealey, and P. A. Low.
1991. “Autonomic involvement in extrapyramidal and
cerebellar disorders.” Clinical Autonomic Research
1:147–55.
Smit, A. A., J. R. Halliwill, P. A. Low, and W. Wieling. 1999.
“Pathophysiological basis of orthostatic hypotension in autonomic failure.” The Journal of Physiology
(London) 519:1–10.
Somers, V. K., M. E. Dyken, A. L. Mark, and F. M. Abboud.
1993. “Sympathetic-nerve activity during sleep in normal subjects.” The New England Journal of Medicine
328:303–7.
Spyer, K. M., P. A. Brooks, and P. N. Izzo. 1994. “Vagal
preganglionic neurons supplying the heart.” In Vagal
control of the heart: Experimental basis and clinical
implications, eds. M. N. Levy and P. J. Schwartz, 45–
64. New York: Futura Publishing Company.
Thieben, M. J., P. Sandroni, D. M. Sletten, et al. 2007.
“Postural orthostatic tachycardia syndrome: The
Mayo Clinic experience.” Mayo Clinic Proceedings
82(3):308–13.
van Ravenswaaij-Arts, C. M., L. A. Kollee, J. C. Hopman,
G. B. Stoelinga, and H. P. van Geijn. 1993. “Heart
rate variability.” Annals of Internal Medicine
118:436–47.
Vinik, A. I., R. A. Maser, B. D. Mitchell, and R. Freeman.
2003. “Diabetic autonomic neuropathy.” Diabetes
Care 26:1553–79.
Wallin, B. G., and J. Fagius. 1988. “Peripheral sympathetic
neural activity in conscious humans.” Annual Review
of Physiology 50:565–76.
Wallin, B. G., and M. Elam. 1994. “Insights from intraneural recordings of sympathetic nerve traffic in humans.”
News in Physiological Sciences 9:203–7.
Wallin, B. G., R. G. Victor, and A. L. Mark. 1989.
“Sympathetic outflow to resting muscles during static
handgrip and postcontraction muscle ischemia.” The
American Journal of Physiology 256:H105–10.
Wieling, W., and K. H. Wesseling. 1993. “Importance
of reflexes in circulatory adjustments to postural
change.” In Cardiovascular reflex control in health
and disease, ed. R. Hainsworth, 35–65. London: WB
Saunders.
Yamashina, S., and J. Yamazaki. 2007. “Neuronal imaging
using SPECT.” European Journal of Nuclear Medicine
and Molecular Imaging 34(6):939–50.
Zhang, R., C. G. Crandall, and B. D. Levine. 2004.
“Cerebral hemodynamics during the Valsalva maneuver: Insights from ganglionic blockade.” Stroke
35(4):843–47.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Chapter 36
Quantitative Sudomotor Axon Reflex
and Related Tests
Phillip A. Low
INTRODUCTION
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
LABORATORY EVALUATION
OF AUTONOMIC FUNCTION
QUANTITATIVE SUDOMOTOR AXON
REFLEX TEST
Physiology and Technique of QSART
Normal Pattern
Abnormal Patterns
Significance of the Test
INTRODUCTION
Typically, the distal ends of the longest nerve
fibers are first affected in the axonal neuropathies. Small nerve fibers are often selectively
involved and these are termed distal small-
fiber neuropathy (DSFN). One method of
recording C-
fiber function is to study the
function of the postganglionic sympathetic
sudomotor “C”-
fiber function (Low et al.
1983; Stewart, Low, and Fealey 1992; Low
1993a; Low et al. 2006). We describe below
Applications
Limitations and Pitfalls of QSART
OTHER METHODS OF SWEAT
MEASUREMENT
Silicone Imprints
QDIRT
Neuropad
SUMMARY
the use of methods to measure sudomotor
fiber function.
LABORATORY EVALUATION
OF AUTONOMIC FUNCTION
A detailed evaluation of autonomic function
currently comprises an evaluation of sudomotor, adrenergic, and cardiovagal function.
The standard autonomic reflex screen noninvasively and quantitatively evaluates each of
628
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
36
Quantitative Sudomotor Axon Reflex and Related Tests
629
Table 36–1 Routine Tests of Autonomic Function
The autonomic reflex screen comprises:
1. QSART distribution (4 sites)
2. Tests of cardiovagal function
a. Heart rate response to deep breathing
b. Valsalva ratio
3. Tests of adrenergic function
a. Blood pressure and heart rate response to head-up tilt
b. Beat-to-beat blood pressure response to Valsalva maneuver and deep breathing
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
QSART, Quantitative sudomotor axon reflex test.
these functions (Low 1993a; Low et al. 2006)
(Table 36–1). The quantitative sudomotor axon
reflex test (QSART) is a component of the
autonomic reflex screen that assesses sudomotor function and is discussed in this chapter.
Testing of adrenergic and cardiovagal functions
is considered in Chapters 37 and 39. Because
autonomic tests are affected substantially by
many confounding variables, standardization,
the recognition of pitfalls, and patient preparation (Table 36–2) are critically important (Low
1993a; Low 1993b; Low 1993c; Low 1993d).
The indications for autonomic testing are
summarized in Table 36–3. The presence of
generalized autonomic failure, a major medical problem, adversely affects prognosis. It is
important to quantify the deficits by system
and by autonomic level. Certain benign disorders, such as chronic idiopathic anhidrosis
and benign syncopes, need to be differentiated
from the more serious dysautonomias. Distal
small-
fiber neuropathy is diagnosable with
autonomic studies, and QSART is abnormal in
80% of cases, suggesting that most patients who
have distal somatic C-fiber involvement also
have autonomic C-fiber impairment (Stewart,
Low, and Fealey 1992; Low et al. 2006; Low
et al. 1985; Tobin, Giuliani, and Lacomis 1999).
This relationship is not invariable, and some
patients with distal small-fiber neuropathy and
abnormal epidermal skin fibers will have a normal QSART (Periquet et al. 1999).
QUANTITATIVE SUDOMOTOR
AXON REFLEX TEST
Many tests of sudomotor function of historical but limited clinical and research interest
exist. For modern clinical neurophysiology
laboratories, only the thermoregulatory sweat
test, QSART, peripheral autonomic surface
potential, sweat imprint test (SIT), QDIRT,
and Neuropad require consideration. The
thermoregulatory sweat test is described in
Chapter 38. QSART and the other sudomotor
tests are described in this chapter.
Physiology and Technique of QSART
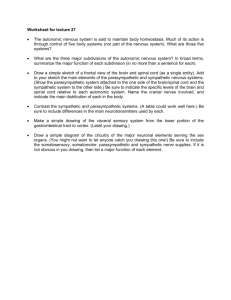
The neural pathway evaluated by QSART
consists of an axon reflex mediated by the
postganglionic sympathetic sudomotor axon
(Figure 36–1). The axon terminal is activated
Table 36–2 Patient Preparation for QSART
No food for 3 hours before testing. The antecedent meal should be a light breakfast or lunch without coffee
or tea.
Treatment with agents that inhibit sweating should be stopped 48 hours (preferably 5 half-lives of the drug
before the study). These include the following classes (with representative examples): anticholinergic
(glycopyrrolate, atropine), anticonvulsant (topiramate, zonisamide), antihistamine (diphenhydramine,
promethazine), antihypertensive (clonidine), antipsychotic/antiemetic (chlorpromazine, clozapine),
antivertigo (scopolamine), bladder antispasmodic (oxybutynin), opioids (fentanyl, hydrocodone), tricyclic
antidepressants (amitriptyline, nortriptyline).
The patient should be comfortable and discomfort-free (e.g., bladder recently emptied).
The room and personnel should be warm and quiet.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Table 36–3 Indications for Autonomic Laboratory Evaluation
Strong indications:
1. Suspicion of generalized autonomic failure
2. Diagnosis of benign autonomic disorders that mimic more serious dysautonomia
3. Detection of distal small-fiber neuropathy
4. Diagnosis of autonomic involvement in peripheral neuropathy
5. Orthostatic intolerance, such as the postural tachycardia syndrome
Desirable indications:
1. Monitoring course of autonomic failure
2. Evaluation of response to therapy
3. Peripheral neuropathies
4. Syncope
5. Amyotrophic lateral sclerosis
6. Extrapyramidal and cerebellar degenerations
7. Research questions
Sweat
gland
D
Sweat
gland
A
ON
OFF
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
C
B
5 min
Figure 36–1. Iontophoresis of acetylcholine activates sweat gland (direct response) and nerve terminal (C), resulting in
retrograde transmission to a branch point followed by orthograde transmission (an axon reflex, shown as arrow) in turn
activating a different population of sweat glands (A). An air gap (B) separates compartments A and C. This is the indirect or
axon-reflex mediated sweat response. The latter is shown on the right (D). Bottom right is a photograph of an actual capsule
with attachments.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
36
Quantitative Sudomotor Axon Reflex and Related Tests
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
by iontophoresed acetylcholine. Iontophoresis
is relatively painless, but is slow and takes minutes to occur. Alternatively, the C-fiber can be
directly stimulated electrically, but is very painful (Namer et al. 2004). The impulse first travels antidromically to a branch point, and then
orthodromically to release acetylcholine from
the nerve terminal. Acetylcholine traverses
the neuroglandular junction and binds to muscarinic receptors on eccrine sweat glands to
evoke the sweat response.
Equipment needed to perform QSART (or
QSWEAT) includes the sudorometer, a multicompartmental sweat cell, a constant current
generator, and some method of displaying
the sweat response. The commercial unit
(QSWEAT, sold by WR Medial, Minnesota),
although built very similarly to the Mayo unit,
for currently inexplicable reasons generates a
response that appears to be approximately 50%
of the volume of the Mayo unit.
The multicompartmental sweat cell
(Figure 36–
2) is attached to the skin and
permits iontophoresis of acetylcholine
through the stimulus compartment (C) and
a constant-
current generator. Axon-
reflex-
mediated sweat response is recorded from
compartment A. QSART responses are
recorded from standard sites, which include
the distal forearm, proximal leg, distal leg,
and proximal foot.
631
Normal Pattern
The QSART responses are sensitive and reproducible in control subjects and in patients with
neuropathy. The coefficient of variation (for the
Mayo unit) was checked in two ways. In a group
of individuals checked on two occasions, the
value was 14.7%. For three subjects (with low,
moderate, and high sweat volumes recorded
on multiple occasions), the mean coefficient of
variation was 8% (Low et al. 1983).
Extensive control data are available from
QSART responses in 139 normal subjects (74
females and 65 males) between 10 and 83 years
old. Mean sweat output was 3.01 µL/cm2 and 1.15
µL/cm2 for the forearms of males and females,
respectively. This difference was significant (p
< 0.001). Values for the foot were 2.65 µL/cm2
and 1.15 µL/cm2 for males and females, respectively. Again, the difference was statistically significant (p < 0.001). Thus, the two groups were
considered separately. For the forearm, QSART
response did not regress with age. For the foot,
however, there was a consistent, negative slope
of QSART responses with increasing age.
Abnormal Patterns
Several abnormal QSART patterns are rec­
ognized. The most reliable pattern is a
C
B
Male 43 yrs
Left forearm
Ouput = 3.81 µL
A
off
on
D
5 minutes
Figure 36–2. Quantitative sudomotor axon reflex test. Left, sweat cell, and right, response. The sweat response in compartment A is evoked in response to iontophoresis of acetylcholine in compartment C. Compartment B is an air gap.
Sweating causes a change in thermal mass of the nitrogen stream (D) that is sensed by the sudorometer and displayed
(right). From Low, P. A. 1992. “Sudomotor function and dysfunction.” In Diseases of the nervous system, eds. A. K. Asbury,
G. M. McKhann, and W. I. McDonald, Vol. 1, 2nd ed., 479–89. Philadelphia: WB Saunders Company. By permission of
Elsevier Science.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
632
Section 5: Assessment of Autonomic Function
axon. The absence of a response indicates failure of this axon, provided that iontophoresis is
successful and eccrine sweat glands are present. Because the axonal segment mediating the
response is likely to be short, the test probably
evaluates distal axonal function.
The QSART latency is sometimes markedly
reduced in painful neuropathies with persistent
sweat activity. The mechanism of the very short
latency (10–30 seconds) is probably augmented
somatosympathetic reflexes, with a reduced
threshold of polymodal C nociceptors—it often
occurs with allodynia.
Left forearm
100
50
0
Left proximal leg
100
50
0
Left distal leg
100
50
Applications
0
Left foot
100
50
0
0
2
4
6
8
10
Minutes
12
14
16
18
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 36–3. Quantitative sudomotor axon reflex test
distribution in a patient with distal small-fiber neuropathy.
Note reduction of sweat response in the distal leg and anhidrosis over the foot. From Low, P. A., and J. G. McLeod.
1997. “Autonomic neuropathies.” In Clinical autonomic
disorders: Evaluation and management, ed. P. A. Low, 2nd
ed., 463–86. Philadelphia: Lippincott-
Raven Publishers.
By permission of Mayo Foundation for Medical Education
and Research.
length-dependent pattern of QSART reduction
(Figure 36–3). Typically, the foot response is
absent first, and then sweating over the distal
leg is lost. Sweat reduction is also accepted if the
distal site is less than one-third that of the more
proximal site.
Another pattern is that of focal postganglionic denervation, as might occur with a peroneal or ulnar nerve lesion. Especially with focal
abnormalities, the best approach is to combine
QSART with thermoregulatory sweat test (see
Chapter 38). In contrast to postganglionic denervation, preganglionic denervation is recognized
by an intact QSART response in an area that is
anhidrotic on thermoregulatory sweat test.
Significance of the Test
A normal QSART test result indicates integrity
of the postganglionic sympathetic sudomotor
QSART has been used to detect postganglionic sudomotor failure in neuropathies (Low
et al. 1983; Low, Zimmerman, and Dyck 1986),
aging (Low et al. 1990), Lambert–Eaton myasthenic syndrome (McEvoy et al. 1989), amyotrophic lateral sclerosis (Litchy et al. 1987),
and preganglionic neuropathies with presumed
transsynaptic degeneration (Cohen et al. 1987;
Sandroni et al. 1991). In patients with distal
small-fiber neuropathy, it is the most sensitive
noninvasive diagnostic test available (Stewart,
Low, and Fealey 1992; Low et al. 2006). Done
under standardized conditions, the test is highly
reproducible and can be utilized to follow the
course of sudomotor deficit. This is useful in
monitoring the course of a neuropathy and in
evaluating response to therapy.
When QSART distribution is taken in conjunction with cardiovascular heart rate tests and
Finapres recordings of the Valsalva maneuver
and tilt as part of the autonomic reflex screen,
it helps define the distribution and severity of
autonomic failure (Low 1993b). Recently, the
test has been used to define the threshold and
duration of the local anhidrotic effect of botulinum toxin (Braune, Erbguth, and Birklein
2001). In studies of sympathetically maintained
pain, QSART recordings are performed bilaterally and simultaneously for evidence of asymmetry of latency, volume, and morphology of
the responses (Low and McManis 1985).
Another application of QSART is in the
detection of the site of the lesion. The QSART
in combination with the thermoregulatory sweat
test can be used to determine whether a lesion
is preganglionic or postganglionic. A preganglionic site is deduced when anhidrosis on the
thermoregulatory sweat test is associated with
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
36
Quantitative Sudomotor Axon Reflex and Related Tests
normal results on the QSART, and the lesion is
postganglionic when both tests show anhidrosis.
For comparisons among patients of different
ages and sex, these confounding variables can
be managed by at least two approaches. One,
the data can be expressed as normal deviates
(Low and McManis 1985). Two, an autonomic
scoring scale can be generated that corrects for
the effects of age and sex (Low 1993b). On this
scale, severity is scored from zero (no deficit)
to 3 (maximal deficit).
QDIRT
Limitations and Pitfalls of QSART
Neuropad
The main limitations of the test relate to the
efficiency of iontophoresis. Some subjects have
high skin resistance and can infrequently have
a spuriously absent response (because of high
skin resistance). Another limitation is that the
latency and volume could vary depending on
efficiency of iontophoresis, resulting in some
variability of response.
Neuropad is not really an autonomic reflex
test. It consists of recording the presence of
spontaneous sweating in the plantar aspect
of the foot by means of an adhesive pad containing an indicator powder. There is a color
change from blue to pink that indicates presence of sweating and presumably intact innervation (Papanas et al. 2013). The major value
of the test is its simplicity. Limitations are
that, unlike the thermoregulatory sweat test,
where you have a stimulus, an adequate endpoint, and a pathway to evaluate, Neuropad
does not test an autonomic reflex, and its
applicability is limited to areas of high resting
sweat response, so it cannot provide information on distribution of neuropathy. It is also
not quantitative.
OTHER METHODS OF SWEAT
MEASUREMENT
Several methods are available to simplify testing of sudomotor function. These include
imprint methods, QDIRT, and Neuropad
(Kennedy and Navarro 1993; Gibbons et al.
2008; Papanas et al. 2013).
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
633
Silicone Imprints
In the imprint method, plastic is dissolved in a
solvent, which dries in approximately 30 seconds.
The sweat droplet forms an imprint (Sutarman
and Thomson 1952). Alternatives are silicone
rubber monomers and colloidal graphite plastic (Sarkany and Gaylarde 1968; Harris, Polk,
and Willis 1972). Sweating can be induced by
pilocarpine iontophoresis (Kennedy et al. 1984).
Counts of sweat gland density are made under
a dissecting microscope and counting grid. This
technique has been applied systematically to
patients with diabetic neuropathy (Kennedy
et al. 1984; Kennedy and Navarro 1989). Of
interest is that approximately one-
third of
patients with normal electrophysiological tests
have abnormal results on the SIT (Kennedy and
Navarro 1993; Navarro and Kennedy 1989).
QDIRT tests axon-reflex sweating but substitutes high-resolution photography for recorded
volumes, requiring less expensive equipment
(Gibbons et al. 2008). Digital photographs
are recorded every 15 seconds and counts and
size can be quantitated. The value in the test
is cost-
saving. The limitation is that sweating results in drops’ coalescing so that counts
become unreliable.
SUMMARY
The application of noninvasive, sensitive,
quantitative, and dynamic tests of sudomotor function significantly enhances our ability to quantitate one aspect of the autonomic
deficit. The QSART has an important role in
clinical applications to better define the course
of neuropathy, its response to treatment,
and guide further exploration of sudomotor
physiology. Simpler methods are available as
screening tests.
REFERENCES
Braune, C., F. Erbguth, and F. Birklein. 2001. “Dose
thresholds and duration of the local anhidrotic effect
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
634
Section 5: Assessment of Autonomic Function
of botulinum toxin injections: Measured by sudometry.” British Journal of Dermatology 144:111–17.
Cohen, J., P. Low, R. Fealey, S. Sheps, and N. S. Jiang.
1987. “Somatic and autonomic function in progressive autonomic failure and multiple system atrophy.”
Annals of Neurology 22:692–99.
Gibbons, C. H., B. M. W. Illigens, J. Centi, and R.
Freeman. 2008. “QDIRT: Quantitative direct and
indirect testing of sudomotor function.” Neurology
70:2299–304.
Harris, D. R., B. F. Polk, and I. Willis. 1972. “Evaluating
sweat gland activity with imprint techniques.” Journal
of Investigative Dermatology 58:78–84.
Kennedy, W. R., and X. Navarro. 1989. “Sympathetic sudomotor function in diabetic neuropathy.” Archives of
Neurology 46:1182–86.
Kennedy, W. R., M. Sakuta, D. Sutherland, and F.
C. Goetz. 1984. “Quantitation of the sweating deficit
in diabetes mellitus.” Annals of Neurology 15:482–88.
Kennedy, W. R., and X. Navarro. 1993. “Evaluation of
sudomotor function by sweat imprint methods.” In
Clinical autonomic disorders: Evaluation and management, ed. P. A. Low, 253–61. Boston: Little, Brown
and Company.
Litchy, W. J., P. A. Low, J. R. Daube, and A. J. Windebank.
1987. “Autonomic abnormalities in amyotrophic lateral sclerosis.” Neurology 37 (Suppl. 1):162.
Low, P. A. 1993a. “Autonomic nervous system function.”
Journal of Clinical Neurophysiology 10:14–27.
Low, P. A. 1993b. “Composite autonomic scoring scale for
laboratory quantification of generalized autonomic
failure.” Mayo Clinic Proceedings 68:748–52.
Low, P. A. 1993c. “Laboratory evaluation of autonomic failure.” In Clinical autonomic disorders: Evaluation and
management, ed. P. A. Low, 169–95. Boston: Little,
Brown and Company.
Low, P. A. 1993d. “Pitfalls in autonomic testing.” In
Clinical autonomic disorders: Evaluation and management, ed. P. A. Low, 355–65. Boston: Little, Brown
and Company.
Low, P. A., P. E. Caskey, R. R. Tuck, R. D. Fealey, and
P. J. Dyck. 1983. “Quantitative sudomotor axon reflex
test in normal and neuropathic subjects.” Annals of
Neurology 14:573–80.
Low, P. A., R. D. Fealey, S. G. Sheps, W. P. Su, J.
C. Trautmann, and N. L. Kuntz. 1985. “Chronic idiopathic anhidrosis.” Annals of Neurology 18:344–48.
Low, P. A., T. L. Opfer-Gehrking, C. J. Proper, and I.
Zimmerman. 1990. “The effect of aging on cardiac
autonomic and postganglionic sudomotor function.”
Muscle and Nerve 13:152–57.
Low, P. A., B. R. Zimmerman, and P. J. Dyck. 1986.
“Comparison of distal sympathetic with vagal function in diabetic neuropathy.” Muscle and Nerve
9:592–96.
Low, P. A., and P. G. McManis. 1985. “Autonomic reflex
testing in sympathetic reflex dystrophy.” Neurology 35
(Suppl. 1):148A.
Low, V. A., P. Sandroni, R. D. Fealey, and P. A. Low. 2006.
“Detection of small-fiber neuropathy by sudomotor
testing.” Muscle and Nerve 34:57–61.
McEvoy, K. M., A. J. Windebank, J. R. Daube, and P.
A. Low. 1989. “3,4-
diaminopyridine in the treatment of Lambert-Eaton myasthenic syndrome.” New
England Journal of Medicine 321:1567–71.
Namer, B., A. Bickel, H. Kramer, F. Birklein, and
M. Schmelz. 2004. “Chemically and electrically
induced sweating and flare reaction.” Autonomic
Neuroscience—Basic and Clinical 114:72–82.
Navarro, X., and W. R. Kennedy. 1989. “Sweat gland reinnervation by sudomotor regeneration after different types of lesions and graft repairs.” Experimental
Neurology 104:229–34.
Papanas, N., A. J. Boulton, R. A. Malik, et al. 2013. “A
simple new non-invasive sweat indicator test for the
diagnosis of diabetic neuropathy.” Diabetic Medicine
30:525–34.
Periquet, M. I., V. Novak, M. P. Collins, et al. 1999. “Painful
sensory neuropathy: Prospective evaluation using skin
biopsy.” Neurology 53:1641–47.
Sandroni, P., J. E. Ahlskog, R. D. Fealey, and P. A. Low.
1991. “Autonomic involvement in extrapyramidal and
cerebellar disorders.” Clinical Autonomic Research
1:147–55.
Sarkany, I., and P. Gaylarde. 1968. “A method for demonstration of sweat gland activity.” British Journal of
Dermatology 80:601–5.
Stewart, J. D., P. A. Low, and R. D. Fealey. 1992. “Distal
small fiber neuropathy: Results of tests of sweating and
autonomic cardiovascular reflexes.” Muscle and Nerve
15:661–65.
Sutarman, and M. L. Thomson. 1952. “A new technique
for enumerating active sweat glands in man.” Journal
of Physiology 117:51–52.
Tobin, K., M. J. Giuliani, and D. Lacomis. 1999.
“Comparison of different modalities for detection of
small fiber neuropathy.” Clinical Neurophysiology
110:1909–12.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Chapter 37
Evaluation of Adrenergic Function
Phillip A. Low
INTRODUCTION
SKIN VASOMOTOR REFLEXES
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
BEAT-TO-BEAT BLOOD PRESSURE
RESPONSE TO THE VALSAVA
MANEUVER
BEAT-TO-BEAT BLOOD PRESSURE
RESPONSE TO TILT-UP
Technique
Findings
INTRODUCTION
Standing up causes a transient decrease in pulse
and blood pressure (BP). Baroreceptors in the
carotid sinus and aortic arch are unloaded.
The efferent portion of the baroreflex consists of a vagally mediated increase in heart
rate and activation of sympathetic efferents,
which increases total peripheral resistance.
Preganglionic sympathetic fibers are cholinergic and postganglionic fibers are adrenergic.
The preganglionic fiber is short and ends in
a paravertebral ganglion. In comparison, the
Composite Autonomic Severity
Score (CASS)
VENOARTERIOLAR REFLEX
DENERVATION SUPERSENSITIVITY
PLASMA NOREPINEPHRINE
SUSTAINED HANDGRIP
BAROREFLEX INDICES
SUMMARY
postganglionic fiber traverses the entire length
of a peripheral nerve.
Peripheral adrenergic function is important in the maintenance of postural normotension. It may be impaired in peripheral
neuropathies, and this may be manifested
as alterations in acral temperature, color, or
sweating. Simple, accurate, and reproducible tests of peripheral adrenergic function
are now routinely used in clinical autonomic
laboratories. This chapter describes methods used to determine peripheral adrenergic
function and their value and shortcomings.
635
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
636
Section 5: Assessment of Autonomic Function
Microneurography is used occasionally to
evaluate adrenergic function, but it is invasive and is not described here.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
SKIN VASOMOTOR REFLEXES
The integrity of postganglionic sympathetic
adrenergic fibers can be evaluated by testing skin vasoconstrictor reflexes (Low et al.
1983). These tests are of interest, although not
routinely used in clinical laboratory testing.
Studies are performed usually on the toe or finger pads, because the sympathetic innervation
in these sites is purely vasoconstrictor, whereas
other sites, such as the forearm, have both
vasoconstrictor and vasodilator fibers (Roddie,
Shepherd, and Whelan 1957).
Skin blood flow (SBF) is measured with
a laser Doppler flowmeter or with plethysmography, and the vasoconstrictor response
to an autonomic maneuver is determined.
Vasoconstriction can be induced by maneuvers such as inspiratory gasp, response to
standing (for the finger), contralateral cold
stimulus, or the Valsalva maneuver (VM). The
response can be expressed as a percentage of
vasoconstriction.
The pathways of these reflexes are complex.
For instance, the response to standing is mediated by the venoarteriolar reflex, low-pressure
and high-
pressure baroreceptors, and, to a
lesser extent, by increased levels in norepinephrine, renin, and vasopressin (Henriksen 1991;
Sundlof and Wallin 1978; Zoller et al. 1972;
Vendsalu 1960; Oparil et al. 1970; Williams et
al. 1986). The advantage of these reflexes is that
they have different afferents but an identical
final efferent pathway. Thus, the relevant afferent pathway can be evaluated. However, this
advantage is offset by a major shortcoming of
tests of skin adrenergic function—namely, the
marked sensitivity of skin sympathetic fibers
to emotional and temperature changes, which
means there is considerable ambient fluctuation of SBF (Burton and Taylor 1940). Skin
vasomotor reflexes have a coefficient of variation greater than 20% and are best regarded as
semiquantitative tests. However, the tests are
useful in comparing vasoconstrictor reflexes
from identical sites simultaneously.
BEAT-TO-BEAT BLOOD PRESSURE
RESPONSE TO THE VALSALVA
MANEUVER (VM)
The widely used tests to evaluate adrenergic
function in an autonomic laboratory are beat-
to-beat BP (and heart rate) responses to the VM
and head-up tilt (HUT). Other tests include
measurement of plasma levels of catecholamines, especially norepinephrine (supine and
standing), the sustained hand-
grip test, and
the response to pharmacological agents (Low
1997). These latter tests are generally insensitive (catecholamines), poorly reproducible in
the clinical laboratory setting, or too invasive.
The best validated tests are the BP and heart
rate responses to HUT and beat-to-beat BP
responses to the VM. These are the focus of
this chapter.
Beat-to-beat BP responses to the VM and tilt
are recorded simultaneously with the heart rate.
Dynamic alterations during tilt and the VM are
particularly important in detecting adrenergic
failure. The VM has four main phases: I, II,
III, and IV, with phase II subdivided into early
(II-E) and late (II-L) phases (Figure 37–1 and
Table 37–1). The mechanisms of the VM are
summarized briefly in Table 37–1.
The phases of the VM can be used to evaluate adrenergic function. This method of evaluating adrenergic function has been validated
in two ways. First, pharmacological dissection
studies have demonstrated that phase II-
L
is primarily under peripheral α-adrenergic
control and is selectively blocked by phentolamine, while phase IV is completely blocked
by propranolol, indicating that it depends on
β-adrenoreceptors (Sandroni, Benarroch, and
Low 1991). Second, the technique has also
been validated by studies of controls and age-
matched and sex-matched patient groups with
graded adrenergic failure (Low 1993; Vogel,
Sandroni, and Low 2005; Schrezenmaier et al.
2007). One group had generalized autonomic
failure, with an orthostatic decrease in systolic
BP during tilt of 30 mm Hg or greater. A second group had less orthostatic decrease in BP
(less than 30 mm Hg but greater than 10 mm
Hg), and a third group had well-documented
peripheral autonomic failure (absence of
response on the quantitative sudomotor
axon reflex test) but did not have orthostatic
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
37 Evaluation of Adrenergic Function
A
Normal subject M 22 yr
180
I
160
BP (mm Hg)
637
IV
II-E
140
II-L
120
100
80
III
60
40
0
20
40
60
Time (sec)
B
Panautonomic Neuropathy M 18 yr
160
I
BP (mm Hg)
140
120
IV
100
II-E
II-L
80
60
40
III
0
20
40
60
Time (sec)
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 37–1. Beat-to-beat BP responses to the VM in a control subject (A) and in a patient with panautonomic neuropathy
(B). In the control subject, reflex vasoconstriction, manifested as phases II-L and IV are well developed. In the patient with
panautonomic neuropathy, pulse pressure is much reduced during the maneuver, phases II-L and IV are absent, and PRT
is increased.
Table 37–1 Major Mechanisms
of Phases of the Valsava Maneuver
Phase
Main Mechanism
I
II-E
Compression of thoracic aorta
↓ in venous return; partial compensation
by vagus nerve
↑ in peripheral arteriolar tone
Release from compression of thoracic
aorta
↑ in cardiac sympathetic tone; sustained
↑ in arteriolar tone
II-L
III
IV
E, early; L, late; ↑, increase; ↓, decrease.
hypotension. In contrast to controls, all the
patient groups, including group 3, exhibited a
significant reduction in phase II-L. An excessive decrease in BP in phase II and absence
of a phase-IV overshoot were observed in the
group with florid orthostatic hypotension.
Intermediate changes were seen in the group
with borderline orthostatic hypotension.
The beat-
to-
beat BP changes during the
VM, when coupled with BP responses to tilt,
provide a significantly better evaluation of
adrenergic failure than did bedside recordings of BP. Patients with peripheral adrenergic
failure—for example. those with neuropathy
involving autonomic C fibers—have an absence
of phase II-L and a slight increase in phase II-
E. Patients with more severe and widespread
autonomic failure, such as widespread involvement of limb and splanchnic adrenergic fibers,
have a large phase II-E, an absence of phase
II-L, and typically have delayed blood pressure recovery time (PRT) and absent phase
IV (Figure 37–1) (Vogel, Sandroni, and Low
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
638
Section 5: Assessment of Autonomic Function
2005; Schrezenmaier et al. 2007). The gradations of alterations of the VM in different types
and degrees of autonomic failure have been
summarized on the basis of the experience in
the Mayo Autonomic Laboratory (Table 37–2).
The simplest approach is to measure PRT.
A more complete evaluation related PRT to the
antecedent fall in BP generating adrenergic
sensitivity (Schrezenmaier et al. 2007). A normative database has been generated for these
adrenergic indices (Huang et al. 2007).
BEAT-TO-BEAT BLOOD PRESSURE
RESPONSE TO TILT-UP
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Technique
Orthostatic BP recordings to tilt are recorded
using beat-to-beat BP and verified with a sphygmomanometer cuff with the patient supine and
following tilt to 70◦. It is important to perform
the upright tilt procedure at a standard time
after the patient lies down, because the orthostatic reduction in BP is greater after 20 minutes of preceding rest than after one minute; we
routinely perform HUT after a minimum of 30
minutes of recumbency. Beat-to-beat recordings
of systolic, mean, and diastolic BP are displayed
continuously on the computer console, as is heart
rate, which is derived from the electrocardiographic leads and monitor. Also, it is important
to ensure that the arm is at heart level, because
arm position influences the measurement of BP.
Findings
During upright tilt, normal subjects have
a transient decrease in systolic, mean, and
diastolic BP, followed by recovery within
one minute (Low et al. 1997). The decrement is modest (less than 10 mm Hg, mean
BP). Patients with adrenergic failure have
a marked and progressive decrease in BP
and pulse pressure. The heart rate response
typically is attenuated, but in patients whose
cardiac adrenergic innervation is spared,
the response is intact and may be increased.
Indices of mild adrenergic impairment
include excessive oscillations of BP, an excessive decrease (more than 50%) in pulse pressure, a transient (first minute) decrease in
systolic BP greater than 30 mm Hg, an excessive increment in heart rate (≥30 beats/minute), and a failure of total systemic resistance
to increase. Premonitory signs of syncope are
a progressive decrease in BP (especially diastolic BP), total peripheral resistance, pulse
pressure, and loss of BP (and heart rate) variability. Some of these indices are expected
abnormalities in a failure of arteriolar vasoconstriction (total peripheral resistance and
diastolic BP). Some are signs of increased
vascular capacitance (reduction in pulse pressure and excessive increment in heart rate).
Increased oscillations are indicative of intact
compensatory mechanisms (but are abnormal
because they indicate a system under stress),
whereas the gradual loss of variability indicates the failure of compensation.
Composite Autonomic Severity
Score (CASS)
A large autonomic database is available.
The normal response varies by age and sex.
To facilitate comparison, a 10-
point composite autonomic severity score (CASS) of
Table 37–2 Changes in Phases of Valsava Maneuver with Types
of Autonomic Failure
Condition
II-E
II-L
IV
Valsalva ratio
Normal
Vagal lesion
Adrenergic failure
Peripheral
Generalized
5–15 mm
<normal
To baseline
<normal
>baseline
Normal
Normal
<normal
↑
↑↑
↓ or absent; ↑ PRT
Absent; ↑ PRT
<normal
Absent
<normal
Reduced
↑, increase; ↓, decrease; PRT, BP recovery time.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
37 Evaluation of Adrenergic Function
autonomic function has been developed
(Low 1993). The scheme allots 4 points for
adrenergic and 3 points each for sudomotor
and cardiovagal failure. Each score is normalized for the confounding effects of age and
sex. Patients with a CASS score of 3 or less
have only mild autonomic failure; those with
scores of 7–10 have severe failure; and those
with scores between these two ranges have
moderate autonomic failure. The sensitivity
and specificity of the method were assessed
by evaluating CASS in four groups of patients
with known degrees of autonomic failure: 18
patients with multisystem atrophy, 20 with
autonomic neuropathy, 20 with Parkinson’s
disease, and 20 with peripheral neuropathy
but no autonomic symptoms. The composite scores (mean ± SD) for these four groups
were 8.5 ± 1.3, 8.6 ± 1.2, 1.5 ± 1.1, and 1.7 ±
1.3, respectively. Patients with symptomatic
autonomic failure had scores of 5 or more,
and those without symptomatic autonomic
failure had scores of 4 or less; no overlap
existed among these groups.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
VENOARTERIOLAR REFLEX
When venous transmural pressure is
increased by 25 mm Hg (e.g., by lowering
the limb by 40 cm), reflex arteriolar vasoconstriction occurs, reducing blood flow by 50%
(Henriksen 1991). This reflex, called the venoarteriolar reflex, has receptors in small veins,
and its neural pathway appears to be that
of the sympathetic C-fiber local axon reflex
(Figure 37–2) (Henriksen 1977). The function of the reflex has been suggested to be to
increase total peripheral resistance, compensating by up to 45% of the orthostatic decrease
in cardiac output (Henriksen 1977; Henriksen
et al. 1983). It may also reduce the orthostatic increase in tissue fluid by adjusting the
precapillary-to-postcapillary resistance ratio.
The venoarteriolar reflex was measured
in the feet of patients with diabetes mellitus
and was reported to be reduced in those with
diabetic neuropathy (Rayman et al. 1986).
The value of this test is its theoretical ability
to examine the status of sympathetic vasoconstrictor fibers at the postganglionic level.
Moy et al. studied the venoarteriolar reflex,
quantitative sudomotor axon reflex test, and
639
Arteriole
Vein
Venoarteriolar
reflex
Figure 37–2. Neural pathway for the venoarteriolar
reflex. The postganglionic axon comprises both the afferent and efferent limbs of the reflex. From Moy, S., T. L.
Opfer-Gehrking, C. J. Proper, and P. A. Low. 1989. “The
venoarteriolar reflex in diabetic and other neuropathies.”
Neurology 39:1490–92. By permission of the American
Academy of Neurology.
heart rate responses to deep breathing and
the VM in 40 control subjects, 49 diabetic subjects, and 29 subjects with other neuropathies
(Moy et al. 1989). The mean vasoconstrictor response was greater in the control group
than the diabetic group or other neuropathy
group, but the overlap among the groups was
marked. The venoarteriolar reflex appeared to
have lower specificity and much lower sensitivity than other tests of autonomic function.
The sensitivity and specificity were considered
inadequate for it to be used as a clinical test of
autonomic function.
DENERVATION SUPERSENSITIVITY
An exaggerated pressor response to the intra-
arterial or intravenous application of directly
acting α-
agonists (such as phenylephrine or
norepinephrine), indicating denervation supersensitivity, may occur when there is widespread
denervation of postganglionic sympathetic
fibers (Low et al. 1975; Moorhouse, Carter,
and Doupe 1966; Smith and Dancis 1964). The
mechanism of denervation supersensitivity is
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
640
Section 5: Assessment of Autonomic Function
an increase in receptor density, affinity, efficacy of receptor–
effector coupling, or other
postreceptor events. These tests of adrenergic
denervation supersensitivity are too invasive
for routine use and are insensitive.
It would be preferable to measure acral
adrenergically mediated vasoconstriction in
response to the above-
mentioned infusion.
However, recordings of vasoconstriction of the
muscle bed are indirect. Plethysmography can
be performed, but recorded flow is contaminated by SBF.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
PLASMA NOREPINEPHRINE
Plasma norepinephrine results from a spillover
of norepinephrine from adrenergic postganglionic nerve terminals. The supine value is an
index of net sympathetic activity and is affected
by the rate of norepinephrine secretion and
clearance (Polinsky et al. 1981; Wallin et al.
1981; Ziegler, Lake, and Kopin 1977; Polinsky
et al. 1985). Plasma norepinephrine has been
used to differentiate postganglionic from preganglionic failure. In a disorder in which the
lesion is preganglionic, resting supine norepinephrine values are normal, but the response
to standing is absent because of failure of activation. In a postganglionic lesion, the supine
norepinephrine plasma values are decreased if
the lesion is widespread. The disadvantage of
the method is its low sensitivity, largely because
80% of released norepinephrine is taken up
again by the neuron, and only 20% enters
venous blood. One method of enhancing clinical utility is to measure the intraneuronal
metabolite dihydroxyphenylglycol (DHPG).
SUSTAINED HANDGRIP
Sustained muscle contraction causes an
increase in systolic and diastolic BP and heart
rate. The stimulus derives from exercising
muscle, the reaction is reflexive in nature, and
the increase in BP is mediated by an increase
in cardiac output and peripheral resistance
(Coote, Hilton, and Perez-
Gonzalez 1971).
The test has been adapted as a simple test of
sympathetic autonomic failure. Ewing et al.
recommend 30% maximal contraction for up
to five minutes. Many patients have difficulty
sustaining the test for five minutes, but three
minutes is sufficient. The test evaluates generalized rather than peripheral adrenergic function (Ewing et al. 1974).
BAROREFLEX INDICES
Baroreflex indices evaluate the heart period
(reciprocal of heart rate) responses to induced
increases and decreases in BP. Phenylephrine
or norepinephrine can be used to increase
BP, and tilt or trinitroglycerin can be used to
decrease it. One approach, adapted from the
method of Korner, is to determine the range
and mean gain of the heart period (Low et al.
1975). These two indices express the range of
heart period in response to a moderate pressor-
hypotensive stress, and the mean rate of change
in heart period in response to sudden changes
in BP. Another related approach, described
by Pickering et al., relates beat-
to-
beat systolic BP to heart rate. An alternative approach
to stimulating baroreceptors is to use a neck
chamber whose pressure can be increased
or decreased (Pickering et al. 1972; Eckberg
et al. 1975). Finally, the heart period responses
to the decrease and increase in BP during the
VM can be related to changes in BP. Baroreflex
gain to an increase or decrease in BP primarily evaluates the vagal responses to changes in
BP. Baroreflex gain can also be determined in
response to spontaneous or induced changes in
BP. Commonly used maneuvers include spectral analysis, the VM, and the sequence method
(Dawson et al. 1997).
All these methods evaluate the vagal component of the baroreflex, and an efficient approach
is to relate the fall in BP during phase II-E to
the resultant heart period. However, the adrenergic component can be selectively involved, as
in certain neuropathies. Methodology is also
available to quantitate the adrenergic component of baroreflex sensitivity (Vogel, Sandroni,
and Low 2005; Schrezenmaier et al. 2007).
The adrenergic component of the baroreflex is
reflected in phase II-L and its continuation, the
PRT, which provides a reproducible index of
adrenergic baroreflex sensitivity. A more complete index can be derived by relating PRT to
the preceding fall in BP (Vogel, Sandroni, and
Low 2005; Schrezenmaier et al. 2007).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
37 Evaluation of Adrenergic Function
SUMMARY
For noninvasive evaluation of autonomic
function, tests of peripheral adrenergic function have recently been developed so that it is
possible to separately evaluate the vagal and
adrenergic components of baroreflex sensitivity. The vagal component is derived from
the heart period response to BP change, and
the adrenergic component by the PRT in
response to the preceding fall in BP, induced
by the VM.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
REFERENCES
Burton, A. C., and R. M. Taylor. 1940. Study of adjustment
of peripheral vascular tone to requirements of regulation of body temperature. The American Journal of
Physiology 129:565–77.
Coote, J. H., S. M. Hilton, and J. F. Perez-Gonzalez. 1971.
“The reflex nature of the pressor response to muscular
exercise.” The Journal of Physiology 215:789–804.
Dawson, S. L., T. G. Robinson, J. H. Youde, et al. 1997.
“The reproducibility of cardiac baroreceptor activity
assessed non-
invasively by spectral sequence techniques.” Clinical Autonomic Research 7:279–84.
Eckberg, D. L., M. S. Cavanaugh, A. L. Mark, and F.
M. Abboud. 1975. “A simplified neck suction device
for activation of carotid baroreceptors.” The Journal of
Laboratory and Clinical Medicine 85:167–73.
Ewing, D. J., J. B. Irving, F. Kerr, J. A. W. Wildsmith, and
B. F. Clarke. 1974. “Cardiovascular responses to sustained handgrip in normal subjects and in patients
with diabetes mellitus: A test of autonomic function.”
Clinical Science and Molecular Medicine 46:295–306.
Henriksen, O. 1977. “Local sympathetic reflex mechanism in regulation of blood flow in human subcutaneous adipose tissue.” Acta Physiologica Scandinavica
450(Suppl):1–48.
Henriksen, O. 1991. “Sympathetic reflex control of blood
flow in human peripheral tissues.” Acta Physiologica
Scandinavica 603(Suppl):33–39.
Henriksen, O., K. Skagen, O. Haxholdt, and V. Dyrberg.
1983. “Contribution of local blood flow regulation
mechanisms to the maintenance of arterial pressure
in upright position during epidural blockade.” Acta
Physiologica Scandinavica 118:271–80.
Huang, C. C., P. Sandroni, D. M. Sletten, S. D. Weigand,
and P. A. Low. 2007. “Effect of age on adrenergic and
vagal baroreflex sensitivity in normal subjects.” Muscle
and Nerve 36(5):637–42.
Low, P. A. 1993. “Composite autonomic scoring scale for
laboratory quantification of generalized autonomic
failure.” Mayo Clinic Proceedings 68:748–52.
Low, P. A. 1997. “Laboratory evaluation of autonomic
function.” In Clinical autonomic disorders: Evaluation
and management, ed. P. A. Low, 179–
208.
Philadelphia: Lippincott-Raven.
641
Low, P. A., C. Neumann, P. J. Dyck, R. D. Fealey, and R.
R. Tuck. 1983. “Evaluation of skin vasomotor reflexes
by using laser Doppler velocimetry.” Mayo Clinic
Proceedings 58:583–92.
Low, P. A., J. C. Denq, T. L. Opfer-Gehrking, P. J. Dyck, P.
C. O’Brien, and J. M. Slezak. 1997. “Effect of age and
gender on sudomotor and cardiovagal function and
blood pressure response to tilt in normal subjects.”
Muscle and Nerve 20:1561–68.
Low, P. A., J. C. Walsh, C. Y. Huang, and J. G. McLeod.
1975. “The sympathetic nervous system in diabetic
neuropathy. A clinical and pathological study.” Brain
98:341–56.
Moorhouse, J. A., S. A. Carter, and J. Doupe. 1966.
“Vascular responses in diabetic peripheral neuropathy.” British Medical Journal 1:883–88.
Moy, S., T. L. Opfer-Gehrking, C. J. Proper, and P. A. Low.
1989. “The venoarteriolar reflex in diabetic and other
neuropathies.” Neurology 39:1490–92.
Oparil, S., C. Vassaux, C. A. Sanders, and E. Haber.
1970. “Role of renin in acute postural homeostasis.”
Circulation 41:89–95.
Pickering, T. G., B. Gribbin, E. S. Petersen, D.
J. Cunningham, and P. Sleight. 1972. “Effects of autonomic blockade on the baroreflex in man at rest and
during exercise.” Circulation Research 30:177–85.
Polinsky, R. J., D. S. Goldstein, R. T. Brown, H. R. Keiser,
and I. J. Kopin. 1985. “Decreased sympathetic neuronal uptake in idiopathic orthostatic hypotension.”
Annals of Neurology 18:48–53.
Polinsky, R. J., I. J. Kopin, M. H. Ebert, and V. Weise.
1981. “Pharmacologic distinction of different orthostatic hypotension syndromes.” Neurology 31:1–7.
Rayman, G., S. A. Williams, P. D. Spencer, L. H. Smaje,
P. H. Wise, and J. E. Tooke. 1986. “Impaired microvascular hyperaemic response to minor skin trauma
in type I diabetes.” British Medical Journal (Clinical
Research Edition) 292:1295–98.
Roddie, I. C., J. T. Shepherd, and R. F. Whelan. 1957. “A
comparison of the heat elimination from the normal
and nerve-blocked finger during body heating.” The
Journal of Physiology (London) 138:445–48.
Sandroni, P., E. E. Benarroch, and P. A. Low. 1991.
“Pharmacological dissection of components of the
Valsalva maneuver in adrenergic failure.” Journal of
Applied Physiology 71:1563–67.
Schrezenmaier, C., W. Singer, N. M. Swift, D. Sletten, J.
Tanabe, and P. A. Low. 2007. “Adrenergic and vagal
baroreflex sensitivity in autonomic failure.” Archives of
Neurology 64:381–86.
Smith, A. A., and J. Dancis. 1964. “Exaggerated response
to infused norepinephrine in familial dysautonomia.”
The New England Journal of Medicine 270:704–7.
Sundlof, G., and B. G. Wallin. 1978. “Human muscle
nerve sympathetic activity at rest. Relationship to
blood pressure and age.” The Journal of Physiology
274:621–37.
Vendsalu, A. 1960. “Studies on adrenaline and noradrenaline in human plasma.” Acta Physiologica Scandinavica
49(Suppl 173):1–123.
Vogel, E. R., P. Sandroni, and P. A. Low. 2005. “Blood pressure recovery from Valsalva maneuver in patients with
autonomic failure.” Neurology 65:1533–37.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
642
Section 5: Assessment of Autonomic Function
Ziegler, M. Q., C. R. Lake, and I. J. Kopin. 1977. “The sympathetic nervous system defect in primary orthostatic
hypotension.” The New England Journal of Medicine
296:293–97.
Zoller, R. P., A. L. Mark, F. M. Abboud, P. G. Schmid,
and D. D. Heistad. 1972. “The role of low pressure
baroreceptors in reflex vasoconstrictor responses
in man.” The Journal of Clinical Investigation
51:2967–72.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Wallin, B. G., G. Sundlof, B. M. Eriksson, P. Dominiak,
H. Grobecker, and L. E. Lindblad. 1981. “Plasma
noradrenaline correlates to sympathetic muscle nerve
activity in normotensive man.” Acta Physiologica
Scandinavica 111:69–73.
Williams, T. D., D. Da Costa, C. J. Mathias, R. Bannister,
and S. L. Lightman. 1986. “Pressor effect of arginine
vasopressin in progressive autonomic failure.” Clinical
Science 71:173–78.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Chapter 38
Thermoregulatory Sweat Test
Robert D. Fealey
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
INTRODUCTION
ROLE OF THERMOREGULATORY SWEAT
TESTING: CLINICAL SYNDROMES
AND PROBLEMS EVALUATED
Small Fiber Neuropathy
Diabetic Peripheral Neuropathies
Severity of Autonomic Failure
Central Disorders
Hyperhidrotic Disorders
METHOD
INTRODUCTION
From a physiological viewpoint, the thermoregulatory sweat test (TST) consists of giving
a controlled heat stimulus to the body in a tolerable fashion to produce a generalized sweat
response (i.e., recruiting all areas of skin capable of sweating). The TST assesses the integrity
of efferent (central and peripheral) sympathetic
sudomotor pathways. Central (preganglionic)
structures tested include the hypothalamus,
bulbospinal projections, inter-mediolateral cell
column in the thoracic and upper lumbar spinal
OTHER METHODS OF MEASURING
SWEAT DISTRIBUTION
THERMOREGULATORY SWEAT
DISTRIBUTION
REPORTING RESULTS
TECHNICAL DIFFICULTIES AND PITFALLS
IN INTERPRETATION
SUMMARY
APPENDIX: SWEAT TEST PROCEDURE
cord, and white rami. Peripheral (postganglionic) autonomic structures tested include the
sympathetic chain ganglia and postganglionic
sudomotor axons, the M3 muscarinic cholinergic synapse, and the sweat glands. Because the
entire anterior body surface is tested for both
preganglionic and postganglionic lesions, the
TST is well suited for screening patients with
certain clinical symptoms or for demonstrating autonomic involvement in many disorders
(Benarroch 2014; Fealey 2008). These include
assessing the integrity of efferent sympathetic
sudomotor pathways, screening patients for
643
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
644
Section 5: Assessment of Autonomic Function
small fiber peripheral neuropathy, and assessing for autonomic involvement in patients with
many neurological and medical disorders.
ROLE OF THERMOREGULATORY
SWEAT TESTING: CLINICAL
SYNDROMES AND PROBLEMS
EVALUATED
A comprehensive listing of clinical syndromes
that can be evaluated with TST is given in
Table 38–1 (Fealey and Hebert 2012; Fealey
2008). Some common neurological applications of the TST evaluation are described in the
following sections.
exams are often normal in these patients,
whereas tests of skin autonomic innervation are usually abnormal. The TST has been
investigated in this syndrome and found to
show impaired sweating of the distal limbs in
72–74% of patients clinically diagnosed (Low
et al. 2006; Stewart, Low, and Fealey 1992).
The value of the TST in characterizing the distribution of neuropathy has been emphasized
in a published algorithm on the evaluation
of peripheral neuropathy (Dyck, Grant, and
Fealey 1996). Patients can be serially evaluated
via TST to document progression or recovery
(Figure 38–1) (Fealey 2010). We have recently
shown that there are neurogenic forms of dermatological condition, such as erythromelalgia,
that have characteristic TST abnormalities in
most instances (Davis et al. 2006).
Small Fiber Neuropathy
Peripheral neuropathies affecting smaller
diameter nerve fibers often cause the “burning
feet” syndrome. Nerve conduction studies and
electromyography and clinical neurological
Diabetic Peripheral Neuropathies
Diabetes mellitus produces distinct peripheral
neurological
disorders,
including
Table 38–1 Diseases Evaluated with TST
I.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
II.
III.
IV.
Generalized Autonomic Failure Syndromes
Pure autonomic failure (PAF)
Progressive autonomic failure as part of multiple system atrophy (MSA)
Primary disorders with isolated acquired idiopathic anhidrosis
Progressive isolated segmental anhidrosis
Idiopathic pure sudomotor failure
Chronic idiopathic anhidrosis
Ross syndrome
Primary autonomic neuropathies
Panautonomic (acute pandysautonomia) neuropathy
Autoimmune Autonomic Ganglionopathy
Postural tachycardia syndrome (POTS) (some cases)
Anhidrosis associated with other neurologic disorders
Cerebral disorders (stroke, tumor, infection, infiltration, trauma, cytokines)
Hypothalamic disorders (primary glioma, pineal tumor, post heat stroke)
Brain stem disorders (pontine and lateral medullary stroke)
Spinal cord disorders (spinal cord injury, multiple sclerosis, HIV myelopathy)
Degenerative disorders (other than MSA)
Dementia with Lewy Body Disease, Parkinson’s disease-autonomic failure
Peripheral nerve disorders
Hereditary sensory and autonomic neuropathy [HSAN types I, II, IV]
Guillain–Barré syndrome
Diabetic autonomic neuropathy
Hereditary and primary systemic amyloidosis
Lepromatous neuropathy
Alcoholic neuropathy
Fabry’s disease
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
38 Thermoregulatory Sweat Test
Table 38–1 (Continued)
V.
VI.
VII.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
VIII.
Idiopathic small fiber neuropathy
Erythromelalgia
Sympathectomy and other surgical lesions
Harlequin syndrome
Postural tachycardia syndrome
Lambert-Eaton myasthenic syndrome
Anhidrosis due to toxins and pharmacologic agents
Botulism, botulinum toxin injections
Venomous sting of box jellyfish
Ganglionic blockers, anticholinergics, carbonic anhydrase inhibitors
Opioids, ketamine-midazolam sedation
Anhidrosis associated with disorders of skin and sweat glands
Physical agents damaging skin (e.g. trauma, burns, pressure, scar, radiation
therapy)
Congenital and acquired skin diseases
Fabry and other congenital metabolic diseases
Anhidrotic ectodermal dysplasia
Ichthyosis
Neutrophilic eccrine hidradenitis
Sjogren’s syndrome
Systemic sclerosis (scleroderma)
Incontinentia pigmenti
Dermatomal vitiligo
Bazex–Dupre–Christol syndrome
Miliaria
Palmoplantar pustulosis
Psoriasis
Lichen planus
Atopic dermatitis
Primary (essential) focal hyperhidrosis
Palmoplantar, axillary, craniofacial, generalized hyperhidrosis
Secondary causes of localized hyperhidrosis
Cerebral infarction (e.g. frontal opercular or brain stem)
Other central nervous system disorders
Arnold–Chiari type 1 malformation
Myelopathies due to infarction, syringomyelia, tumor
Cold-induced sweating syndrome
Olfactory hyperhidrosis
Spinal Cord Injury
Autonomic dysreflexia
Posttraumatic Syringomyelia
Orthostatic hypotension triggered
Peripheral nervous system disorders
Peripheral motor neuropathy with autonomic dysfunction
Dermatomal or focal hyperhidrosis due to nerve trunk irritation
Compensatory segmental hyperhidrosis (postsympathectomy, Ross syndrome,
Pure Autonomic Failure)
Familial dysautonomia (Riley–Day), Morvan’s fibrillary chorea
Others
Gustatory sweating (physiologic, idiopathic, postherpetic, post nerve injury
[postsurgical, diabetic neuropathy, post infectious, tumor) invasion)
Lacrimal sweating
Harlequin syndrome
Idiopathic, localized hyperhidrosis
Idiopathic unilateral circumscribed hyperhidrosis
Postmenopausal localized hyperhidrosis
(continued)
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
645
646
Section 5: Assessment of Autonomic Function
Table 38–1 (Continued)
IX.
Associated with local skin disorders (e.g. blue rubber bleb nevi, glomus tumor,
burning feet syndrome, granulosis rubra nasi, pretibial myxedema, POEMS
syndrome)
Secondary causes of generalized hyperhidrosis
Central nervous system disorders
Episodic hypothermia with hyperhidrosis (Hines–Bannick or Shapiro’s
syndrome)
Posttraumatic or posthemorrhagic “diencephalic epilepsy”
Fatal familial insomnia and Parkinson’s disease
Fever and chronic infection (e.g. tuberculosis, malaria, brucellosis,
endocarditis)
Metabolic and systemic medical diseases (e.g. hyperthyroidism, diabetes
mellitus, hypoglycemia, hypercortisolism, acromegaly)
Malignancy (e.g. leukemia, lymphoma, pheochromocytoma, Castleman’s
disease, carcinoids, renal cell)
Medication induced (e.g. neuroleptic malignant syndrome, serotonin
syndrome, other medications)
Toxic syndromes (e.g. alcohol, opioid withdrawal, delirium tremens)
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
length-
dependent axonal neuropathy, painful truncal radiculopathy, and segmental and
diffuse autonomic neuropathy (Dyck and
Dyck 1999; Low and Fealey 1999). The ability to examine the whole anterior body surface in detail and the common involvement
of sudomotor axons in diabetes make the
TST particularly well suited to the evaluation
of this disorder. Most of the abnormal TST
distributions described later in the section
on “Thermoregulatory Sweat Distribution”
are from patients with diabetic neuropathy
(Fealey, Low, and Thomas 1989).
Peripheral neuropathy first produces distal sweat loss in the lower extremities, and
as the neuropathy advances, the fingertips
and the lower anterior abdomen become
affected. Painful truncal radiculopathy has
3/21/01
4/12/01
11/5/01
1/2/03
1/13/06
70
64
41
22
6
Figure 38–1. Recovering small fiber neuropathy. Serial TSTs in a patient with small fiber neuropathy. Extensive anhidrosis
(yellow shade) correlated with impaired temperature perception, the latter being the only abnormality on neurological exam.
Patient underwent intravenous immunoglobulin (IVIG) therapy between March 21 and Nov. 5, 2001, and began to improve.
Subsequent TSTs document near-complete recovery of sudomotor function in a length-dependent fashion. The percentage of
anhidrosis of the anterior body surface (TST%) (described in the “Reporting Results” section of this chapter) appears below
each figure, providing a quantitative measure of the improvement (sweating in purple shaded regions). (see color insert 38–1)
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
38 Thermoregulatory Sweat Test
a distinct clinical presentation of agonizing, and at times, lancinating pain associated
with cutaneous dysesthesia and a characteristic TST pattern of patchy, asymmetrical
anhidrosis primarily in the anterior distribution of one or several adjacent thoracic dermatomes in the distribution of the pain.
Radiculoplexus neuropathy commonly produces a large, asymmetrical sweat deficit in
the involved limb and, when the sympathetic
chain is involved, an “autosympathectomy”
appearance. Uncommonly, severe diabetic
autonomic neuropathy produces global anhidrosis. In general, the percentage of body
surface anhidrosis (TST%) correlates highly
with the degree of autonomic neuropathy symptoms and signs (Fealey, Low, and
Thomas 1989). Other neuropathies (e.g.,
primary systemic amyloid, autoimmune autonomic ganglionopathy, paraneoplastic, and
leprosy) with widespread, multifocal involvement are best evaluated via the TST (Wang
et al. 2008; Vernino et al. 2000; Vernino et al.
1998; Fealey 2012; Kimpinski et al. 2012b).
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Severity of Autonomic Failure
The TST is helpful in identifying autonomic
involvement in many neurological disorders.
An important use is in evaluating patients presenting with an extrapyramidal syndrome. The
differential diagnosis often involves separating multiple system atrophy (MSA), with its
severe autonomic failure, widespread anhidrosis, and poor prognosis, from Parkinson’s disease with mild or no autonomic involvement
on TST and better prognosis and response to
treatment (Fealey 2001; Sandroni et al. 1991;
Kihara, Sugenoya, and Takahashi 1991; Cohen
et al. 1987). Often the patient with early MSA
will exhibit a preganglionic, segmental sweat
deficit compatible with a central lesion affecting the intermediolateral cell columns of the
spinal cord (Low et al. 1981). Progression of
autonomic failure as documented via TST
has been shown to be characteristic of MSA
in well-
studied clinical and autopsy-
proven
cases (Figueroa et al. 2014; Kimpinski, Iodice,
Burton, et al. 2012a; Iodice et al. 2012; Lipp
et al. 2009).
Syndromes with selective sympathetic sudomotor failure include chronic idiopathic anhidrosis and Ross syndrome, clinical disorders
647
where TST can provide diagnostic information
when obtained in conjunction with cardiovagal, cardiovascular adrenergic, and postganglionic sympathetic sudomotor autonomic
tests (Fealey 2012; Nakazato et al. 2004; Low
et al. 1985; Faden, Chan, and Mendoza 1982;
Chemmanam et al. 2007; Nolano et al. 2006;
Ross 1958).
Central Disorders
Central disorders such as traumatic and
inflammatory myelopathy, hypothalamic neuroendocrine disorders, and disorders of thermoregulation (heat stroke, Shapiro syndrome)
may show abnormalities on TST, either in the
sweat pattern and/or in the core temperature
at which sweating/
anhidrosis is occurring.
Spinal cord disorders cause preganglionic TST
abnormalities, often showing the level of spinal
cord involvement in great detail (Figure 38–2)
(Fealey and Hebert 2012; Fealey 1997; Fealey
et al. 1984). The TST should be coupled with
a test of postganglionic sudomotor function to
confirm the central involvement.
Hyperhidrotic Disorders
Focal hyperhidrosis syndromes are routinely
evaluated via TST. Many times the area of
excessive sweating is unilateral and occurs in
compensation for widespread loss of sweating elsewhere (e.g., in pure autonomic failure
[PAF] or Ross syndrome). When excessive
sweating is confined to the palmar and plantar
areas in the resting-preheat state and there is
normal thermoregulatory sweating elsewhere,
the TST provides confirmation of a diagnosis
of primary focal (essential) hyperhidrosis. We
have used TST to delineate the effects of sympathotomy, a less invasive, endoscopic technique to treat hyperhidrosis of the hands and
to evaluate any patients having compensatory
hyperhidrosis after such procedures (Atkinson
et al. 2011; Atkinson and Fealey 2003).
METHOD
Thermoregulatory sweating is influenced by the
mean and local skin temperature as well as by the
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
648
Section 5: Assessment of Autonomic Function
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 38–2. Traumatic myelopathy. A patient with
segmental anhidrosis (yellow) with compensatory left-
sided hemihyperhidrosis (purple) due to a right greater
than left-sided upper thoracic spinal cord injury (alizarin
red indicator powder). From Fealey, R. D., and K. Sato.
2008. “Disorders of the eccrine sweat glands and sweating.” In Fitzpatrick’s dermatology in general medicine, eds.
K. Wolff, L. A. Goldsmith, S. I. Katz, B. A. Gilchrest, A. S.
Paller, and D. J. Leffell, Vol. 1, 7th ed., 720–30, Figure 82–2.
New York City: McGraw-Hill. (see color insert 38–2)
central (blood/
core) temperature (McCaffrey
et al. 1979). A maximal sweat response occurs
when both central (oral) and mean skin temperatures are increased in a moderately humid
(about 35–40% relative humidity) environment
in which some degree of sweat evaporation
can occur (Fealey 2008; Hsieh, McNeeley, and
Chelimsky 2001). Therefore, proper technique
includes controlling the ambient air temperature and humidity as well as the patient’s core
and skin temperature.
Equipment. Several techniques, including
hot baths and infrared (IR) and incandescent
heat lamps, have been used for the last 50 years
to produce sweating, but the most satisfactory
method is to use a cabinet in which the environment is controlled and the entire body (including the head) is heated. Guttmann described
such a cabinet and demonstrated the usefulness of the TST in the diagnosis and monitoring of spinal cord and peripheral nerve lesions
(Guttmann 1947). The TST conducted in the
Mayo Clinic Thermoregulatory Laboratory is
a modification of Guttmann’s quinizarin sweat
test and is described below (Guttmann 1947).
The patient, clad only in a towel(s) to
maintain modesty, is placed in a supine position on a gurney and enclosed in the cabinet
(Figure 38–3). The “head end” of the cabinet
is a clear vinyl curtain (tented over the gurney);
this arrangement allows the head to be in the
heated environment yet provides the patient a
clear view of the technician and outside world
to minimize claustrophobia. Windowed access
doors allow access and patient visibility. The
rear end of the cabinet contains the electrical and plumbing components that regulate
the environmental temperature, humidity, and
slow airflow rate.
Suitable parameters for achieving a generalized, maximal sweat response within 60 minutes
include an ambient temperature of 44–48oC
and a relative humidity of 35–40% while maintaining skin temperature between 39oC and
40oC. National Instruments components provide accurate measurement and proportional
control of the infrared heater lamps and skin
temperature, while Labview™ software provides a technician interface that monitors all
patient and cabinet parameters to ensure a safe
test with adequate stimulus parameters.
The major inside components of the TST
cabinet are shown in Figure 38–3. Within the
insulated walls are three overhead IR heaters
that heat the skin and are carefully regulated
by skin temperature feedback control. The
wide gurney, music played over rear-mounted
speakers (Spk), and bright fluorescent lighting
provide comfort for the patients as they rest
supine with palms down. Ceiling-
mounted,
remotely operated digital cameras (DC) photograph the developing sweat distribution
during the test and provide real-time patient
monitoring.
Measurement of Temperature and
Sweating. Thermistor probes (skin and oral
temperature probes [Sk/
OrPr]) continuously
measure skin and oral temperatures during the
test. Sweating on the skin surface is best visualized by an indicator powder that is applied to
the body before heating. The indicator powder
providing high color contrast between sweating
and non-sweating skin and applied over most
of the anterior body surface beforehand gives
the best result. A mixture of alizarin red, cornstarch, and sodium carbonate in a 50:100:50
gram ratio, respectively, is suitable (Fealey,
Low, and Thomas 1989). It is light orange on
non-sweating skin and turns dark purple on
sweating skin. Other indicators currently used
include iodinated cornstarch and starch and
iodine in solution (Sato et al. 1988; Khurana
1995). Overhead cameras can monitor the
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
38 Thermoregulatory Sweat Test
649
Cabinet vent
Environmental
air and humidity
control
Air duct heater
and fan
Vapor Logic
humidity
controller
DriSteem
humidifier
IR
Spk
DC
FL
Sk/OrPr
DC
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
IR
Figure 38–3. Top two images: Mayo Thermoregulatory Sweat Cabinet (outside front view on left, rear view on right).
Bottom two images: Inside view of Mayo Thermoregulatory Sweat Cabinet (ceiling shown on right). IR, infrared heaters;
DC, digital camera; Sk/OrPr, skin and oral temperature probes; FL, fluorescent light; Spk, speakers.
patient, show the recruitment pattern of sweating, and provide photographs of the body surface at test end. These photos and those taken
outside the cabinet at the end document the
result and are used to create a digital image
that can be analyzed for percent anhidrosis
(TST%).
Temperature Response. The average
response of the oral temperature in 35 healthy
control subjects (20–75 years old) who achieved
full-body, maximal sweating during the TST
was an increase of 1.2oC in 35–40 minutes.
Because all subjects had sweated profusely at
an oral temperature of less than or equal to
38oC, we use this temperature as a test end
point (Figure 38–4).
For 1,412 patients having a TST in 2006,
the mean oral temperature increase was 1.5oC,
with 38oC or a 1oC increase above baseline
(whichever yielded the higher temperature)
as an end point (Fealey 2008). These observations indicate that the often-
quoted 1oC
temperature-increase criterion for an adequate
TST is inadequate in patients with lower (i.e.,
<37oC) initial temperatures (Bannister, Ardill,
and Fentem 1967).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
650
Section 5: Assessment of Autonomic Function
39.0
38.0
ºC
37.0
36.0
0
5
10
15
20
25
30
Heating time (min)
Skin temp
Oral (core) temp
Sweat rate (arbitrary units)
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 38–4. Mean skin and oral temperatures and sweat rates of 35 healthy controls during the TST. By 38°C oral temperature, all had reached a maximum sweat rate. From Fealey, R. D. 1997. “Thermoregulatory sweat test.” In Clinical autonomic disorders: Evaluation and management, ed. P. A. Low, 2nd ed., 245–57, Figure 2. Philadelphia: Lippincott-Raven.
If generalized sweating occurs at a lower
body temperature, the test can be ended
before 38oC is reached. For reasons of patient
comfort and safety, we do not increase oral
temperature above 38.5oC or extend the heating period beyond 65 minutes. The current
procedure followed by the TST lab technician
is specified in the appendix to this chapter.
Achieving maximal sweating is of great importance in evaluating sympathetic sudomotor
function and in test reliability and reproducibility. A study using a similar magnitude of
air and skin temperature and humidity and
exposure duration has clearly shown that this
thermal stress produces maximal thermoregulatory sweating (Hsieh, McNeeley, and
Chelimsky 2001).
OTHER METHODS OF MEASURING
SWEAT DISTRIBUTION
Sweat gland activity can be studied quantitatively by a number of other techniques, including the sympathetic skin response (SSR), filter
paper collection, weighing and analyzing of
sweat composition, the quantitative sudomotor axon reflex tests (QSART, QSWEAT and
QDIRT), silastic mold or iodine-impregnated
paper imprint following pilocarpine stimulation,
microcannulation of the sweat duct, collection into a Macroduct® coil, and humidity
sensors within ventilated capsules (Hilz and
Dutsch 2006; Kucera, Goldenberg, and Kurca
2004; Low et al. 1983; Sletten, Weigand, and
Low 2010; Gibbons et al. 2008; Kennedy,
Wendelschafer-
Crabb, and Brelje 1994; Sato
and Sato 1983; Cole and Boucher 1986). Other,
more sophisticated, techniques utilize microdialysis membranes delivering minute quantities of transmitter substances to the dermis
or employ confocal electronmicroscopy, and
immunohistochemical analysis of biopsied skin
stained for peptides and proteins making up the
structure and innervation of the sweat gland
(Morgan et al. 2006; Kennedy, Wendelschafer-
Crabb, and Brelje 1994; Gibbons et al. 2009).
QSART and QSWEAT measure postganglionic axon reflex sweating. The SSR measures hand and foot spinal and postganglionic
sympathetic activity. Silastic mold, iodine-
impregnated paper imprint, and Macroduct
measure direct sweat gland activation and
postganglionic innervation via pilocarpine iontophoresis. Punch biopsies can examine sweat
gland and intra-epidermal nerve fiber densities. These techniques are sometimes done at
multiple sites to provide information on the
distribution of sweating abnormalities.
It is desirable to combine several methods
for determining the integrity of the eccrine
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
651
38 Thermoregulatory Sweat Test
sweat response. For example, a TST can be
combined with tests of the sweat gland and/
or its peripheral nerve innervation to localize
a sweating disorder to the peripheral or central nervous system, or a volumetric technique
can be combined with a sweat droplet distribution imprint to estimate the sweat volume per
active gland. The TST done first can provide
direction to the optimum testing site for more
focused techniques.
THERMOREGULATORY SWEAT
DISTRIBUTION
Elderly men and women tend to have types 2
and 3, and the lighter-sweating areas may have
a higher threshold of activation.
Abnormal Distributions
Six types of abnormal thermoregulatory sweat
patterns or distributions have been described
(Figure 38–6) (Fealey 2008).
1. Distal anhidrosis is characterized by sweat
loss in the fingers; the distal legs, feet,
and toes; and the lower anterior abdomen
(Figure 38–6 (1)). When this pattern is
Normal Distributions
1
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
The normal variants in sweat distribution
observed in the Mayo TST clinic laboratory
in healthy control subjects from age 20–75 is
shown in Figure 38–5 (Fealey 2008). Areas
of “normal” anhidrosis may occur over bony
prominences (e.g., the patella and clavicle)
and in the inner thighs. The proximal extremities frequently show less sweating than the distal, but left–right symmetry is always the rule.
Males tend to show the type 1 (heavy, generalized sweating) pattern, whereas females
usually show the type 2 (heavy, generalized
sweating but less in proximal extremities) or
type 3 (generalized sweating but less in proximal extremities and lower abdomen) pattern.
3
4
6
Type 2
Type 1
Type 3
Figure 38–5. Normal thermoregulatory sweat distributions. Sweating areas in purple(darker) shading. From
Low, P. A., and R. D. Fealey. Sudomotor neuropathy.” In
Diabetic neuropathy, edited by Dyck, P. J. and Thomas
Dyck, P. K. Philadelphia: W.B. Saunders Company.
Chapter 13: 191–199. (see color insert 38–5)
2
5
7
Figure 38–6. Abnormal TST distributions compared with
Type 1 normal. Examples of the most commonly encountered
abnormal sweat distribution patterns: Distal (1), segmental
(2 and 4), regional (3), global (6), focal (5) and mixed (2, 4,
and 5); normal image (7). Sweating areas in purple (darker)
shading. From Low, P. A., and R. D. Fealey. Sudomotor neuropathy.” In Diabetic neuropathy, edited by Dyck, P. J. and
Thomas Dyck, P. K. Philadelphia: W.B. Saunders Company.
Chapter 13: (191–199). (see color insert 38–6)
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
652
2.
3.
4.
5.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
6.
Section 5: Assessment of Autonomic Function
noted, a peripheral autonomic neuropathy
is highly likely.
Segmental anhidrosis involves large contiguous zones of the body surface bordered
by areas of normal sweating; these usually
respect sympathetic dermatomal borders or
spinal cord levels and are often asymmetric. (Figure 38–6 (2) and 38–6 (4)). Testing
the TST area of anhidrosis with a peripheral sudomotor test such as QSART is often
needed to characterize the segmental anhidrosis as central or peripheral (preganglionic vs. postganglionic).
Regional anhidrosis refers to large anhidrotic areas (but <80%) that blend gradually into sweating areas and that may or may
not be contiguous; anhidrosis of the trunk
alone and anhidrosis of the proximal parts
of all four extremities are examples of this
pattern (Figure 38–6 (3)).
Mixed patterns are combinations of any of
the above in the same patient; for example, focal and distal patterns of anhidrosis
(Figure 38–6 (2), 38–6 (4), and 38–6 (5)).
Focal sweat loss is confined to isolated dermatomes, peripheral nerve territories, or small
localized areas of the skin (Figure 38–6 (5)).
This pattern is usually diagnostic of a peripheral nerve branch or a focal skin disorder.
Global anhidrosis, by definition, occurs
when more than 80% of the body surface is
involved (Figure 38–6 (6)). Small “islands”
of active sweat glands may be present, or
there may be acral (hands and feet) preservation of sweating with this pattern.
REPORTING RESULTS
Data about the age, sex, identity number, clinical problem of the patient, and the date of the
TST are indicated on the report (Figure 38–7).
The body of the report includes a Results section showing the initial and final core temperatures, the percentage of body surface
anhidrosis, the type of sweat pattern, and an
anatomical figure drawing showing the distribution of the sweating or anhidrosis. This
anatomical figure is generated by modifying a
computerized graphics body image to look like
the digital camera images taken of the patient
at the end of the test. This figure is used to calculate the percentage of anterior body surface
anhidrosis (TST%) (Fealey, Low, and Thomas
1989). This technique has recently been modified as described below. The body figure also
provides a permanent record of the sweat distribution when printed on a color inkjet printer.
The figure and camera images are reviewed by
the reporting physician to ensure accuracy, and
an impression of what the results are and then
their clinical significance is noted.
The TST result can be quantified by determining the cumulative area of the anterior
body surface that does not sweat. This is called
the percent of anhidrosis (TST%). Using the
digital camera images and the computerized
graphic body image template having three
basic colors (yellow for anhidrosis, purple for
sweating skin, and black for the outline and
body landmarks), the technician creates an
accurate patient graphic body image in a .gif
file format. This image is then processed using
a pixel-
counting program known as ImageJ
(Schneider, Rasband, and Eliceiri 2012). This
program determines the number of purple pixels from an image histogram, and the percent of
anhidrosis is calculated using the formula: percent anhidrosis = [1-pixel count/90899] x 100.
The 90899 number is the purple pixel count of
the template normal body image.
Another accurate method for deriving the
TST% is to use planimetry (LASICO, Model
1252 M; resolution = 0.005 cm2). The drawn
body image is scrutinized, and the region(s)
of anhidrosis are outlined and measured; individual areas are summated to produce a total
anterior body surface estimate.
The TST% provides for quantitation of the
test result and can be useful in clinical studies
and in following the clinical course of patients
with autonomic disorders (Lipp et al. 2009;
Kimpinski et al. 2009; Low et al. 2006; Vernino
et al. 2000; Sandroni et al. 1991; Fealey, Low,
and Thomas 1989; Kimpinski, Iodice, Sandroni,
et al. 2012; Kimpinski, Iodice, Burton, et al.
2012; Fealey 2010).
TECHNICAL DIFFICULTIES
AND PITFALLS IN INTERPRETATION
Interpretation Pitfalls
The interpreter must be aware of the normal patterns of thermoregulatory sweating,
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
38 Thermoregulatory Sweat Test
653
Figure 38–7. TST report form: Example from a patient with autoimmune autonomic ganglionopathy. (see color insert 38–7)
including areas where anhidrosis may be seen
normally, such as over bony prominences or
the lateral calves (Figure 38–5).
Patients who have worn pressure wraps (i.e.,
ace bandages and abdominal binders) within
12 hours before the test may show anhidrosis in
the areas that had been covered. This is usually
recognized by the straight edges of the deficit.
Severely dehydrated patients may sweat less
overall, but they generally do not have focal
defects (Fortney et al. 1981). Anticholinergic
drugs, including most tricyclic antidepressants, may inhibit thermoregulatory sweating and should be stopped 48 hours before
the TST is performed. Mu-
receptor opioid
agonists (narcotic analgesics) can elevate the
set point temperature for sweat onset and so
may produce a false-positive result if the usual
endpoint temperature is used to end the test.
Retesting 12–24 hours off short-acting opioids
is required for an accurate test.
Patients who are febrile and have an elevated
core temperature above 37.0oC at the start of
the TST may not sweat normally at the usual
endpoint temperature of 38.0oC. We therefore
will test such patients after they have become
afebrile.
The application of skin lotions such as moisturizing creams may produce a discoloration
of alizarin-covered skin, making it difficult to
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
654
Section 5: Assessment of Autonomic Function
discern areas of anhidrosis as well as normal
sweating. Consequently, the use of lotions is
prohibited on the day of the TST.
Anhidrosis in elderly patients may present
an interpretative challenge, because the effect
of aging on the autonomic nervous system
may be responsible for the regional anhidrosis (most often affecting the lower abdomen
and proximal extremities) that is seen in some
older women who have normal neurological
examinations but report having had dry skin
for many years. Whether this represents a variant of chronic idiopathic anhidrosis or a loss
of functional sweat glands, or reflects the loss
of preganglionic autonomic neurons known to
occur with aging, is unclear (Low et al. 1985;
Low, Okazaki, and Dyck 1977). Aging is associated with declining postganglionic sympathetic sudomotor responses in the distal leg
and foot as well (Low 1997). In our controls
aged 20–75 years (19 men and 16 women),
there was no significant regression of percent
anhidrosis with age, although the mean age was
a relatively young 52 years (Fealey, Low, and
Thomas 1989). Senile atrophy of the skin and
differences in sweat gland training between
young and old may also be a factor. Our current view is to interpret the anhidrosis of the
elderly as abnormal and deserving of additional
workup to find an etiology.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Technical Problems
Potential technical problems with the TST
include the untidiness and duration of the test,
the possibility of skin heat injury, or skin irritation caused by the indicator powder alizarin.
Contact dermatitis occurs rarely (observed frequency, 3:1000 subjects) and is readily treated
with oral and topical agents. A more common
but harmless problem is the persistence of purple discoloration of small skin areas; it may take
several days for the color to wash off. Because of
repeated exposure to the indicator powder, technicians in our laboratory wear masks, gloves, and
goggles when applying the powder to minimize
inhalation, oral ingestion, or contact with the
eyes. Patients are also given goggles and masks
while the powder is applied under a ventilated
hood that traps airborne indicator dust, protecting personnel, patients, and equipment.
Technicians and patients are made aware of
possible skin reactions before application, and
extremely sensitive individuals are not tested.
Our legal department is aware of the non-FDA-
approved use; we accept the use of alizarin as
a reasonable medical risk where no good substitute (except perhaps iodinated starch) exists
and the incidence of skin reactions is very low.
Patients who are extremely claustrophobic,
who indicate a history of severe contact dermatitis, or who are less than five years old are usually not tested.
The TST can be used in controlled trials
to monitor the progression of disease or the
response to treatment as long as one adheres
rigorously to thermoregulatory stimulus guidelines and has a way to quantitate the results
(such as the percentage of body surface anhidrosis). The TST produces reproducible data
and is complementary to anatomically focused
techniques of autonomic testing.
SUMMARY
The TST assesses the integrity of central and
peripheral efferent sympathetic sudomotor
neural pathways. A controlled heat and humidity stimulus is given to produce a generalized
sweating response in all skin areas capable of
sweating. Sweating is visualized by placing an
indicator powder on the skin beforehand. The
entire anterior body surface can be examined,
and abnormalities can usually be detected at a
glance.
Clinical disorders effectively evaluated by
the TST, the characteristic normal and abnormal sweat distributions, the methods to reliably
perform the TST, preparation of a report of the
test results, and the techniques to quantify the
response including the “percentage of anhidrosis” were described herein. Important parameters of the heat stimulus, the patient’s oral and
skin temperature response, and pitfalls in the
interpretation of the sweat test results were
also described.
APPENDIX: SWEAT TEST
PROCEDURE
1. Preheat and humidify the sweat cabinet
by turning it on 45–60 minutes before
the test. The set points are 48oC air
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
38 Thermoregulatory Sweat Test
2.
3.
4.
5.
6.
7.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
8.
9.
10.
temperature and 40% relative humidity.
The overhead IR heaters can also be set
to 48oC to accelerate the preparation.
Meet the patient and briefly describe the
test; weigh the patient and then have
them undress.
Place towel(s) on the patient to cover as
little skin as feasible to maintain modesty. Place respirator mask on the patient.
Remove after powdering. Put on your
respirator mask, goggles, and gloves.
Start the ventilator hood and apply the
indicator powder (alizarin red, cornstarch, and sodium carbonate).
Place elastic straps to hold the anterior
abdomen, proximal leg, and forehead
thermistor probes. Take the sterile oral
probe and its sponge holder and place it
in the patient’s mouth between the gum
and the cheek. Turn down the overhead
IR heater control setting from 48oC (step
1) to 36oC.
As quickly as possible, open the vinyl curtain and place the patient and gurney in
the cabinet; close the curtain. Open side
doors and place the skin temperature
probes under the elastic straps.
Connect probes to thermometer input
plugs. Record baseline oral and skin temperatures. Check stability of oral temperature during breathing and talking; allow
three minutes for stabilization; begin timing the sweat test.
Check the cabinet temperature and
humidity every five minutes; operating conditions have to be as follows to
ensure an adequate and safe heat stimulus: Air temperature 44°C–48°C. Relative
humidity 35%–
40%. Skin temperature
38.5°C–39.5°C
Try to make all observations through the
closed side doors; open the curtain if necessary to wipe the patient’s forehead.
If the patient sweats completely (fully
saturating the powder on all skin areas)
before the oral temperature reaches
38.0°C, advise the physician and end the
test. Otherwise, continue the test until
the oral temperature is 38.0°C or 1.0°C
above the initial oral temperature (whichever is greater). Do not exceed oral temperature of 38.5°C or total heating time
of 65 minutes. Using the overhead digital
cameras, photograph the developing sweat
11.
12.
13.
14.
15.
655
distribution, obtaining additional photos
for abnormalities.
At the end of the test, turn off heat, remove
the probes, and take the patient out of
the cabinet. Obtain additional digital photos of abnormal areas, chart the pattern of
sweating on the report form, and call the
physician to inspect the sweat distribution
and prepare the report. Help the patient
shower. Keep the laboratory neat by making sure the shower curtain is inside the
stall, by vacuuming any loose powder and
briefly mopping floor. Wash the skin probes
with soap and warm water; wash off the oral
probe and put it in its pouch for sterilization.
Put fresh linen on gurney for next test.
Check to see that the patient has showered
off most of the powder, and help him or
her dress if necessary. Weigh the patient
again.
Offer
electrolyte-
replacement
drink. Place all used towels and linen in the
laundry bag.
Enter the test data into the laboratory
computer; draw the final body sweat-
distribution image and calculate or measure the percentage of anhidrosis. Prepare
the electronic report for patient’s medical
record and print a paper copy for the laboratory report file.
When performing a second sweat test on
the same patient, ensure the same endpoint temperature and increase in oral
temperature are achieved to allow comparison of resulting sweat distributions.
REFERENCES
Atkinson, J. L., and R. D. Fealey. 2003. “Sympathotomy
instead of sympathectomy for palmar hyperhidrosis: Minimizing postoperative compensatory hyperhidrosis.” Mayo Clinic Proceedings 78(2):167–72.
doi: 10.4065/78.2.167
Atkinson, J. L., N. C. Fode-
Thomas, R. D. Fealey, J.
H. Eisenach, and S. J. Goerss. 2011. “Endoscopic
transthoracic limited sympathotomy for palmar-
plantar hyperhidrosis: Outcomes and complications
during a 10-year period.” Mayo Clinic Proceedings
86(8):721–29. doi: 10.4065/mcp.2011.0199
Bannister, R., L. Ardill, and P. Fentem. 1967. “Defective
autonomic control of blood vessels in idiopathic orthostatic hypotension.” Brain: A Journal of Neurology
90(4):725–46.
Benarroch, E. E. 2014. Autonomic neurology.
Contemporary neurology series. Chapter 10, pp. 126–
143. New York: Oxford University Press.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
656
Section 5: Assessment of Autonomic Function
Chemmanam, T., J. D. Pandian, R. S. Kadyan, and S.
M. Bhatti. 2007. “Anhidrosis: A clue to an underlying autonomic disorder.” Journal of Clinical
Neuroscience: Official Journal of the Neurosurgical
Society of Australasia 14(1):94–
96. doi: 10.1016/
j.jocn.2005.11.041
Cohen, J., P. Low, R. Fealey, S. Sheps, and N. S. Jiang.
1987. “Somatic and autonomic function in progressive autonomic failure and multiple system atrophy.”
Annals of Neurology 22(6):692–
99. doi: 10.1002/
ana.410220604
Cole, D. E., and M. J. Boucher. 1986. “Use of a new
sample-collection device (Macroduct) in anion analysis
of human sweat.” Clinical Chemistry 32(7):1375–78.
Davis, M. D., J. Genebriera, P. Sandroni, and R. D. Fealey.
2006. “Thermoregulatory sweat testing in patients
with erythromelalgia.” Archives of Dermatology
142(12):1583–88. doi: 10.1001/archderm.142.12.1583
Dyck, P. J., and J. B. Dyck. 1999. “Diabetic polyneuropathy.” In Diabetic neuropathy, edited by Dyck, P. J. and
Thomas, P. K. Philadelphia: W.B. Saunders Company.
Dyck, P. J., I. A. Grant, and R. D. Fealey. 1996. “Ten steps
in characterizing and diagnosing patients with peripheral neuropathy.” Neurology 47(1):10–17.
Faden, A. I., P. Chan, and E. Mendoza. 1982. “Progressive
isolated segmental anhidrosis.” Archives of Neurology
39(3):172–75.
Fealey, R. 2010. “Subacute immune sensory and
autonomic neuropathy following a cytomegalovirus infection.” In Companion to peripheral neuropathy, edited by P. J. Dyck. Chapter 62: 267–270.
Philadelphia: SAUNDERS.
Fealey, R. D. 1997. “Autonomic dysfunction in spinal cord
disease.” In Spinal cord disease basic science, diagnosis and management, edited by E. and Eisen Critchley,
A. Chapter 13: 219–227. London: Springer-Verlag.
Fealey, R. D. 2001. “Use of the thermoregulatory sweat test
in the evaluation of patients with autoimmune autonomic neuropathy and early multiple system atrophy.”
Japanese Journal of Perspiration Research 8:37–40.
Fealey, R. D. 2008. “Thermoregulatory sweat test.”
Clinical Autonomic Disorders Third edition. Chapter
18: 244–260.
Fealey, R. D., P. A. Low, and J. E. Thomas. 1989.
“Thermoregulatory sweating abnormalities in diabetes
mellitus.” Mayo Clinic Proceedings 64(6):617–28.
Fealey, R. D., J. H. Szurszewski, J. L. Merritt, and E.
P. DiMagno. 1984. “Effect of traumatic spinal cord
transection on human upper gastrointestinal motility
and gastric emptying.” Gastroenterology 87(1):69–75.
Fealey, R. D., and A. A. Hebert. 2012. “Disorders
of the eccrine sweat glands and sweating.” In
Fitzpatrick’s dermatology in general medicine,
edited by L. A. Goldsmith, K. Wolff, S. I. Katz, B.
A. Gilchrest, A. S. Paller, and D. J. Leffell. 936–947.
New York: McGraw-Hill.
Figueroa, J. J., W. Singer, A. Parsaik, et al. 2014. “Multiple
system atrophy: Prognostic indicators of survival.”
Movement Disorders: Official Journal of the Movement
Disorder Society 29(9):1151–
57. doi: 10.1002/
mds.25927
Fortney, S. M., E. R. Nadel, C. B. Wenger, and J. R. Bove.
1981. “Effect of blood volume on sweating rate and
body fluids in exercising humans.” Journal of Applied
Physiology 51:1594–600.
Gibbons, C. H., B. M. Illigens, J. Centi, and R. Freeman.
2008. “QDIRT: Quantitative direct and indirect test
of sudomotor function.” Neurology 70(24):2299–304.
doi: 10.1212/01.wnl.0000314646.49565.c0
Gibbons, C. H., B. M. Illigens, N. Wang, and R.
Freeman. 2009. “Quantification of sweat gland
innervation:
A
clinical-pathologic
correlation.” Neurology 72(17):1479–
86. doi: 10.1212/
WNL.0b013e3181a2e8b8
Guttmann, L. 1947. “The management of the quinizarin
sweat test (Q.S.T.).” Postgraduate Medical Journal
23(262):353–66.
Hilz, M. J., and M. Dutsch. 2006. “Quantitative studies of
autonomic function.” Muscle and Nerve 33(1):6–20.
doi: 10.1002/mus.20365
Hsieh, C., K. McNeeley, and T. C. Chelimsky. 2001. “The
clinical thermoregulatory sweat test induces maximal sweating.” Clinical Autonomic Research: Official
Journal of the Clinical Autonomic Research Society
11(4):227–34.
Iodice, V., A. Lipp, J. E. Ahlskog, et al. 2012. “Autopsy confirmed multiple system atrophy cases: Mayo experience and role of autonomic function tests.” Journal of
Neurology, Neurosurgery, and Psychiatry 83(4):453–
59. doi: 10.1136/jnnp-2011-301068
Kennedy, W. R., G. Wendelschafer-Crabb, and T. C. Brelje.
1994. “Innervation and vasculature of human sweat
glands: An immunohistochemistry-laser scanning confocal fluorescence microscopy study.” The Journal of
Neuroscience: The Official Journal of the Society for
Neuroscience 14(11 Pt 2):6825–33.
Khurana, R. K. 1995. “Oculocephalic sympathetic dysfunction in posttraumatic headaches.” Headache
35(10):614–20.
Kihara, M., J. Sugenoya, and A. Takahashi. 1991. “The assessment of sudomotor dysfunction in multiple system atrophy.” Clinical Autonomic Research: Official Journal of
the Clinical Autonomic Research Society 1(4):297–302.
Kimpinski, K., V. Iodice, D. D. Burton, et al. 2012a. “The
role of autonomic testing in the differentiation of
Parkinson’s disease from multiple system atrophy.”
Journal of the Neurological Sciences 317(1–2):92–96.
doi: 10.1016/j.jns.2012.02.023
Kimpinski, K., V. Iodice, P. Sandroni, R. D. Fealey, S.
Vernino, and P. A. Low. 2009. “Sudomotor dysfunction in autoimmune autonomic ganglionopathy.” Neurology 73(18):1501–
06. doi: 10.1212/
WNL.0b013e3181bf995f
Kimpinski, K.l, V. Iodice, P. Sandroni, R. D. Fealey, S.
Vernino, and P A. Low. 2012b. “Sudomotor dysfunction
in autoimmune autonomic ganglionopathy: A follow-
up study.” Clinical Autonomic Research: Official
Journal of the Clinical Autonomic Research Society
22(3):131–36. doi: 10.1007/s10286-011-0152-4
Kucera, P., Z. Goldenberg, and E. Kurca. 2004.
“Sympathetic skin response: Review of the method
and its clinical use.” Bratislavske Lekarske Listy
105(3):108–16.
Lipp, A., P. Sandroni, J. E. Ahlskog, et al. 2009.
“Prospective differentiation of multiple system atrophy from Parkinson disease, with and without autonomic failure.” Archives of Neurology 66(6):742–50.
doi: 10.1001/archneurol.2009.71
Low, P. A. 1997. “The effects of ageing on the autonomic
nervous system.” In Clinical autonomic disorders,
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
38 Thermoregulatory Sweat Test
2nd ed., edited by P. A. Low, 161–175. Philadelphia,
PA: Lippincott-Raven Publishers.
Low, P. A., P. E. Caskey, R. R. Tuck, R. D. Fealey, and
P. J. Dyck. 1983. “Quantitative sudomotor axon
reflex test in normal and neuropathic subjects.”
Annals of Neurology 14(5):573–
80. doi: 10.1002/
ana.410140513
Low, P. A., P. J. Dyck, H. Okazaki, R. Kyle, and R.
D. Fealey. 1981. “The splanchnic autonomic outflow in
amyloid neuropathy and Tangier disease.” Neurology
31(4):461–63.
Low, P. A., R. D. Fealey, S. G. Sheps, W. P. Su, J.
C. Trautmann, and N. L. Kuntz. 1985. “Chronic idiopathic anhidrosis.” Annals of Neurology 18(3):344–48.
doi: 10.1002/ana.410180312
Low, P. A., and R. D. Fealey. 1999. “Sudomotor neuropathy.” In Diabetic neuropathy, edited by Dyck, P. J. and
Thomas, P. K. Philadelphia: W.B. Saunders Company.
Chapter 13: 191–199.
Low, P. A., H. Okazaki, and P. J. Dyck. 1977. “Splanchnic preganglionic neurons in man. 1. Morphometry of preganglionic cytons.” Acta Neuropathologica (Berlin) 40:55–61.
Low, V. A., P. Sandroni, R. D. Fealey, and P. A. Low. 2006.
“Detection of small-fiber neuropathy by sudomotor
testing.” Muscle and Nerve 34(1):57–61. doi: 10.1002/
mus.20551
McCaffrey, T. V., R. D. Wurster, H. K. Jacobs, D. E. Euler,
and G. S. Geis. 1979. “Role of skin temperature
in the control of sweating.” Journal of Applied
Physiology: Respiratory, Environmental, and Exercise
Physiology 47(3):591–97.
Morgan, C. J., P. S. Friedmann, M. K. Church, and G.
F. Clough. 2006. “Cutaneous microdialysis as a novel
means of continuously stimulating eccrine sweat glands
in vivo.” The Journal of Investigative Dermatology
126(6):1220–25. doi: 10.1038/sj.jid.5700197
Nakazato, Y., N. Tamura, A. Ohkuma, K. Yoshimaru, and
K. Shimazu. 2004. “Idiopathic pure sudomotor failure: Anhidrosis due to deficits in cholinergic transmission.” Neurology 63(8):1476–80.
Nolano, M., V. Provitera, A. Perretti, et al. 2006. “Ross
syndrome: A rare or a misknown disorder of thermoregulation? A skin innervation study on 12 subjects.”
657
Brain: A Journal of Neurology 129(Pt 8):2119–
31.
doi: 10.1093/brain/awl175
Ross, A. T. 1958. “Progressive selective sudomotor denervation; a case with coexisting Adie’s syndrome.”
Neurology 8(11):809–17.
Sandroni, P., J. E. Ahlskog, R. D. Fealey, and P. A. Low.
1991. “Autonomic involvement in extrapyramidal and
cerebellar disorders.” Clinical Autonomic Research:
Official Journal of the Clinical Autonomic Research
Society 1(2):147–55.
Sato, K., and F. Sato. 1983. “Individual variations in structure and function of human eccrine sweat gland.” The
American Journal of Physiology 245(2):R203–08.
Sato, K. T., A. Richardson, D. E. Timm, and K. Sato. 1988.
“One-step iodine starch method for direct visualization of sweating.” The American Journal of the Medical
Sciences 295(6):528–31.
Schneider, C. A., W. S. Rasband, and K. W. Eliceiri. 2012.
“NIH Image to ImageJ: 25 years of image analysis.”
Nature Methods 9(7):671–75.
Sletten, D. M., S. D. Weigand, and P. A. Low. 2010.
“Relationship of Q-sweat to quantitative sudomotor
axon reflex test (QSART) volumes.” Muscle and Nerve
41(2):240–46. doi: 10.1002/mus.21464
Stewart, J. D., P. A. Low, and R. D. Fealey. 1992. “Distal
small fiber neuropathy: Results of tests of sweating and
autonomic cardiovascular reflexes.” Muscle and Nerve
15(6):661–65. doi: 10.1002/mus.880150605
Vernino, S., J. Adamski, T. J. Kryzer, R. D. Fealey, and
V. A. Lennon. 1998. “Neuronal nicotinic ACh receptor antibody in subacute autonomic neuropathy and
cancer-related syndromes.” Neurology 50(6):1806–13.
Vernino, S., P. A. Low, R. D. Fealey, J. D. Stewart, G.
Farrugia, and V. A. Lennon. 2000. “Autoantibodies
to ganglionic acetylcholine receptors in autoimmune autonomic neuropathies.” The New England
Journal of Medicine 343(12):847–
55. doi: 10.1056/
NEJM200009213431204
Wang, A. K., R. D. Fealey, T. L. Gehrking, and P.
A. Low. 2008. “Patterns of neuropathy and autonomic failure in patients with amyloidosis.” Mayo
Clinic Proceedings 83(11):1226–
30. doi: 10.4065/
83.11.1226
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Chapter 39
Cardiovagal Reflexes
William P. Cheshire, Jr.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
INTRODUCTION
HEART RATE RESPONSE TO DEEP
BREATHING
Physiological Basis
Technique
Methods of Analysis
Reproducibility
Factors Affecting the Heart Rate Response
to Deep Breathing
Problems and Controversies
THE VALSALVA MANEUVER
Normal Response and Physiological Basis
INTRODUCTION
Vagal nerve traffic cannot be recorded directly
in humans. Reliable, reproducible measurement of vagal function is possible indirectly,
however, through noninvasive tests of heart
rate variability. The clinical relevance of heart
rate variability in evaluating autonomic function was first recognized in obstetrics as a
marker of fetal distress (Hon and Lee 1965).
Although the physiological basis of heart rate
Technique
The Valsalva Ratio
Vagal Baroreflex Sensitivity
Factors Affecting the Valsalva Response
Pitfalls of the Valsalva Maneuver
CARDIOVAGAL SCORING
POWER SPECTRUM ANALYSIS
HEART RATE RESPONSE TO STANDING
OTHER TESTS OF CARDIOVAGAL
FUNCTION
SUMMARY
variability has been known for a long time,
it has been mainly in the last three decades
that cardiovascular heart rate tests have been
applied clinically, thanks to the enthusiastic
promotion by Ewing and associates (Ewing
et al. 1985). Clinical tests of cardiovagal function are now widely used, although the full
range of their application as well as their limitations remain underappreciated (van Lieshout
et al. 1989b; Wieling and van Lieshout 1990;
Low and Sletten 2008; Spallone et al. 2011).
658
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
39 Cardiovagal Reflexes
Divergent views exist regarding what types
of clinical studies constitute an adequate battery of tests of autonomic function and what are
the optimal conditions for testing (Ewing et al.
1985; Freeman 2008). Nevertheless, an expert
consensus has formed in regard to reasonable
parameters for a number of basic methodologies for the evaluation of cardiovagal function
that provide sensitive and reproducible results
(Freeman 2008; Low 2003; Freeman 2006;
Gibbons, Cheshire, and Fife 2014). The most
reproducible tests of cardiovagal function are
those that are performed under standardized
conditions and evaluate heart rate changes in
response to inspiration and expiration, to the
Valsalva maneuver, or to standing (Spallone
et al. 2011; Tannus et al. 2013). The following
description focuses on the most useful tests of
cardiovagal function. Their underlying physiology, methodology, clinical utility, and shortcomings are described.
HEART RATE RESPONSE
TO DEEP BREATHING
The heart rate response to deep breathing
(Figure 39–
1) is probably the most reliable
of the cardiovascular heart rate tests, because
the major afferent and efferent pathways are
both vagal (Katona and Jih 1975). The vagus
nerve provides a beat-to-beat control of the
sinus node (Jalife and Michaels 1994). This
is mediated by M2-type muscarinic cholinergic receptors coupled to G-protein-activated
inward rectifying potassium channels (GIRKs).
In humans, muscarinic receptor blockade with
atropine completely abolishes respiratory sinus
arrhythmia.
The primary basis of respiratory sinus
arrhythmia appears to be the interactions
between the respiratory centers and the cardioinhibitory centers in the medulla, particularly
the nucleus ambiguus (Spyer 1999). Evidence
for this is cessation of vagal efferent activity during the inspiratory phase of natural—but not
artificial—ventilation, and the loss of respiratory
sinus arrhythmia in some patients with brain
stem lesions (Vallbona et al. 1965). Respiratory
sinus arrhythmia is modulated by input from the
lungs, heart, and baroreceptors (Saul and Cohen
1994). Pulmonary stretch receptors that mediate the Hering–Breuer respiratory reflex modulate respiratory sinus arrhythmia, although their
role may be less important in humans than in
experimental animals. Receptors from the right
atrium initiate the vagally-mediated Bainbridge
reflex and a venoatrial mechanoreceptor sympathetic reflex (Spyer 1999). Baroreflex sensitivity
changes throughout deep breathing, thus modulating respiratory sinus arrhythmia (Eckberg,
Kifle, and Roberts 1980).
Technique
For testing the heart rate response to deep
breathing, care should be taken to ensure that
the patient is relaxed and comfortable, because
250
mm Hg, mVolts ×50
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Physiological Basis
659
200
150
100
50
0
01:20 01:21 01:22 01:23 01:24 01:25 01:26 01:27 01:28 01:29 01:30 01:31 01:32 01:33 01:34 01:35 01:36 01:37
Figure 39–1. Heart rate response to deep breathing in a normal subject. Chest wall expansion during deep breathing is
represented by the slow sinusoidal waveform, and above it is displayed a single-lead electrocardiogram (EKG) tracing. The
heart rate, which is the inverse of the EKG R–R intervals, normally increases during inspiration and then decreases during
expiration.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
660
Section 5: Assessment of Autonomic Function
sympathetic activation diminishes the response.
Medications known to inhibit respiratory sinus
arrhythmia should be withheld if it is practical
and safe to do so. The patient is tested in the
supine position to maximize vagal tone.
Either of two methods of training the respiratory cycle is customarily used. The more
common method is to have the subject follow
and breathe in timing with a visual cue, such
as a sinusoidal oscillating bar generated by
a computer. The alternative is to instruct the
subject to breathe in and out as the technician
gestures. The difference of the two approaches
has not been studied systematically but is likely
to be minor. What is most important is that the
patient breathe slowly and continuously, rather
than gasping or pausing, with full breaths, and
at a consistent rate of 5–6 cycles per minute.
A standardized deep-breathing protocol can be
used without the need to factor in variations in
the depth of respiration. This is because depth
of breathing above a tidal volume of approximately 1.2 L causes insignificant changes in
the heart rate response to deep breathing
(Freyschuss and Melcher 1975). Bennett and
associates and Eckberg found little or no difference in the response for different depths of respiration (Bennett et al. 1977; Eckberg 1983).
The electrocardiogram (ECG) is continuously monitored. A computer program captures
each QRS complex over time and displays beat-
to-
beat heart rate. Most laboratories record
the mean difference in R–R intervals over a
series of six respiratory cycles. Some investigators have advocated measuring the heart rate
response to one breath on the basis that a single deep breath is a more potent stimulus for
heart rate change than repeated deep breaths
(O’Brien et al. 1986; Bennett et al. 1978).
Direct comparisons have shown no advantage
of a single deep breath over repeated breaths
(Espi, Ewing, and Clarke 1982). Rather, assessments of heart rate responses to a series of
breaths are more likely to be reproducible.
Methods of Analysis
The three methods of analysis generally used
are the heart rate range, the heart period range,
and the E:I ratio (Vallbona et al. 1965). The E:I
ratio is the ratio of the shortest R–R interval
during inspiration to the longest R–R interval
during expiration. Our laboratory utilizes the
heart rate range, because the effect of resting
heart rate on the range is smaller than its effect
on heart period (Figure 39–2).
Weinberg and Pfeifer recommended calculation of the circular mean resultant, a
method based on vector analysis, to eliminate
the effects of trends in heart rate over time
and to attenuate the effect of basal heart rate
and ectopic beats in the calculated variability of heart rate (Weinberg and Pfeifer 1984;
Genovely and Pfeifer 1988). In this method,
R–R intervals over a five-minute interval are
plotted on a circular graph in which one revolution corresponds to a single respiratory cycle.
Normal heart rate variability results in a clustering of time events, whereas reduced heart
rate variability results in less periodically distributed time events on the circle.
Reproducibility
Tests of heart rate response to deep breathing have been reproducible with typical coefficients of variation 11% and 8.9% (Bennett
et al. 1977; Smith 1982). When combined with
a second, independent test of the parasympathetic control of heart rate, the results are
highly reliable in the diagnosis of cardiovagal
dysfunction (Wieling 1983).
Factors Affecting the Heart Rate
Response to Deep Breathing
Numerous factors affect the heart rate response
to deep breathing. From the standpoint of
clinical autonomic testing, the most important
of these are the effects of age and the rate of
forced respiration. A progressive decrease
in the response with increasing age has been
reported in all large studies (Ewing et al. 1985;
O’Brien, O’Hare, and Corrall 1986; Bergstrom
et al. 1986; Ingall 1986; Kaijser and Sachs
1985; Masaoka et al. 1985; Wieling et al. 1982;
Clark and Mapstone 1986; Low et al. 1990;
Low et al. 1997). An investigation of 557 normal subjects, evenly distributed by age and sex
from 10–83 years old, found that the decline
in heart rate responses to deep breathing with
age did not regress to zero but leveled off in the
older subjects, indicating that it is possible to
diagnose cardiovagal failure in elderly patients
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
39 Cardiovagal Reflexes
Normal deep breathing
200
180
180
SBP
140
mm Hg
120
100
160
MBP
140
DBP
120
80
60
40
100
HR
Beats/minute
160
661
80
60
20
40
0
Time
Abnormal deep breathing
200
200
SBP
120
80
160
MBP
DBP
120
HR
Beats/minute
mm Hg
160
80
40
40
0
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Time
Figure 39–2. Heart rate response to deep breathing in a normal subject (top) and in a patient with diabetic autonomic
neuropathy (bottom). In each panel, the three upper tracings correspond to systolic blood pressure (SBP), mean blood pressure (MBP), and diastolic blood pressure (DBP). The bottom tracing corresponds to heart rate (HR).
by comparison to normative data (Table 39–1)
(Low et al. 1997).
Maximal heart rate response to deep
breathing occurs at a breathing frequency of
5–
6 respirations per minute in normal subjects (Saul and Cohen 1994; Bennett et al.
1977; Angelone and Coulter 1964; Pfeifer et al.
1982). This observation defines the basis for
Table 39–1 Normative Data for Heart Rate Variability
to Deep Breathing
Percentile
20 years
40 years
60 years
2.5
5.0
95.0
97.5
13
14
41
43
9
10
33
36
7
7
27
29
80 years
7
7
27
29
Normative data were obtained from 376 subjects aged 10–83 and were derived by plotting
the regression of heart rate variation in beats/minute against age in years. A significant (p <
0.001) difference was found in which y = 37.5448 ′ log 10 0.9832x. Breakdown by sex was
approximately equal (Low et al. 1997).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
662
Section 5: Assessment of Autonomic Function
the standard test of deep breathing (Freeman
2008). In patients with vagal neuropathy, the
maximal heart rate response to deep breathing
occurs at lower respiratory frequencies, which
is of little pragmatic concern. Of greater practical importance is the selection for each subject of a respiratory rate in which the neural
contributions that increase and decrease the
heart rate in this composite reflex are additive
instead of subtractive (Angelone and Coulter
1964). A clue to waveform cancelation is the
observation of a large first or second response,
followed by smaller responses.
The position of the subject has some effect
on respiratory sinus arrhythmia. The response
is larger when the subject is supine than when
sitting or erect (Bennett et al. 1977). Unlike
some other tests of autonomic function, the
heart rate response to deep breathing is not
greatly affected by the sex of the subject (Low
et al. 1990; Low et al. 1997). The duration of
antecedent rest is not important in relaxed subjects. After five minutes of rest, another 25 minutes of supine rest will not alter the response.
No significant differences have been found in
the response whether the test is performed in
the morning or in the afternoon in the same
subjects (Bennett et al. 1977). A number of
studies have correlated cardiovagal control
to depression, but the overall variance is only
about 2% (Rottenberg 2007).
Prolonged hyperventilation and the reduction of partial pressure of carbon dioxide
(PaCO2), however, result in a depression in
respiratory sinus arrhythmia. There is a sympathetic modulation of the heart rate response
to deep breathing that is inhibited by mental
stress and enhanced by β-adrenergic blockade
(Coker et al. 1984; Pitzalis et al. 1998; Elghozi
and Julien 2007; Overbeek, van Boxtel, and
Westerink 2014). Also, the response is impaired
in obesity, during severe tachycardia, in heart
failure, during sleep in patients with upper
airway obstruction, and in deeply unconscious
patients (Vallbona et al. 1965; Pfeifer et al.
1982; Coker et al. 1984; Tonhajzerova et al.
2008; Kabir et al. 2013). Medications that have
been shown to reduce the heart rate response to
deep breathing include muscarinic antagonists,
nicotine, opioids, and norepinephrine reuptake
and serotonin-
selective reuptake inhibitors
(SSRIs) (Lacroix et al. 1992; Wang et al. 2003;
Loula, Jantti, and Yli-Hankala 1997; Davidson
et al. 2005; Low and Opfer-Gehrking 1992).
Problems and Controversies
The heart rate response to deep breathing is
an indirect measure of cardiovagal function.
A reduced response indicates a lesion anywhere in the intricate autonomic nervous system; that is, in the afferent, central processing
unit, efferent, synapse, or effector apparatus.
To further complicate interpretation, a
reduced response does not unequivocally indicate cardiovagal failure. The general observation that heart rate usually increases during
inspiration and decreases during expiration is
an approximation of a composite set of phenomena. Both inspiration and expiration are
followed by an increase, then a decrease, in
heart rate but at a different rate of change,
amplitude, time of appearance, and duration.
Mehlsen and colleagues suggested that the
reason the maximal heart rate range in many
subjects is six beats per minute is because
they have well-defined heart rate maxima with
positive interference of phases (Mehlsen et al.
1987). The reason subjects have a decreased
heart rate range less than seven beats per minute can be because of negative interference.
THE VALSALVA MANEUVER
The Valsalva maneuver is a global test of reflex
cardiovascular responses. It consists of an abrupt
transient increase in intrathoracic and intra-
abdominal pressures induced by blowing against
pneumatic resistance while maintaining a predetermined pressure (straining) (Booth et al. 1962;
Brooker, Alderman, and Harrison 1974; Sharpey-
Schafer 1955; Nishimura and Tajik 1986).
Normal Response
and Physiological Basis
Intra-
arterial recordings of arterial pressure
and, more recently, noninvasive monitoring
of arterial pressure with a photoplethysmographic technique (Finapres or Finometer)
or tonometry (Colin Pilot or Colin 7000) have
provided important information about the
hemodynamic changes during the Valsalva
maneuver in normal and pathological conditions (Benarroch, Opfer-
Gehrking, and Low
1991; Imholz et al. 1988).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
39 Cardiovagal Reflexes
after administration of α1-adrenergic blocking
drugs (Korner, Tonkin, and Uther 1976). The
slowing of the heart rate is reflexive and mediated by increased parasympathetic efferent
activity (Eckberg 1980).
Phase II consists of a decrease (early phase
II: IIe) and subsequent partial recovery (late
phase II: IIl) of arterial pressure and continuous increase of heart rate during straining.
Continuous straining impedes venous return
to the heart, which is the true stimulus for
the autonomic responses that are to be measured. The increase in intrathoracic pressure
displaces large volumes of blood from the thorax and abdomen to the limbs. The decrease
in venous return reduces left atrial and left
The responses to the Valsalva maneuver have
been divided into four phases (Figure 39–3)
(Booth et al. 1962; Brooker, Alderman,
and Harrison 1974; Sharpey-
Schafer 1955;
Nishimura and Tajik 1986; Benarroch, Opfer-
Gehrking, and Low 1991; Imholz et al. 1988;
Korner, Tonkin, and Uther 1976). Phase I consists of a brisk increase in systolic and diastolic
arterial pressure and a decrease in heart rate
immediately after the onset of the Valsalva
strain and lasts approximately four seconds.
The increase in arterial pressure during phase
I reflects mechanical factors and is not associated with an increase in sympathetic activity.
It persists in patients with transections of the
high cervical spinal cord and in normal subjects
Normal Valsalva maneuver
IV
180
mm Hg
140
I
SBP
160
III
120
100
80
60
80
HR
60
40
EP
20
40
20
Time
Abnormal Valsalva maneuver
180
mm Hg
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
0
160
140
120
II
100
180
SBP
240
220
140
200
120
180
100
160
80
140
60
120
40
20
0
Beats/minute
160
200
Beats/minute
200
663
100
HR
80
EP
Time
60
Figure 39–3. Changes in systolic blood pressure (SBP) and heart rate (HR) during the Valsalva maneuver in a normal
subject (top) and in a patient with diabetic autonomic failure (bottom). The normal beat-to-beat SBP recording shows the
typical four phases (I, II, III, IV) of the Valsalva maneuver. The abnormal Valsalva maneuver is characterized by a profound
decrease in SBP in early phase II, absence of recovery in late phase II, delay in SBP recovery, and absence of SBP overshoot
in phase IV. Note the attenuated HR responses during phases I and IV, resulting in a reduced Valsalva ratio. EP, expiratory
pressure.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
664
Section 5: Assessment of Autonomic Function
ventricular dimensions, left ventricular stroke
volume, and cardiac output (Booth et al. 1962;
Brooker, Alderman, and Harrison 1974).
This triggers reflex compensatory tachycardia
and vasoconstriction. The tachycardia during
phase II results from a prominent, early component of inhibition of cardiovagal output and
is abolished with muscarinic blockade with
atropine (Leon, Shaver, and Leonard 1970).
There is also a late contribution of increased
sympathetic cardioacceleratory output that
is blocked with propranolol. The progressive
recovery of arterial pressure during phase
II reflects a similarly progressive increase
in total peripheral resistance caused by
increased sympathetic vasoconstrictor activity (Sharpey-Schafer 1955; Delius et al. 1972;
Wallin and Eckberg 1982). Increased arterial
pressure during late phase II is abolished by
α1-
adrenergic blockade with phentolamine.
The fall in blood pressure during phase II is
more pronounced if compensatory tachycardia is prevented by atropine and propranolol
and if vasoconstriction is prevented by α1-
adrenergic blockade (Sandroni, Benarroch,
and Low 1991).
Phase III consists of a sudden, brief (1–2
seconds) further decrease in arterial pressure
and increase in heart rate immediately after the
release of the straining. It is essentially mechanical in nature and is the inverse of phase I.
Phase IV is characterized by increased systolic and diastolic arterial pressure above control levels, termed overshoot, accompanied
by bradycardia relative to the control level of
heart rate. In phase IV, venous return to the
heart, left ventricular stroke volume, and cardiac output return nearly to baseline, whereas
the arteriolar bed remains vasoconstricted
because of the long time constant of sympathetic responses (Korner, Tonkin, and Uther
1976). This combination results in an overshoot of arterial pressure above baseline values. Post-straining arterial pressure increases
are proportional to the preceding increases
in sympathetic nerve activity. The increase in
arterial pressure during phase IV can be prevented by β-
adrenergic blockade (Sandroni,
Benarroch, and Low 1991). Increases in both
cardiac output and total peripheral resistance
are important in producing the increase in
arterial pressure in phase IV.
Pharmacological evidence indicates that
an increase in cardiac output-
mediated
cardioacceleration is more important than vasoconstriction in producing arterial pressure overshoot in phase IV. This overshoot is abolished by
β-blockade with propranolol but is maintained
or even exaggerated during α-adrenergic blockade with phentolamine (Brooker, Alderman,
and Harrison 1974). The increase in arterial
pressure during phase IV stimulates the baroreceptors and results in reflex bradycardia caused
by increased parasympathetic activity, which is
abolished with atropine (Eckberg 1980; Levin
1966). Sympathetic inhibition after straining
persists much longer than the increase in arterial pressure.
The responses during the four phases of
the Valsalva maneuver depend on the variable relationships between carotid and aortic baroreceptor inputs. Pressure transients
lasting only seconds may reset the relationships between the arterial pressure and the
sympathetic or vagal responses (Smith et al.
1996). Examples of the Valsalva maneuvers
in a normal subject and subjects with mild
and severe autonomic failure are shown in
Figure 39–4.
Technique
For testing the responses to the Valsalva
maneuver, care should be taken, as in any other
autonomic test, to ensure that the patient is well
hydrated and is not taking medications known
to affect blood volume, cholinergic function,
or vasoreactivity (unless it would be medically
unsafe to withhold such medications). At our
institution, subjects are tested in the supine
position and asked to maintain a column of
mercury at 40 mm Hg for 15 seconds by blowing through a bugle with an air leak (to ensure
an open glottis). The responses are obtained in
triplicate, and the largest response is accepted
(Benarroch, Opfer-Gehrking, and Low 1991;
Sandroni, Benarroch, and Low 1991; Denq,
O’Brien, and Low 1998). In some laboratories,
only heart rate is monitored continuously, so
that it may not be possible to know with certainty whether a decreased Valsalva response
reflects autonomic failure or an inadequate
stimulus. Our laboratory and many others also
monitor beat-to-beat arterial pressure with a
noninvasive photoplethysmographic technique
(Benarroch, Opfer-Gehrking, and Low 1991;
Sandroni, Benarroch, and Low 1991; Denq,
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
39 Cardiovagal Reflexes
665
SBP
DBP
HR
A
B
C
Figure 39–4. Valsalva maneuvers in three different subjects showing beat-to-beat blood pressure (BP) and heart rate
(HR) in (A) a normal response, (B) impaired late phase II response and decreased Valsalva ratio in mild autonomic failure,
and (C) absent late phase II, absent phase IV, and absent HR response in severe autonomic failure.
O’Brien, and Low 1998; Parati et al. 1989;
Ten Harkel et al. 1990). The “normal” Valsalva
response should be defined according to the
technique used in each laboratory, because
several technical variables affect the magnitude of the response.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
The Valsalva Ratio
The Valsalva ratio is defined as the longest R–R
interval (pulse interval, in milliseconds) within
30 seconds after the maneuver (in phase IV)
divided by the shortest R–R interval during the
maneuver (in phase II). In clinical settings, the
Valsalva maneuver commonly has been used to
calculate the Valsalva ratio. The best of three
responses is accepted. In more than 96% of
control subjects, this ratio exceeds 1.5 (Bennett
et al. 1977; Pfeifer et al. 1982; Eckberg 1980;
Leon, Shaver, and Leonard 1970; Levin 1966).
The Valsalva ratio decreases significantly with
age (Low et al. 1990).
Vagal Baroreflex Sensitivity
The relationships between arterial pressure
and heart rate during phase II and phase IV of
the maneuver have been used to assess baroreflex sensitivity (Kautzner et al. 1996). Vagal
baroreflex sensitivity, which is the change in
heart rate resulting from a change in blood
pressure, can be quantified by plotting each
heart interval against the preceding systolic
blood pressure value. The slope of the simple
linear regression is a measure of baroreflex
sensitivity (Trimarco et al. 1983). One limitation of this method is that there is an unknown
reflex latency between the pressure change
and the change in heart period. Thus, the best
of two regression slopes, one correlating blood
pressure to its corresponding heart period
and the other to its subsequent pulse interval,
should be accepted. Vagal baroreflex sensitivity declines with age (Huang et al. 2007). The
adrenergic component of baroreflex sensitivity,
which relates the blood pressure recovery time
to the preceding decrease in blood pressure,
correlates more closely than vagal baroreflex
sensitivity to adrenergic failure (Schrezenmaier
et al. 2007).
Factors Affecting
the Valsalva Response
The cardiovascular changes during the
Valsalva maneuver are determined mainly
by the magnitude of hemodynamic change
during the forced expiratory effort, the time
course and efficiency of reflex cardiovagal
and sympathetic vasomotor and cardiomotor responses, and the modification of these
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
666
Section 5: Assessment of Autonomic Function
responses by interactions with respiratory
mechanisms at both central and peripheral
levels. Accordingly, the responses to the
Valsalva maneuver may be affected by (1) the
position of the subject during the maneuver;
(2) the magnitude and duration of the straining; (3) the breathing pattern before and after
the maneuver, including depth and phase of
respiration preceding the straining; and (4)
the control of respiration after release of the
straining. Normative data on the phases of
the Valsalva maneuver have been published
(Table 39–2) (Low et al. 1997; Denq, O’Brien,
and Low 1998; Faulkner, Hathaway, and
Tolley 2003).
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
EFFECTS OF POSTURE
In subjects in the supine position, changes
in arterial pressure during phases II and IV
may be modest, because the large intrathoracic blood volume may buffer the reduced
venous return during phase II. In the supine
position, some normal subjects may show
a square-
wave response similar to that
of patients with congestive heart failure.
Changing from a supine to an inclined or
upright posture increases the magnitudes of
the arterial pressure decrease during phase
II, the systolic blood pressure overshoot
during phase IV, and the Valsalva ratio (Ten
Harkel et al. 1990). In our laboratory, when
a square-wave response is encountered, the
Valsalva maneuver is repeated after inclining
the table to 30°.
EFFECTS OF TEST DURATION
The duration of straining during the Valsalva
maneuver differentially affects the vagally and
sympathetically mediated responses because
of their differing latencies and time constants.
When the Valsalva maneuver is performed
at low expiratory pressures (20 mm Hg), the
magnitude of the tachycardia in phase II is
independent of the duration of the test, consistent with the short latency of vagal responses.
The maximal increase in arterial pressure in
late phase II and phase IV correlates with the
duration of the Valsalva maneuver. This may
reflect the longer latency of sympathetic vasoconstrictor and cardioacceleratory responses
(Korner, Tonkin, and Uther 1976). A test
duration of 10 seconds is effective, while 15
seconds is a practical optimum and may be
sufficient to assess sympathetically mediated responses in a clinical setting (Khurana,
Mittal, and Dubin 2011; Benarroch, Opfer-
Gehrking, and Low 1991).
EFFECTS OF EXPIRATORY PRESSURE
The magnitude of most heart rate and arterial pressure responses during phase II and
phase IV correlates with the magnitude of
expiratory pressure used during the Valsalva
maneuver. Maximal arterial pressure and heart
rate responses are obtained with expiratory
pressures of 40–50 mm Hg (Nishimura and
Tajik 1986; Eckberg 1980; Leon, Shaver, and
Leonard 1970; Levin 1966).
PHASE OF RESPIRATION
In normal subjects, the magnitude of heart rate
responses during the Valsalva maneuver is significantly lower if the expiratory strain is preceded by maximal inspiration instead of tidal
inspiration (Eckberg 1980).
Table 39–2 Normative Data for the Valsalva Ratio
Percentile
2.5
5.0
95.0
97.5
20 years
40 years
60 years
80 years
M
F
M
F
M
F
M
F
1.50
1.59
2.87
2.97
1.41
1.46
2.73
2.97
1.36
1.44
2.52
2.60
1.47
1.51
2.64
2.88
1.21
1.29
2.18
2.23
1.36
1.39
2.41
2.65
1.21
1.29
2.18
2.23
1.36
1.39
2.41
2.65
Normative data were obtained by plotting the regression of Valsalva ratio against age in 425 subjects of 10–83 years
(Low et al. 1997).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
39 Cardiovagal Reflexes
Pitfalls of the Valsalva Maneuver
PITFALLS IN PERFORMING THE
VALSALVA MANEUVER
There are several precautions to keep in mind
when asking patients to perform the Valsalva
maneuver (Nishimura and Tajik 1986):
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
1. The test requires patient cooperation and,
thus, cannot be performed in patients who
are seriously ill or who have weak respiratory, facial, or oropharyngeal muscles.
2. The maneuver should be avoided in patients
with proliferative retinopathy, because of
the risk of intraocular hemorrhage, and in
patients with known cerebral aneurysms,
because of the theoretical risk of subarachnoid hemorrhage.
3. Theoretically, the Valsalva maneuver can
precipitate arrhythmias and angina and may
cause syncope, particularly in elderly patients
with impaired reflex mechanisms that
respond to the decrease in venous return.
4. Patients with congestive heart failure, mitral
stenosis, aortic stenosis, constrictive pericarditis, or atrial septal defect may have an
abnormal square-wave response of arterial
pressure to the Valsalva maneuver because
of the increase in pulmonary blood volume,
which is capable of maintaining ventricular
filling during the Valsalva strain.
PITFALLS IN INTERPRETING
THE VALSALVA RATIO
There is evidence that the Valsalva ratio in
normal subjects depends mainly on cardiovagal function (Pfeifer et al. 1982; Eckberg 1980;
Leon, Shaver, and Leonard 1970; Levin 1966).
However, the interpretation of this ratio as a
test of cardiovagal function without simultaneous recordings of arterial pressure may be misleading for several reasons:
1. The Valsalva ratio correlates better with the
heart rate response in phase II than with the
response in phase IV (Benarroch, Opfer-
Gehrking, and Low 1991). Therefore, if sufficient tachycardia is present in phase II, the
Valsalva ratio may be “normal” even in the
absence of significant bradycardia in phase IV.
This may occur in patients with cardiovagal
667
impairment but intact sympathetic innervation (Opfer-Gehrking and Low 1993).
2. The Valsalva ratio also correlates with the
magnitude of arterial pressure overshoot
in phase IV (Benarroch, Opfer-Gehrking,
and Low 1991). The absence of bradycardia
in phase IV, and thus an abnormal Valsalva
ratio, may be caused not only by vagal dysfunction but also by the inability to increase
arterial pressure in phase IV.
3. Both the heart rate increase in phase II and the
heart rate decrease in phase IV are affected
critically by the magnitude of the decrease in
venous return during the Valsalva maneuver,
which depends on the position of the subject
and the pooling and buffering effect of thoracic vessels (Ten Harkel et al. 1990).
4. Assessing the integrity of the total baroreflex arc during the Valsalva maneuver by
only testing the Valsalva ratio is unreliable,
because the magnitude and time course
of the heart rate response may be normal
despite a response of arterial pressure typical of sympathetic failure (Opfer-Gehrking
and Low 1993).
The integrity of reflex sympathetic responses
cannot be inferred on the basis of the Valsalva
ratio. Both the magnitude of the decrease in
mean arterial pressure in phase II and the
overshoot of arterial pressure in phase IV have
been considered indices of vasomotor function
(Korner, Tonkin, and Uther 1976; Sandroni,
Benarroch, and Low 1991). However, the magnitude of the decrease in arterial pressure in
early phase II is also affected by the heart rate
responses, and the overshoot of arterial pressure in phase IV may be more dependent on
cardiac output. In our laboratory, the changes
in arterial pressure during early and late phase
II and phase IV are used to assess sympathetic
vasomotor function (Sandroni, Benarroch, and
Low 1991; Denq, O’Brien, and Low 1998).
Late phase II is impaired in patients with α-
adrenergic failure caused, for example, by
dopamine-β-hydroxylase deficiency (Biaggioni
et al. 1990; Cheshire et al. 2006).
CARDIOVAGAL SCORING
Low and associates have developed and validated a 10-point composite autonomic severity
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
668
Section 5: Assessment of Autonomic Function
score (CASS), which grades autonomic failure
according to the results of clinical autonomic
testing while correcting for the confounding
effects of age and sex. In addition to adrenergic
(maximum 4 points) and sudomotor (maximum
3 points) subscores, a cardiovagal subscore
(maximum 3 points) is assigned. A subscore
of 1 is assigned if heart rate variability to deep
breathing is mildly reduced but above 50% of
the minimum value. A subscore of 2 is assigned
if heart rate variability is below 50% of the
minimum value. A subscore of 3 indicates that
both the heart rate variability to deep breathing and the Valsalva ratio are reduced to below
50% of their minimum normative values (Low
and Sletten 2008).
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
POWER SPECTRUM ANALYSIS
Autonomic data generally are evaluated in
the time domain, with a focus on the changes
over time in the amplitude of a response to a
standardized stimulus. Spontaneous oscillations also contain key information. Frequency
analysis focuses on the changes in amplitude
as a function of frequency (Freeman 2008).
In recordings of the heart period (the reciprocal of heart rate), oscillations at the respiratory frequency (typically approximately 0.25
Hz) are determined by parasympathetic function; hence, its power (amplitude) reflects the
proportion of frequencies due to parasympathetic activity. A slower frequency, approximately 0.07–0.1 Hz, reflects the periodicity of
the baroreflex loop. Power at this frequency
reflects both sympathetic and parasympathetic
functions. Similar oscillations occur in blood
pressure recordings.
Several methods are available for evaluating
autonomic signals in the frequency domain.
Fast Fourier transform and autoregressive
models are commonly used. Both of these
require stationarity, a condition that is difficult
to satisfy with changing autonomic signals. An
alternative approach is time frequency analysis,
a method that resolves signals in both the time
and the frequency domains simultaneously.
Head-
up tilt results in attenuation of the
respiratory frequency and augmentation of the
lower frequency. An advantage of frequency
analysis is its ability to evaluate sympathovagal
balance. It can be expressed as the power in
the low frequency in blood pressure (reflecting
pure sympathetic function) over the respiratory frequency in heart period (pure parasympathetic function) (Novak et al. 1996).
For clinical recordings of autonomic signals,
it is essential that respiration be recorded or
paced, because respiration can entrain heart
rate oscillations over a wide range of frequencies (from 0.01 to 0.5 Hz), and if the subject
breathes slowly, respiratory rhythms will
eclipse the lower frequency signals (Novak
et al. 1993). Either an increased tidal volume
at lower respiratory rates or breath-
holding
can interact with spectral power at lower frequencies and greatly bias the estimation of
power. Slowing of respiration can thus lead
to a falsely positive increase in low-frequency
power (Novak et al. 1993). A minimal duration
of recording for valid analysis is at least five
minutes of good-quality recording.
HEART RATE RESPONSE
TO STANDING
The immediate heart rate response to standing can be recorded using an ECG machine.
In normal subjects, tachycardia is maximal at
about the fifteenth beat, and relative bradycardia occurs around the thirtieth beat (Ewing
et al. 1978). The 30:15 ratio (R–R interval at
beat 30/R–R interval at beat 15) has been recommended as an index of cardiovagal function.
Reflex tachycardia is thought to be mediated
by the vagus nerve, because the response is
abolished by atropine but not by propranolol
(Ewing et al. 1978). The heart rate response
to standing attenuates with age (Cybulski and
Niewiadomski 2003).
The hemodynamic response to active standing is trimodal (Borst et al. 1982). There is an
abrupt increase in heart rate that peaks at 3
seconds, a further more gradual tachycardia
that peaks at 12 seconds, and a bradycardia
at 20 seconds. The initial cardioacceleration
is an exercise reflex mediated by muscle contraction, resulting in the sudden inhibition of
vagal tone. The second tachycardia is caused by
further vagal inhibition and by reduced baroreflex activity, which is due to transient hypotension caused by a fall in peripheral vascular
resistance. This transient hypotension appears
to be the result of local, non–autonomically
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
39 Cardiovagal Reflexes
mediated vasodilatation in contracting muscles,
central command, and cholinergic-
mediated
vasodilatation (Wieling et al. 1996; Goodwin,
McCloskey, and Mitchell 1972; Sanders, Mark,
and Ferguson 1989). An overshoot in blood
pressure then evokes baroreflex-mediated bradycardia. The series of autonomic responses to
standing thus not only reflects the integrity of
the cardiovagal system, but also depends on an
intact sympathetic nervous system, local muscle
reflexes, baroreflexes, and central command.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
OTHER TESTS OF CARDIOVAGAL
FUNCTION
Available tests of cardiovagal function are
numerous. In a reversal of testing the heart
rate response to standing, a related test measures the heart rate response to lying down.
Recumbency evokes an immediate, vagally
mediated decrease in the R–R interval that is
maximal at the third or fourth beat. This is followed by a sympathetically mediated increase
in the R–
R interval at the twenty-
fifth–
thirtieth beat (Sanders, Mark, and Ferguson
1989; Bellavere and Ewing 1982; Bellavere
et al. 1987).
The heart rate response to squatting has
been defined in normal subjects in comparison
to its decline in diabetic autonomic neuropathy
(Marfella et al. 1994). In this test, the subject
stands still for three minutes, squats down for
one minute, and then stands up during inspiration. The normal response is vagally mediated lengthening of the R–R interval during
squatting, followed by sympathetically mediated shortening of the R–R interval at standing. The response declines with age (Marfella
et al. 1994).
Coughing, which involves inspiration and
an expiratory effort against a closed glottis,
followed by explosive expiration as the glottis
opens, generates a transient intrathoracic pressure gradient of 25–250 mm Hg. This evokes
a decrease in R–R interval, which is maximal
at 2–3 seconds and returns to resting value in
approximately 12–14 seconds (Wei et al. 1983;
Cardone et al. 1987). The cough-induced cardioacceleration is primarily under cholinergic control, although it is partly related to the
intense contraction of abdominal and expiratory muscles (Cardone et al. 1987). The cough
669
test has been applied to the evaluation of cardiac parasympathetic integrity (Cardone et al.
1990). Comparison to conventional tests of cardiovagal function, such as the standing test and
the Valsalva maneuver, has shown no advantage
to the cough test (van Lieshout et al. 1989a).
The diving reflex is provoked by facial cooling and consists of reflex bradycardia, apnea,
and vasoconstriction. The bradycardia depends
on a trigeminal–
cardiovagal reflex in which
stimulation of the sensory branches of the trigeminal nerve evokes an efferent response in
the motor nucleus of the vagus nerve (Khurana
et al. 1980; Schaller 2004). A practical alternative to facial immersion in cold water (the diving test) is the application of cold compresses
to the face (the cold face test), which avoids
the potential for aspiration (Khurana and
Wu 2006).
Baroreflex sensitivity has also been assessed
by regressing the change in heart period to a
titrated decrease or increase in blood pressure evoked by vasoactive drugs (Kingwell,
McPherson, and Korner 1991; Korner et al.
1974; Korner et al. 1972). Alternatively, baroreflex sensitivity has been estimated by baroslopes generated by negative pressure applied
to the carotid sinus by a finely regulated neck
suction device (Ebert et al. 1984; Kardos
et al. 1995).
SUMMARY
Noninvasive cardiovascular tests are reliable
and reproducible and are widely used to evaluate autonomic function in human subjects.
The heart rate response to deep breathing is
probably the most reliable test for assessing
the integrity of the vagal afferent and efferent
pathways to the heart. This is because respiratory sinus arrhythmia is a relatively pure test
of cardiovagal function, whereas many other
conditions, such as plasma volume, antecedent
rest, and cardiac and peripheral sympathetic
functions, factor into the Valsalva response.
Heart rate variability to deep breathing is usually tested at a breathing frequency of five or six
respirations per minute and decreases linearly
with age. The Valsalva maneuver consists of a
forced expiratory effort against resistance and
produces mechanical (phases I and III) and
reflex (phases II and IV) changes in arterial
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
670
Section 5: Assessment of Autonomic Function
pressure and heart rate. When performed
under continuous arterial pressure monitoring with a noninvasive technique, the Valsalva
maneuver provides valuable information about
the integrity of the cardiac parasympathetic,
cardiac sympathetic, and sympathetic vasomotor outputs. The responses to the Valsalva
maneuver are affected by the position of the
subject and the magnitude and duration of the
expiratory effort. In general, it is performed at
an expiratory pressure of 40 mm Hg sustained
for 15 seconds. The Valsalva ratio, which is the
relationship between the maximal heart rate
response during phase II (straining) and the
minimal heart rate response during phase IV
(after release of straining), has been considered a test of cardiac parasympathetic function. However, without simultaneous recording
of arterial pressure, this may be misleading.
An exaggerated decrease in arterial pressure
during phase II suggests sympathetic vasomotor failure, whereas a delay in recovery or an
absence of overshoot during phase IV indicates
the inability to increase cardiac output and cardiac adrenergic failure.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
REFERENCES
Angelone, A., and N. A. Coulter, Jr. 1964. “Respiratory
sinus arrhythmia: A frequency dependent phenomenon.” Journal of Applied Physiology 19:479–82.
Bellavere, F., and D. J. Ewing. 1982. “Autonomic control
of the immediate heart rate response to lying down.”
Clinical Science 62:57–64.
Bellavere, F., C. Cardone, M. Ferri, et al. 1987. “Standing
to lying heart rate variation. A new simple test in the
diagnosis of diabetic autonomic neuropathy.” Diabetic
Medicine 4:41–43.
Benarroch, E. E., T. L. Opfer-Gehrking, and P. A. Low.
1991. “Use of the photoplethysmographic technique
to analyze the Valsalva maneuver in normal man.”
Muscle and Nerve 14:1165–72.
Bennett, T., I. K. Farquhar, D. J. Hosking, and J.
R. Hampton. 1978. “Assessment of methods for estimating autonomic nervous control of the heart in
patients with diabetes mellitus.” Diabetes 27:1167–74.
Bennett, T., P. H. Fentem, D. Fitton, J. R. Hamptom,
D. J. Hosking, and P. A. Riggott. 1977. “Assessment
of vagal control of the heart in diabetes. Measures of
R–
R interval variation under different conditions.”
British Heart Journal 39:25–28.
Bergstrom, B., B. Lilja, K. Rosberg, and G. Sundkvist.
1986. “Autonomic nerve function tests. Reference values in healthy subjects.” Clinical Physiology 6:523–28.
Biaggioni, I., D. S. Goldstein, T. Atkinson, and D.
Robertson. 1990. “Dopamine-
beta-
hydroxylase deficiency in humans.” Neurology 40:370–73.
Booth, R. W., J. M. Ryan, H. C. Mellet, E. Swiss, and E.
Neth. 1962. “Hemodynamic changes associated with
the Valsalva maneuver in normal men and women.” The
Journal of Laboratory and Clinical Medicine 59:275–85.
Borst, C., W. Wieling, J. F. van Brederode, A. Hond, L.
G. de Rijk, and A. J. Dunning. 1982. “Mechanisms
of initial heart rate response to postural change.” The
American Journal of Physiology 243:H676–81.
Brooker, J. Z., E. L. Alderman, and D. C. Harrison. 1974.
“Alterations in left ventricular volumes induced by
Valsalva manoeuvre.” British Heart Journal 36:713–18.
Cardone, C., F. Bellavere, M. Ferri, and D. Fedele. 1987.
“Autonomic mechanisms in the heart rate response to
coughing.” Clinical Science 72:55–60.
Cardone, C., P. Paiusco, G. Marchetti, et al. 1990. “Cough
test to assess cardiovascular autonomic reflexes in diabetes.” Diabetes Care 13:719–24.
Cheshire, W. P., D. W. Dickson, K. F. Nahm, et al. 2006.
“Dopamine beta-hydroxylase deficiency involves the
central autonomic network.” Acta Neuropathologica
(Berlin) 112:227–29.
Clark, C. V., and R. Mapstone. 1986. “Age-adjusted normal
tolerance limits for cardiovascular autonomic function
assessment in the elderly.” Age and Ageing 15:221–29.
Coker, R., A. Koziell, C. Oliver, and S. E. Smith. 1984. “Does
the sympathetic nervous system influence sinus arrhythmia in man? Evidence from combined autonomic blockade.” The Journal of Physiology (London) 356:459–64.
Cybulski, G., and W. Niewiadomski. 2003. “Influence of
age on the immediate heart rate response to the active
orthostatic test.” Journal of Physiology and Pharma­
cology 54:65–80.
Davidson, J., L. Watkins, M. Owens, et al. 2005.
“Effects of paroxetine and venlafaxine XR on heart
rate variability in depression.” Journal of Clinical
Psychopharmacology 25:480–84.
Delius, W., K. E. Hagbarth, A. Hongell, and B. G. Wallin.
1972. “Manoeuvres affecting sympathetic outflow in human muscle nerves.” Acta Physiologica
Scandinavica 84:82–94.
Denq, J. C., P. C. O’Brien, and P. A. Low. 1998. “Normative
data on phases of the Valsalva maneuver.” Journal of
Clinical Neurophysiology 15:535–40.
Ebert, T. J., J. J. Hayes, J. Ceschi, et al. 1984. “Repetitive
ramped neck suction: A quantitative test of human
baroreceptor function.” The American Journal of
Physiology 247:H1013–17.
Eckberg, D. L. 1980. “Parasympathetic cardiovascular
control in human disease: A critical review of methods and results.” The American Journal of Physiology
239:H581–93.
Eckberg, D. L. 1983. “Human sinus arrhythmia as an
index of vagal cardiac outflow.” Journal of Applied
Physiology 54:961–66.
Eckberg, D. L., Y. T. Kifle, and V. L. Roberts. 1980. “Phase
relationship between normal human respiration and
baroreflex responsiveness.” The Journal of Physiology
(London) 304:489–502.
Elghozi, J. L., and C. Julien. 2007. “Sympathetic control of
short-term heart rate variability and its pharmacologic
modulation.” Fundamental and Clinical Pharmacology
21:337–47.
Espi, F., D. J. Ewing, and B. F. Clarke. 1982. “Testing for
heart rate variation in diabetes: Single or repeated
deep breaths?” Acta Diabetologica Latina 19:177–81.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
39 Cardiovagal Reflexes
Ewing, D. J., C. N. Martyn, R. J. Young, and B. F. Clarke.
1985. “The value of cardiovascular autonomic function
tests: 10 years experience in diabetes.” Diabetes Care
8:491–98.
Ewing, D. J., I. W. Campbell, A. Murray, J. M. Neilson, and
B. F. Clarke. 1978. “Immediate heart-rate response to
standing: Simple test for autonomic neuropathy in diabetes.” British Medical Journal 1:145–47.
Faulkner, M. S., D. Hathaway, and B. Tolley. 2003.
“Cardiovascular autonomic function in healthy adolescents.” Heart and Lung 32:10–22.
Freeman, R. 2006. “Assessment of cardiovascular autonomic
function.” Clinical Neurophysiology 117: 716–30.
Freeman, R. L. 2008. “Noninvasive evaluation of heart
rate: Time and frequency.” In Clinical autonomic
disorders: Evaluation and management, eds. P.
A. Low and E. E. Benarroch, 3rd ed., 185–
197.
Philadelphia: Wolters Kluwer-Lippincott Williams &
Wilkins Publishers.
Freyschuss, U., and A. Melcher. 1975. “Sinus arrhythmia in man: Influence of tidal volume and oesophageal pressure.” Scandinavian Journal of Clinical and
Laboratory Investigation 35:487–96.
Genovely, H., and M. A. Pfeifer. 1988. “RR-variation: The
autonomic test of choice in diabetes.” Diabetes/
Metabolism Reviews 4:255–71.
Gibbons, C. H., W. P. Cheshire, and T. D. Fife. 2014.
“Autonomic testing: American Academy of Neurology
model coverage policy.” Accessed December 14, 2015, at:
https://www.aan.com/uploadedFiles/Website_Library_
Assets/Documents/3.Practice_Management/
1.Reimbursement/1.Billing_and_Coding/5.Coverage_
Policies/14%20Autonomic%20Testing%20Policy%20
v001.pdf.
Goodwin, G. M., D. I. McCloskey, and J. H. Mitchell. 1972.
“Cardiovascular and respiratory responses to changes in
central command during isometric exercise at constant
muscle tension.” Journal of Physiology 226:173–90.
Hon, E. H., and S. T. Lee. 1965. “Electronic evaluation of the fetal heart rate patterns preceding fetal
death: Further observations.” American Journal of
Obstetrics and Gynecology 87:814–26.
Huang, C. C., P. Sandroni, D. M. Sletten, et al. 2007.
“Effect of age on adrenergic and vagal baroreflex
sensitivity in normal subjects.” Muscle and Nerve
36:637–42.
Imholz, B. P., G. A. van Montfrans, J. J. Settels, G. M. van
der Hoeven, J. M. Karemaker, and W. Wieling. 1988.
“Continuous non-invasive blood pressure monitoring: Reliability of Finapres device during the Valsalva
manoeuvre.” Cardiovascular Research 22: 390–97.
Ingall, T. J. 1986. “Autonomic nervous system function in
ageing and in diseases of the peripheral nervous system.” Thesis, University of Sydney.
Jalife, J., and D. C. Michaels. 1994. “Neural control of
sinoatrial pacemaker activity.” In Vagal control of
the heart: Experimental basis and clinical implications, eds. M. N. Levy and P. J. Schwartz, 173–205.
New York: Futura Publishing Company.
Kabir, M. M., M. Kohler, Y. Pamula, et al. 2013.
“Respiratory sinus arrhythmia during sleep in children with upper airway obstruction.” Journal of Sleep
Research 22:463–70.
Kaijser, L., and C. Sachs. 1985. “Autonomic cardiovascular
responses in old age.” Clinical Physiology 5:347–57.
671
Kardos, A., H. Rau, M. W. Greenlee, et al. 1995.
“Comparison of two mechanical carotid baroreceptor
stimulation techniques.” Acta Physiologica Hungarica
83:121–33.
Katona, P. G., and F. Jih. 1975. “Respiratory sinus arrhythmia: Noninvasive measure of parasympathetic cardiac
control.” Journal of Applied Physiology 39:801–5.
Kautzner, J., J. E. Hartikainen, A. J. Camm, and M. Malik.
1996. “Arterial baroreflex sensitivity assessed from
phase IV of the Valsalva maneuver.” The American
Journal of Cardiology 78:575–79.
Khurana, R. K., and R. Wu. 2006. “The cold face test:
A non-baroreflex mediated test of cardiac vagal function.” Clinical Autonomic Research 16:202–7.
Khurana, R. K., D. Mittal, and N. H. Dubin. 2011.
“Valsalva maneuver: Shortest optimal expiratory strain
duration.” Journal of Community Hospital Internal
Medicine Perspectives 18:1.
Khurana, R. K., S. Watabiki, J. R. Hebel, R. Toro, and
E. Nelson. 1980. “Cold face test in the assessment
of trigeminal-brain stem-vagal function in humans.”
Annals of Neurology 7:144–49.
Kingwell, B. A., G. A. McPherson, and P. I. Korner. 1991.
Assessment of gain of tachycardia and bradycardia responses of cardiac baroreflex.” The American
Journal of Physiology 260:H1254–63.
Korner, P. I., A. M. Tonkin, and J. B. Uther. 1976. “Reflex
and mechanical circulatory effects of graded Valsalva
maneuvers in normal man.” Journal of Applied
Physiology 40:434–40.
Korner, P. I., J. Shaw, M. J. West, and J. R. Oliver. 1972.
“Central nervous system control of baroreceptor reflexes in the rabbit.” Circulation Research
31: 637–52.
Korner, P. I., M. J. West, J. Shaw, and J. B. Uther. 1974.
““Steady-state” properties of the baroreceptor-heart
rate reflex in essential hypertension in man.” Clinical
and Experimental Pharmacology and Physiology
1:65–76.
Lacroix, D., R. Logier, S. Kacet, et al. 1992. “Effects of
consecutive administration of central and peripheral
anticholinergic agents on respiratory sinus arrhythmia
in normal subjects.” Journal of the Autonomic Nervous
System 39:211–17.
Leon, D. F., J. A. Shaver, and J. J. Leonard. 1970. “Reflex
heart rate control in man.” American Heart Journal
80:729–39.
Levin, A. B. 1966. “A simple test of cardiac function based
upon the heart rate changes induced by the Valsalva
maneuver.” The American Journal of Cardiology
18:90–99.
Loula, P., V. Jäntti, and A. Yli-Hankala. 1997. “Respiratory
sinus arrhythmia during anaesthesia: Assessment of
respiration related beat-to-beat heart rate variability
analysis methods.” International Journal of Clinical
Monitoring and Computing 14:241–49.
Low, P. A. 2003. “Testing the autonomic nervous system.”
Seminars in Neurology 23:407–21.
Low, P. A., and D. M. Sletten. 2008. “Laboratory evaluation
of autonomic failure.” In Clinical autonomic disorders:
Evaluation and management, eds. P. A. Low and E.
E. Benarroch, 3rd ed., 130–63. Philadelphia: Wolters
Kluwer-Lippincott Williams & Wilkins Publishers.
Low, P. A., and T. L. Opfer-Gehrking. 1992. “Differential
effects of amitriptyline on sudomotor, cardiovagal, and
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
672
Section 5: Assessment of Autonomic Function
adrenergic function in human subjects.” Muscle and
Nerve 15:1340–44.
Low, P. A., J. C. Denq, T. L. Opfer-Gehrking, P. J. Dyck, P.
C. O’Brien, and J. M. Slezak. 1997. “Effect of age and
gender on sudomotor and cardiovagal function and
blood pressure response to tilt in normal subjects.”
Muscle and Nerve 20:1561–68.
Low, P. A., T. L. Opfer-Gehrking, C. J. Proper, and I.
Zimmerman. 1990. “The effect of aging on cardiac
autonomic and postganglionic sudomotor function.”
Muscle and Nerve 13:152–57.
Marfella, R., D. Giugliano, G. di Maro, R. Acampora, R.
Giunta, and F. D’Onofrio. 1994. “The squatting test.
A useful tool to assess both parasympathetic and sympathetic involvement of the cardiovascular autonomic
neuropathy in diabetes.” Diabetes 43:607–12.
Masaoka, S., A. Lev-Ran, L. R. Hill, G. Vakil, and E.
H. Hon. 1985. “Heart rate variability in diabetes: Relationship to age and duration of the disease.”
Diabetes Care 8:64–68.
Mehlsen, J., K. Pagh, J. S. Nielsen, L. Sestoft, and S.
L. Nielsen. 1987. “Heart rate response to breathing: Dependency upon breathing pattern.” Clinical
Physiology 7:115–24.
Nishimura, R. A., and A. J. Tajik. 1986. “The Valsalva
maneuver and response revisited.” Mayo Clinic
Proceedings 61:211–17.
Novak, V., P. Novak, J. de Champlain, et al. 1993. “Influence
of respiration on heart rate and blood pressure fluctuations.” Journal of Applied Physiology 74:617–26.
Novak, V., P. Novak, T. L. Opfer-Gehrking, and P. A. Low.
1996. “Postural tachycardia syndrome: Time frequency mapping.” Journal of Autonomic Nervous
System 61:313–20.
O’Brien, I. A., P. O’Hare, and R. J. Corrall. 1986. “Heart
rate variability in healthy subjects: Effect of age and
the derivation of normal ranges for tests of autonomic
function.” British Heart Journal 55:348–54.
Opfer-Gehrking, T. L., and P. A. Low. 1993. “Impaired
respiratory sinus arrhythmia with paradoxically normal Valsalva ratio indicates combined cardiovagal and
peripheral adrenergic failure.” Clinical Autonomic
Research 3:169–73.
Overbeek, T. J., A. van Boxtel, and J. H. Westerink. 2014.
“Respiratory sinus arrhythmia responses to cognitive tasks: Effects of task factors and RSA indices.”
Biological Psychology 99:1–14.
Parati, G., R. Casadei, A. Groppelli, M. Di Rienzo, and G.
Mancia. 1989. “Comparison of finger and intra-arterial
blood pressure monitoring at rest and during laboratory testing.” Hypertension 13:647–55.
Pfeifer, M. A., D. Cook, J. Brodsky, et al. 1982. “Quantitative
evaluation of cardiac parasympathetic activity in normal and diabetic man.” Diabetes 31:339–45.
Pitzalis, M. V., F. Mastropasqua, F. Massari, et al. 1998.
“Beta-
blocker effects on respiratory sinus arrhythmia and baroreflex gain in normal subjects.” Chest
114:185–91.
Rottenberg, J. 2007. “Cardiac vagal control in depression:
A critical analysis.” Biological Psychology 74:200–11.
Sanders, J. S., A. L. Mark, and D. W. Ferguson. 1989.
“Evidence for cholinergically mediated vasodilatation
at the beginning of isometric exercise in humans.”
Circulation 79:815–24.
Sandroni, P., E. E. Benarroch, and P. A. Low. 1991.
“Pharmacological dissection of components of the
Valsalva maneuver in adrenergic failure.” Journal of
Applied Physiology 71:1563–67.
Saul, J. P., and R. J. Cohen. 1994. “Respiratory sinus arrhythmia.” In Vagal control of the heart: Experimental
basis and clinical implications, eds. M. N. Levy and
P. J. Schwartz, 511–36. New York: Futura Publishing
Company.
Schaller, B. 2004. “Trigeminocardiac reflex: A clinical phenomenon or a new physiological entity?” Journal of
Neurology 251:658–65.
Schrezenmaier, C., W. Singer, N. M. Swift, et al. 2007.
“Adrenergic and vagal baroreflex sensitivity in autonomic failure.” Archives of Neurology 64:381–86.
Sharpey-Schafer, E. P. 1955. “Effects of Valsalva’s manoeuvre on the normal and failing circulation.” British
Medical Journal 1:693–95.
Smith, M. L., L. A. Beightol, J. M. Fritsch-
Yelle, K.
A. Ellenbogen, T. R. Porter, and D. L. Eckberg. 1996.
“Valsalva’s maneuver revisited: A quantitative method
yielding insights into human autonomic control.” The
American Journal of Physiology 271:H1240–49.
Smith, S. A. 1982. “Reduced sinus arrhythmia in diabetic autonomic neuropathy: Diagnostic value of an
age-
related normal range.” British Medical Journal
285:1599–601.
Spallone, V., F. Bellavere, L. Scionti, et al. 2011.
“Recommendations for the use of cardiovascular tests in
diagnosing diabetic autonomic neuropathy.” Nutrition,
Metabolism, and Cardiovascular Diseases 21:69–78.
Spyer, K. M. 1999. “Central nervous control of the cardiovascular system.” In Autonomic failure: A textbook of
clinical disorders of the autonomic nervous system,
eds. C. J. Mathias and R. Bannister, 4th ed., 45–55.
New York: Oxford University Press.
Tannus, L. R., S. Sperandei, R. M. Montenegro Júnior,
et al. 2013. “Reproducibility of methods used for the
assessment of autonomic nervous system’s function.”
Autonomic Neuroscience 177:175–79.
Ten Harkel, A. D., J. J. Van Lieshout, E. J. Van Lieshout,
and W. Wieling. 1990. “Assessment of cardiovascular
reflexes: Influence of posture and period of preceding
rest.” Journal of Applied Physiology 68:147–53.
Tonhajzerova, I., M. Javorka, Z. Trunkvalterova, et al.
2008. “Cardio-respiratory interaction and autonomic
dysfunction in obesity.” Journal of Physiology and
Pharmacology 59(Suppl 6):709–18.
Trimarco, B., M. Volpe, B. Ricciardelli, et al. 1983.
“Valsalva maneuver in the assessment of baroreflex responsiveness in borderline hypertensives.”
Cardiology 70:6–14.
Vallbona, C., D. Cardus, W. A. Spencer, and H. E. Hoff.
1965. “Patterns of sinus arrhythmia in patients with
lesions of the central nervous system.” The American
Journal of Cardiology 16:379–89.
van Lieshout, E. J., J. J. van Lieshout, A. D. ten Harkel,
and W. Wieling. 1989a. “Cardiovascular responses
to coughing: Its value in the assessment of autonomic nervous control.” Clinical Science (London)
77:305–10.
van Lieshout, J. J., W. Wieling, K. H. Wesseling, and J.
M. Karemaker. 1989b. “Pitfalls in the assessment of
cardiovascular reflexes in patients with sympathetic
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
39 Cardiovagal Reflexes
Assessment of cardiac autonomic function.” Biometrics
40:855–61.
Wieling, W. 1983. “Reduced sinus arrhythmia in diabetic
autonomic neuropathy.” British Medical Journal
286:1285.
Wieling, W., and J. J. van Lieshout. 1990. “The assessment
of cardiovascular reflex activity: Standardization is
needed.” Diabetologia 33:182–83.
Wieling, W., J. F. van Brederode, L. G. de Rijk, C. Borst,
and A. J. Dunning. 1982. “Reflex control of heart
rate in normal subjects in relation to age: A data
base for cardiac vagal neuropathy.” Diabetologia
22:163–66.
Wieling, W., M. P. Harms, A. D. ten Harkel, et al. 1996.
“Circulatory response evoked by a 3 s bout of dynamic
leg exercise in humans.” Journal of Physiology
494:601–11.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
failure but intact vagal control.” Clinical Science
76:523–28.
Wallin, B. G., and D. L. Eckberg. 1982. “Sympathetic transients caused by abrupt alterations of carotid baroreceptor activity in humans.” The American Journal of
Physiology 242:H185–90.
Wang, J., X. Wang, M. Irnaten, et al. 2003. “Endogenous
acetylcholine and nicotine activation enhances
GABAergic and glycinergic inputs to cardiac vagal
neurons.” Journal of Neurophysiology 89:2473–81.
Wei, J. Y., J. W. Rowe, A. D. Kestenbaum, and
S. Ben-
Haim. 1983. “Post-
cough heart rate
response: Influence of age, sex, and basal blood
pressure.” The American Journal of Physiology
245:R18–24.
Weinberg, C. R., and M. A. Pfeifer. 1984. “An improved
method for measuring heart-
rate variability:
673
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Chapter 40
Electrophysiology of Pain
Paola Sandroni
INTRODUCTION
LASER EVOKED POTENTIALS
QUANTITATIVE SENSORY TEST
CONTACT HEAT EVOKED POTENTIALS
AUTONOMIC TESTS
SUMMARY
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
MICRONEUROGRAPHY
INTRODUCTION
The diagnosis and treatment of neuropathic
pain are a challenge for physicians caring for
patients who have medical conditions causing
this type of pain. The incompletely understood
complex mechanisms of neuropathic pain contribute to the difficulty. Another major obstacle
has been finding a test to objectively demonstrate and quantify a physiological disruption
in sensory function that may be the cause of
the pain. For many years, those involved in the
study of pain have attempted to quantify the
pain experience solely by bedside psychophysical evaluations and the subjective reports of
patients. Tests of large-fiber function, including
vibrometry, sensory nerve conduction studies,
and routine somatosensory evoked potentials,
have been used to document large myelinated
fiber sensory abnormalities that might also
involve small-diameter axons of the nociceptive
system. The first step was to develop neurophysiological techniques to assess the function
of the peripheral and central components of
pain pathways in normal subjects. The next
step was to refine the techniques and to gather
normal data. These techniques can be applied
to patients with altered sensory function, specifically those with neuropathic pain. The tests
are objective or semi-
objective physiological
measures that correlate with abnormal function in the nociceptive system and document
a lesion that potentially could result in pain.
They allow clinicians to assess neuropathic
pain by quantifying responses to neurophysiological tests and using the results to develop a
better understanding of the underlying pathophysiological mechanisms of the pain.
674
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
40 Electrophysiology of Pain
This chapter reviews various neurophysiological techniques used to study the function
and dysfunction of the nociceptive system in
humans, including quantitative sensory tests
(QSTs), autonomic tests, microneurography
(MCNG), laser evoked potentials (LEPs)
and contact heat evoked potential stimulators
(CHEPS). The review outlines the physiological basis of and methods for performing these
techniques, some applications of the tests in
patients with pain, and some of the potential
pitfalls in the use of these tests. Details of the
techniques for performing autonomic tests are
given in Chapters 35–39.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
QUANTITATIVE SENSORY TEST
The quantitative sensory test (QST) is useful
for assessing myelinated and unmyelinated sensory fibers in the periphery and in nociceptive
pathways of the central nervous system in persons with neurogenic pain (Greenspan 2001).
The test uses controlled thermal stimulation
of the skin to allow examiners to reproducibly
quantify sensory nerve function of nociceptive
pathways. It relies on the subjective report of
the patient that he or she perceives the stimulus. The QST quantifies sensory nerve function by allowing the examiner to determine the
intensity of stimulus required for perception
and, at times, to correlate this with the patient’s
report of the type and intensity of sensation.
The test must use one stimulus type at a time,
with precisely defined physical characteristics
and intensity. The apparatus must have a program that allows the examiner to deliver stimuli to the skin of the patient using appropriate
algorithms. This ensures that the test provides
an accurate, consistent, and semi-
objective
assessment of sensory function.
The most useful and efficient algorithm
for determining pain thresholds—that is, the
intensity at which at least 50% of the stimuli
are perceived as painful—is the method of limits. In addition, this algorithm allows the examiner to obtain reliable results with delivery of
the lowest number of potentially unpleasant
stimuli. This is important because repetitive
stimulation of a primary afferent can produce
sensitization. The method of limits exposes the
patient to a stimulus of changing intensity after
he or she has been instructed to signal the first
675
perception of pain or temperature sensation,
called the appearance threshold. Thresholds
may also be approached from above threshold level, with the patient reporting the cessation of sensation, called the disappearance
threshold. This algorithm is as sensitive and
reproducible as other, less time-
efficient,
methods—
for example, forced-
choice testing, which may give lower absolute values but
does not provide more accurate data (Claus,
Hilz, and Neundorfer 1990; Dyck et al. 1990;
Peripheral Neuropathy Association 1993).
Magnitude estimation, an algorithm that
uses a visual analog scale to rate sensation
perceived when a suprathreshold stimulus is
applied, is useful in evaluating pain (Price et al.
1983; Price 1988; Gruener and Dyck 1994).
Dyck et al. developed a method called the 4,
2, and 1 stepping algorithm that incorporates
magnitude estimation with the addition of null
stimuli randomly interposed between pyramidal and flat-topped pyramidal stimuli (Dyck
et al. 1993). The testing starts at an intermediate level of stimulus intensity, uses 25 steps
to reach maximal intensity, and uses the visual
analogue scale that allows patients to rate the
pain intensity. This method of testing produces results that are well correlated with the
standard forced-choice algorithm (Dyck et al.
1993; Dyck et al. 1993). The examiner can
observe abnormal patterns that correspond to
pathophysiological changes in the sensory nervous system, central or peripheral. There are
also clues to nonphysiological or psychogenic
abnormal patterns with erratic results that are
not reproducible.
QST systems provide a temperature stimulus by means of a contact Peltier-type thermode, with a surface area of 3–13 cm2 that is
applied to the skin to warm or cool the area
under the thermode. A thermocouple is placed
at the skin–thermode interface to monitor the
temperature of the stimulus. The thermode is
set initially at the adaptation or holding temperature of 30°C–34°C, within the range of
temperature at which only a transient thermal sensation is caused by placing the probe
on the skin (Darian-Smith 1984). The examiner operates the apparatus to cause temperature changes within certain limits, usually
0°C–50°C, that are set to prevent burning the
patient’s skin. The rate of temperature change
should be standardized to ensure the validity of normal data. The findings from a study
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
676
Section 5: Assessment of Autonomic Function
using psychophysical measures and MCNG
to record C nociceptor activity in response
to noxious heat stimuli delivered with a QST
apparatus to the skin of normal human volunteers are shown in Figure 40–1. This study
showed that both the magnitude of pain perceived by the subjects and the frequency of C
nociceptor discharges in response to the stimulus increased with faster rates of temperature
increase (Yarnitsky et al. 1992). Therefore, the
examiner should conduct the QST using a consistent temperature ramp for gathering normal
data and testing patients.
The patient indicates when the first sensation occurs in response to cooling or warming
the stimulus probe attached to the skin. The
sensation (stimulus perception or pain) that
occurs in response to a cold or hot stimulus is
indicated by the patient, who either tells the
examiner or presses a button to halt the stimulus and to reset the thermode temperature to
the holding level. The QST apparatus records
the stimulus temperature at which the patient
indicated perception of a change in temperature or pain. The test apparatus includes standardized thermode size, stimulation sites, rate
of change in stimulus temperature, interstimulus intervals, and pre-test skin temperature.
Tests are performed in normal volunteers
and in patients who have pain, to provide standardized normal values and valid comparisons.
In addition, comparison of the results obtained
on painful areas of skin with those obtained
from the same site on the uninvolved side
allows the examiner to determine whether unilateral cold or heat hyperalgesia or allodynia
is present. The interpreter of results should
consider that cold hypalgesia may occur in normal subjects as well as in patients with pain.
Heat hypalgesia alone is rare and difficult to
document because of the setting of an upper
temperature limit of 50°C to prevent injury.
The normal ranges of pain thresholds obtained
using the method of limits are 44°C–47°C for a
hot stimulus and 9°C–12°C for a cold stimulus
(Verdugo and Ochoa 1992).
The QST evaluates the entire peripheral
and central portions of the sensory system that
participate in the transmission and perception of painful hot or cold stimuli. Thermal
stimulation directly activates the receptor in
the skin, and the receptor in turn activates the
axon innervating it. In the peripheral nervous
system, the primary afferent fibers that convey
these messages to the central nervous system
are C and Aδ nociceptors. The central nociceptive system consists of the spinothalamic tract,
cerebral cortex, antinociceptive areas of the
brain stem, and probably the hypothalamus,
amygdala, and limbic cortex (Willis 1995).
Decreased (hyperalgesia or allodynia) or
increased (hypalgesia) thresholds for the perception of a cold or hot stimulus may occur
in various combinations, as demonstrated by
Verdugo and Ochoa in patients with somatosensory disorders (Figures 40–
2, 40–
3,
and 40–4) (Verdugo and Ochoa 1992). In some
patients with pain, the somatosensory abnormality is hyperalgesia selectively in response to
a cold or a hot stimulus. Ochoa and Yarnitsky
described patients with neuropathy who had
cold skin, reduced ability to perceive cool
stimuli, and cold hyperalgesia. These patients
had evidence of small myelinated Aδ-fiber neuropathy with sparing of unmyelinated C fibers.
Many clinical reports indicate that patients
with complex regional pain syndrome (CRPS),
or reflex sympathetic dystrophy (RSD), frequently report cold hyperalgesia on the QST
or bedside examination. In fact, a comprehensive QST evaluation of patients with this clinical diagnosis by means of the QST showed that
they may have cold hyperalgesia, heat hyperalgesia, or both. These abnormalities can be
quantified and followed clinically with the QST
to show response to treatment (Verdugo and
Ochoa 1992; Wahren and Torebjork 1992).
Heat hyperalgesia with spontaneous burning
pain occurs in erythromelalgia or capsaicin-
treated skin. The QST pattern in these
instances is one of decreased threshold for pain
to hot, but not to cold, stimuli. The spontaneous burning pain and mechanical hyperalgesia
in these patients can be lessened by decreasing skin temperature, but the pain remains
during compression-
ischemia A-
fiber nerve
block. This experimental finding indicates
that C fibers mediate these sensory changes
of primary hyperalgesia within the actual area
of injury in patients or in the area where capsaicin is applied directly to the skin of normal
subjects (Culp et al. 1989). A study in human
subjects that used QST and MCNG to identify sensitized C nociceptors in the peripheral nerve innervating an area of skin where
the patient experienced spontaneous burning
pain and heat hyperalgesia showed that the
neural discharge of the abnormal, sensitized
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
A
Overall
discharge
rate
0.83 impulses/s
Temp. (ºC)
47
44
41
38
35
32
0.3 ºC/s
10
0
20
Stim.
on
30
Peak
magnitude of
suprathreshold
pain = 5
40
Stim.
off
Time (s)
B
Overall
discharge
rate
5.25 impulses/s
Temp. (ºC)
47
44
41
38
35
32
2 ºC/s
0
2
4
6
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Stim.
on
8
Time (s)
10
12
14
16
Peak
magnitude of
suprathreshold
pain = 10
Stim.
off
C
Overall
discharge
rate
17.1 impulses/s
Temp. (ºC)
47
44
41
38
35
32
6 ºC/s
0
1
2
Stim.
on
3
4
5
6
7
8
9
Peak
magnitude of
suprathreshold
pain = 55
Stim.
off
Time (s)
Figure 40–1. A–C, Discharge of a single C nociceptor in response to heat stimulus ramps between 32°C and 47°C, at
three rates of temperature rise. Note different time bases for each of the three graphs. Discharge rate recorded and peak
magnitude estimate of evoked pain are given. From Yarnitsky, D., D. A. Simone, R. M. Dotson, M. A. Cline, and J. L.
Ochoa. 1992. “Single C nociceptor responses and psychophysical parameters of evoked pain: Effect of rate of rise of heat
stimuli in humans.” The Journal of Physiology 450:581–92. By permission of the Physiological Society.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
678
Section 5: Assessment of Autonomic Function
A
50ºC
B
C
A
D
HP
50ºC
B
C
D
E
HP
WS
WS
32ºC
CS
32ºC
CS
5ºC
5ºC
CP
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 40–2. Pure cold pain and/or heat pain hyperalgesia. A, Normal pattern; B, Pure cold pain hyperalgesia
(30 patients); C, Pure heat hyperalgesia (26 patients);
D, Combined cold pain and heat pain hyperalgesia (5
patients). CP, cold pain; CS, cold sensation; HP, heat pain;
WS, warm sensation. From Verdugo, R., and J. L. Ochoa.
1992. “Quantitative somatosensory thermotest. A key
method for functional evaluation of small calibre afferent
channels.” Brain 115:893–913. By permission of Oxford
University Press.
C nociceptors correlated with the perceived
magnitude of pain as measured by the visual
analog scale (Figures 40–5 and 40–6) (Cline,
Ochoa, and Torebjork 1989). The QST is useful in determining the pattern and degree of
abnormality, in following the clinical course,
and in documenting the response to treatment (Wahren and Torebjork 1992; Wahren,
Torebjork, and Nystrom 1991).
QST measurements can document and
quantify hypesthesia, hyperesthesia, hypalgesia, and hyperalgesia. Thus, the clinician has a
reproducible measurement of nerve dysfunction that can be attributed to a particular type
of primary afferent nerve fiber or central pathway that may be involved in pain production.
In a large study of 1236 patients with clinical diagnosis of neuropathic pain Maier et al.
(2010) found 92% of patients had at least one
abnormality. The most frequent combinations
of gain and loss were mixed thermal/mechanical loss without hyperalgesia (central pain and
polyneuropathy), mixed loss with mechanical
CP
Figure 40–3. Thermal hypesthesia combined with thermal pain hyperalgesia. A, Normal pattern; B, Warm hypesthesia associated with cold pain hyperalgesia (6 patients); C,
Warm hypesthesia associated with heat pain hyperalgesia
(1 patient); D, Cold hypesthesia associated with cold pain
hyperalgesia (4 patients); E, Cold hypesthesia associated
with heat pain hyperalgesia (17 patients). CP, cold pain;
CS, cold sensation; HP, heat pain; WS, warm sensation.
From Verdugo, R., and J. L. Ochoa. 1992. “Quantitative
somatosensory thermotest. A key method for functional
evaluation of small calibre afferent channels.” Brain
115:893–913. By permission of Oxford University Press.
hyperalgesia in peripheral neuropathies, and
mechanical hyperalgesia without any loss in
trigeminal neuralgia. Thus, somatosensory
profiles with different combinations of loss and
gain are shared across the major neuropathic
pain syndromes.
However, the QST does not differentiate central from peripheral dysfunction, because the
abnormalities found are not specifically localized and may be located in the nociceptive pathway at any level of the neuraxis. This test can be
used to make the initial assessment, to follow the
clinical course, and to determine the response
to medications and other forms of intervention
(Nygaard et al. 2000; Attal et al. 2000).
The Neuropathic Pain Special Interest
Group of the International Association for the
Study of Pain in 2013 (Backonja et al.) publishes a consensus paper recommending the
use of QST in clinical practice for screening for
small and large fiber neuropathies; monitoring
somatosensory deficits; and monitoring evoked
pains, allodynia, and hyperalgesia. QST is not
recommended as a stand-
alone test for the
diagnosis of neuropathic pain.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
40 Electrophysiology of Pain
A
50ºC
C
B
D
HP
WS
32ºC
CS
CP
5ºC
AUTONOMIC TESTS
Patients with neurogenic pain and features
indicating involvement of the sympathetic nervous system, either sudomotor or vasomotor,
have a poorly understood pain symptom complex known as complex regional pain syndrome
(CRPS) or reflex sympathetic dystrophy (RSD)
(Dotson 1993; Stanton-
Hicks et al. 1995).
Visual inspection and patients’ reports of alterations in sweating and skin temperature of
involved body areas implicate the sympathetic
nervous system. The multiple pathophysiological mechanisms that may result in this clinical
pattern are not completely known. There are
several possibilities regarding the exact role of
the sympathetic efferents in this context, and
this may vary from patient to patient or even
within the same patient. These efferents may
be the passive or the reactive arc of a somatosympathetic reflex response to noxious input.
Also, denervated sympathetic end organs in
case of nerve injury may cause the clinical
symptoms or signs of autonomic nervous system involvement in neuropathic pain. Roberts
proposed that sympathetic efferents normally
have an active role in helping maintain low-
threshold mechanoreceptor input to sensitized
central nociceptors (Roberts 1986). Another
hypothesis is that nociceptor activity is maintained by sympathetic efferent activity, thereby
Maximum pain
Pain rating
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 40–4. Thermal hypesthesia combined with thermal pain hyperalgesia (continuation of Figure 40–
3).
A, Normal pattern; B, Cold hypesthesia associated with
cold and heat pain hyperalgesia (5 patients); C, Cold and
warm hypesthesia associated with cold pain hyperalgesia
(1 patient); D, Cold and warm hypesthesia associated with
cold and heat pain hyperalgesia (1 patient). CP, cold pain;
CS, cold sensation; HP, heat pain; WS, warm sensation.
From Verdugo, R., and J. L. Ochoa. 1992. “Quantitative
somatosensory thermotest. A key method for functional
evaluation of small calibre afferent channels.” Brain
115:893–913. By permission of Oxford University Press.
679
No pain
2 seconds
Figure 40–5. Correlation between neural discharge of an identified sensitized C polymodal nociceptor with receptive field
in symptomatic skin (upper trace) and simultaneous temporal profile of pain magnitude (lower trace) in response to gentle
stroking of the receptive field. From Cline, M. A., J. Ochoa, and H. E. Torebjörk. 1989. “Chronic hyperalgesia and skin
warming caused by sensitized C nociceptors.” Brain 112:621–47. By permission of Oxford University Press.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
680
Section 5: Assessment of Autonomic Function
2 seconds
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 40–6. Response of an identified C polymodal unit
in symptomatic skin (upper trace) compared with that from
opposite non-painful hand (lower trace). The mechanical
stimulus (stroking with a blunt wooden stick) was applied
to the receptive fields, at a time marked by arrowheads.
Note the prolonged after-discharge for the C unit in symptomatic skin. From Cline, M. A., J. Ochoa, and H. E.
Torebjörk. 1989. “Chronic hyperalgesia and skin warming
caused by sensitized C nociceptors.” Brain 112:621–47. By
permission of Oxford University Press.
causing spontaneous or stimulus-induced sympathetically maintained pain. Indirect evidence
supports the idea that there is sympathetic
activation of nociceptors in humans with the
clinical features of CRPS (Campbell, Meyer,
and Raja 1992). However, data from animal
research indicate that, in peripheral nerve
injury, sympathetic efferent activity causes
excitation of cutaneous nociceptors (Levine
et al. 1986; Sato and Perl 1991; Sato et al. 1993;
Gold et al. 1994).
qsart. The quantitative sudomotor axon
reflex test (QSART), discussed in Chapter 36,
is a sensitive test with an approximately 20%
coefficient of variation. Thus, this test gives
reproducible results in normal subjects and in
patients with neuropathy. Furthermore, there
is no significant side-to-side difference in normal subjects. This allows clinicians to compare
the results in patients to normative values
and to determine side-to-side differences in
a patient with a unilateral painful condition to
obtain useful information about sympathetic
dysfunction or sympathetic involvement in
neuropathic pain states that fit the definition
of CRPS (Low 1993; Chelimsky et al. 1995;
Sandroni et al. 1998).
Patterns of QSART response that occur
in limbs affected by painful peripheral neuropathies and CRPS are excessive or persistent sweat responses with reduced latencies
or, in some cases, decreased sweat volumes
(Low 1993; Chelimsky et al. 1995; Sandroni
et al. 1998). An abnormal QSART pattern in a
patient complaining of pain provides an objective measure indicating a pathophysiological
change in the involved limb that may occur
with, but is not necessarily a causative factor
for, the neuropathic pain.
Measurements of resting sweat output are
helpful in conjunction with QSART to show
sudomotor abnormalities in patients with the
clinical features of CRPS. These patients tend
to have increased resting sweat output on the
involved limb compared with the normal side
(Chelimsky et al. 1995; Sandroni et al. 1998).
Sympathetic Skin Response. The sympathetic skin response (SSR) evaluates
sympathetic sudomotor function through
somatosympathetic reflexes (Shahani et al.
1984). Some reports have documented SSR
abnormalities in sudomotor function in patients
with CRPS (Cronin, Kirsner, and Fitzroy 1982;
Rommel et al. 1995). Because of inherent difficulties in producing quantifiable and reproducible data with the SSR technique, it is not
a useful neurophysiological tool for the assessment of neuropathic pain.
Skin Temperature Measurements. Skin
temperature measurements with a surface
thermistor or infrared thermography can compare multiple sites on the skin of the involved
extremity with the corresponding areas on the
asymptomatic extremity. Because patients with
neuropathic pain or CRPS may have alterations in skin temperature in conjunction with
sensory aberrations, these measurements
permit examiners to document clinically useful abnormal temperature patterns or asymmetries caused by various pathophysiological
mechanisms (Chelimsky et al. 1995). Patients
with lesions causing deafferentation pain and
vasomotor denervation may have relatively
warm skin on the involved side because of vasodilatation. Later in the course of the condition,
denervation supersensitivity results in vasoconstriction caused by upregulation of adrenoreceptors on blood vessels that begin to respond
more vigorously to circulating catecholamines.
Thus, the skin on the involved side becomes
cooler than that on the normal side. Maneuvers
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
40 Electrophysiology of Pain
that usually result in reflex warming of the skin,
such as warming another part of the body or
sympathetic blockade of the affected area, do
not cause warming of that area of skin.
Patients with sensitized C nociceptors,
erythromelalgia, or topically applied capsaicin
secrete vasodilating substances antidromically
from active nociceptors, and as a result, the skin
is warm in the areas with pain and hyperalgesia (Culp et al. 1989; Ochoa 1986; Ochoa et al.
1987). This effect can be reproduced in normal human volunteers by performing MCNG
with intraneural microstimulation at intensities
that produce a painful sensation. Initially, the
pain may cause vasoconstriction that is readily
apparent on infrared thermography as cooling
of the skin. Continued activity in the primary
nociceptors with microstimulation causes vasodilatation and warming of the skin that sympathetic reactivation can override to produce cool
skin. This may provide a pathophysiological
explanation for the variability in the temperature of the painful area of skin compared with
that of the normal skin in patients with neuropathic pain (Ochoa et al. 1993).
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
MICRONEUROGRAPHY (MCNG)
In MCNG, semi-
microelectrodes with a tip
diameter of 1–15 µm are inserted percutaneously into an accessible peripheral nerve to
record the activity in a single axon, in a portion of a fascicle, or in an entire nerve fascicle (Vallbo et al. 1979). MCNG is useful
for uncovering the physiological mechanisms
of neuropathic pain (Torebjork 1993). It is a
time-
consuming test that requires a highly
motivated and observant patient for successful
acquisition of useful data. The electrode is connected via a preamplifier to an amplifier with
attached audiomonitors and an oscilloscope
to permit the examiner to monitor the neural
activity of a peripheral nerve innervating an
involved area of skin. The recording of skin and
muscle sympathetic activity, Aβ low-threshold
mechanoreceptors, and Aδ and C nociceptor
afferent activity can provide pathophysiological
information about the mechanisms of different
types of neuropathic pain.
As noted above, MCNG has documented
the occurrence of sensitized C nociceptors in a
patient with erythromelalgia-type pain (Cline,
681
Ochoa, and Torebjork 1989). Torebjork et al.
used MCNG to provide evidence that an injury
or the application of capsaicin to the skin causes
central sensitization in the area of secondary
hyperalgesia outside the actual area of capsaicin injection or topical application (Torebjork,
Lundberg, and LaMotte 1992). Ongoing nociceptive input appears to help maintain this sensitization (Torebjork 1993).
With MCNG, investigators have identified
three previously undescribed types of human
C nociceptors that respond only to mechanical, heat, or chemical stimuli (Schmidt et al.
1995). Some of these units were sensitized
to heating or mechanical stimuli after chemical stimulation with mustard oil, capsaicin, or
tonic pressure (Schmidt et al. 2000; Schmelz
et al. 2000). These probably play a role in the
primary hyperalgesia that occurs with chemical
irritation or inflammation and in the secondary
hyperalgesia caused by central sensitization.
Animal experiments have shown that sympathetic activation of primary afferents occurs
with direct stimulation of sympathetic nerves
(Roberts 1986). This was not found in MCNG
studies of human subjects and patients with
the clinical features of CRPS in whom reflex
activation of sympathetic efferents did not
activate low-
threshold mechanoreceptors
(Dotson et al. 1990). In animals, the activity of sympathetic efferents results in neural
activity in low-
threshold mechanoreceptors
even in the normal state; sympathetic efferents have a similar effect on nociceptors only
after nerve injury (Sato and Perl 1991; Sato
et al. 1993; Gold et al. 1994). Although patients
with CRPS symptoms have allodynia on neurological examination, activity in single, isolated
low-threshold mechanoreceptors produced by
intraneural microstimulation at frequencies
up to 30 Hz did not cause pain (Dotson et al.
1992). This suggests that temporal and spatial
summation may be necessary for spontaneous
or stimulus-induced pain to occur with activation of low-threshold mechanoreceptors in the
presence of central nociceptor sensitization.
MCNG may be used to unravel the complex story of pain and the sympathetic nervous
system in humans by directly recording sympathetic efferent activity. With MCNG, Casale
and Elam demonstrated normal activity in a
sympathetic efferent fiber in a nerve innervating a painful area of skin of a patient with
the clinical symptom complex of CRPS. Our
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
682
Section 5: Assessment of Autonomic Function
observations in several such patients are consistent with this finding (Casale and Elam 1992).
Serra et al. (Serra et al. 2012) have shown
the presence of spontaneous activity of
peripheral nociceptors in patients with neuropathic pain, which could be a biomarker of
spontaneous pain.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
LASER EVOKED POTENTIALS
LEPs provide a noninvasive, easily tolerated
means of directly assessing function of the central and peripheral portions of the nociceptive
system (Rossi et al. 2000). Carmon et al. first
showed that stimulation of normal human skin
with short-duration infrared CO2 laser pulses
produced a near-field cerebral potential at the
vertex (Carmon, Mor, and Goldberg 1976).
Amplitudes of the cerebral response usually
correlate well with the intensity of perceived
pain reported by patients in response to the
stimulus and with the intensity of the applied
stimulus (Beydoun et al. 1993). Wu et al.
reported on two patients with hyperalgesia
(caused by central pain in one and peripheral
neuropathic pain in the other) in whom the
LEP responses were delayed, desynchronized,
and attenuated (Wu et al. 1999).
Heat pain–producing lasers, as opposed to
transcutaneous electrical stimulation of peripheral nerves traditionally used for somatosensory evoked potentials, can induce pain with
minimal influence on other sensations.
Only minimal habituation, adaptation, or tissue damage tends to occur even with repeated
applications of the laser stimulus. Although
some laboratories use intracutaneous electrical shock to obtain pain somatosensory evoked
potentials, most laboratories perform LEPs.
The laser does not contact the skin directly as it
produces an invisible, inaudible, short-duration
(20 ms) radiant heat pulse. The very superficial
layers of skin (20–50 mm) are able to absorb
this pulse because of its long wavelength (CO2
laser, 10.6 µm; and thulium YAG laser, 1.8–
2.01 µm) (Carmon, Mor, and Goldberg 1976;
Bromm 1995; Kazarians, Scharein, and Bromm
1995; Treede et al. 1995; Spiegel, Hansen, and
Treede 2000). This type of stimulus produces
a rapid increase in skin surface temperature
(50°C per second) and selectively activates
the smallest diameter nerve terminals of thinly
myelinated Aδ and unmyelinated C fibers
(Casale and Elam 1992; Wu et al. 1999; Bromm
1995). Laser stimulus intensity is best characterized as stimulus energy per unit area, and
the average pain threshold in young healthy
adults is 10 mJ/mm2 (Gibson, LeVasseur, and
Helme 1991).
LEPs have larger amplitudes than do routine somatosensory evoked potentials and
require averaging of only 25–40 responses. The
components of LEPs include late and ultra-late
waveforms with a maximal amplitude over the
vertex at the Cz electrode (according to the
International 10–20 System). Laser activation
of Aδ fibers that have conduction velocities of
4–30 m/second in humans causes first pain,
with a latency of approximately 500 ms corresponding with the late LEP (Vallbo et al. 1979).
The typical waveform obtained with stimulation of the skin on the dorsum of the hand
has middle latency negative peaks (N1, N170),
a negative peak (N2) at a latency of 250 ± 20
ms (mean ± SD), and a positive peak (P2) at
390 ± 30 ms. N2 is maximal at Cz, with extension into the central leads, but P2 is maximal
at Cz and Pz electrodes. The level of attention,
arousal, and distraction influences these potentials, especially Pz, and these factors must be
taken into account when performing the test
(Carmon, Mor, and Goldberg 1976; Treede
et al. 1995; Tarkka and Treede 1993).
Activation of C fibers (conduction velocity,
0.4–
1.8 m/
second in humans) results in the
ultra-late components of LEPs. This response
has a positive peak maximal at the vertex and
a latency of about 1400 ms. It is unreliable in
recordings unless preferential A-
fiber block
suppresses the late component (Treede et al.
1995). The ultra-late wave is easily obtained if
the late component is absent because of disease selectively affecting Aδ and not C fibers.
Scalp topography and waveforms of the late
and ultra-
late LEPs are similar, suggesting
that they have the same cerebral generators
(Treede and Bromm 1988). Spatiotemporal
source analysis probably indicates that N2
is generated by activity mainly bilaterally
in secondary somatosensory cortex. A deep
dipole in the midline corresponding to the
location of the anterior cingulate gyrus is
primarily responsible for the P2 component.
Contralateral primary and secondary somatosensory cortex activity appears to be the generator of the middle latency (N1) component.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
40 Electrophysiology of Pain
LEPs are useful clinically to evaluate objectively the peripheral and central nociceptive
pathways in patients with neuropathic pain and
disturbances of pain perception, such as hypalgesia, hyperalgesia, allodynia, and spontaneous
pain (Antonini et al. 2000; Agostino et al. 2000a;
Agostino et al. 2000b). They have been used in
the assessment of various peripheral neuropathies, central nervous system disorders such as
syringomyelia, demyelinating disease, vascular
lesions, as well as various conditions such as
migraine and fibromyalgia. An excellent review
of the usefulness of LEPs was published by
Valeriani et al. in 2012. Some of these patients
have abnormal summation, or wind-up, consisting of the perception of continuous burning
pain instead of the normal individual sharp-
pricking painful sensations when a repetitive
1 Hz pinprick stimulus is applied to the skin.
LEPs indicated the involvement of Aβ and Aδ
fibers in a patient with polyneuropathy, muscle weakness, impaired sensation (cold, position, and vibratory), absence of conventional
tibial nerve somatosensory evoked potentials,
and large myelinated fiber loss on sural nerve
biopsy (Treede et al. 1995). In this patient,
LEPs showed small late responses, evidence
for impaired Aδ function, and large ultra-late
responses, with a peak latency of approximately
1600 ms, which is evidence for preserved function of C fibers.
In a case of polyneuropathy in which the
nerve conduction distance between the hand
and the foot was 0.8 m, the late and ultra-late
LEP responses corresponded to conduction
velocities of 16 m/second and 1.2 m/second,
respectively (Treede et al. 1995). This study
confirmed that Aδ peripheral afferents are
responsible for transmission of the late component and C-fiber activation for the ultra-late
component. This patient had marked wind-
up, despite hypalgesia in response to a single
pinprick stimulus, and there was unmasking
of the ultra-late component of the LEP. This
unmasking appeared to provide a cortical correlate for disinhibition of C-fiber responses to
noxious heat that occurs in persons who display
wind-up when A fibers are impaired (Treede
et al. 1995). Therefore, this technique can be
useful in the evaluation of nociceptive pathways in general. Also, it can help document
Aδ-fiber impairment with sparing of C-fiber
function. The selective loss of small unmyelinated fibers can only be documented when
683
A fibers are blocked or impaired, because
activity in C fibers produces the highly variable
ultra-late LEP response (Treede et al. 1995).
Pazzaglia et al. (2010) nicely showed impairment of Aδ afferents in patients with CMT1A
(Figure 40–
7). Garcia-
Larrea et al. (2010)
showed the difference in LEP amplitudes
in patients with non-organic pain (normal or
increased) as opposed to patients with neuropathic pain (reduced) (Figure 40–8).
CONTACT HEAT EVOKED
POTENTIALS
LEPs have not achieved wide use in clinical
practice due to their intrinsic technical difficulties (requiring skilled personnel to calibrate and operate the expensive equipment)
and pitfalls, which include the fact that they
are not a natural stimulus and can cause skin
burns and hyperpigmentation. Contact heat is
a natural stimulus, but previously could not be
used as a suitable stimulus for evoked potentials due to its slow rise time. Over the years,
heat-foil technology has been developed that
can elicit CHEPS as it has a rapid rising time
of 50°C/second (Chen, Niddam, and Arendt-
Nielsen 2001). Peak temperature is reached
360 ms after the offset of the 300-ms duration
stimulus. The stimuli are delivered at random
intervals; mean = 10 seconds. Forty trials are
averaged and recordings are performed as per
routine somatosensory evoked potential. The
largest activation occurs at the vertex area. To
generate well-formed waveforms, the stimulus
intensity has to be able to induce at least moderate pain in the subjects, with a VAS rating
of 6 or higher (Figure 40–9). This is generally
achieved with peak temperatures in the range
of 50°C. Four peaks become visible then: N450
(at T3), N550 (at Cz), P750 (at Cz), and P1000
(at Pz). This stimulus appears to activate both
Aδ and C fibers; it sometimes can induce two
types of sensations: a first sharp pain followed
by a second, duller type pain. The calculated
conduction velocities for the first peak (N550)
would fit Aδ fibers (10 m/second) and can be
generated at temperatures of 45°C. The later
components (around 1000 ms) would be the
result of C-
fiber activation (velocities estimated at 2–3 m/second) and are visible only
with higher peak temperatures around 52°C.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Foot
Hand
Face
EOG
T3-Fz
N 1 P2
N1
P2
Cz
N2
N2
20 µV
200 ms
EOG
T3-Fz
N1
Cz
N1
P2
N1
P2
P2
N2
N2
N2
Figure 40–7. LEPs recorded to foot, hand, and face stimulation in a CMT1A patient and in a control subject. Notice
that no LEP component is identifiable to foot stimulation in the patient and that the N2/P2 amplitude to hand stimulation is lower in the patient than in the healthy subject. Used with permission: Pazzaglia, C., C. Vollono, D. Ferraro, et al.
2010. “Mechanisms of neuropathic pain in patients with Charcot–Marie–Tooth 1A: A laser-evoked potential study.” Pain
149:379–85.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
EOG
With Allodynia/Hyperalgesia
EOG
Spontaneous only
EOG
Fz
Fz
Fz
Cz
Cz
Cz
Pz
Pz
Pz
ms
ms
ms
–
0
200 400 600
A: Pain sine materia
800 1000
0
200 400 600 800 1000
B: Neuropathic central pain
5 µV
+
0
200 400 600 800 1000
C: Neuropathic central pain
Figure 40–8. LEPs recorded in a patient with pain sine materia (A); in a patient with neuropathic pain and allodynia/
hyperalgesia (B); and in a patient with spontaneous neuropathic pain only (C). LEPs were obtained after stimulation of both
a painful and a non-painful zone. Notice that in patients with neuropathic pain, LEP amplitude is lower after stimulation of
the painful zone, as compared to the stimulation of a non-painful area. LEP amplitude reduction is larger in the patient with
spontaneous pain only than in the patient showing also allodynia/hyperalgesia. In the patient with pain sine materia, LEP
amplitude is similar after stimulation of both the painful and the non-painful zone. Used with permission: Garcia-Larrea,
L., P. Convers, M. Magnin, et al. 2002. “Laser-evoked potential abnormalities in central pain patients: The influence of
spontaneous and provoked pain.” Brain 125:2766–81.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
40 Electrophysiology of Pain
Amplitude (µV)
–10
685
Warm, nonpainful (I–2)
–5
0
5
0
Amplitude (µV)
–10
Slight pain (I–4)
–5
0
5
0
Amplitude (µV)
–15
–10
Moderate pain (I–6)
Cz/N550
–5
0
5
10
0
Cz/P1000
Cz/P750
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Figure 40–9. Contact heat evoked potentials. Vertex waveforms in relation to stimulus heat energy levels (I-2, I-4, I-6),
resulting in increasing pain sensation on verbal rating score. Amplitude increase correlated to increase of energy levels, and
the results also demonstrated the consistency and reproducibility between Study-I (dark) and Study-II (gray). Prominent
vertex components are marked: Cz/N550, Cz/P750, and Cz/P1000 at I-6 (moderate pain level). From Chen, A. C. N., D. M.
Niddam, and L. Arendt-Nielsen. 2001. “Contact heat evoked potentials as a valid mean to study nociceptive pathways in
human subjects.” Neuroscience Letters 316:79–82. By permission of Elsevier.
Reproducibility and reliability of CHEPS are
comparable to those of LEPs.
Varying the attentional target toward different properties of the stimulus did not cause any
significant change in CHEPS response amplitudes and latencies, suggesting that CHEPS
represent a reliable functional measure of the
nociceptive pathways (Le Pera et al. 2002).
CHEPS amplitudes correlate negatively
with age. Amplitudes and latencies of CHEPS
correlate with verbal pain scores: the higher
the rating, the shorter the N1 latency and
the higher the N1–
P1 amplitude (Chao
et al. 2007).
In a study performed on patients with
symptoms of sensory neuropathy compared
to controls, CHEPS were compared to other
methods used to evaluate small fibers—
the
histamine-induced skin flare response, intra-
epidermal fibers (IEF) count, and quantitative sensory testing. Amplitudes of Aδ evoked
potentials were reduced in patients, who
also showed reduced leg skin flare responses
and reduced IEF compared to controls. The
reduction in flare response and fiber count
correlated with the potential amplitude. The
authors concluded CHEPS provide a clinically
practical, noninvasive, and objective measure,
and can be a useful additional tool for the
assessment of sensory small-fiber neuropathy
(Atherton et al. 2007). Two children with congenital insensitivity to pain were tested: they
had normal flare response but absent cortical
heat evoked potentials, suggesting an abnormality in more proximal or central pain pathways (Facer et al. 2007).
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
686
Section 5: Assessment of Autonomic Function
In a study to evaluate trigeminal small-fiber
function, Truini et al. found contact heat stimuli
at 51°C evoked vertex potentials consisting of an
negative-positive (NP) complex similar to that
elicited by laser pulses, though with a latency
some 100 ms longer. Perioral stimulation
yielded higher pain intensity ratings, shorter
latency, and larger amplitude CHEPS than
supraorbital stimulation. Contact heat stimuli at
53°C evoked a blink-like response in the relaxed
orbicularis oculi muscle and a silent period in
the contracted masseter muscle. In patients
with facial neuropathic pain, the CHEPS abnormalities paralleled those seen with LEPs (Truini
et al. 2007).
A dipolar model explaining the scalp CHEPS
distribution is very similar to that previously
described to explain the topography of evoked
potentials to radiant heat stimulation by laser
pulses (Valeriani et al. 2002). Since laser stimuli
activate the nociceptive fibers, the strong similarity of the cerebral dipoles activated by contact heat stimuli and by laser pulses suggests
that only nociceptive inputs are involved in
the scalp CHEPS generation. Therefore, like
LEPs, CHEPS recording can reliably assess
nociceptive pathways.
There is evidence showing that CHEPS
evoked response amplitudes correlate negatively with age and the initial negative latency
correlates with gender, with shorter latencies noted in females. Pain intensity per
the verbal rating scale (VRS) was decreased
with aging and higher in females than males.
Higher VRS responses correlated positively
with higher CHEPS amplitude and a shorter
latency of the first negative peak. Thus, age-
related changes in thermal pain perception
and CHEPS should be considered when using
this modality of testing somatosensory function (Chao et al. 2007).
SUMMARY
Pain is a subjective experience in which the
patient’s emotional state has a major role, contributing to the challenge pain clinicians have
in quantifying and objectively evaluating this
common complaint. The multiplicity and complexity of the neural mechanisms that produce
chronic pain make the clinician’s task even
more challenging. During the last 20 years,
research in the assessment of the nociceptive
and autonomic systems has provided useful
tools for the diagnosis, treatment, and scientific investigation of neuropathic pain. QSTs
provide an accurate, reproducible assessment
of the sensory response to well-
delineated
controlled stimuli for evaluating the function of small myelinated and unmyelinated
fibers. These tests can be useful for documenting sensory disturbances that may occur
in patients with neuropathy who experience
hypalgesia, hyperalgesia, or allodynia. The
inclusion of autonomic tests in the evaluation
of some patients with neuropathic pain may
provide objective evidence of increased sympathetic tone, heightened somatosympathetic
reflexes, or sympathetic denervation. This
information may help the clinician diagnose
more accurately the particular type of pain
syndrome the patient has, so that the treatment may be better directed at the underlying mechanism. MCNG, primarily a research
tool, is a powerful method for directly studying primary afferent and sympathetic efferent
neural activity in patients with pain caused
by lesions of the nervous system. LEPs allow
clinicians and researchers to investigate
objectively functions of the peripheral and
central nociceptive pathways in patients with
neuropathic pain.
REFERENCES
Agostino, R., G. Cruccu, A. Romaniello, P. Innocenti, M.
Inghilleri, and M. Manfredi. 2000a. “Dysfunction of
small myelinated afferents in diabetic polyneuropathy, as assessed by laser evoked potentials.” Clinical
Neurophysiology 111:270–76.
Agostino, R., G. Cruccu, G. D. Iannetti, et al. 2000b.
“Trigeminal small-fibre dysfunction in patients with
diabetes mellitus: A study with laser evoked potentials and corneal reflex.” Clinical Neurophysiology
111:2264–67.
Antonini, G., F. Gragnani, A. Romaniello, et al. 2000.
“Sensory involvement in spinal-
bulbar muscular
atrophy (Kennedy’s disease).” Muscle and Nerve 23:
252–58.
Atherton, D. D., P. Facer, K. M. Roberts, et al. 2007. “Use
of the novel contact heat evoked potential stimulator (CHEPS) for the assessment of small fibre neuropathy: Correlations with skin flare responses and
intra-epidermal nerve fibre counts.” BMC Neurology
7(1):21.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
40 Electrophysiology of Pain
Attal, N., V. Gaude, L. Brasseur, et al. 2000. “Intravenous
lidocaine in central pain: A double-
blind, placebo-
controlled,
psychophysical
study.”
Neurology
54:564–74.
Backonja, M. M., N. Attal, R. Baron, et al. 2013. “Value of
quantitative sensory testing in neurological and pain
disorders: NeuPSIG consensus.” Pain 154(9):1807–19.
Beydoun, A., T. J. Morrow, J. F. Shen, and K.
L. Casey. 1993. “Variability of laser-
evoked potentials: Attention, arousal and lateralized differences.”
Electroencephalography and Clinical Neurophysiology
88:173–81.
Bromm, B. 1995. “Consciousness, pain, and cortical activity.” Advances in Pain Research and Therapy 22:35–59.
Campbell, J. N., R. A. Meyer, and S. N. Raja. 1992. “Is
nociceptor activation by alpha-1 adrenoreceptors the
culprit in sympathetically maintained pain?” American
Pain Society Journal 1:3–11.
Carmon, A., J. Mor, and J. Goldberg. 1976. “Evoked cerebral responses to noxious thermal stimuli in humans.”
Experimental Brain Research 25:103–7.
Casale, R., and M. Elam. 1992. “Normal sympathetic nerve
activity in a reflex sympathetic dystrophy with marked
skin vasoconstriction.” Journal of the Autonomic
Nervous System 41:215–19.
Chao, C. C., S. T. Hsieh, M. J. Chiu, M. T. Tseng, and Y.
C. Chang. 2007. “Effects of aging on contact heat-
evoked potentials: The physiological assessment of
thermal perception.” Muscle and Nerve 36(1):30–38.
Chelimsky, T. C., P. A. Low, J. M. Naessens, P. R. Wilson,
P. C. Amadio, and P. C. O’Brien. 1995. “Value of autonomic testing in reflex sympathetic dystrophy.” Mayo
Clinic Proceedings 70:1029–40.
Chen, A. C. N., D. M. Niddam, and L. Arendt-Nielsen.
2001. “Contact heat evoked potentials as a valid mean
to study nociceptive pathways in human subjects.”
Neuroscience Letters 316:79–82.
Claus, D., M. J. Hilz, and B. Neundorfer. 1990. “Thermal
discrimination thresholds: A comparison of different
methods.” Acta Neurologica Scandinavica 81:533–40.
Cline, M. A., J. Ochoa, and H. E. Torebjörk. 1989. “Chronic
hyperalgesia and skin warming caused by sensitized C
nociceptors.” Brain 112:621–47.
Cronin, K. D., R. L. Kirsner, and V. P. Fitzroy. 1982.
“Diagnosis of reflex sympathetic dysfunction. Use of
the skin potential response.” Anaesthesia 37:848–52.
Culp, W. J., J. Ochoa, M. Cline, and R. Dotson. 1989.
“Heat and mechanical hyperalgesia induced by capsaicin. Cross modality threshold modulation in human C
nociceptors.” Brain 112:1317–31.
Darian-Smith, I. 1984. “Thermal sensibility.” In Handbook
of physiology: A critical, comprehensive presentation of physiological knowledge and concepts, Vol.
3, The nervous system, eds. J. M. Brookhart, and V.
B. Mountcastle, 879–913. Bethesda, MD: American
Physiological Society.
Dotson, R. M. 1993. “Causalgia—
reflex sympathetic
dystrophy—
sympathetically maintained pain: Myth
and reality.” Muscle and Nerve 16:1049–55.
Dotson, R., J. Ochoa, M. Cline, P. Marchettini, and
D. Yarnitsky. 1992. “Intraneural microstimulation of
low threshold mechanoreceptors in patients with causalgia/RSD/SMP (abstract).” Abstracts—Society of
Neuroscience 18:290.
687
Dotson, R., J. Ochoa, M. Cline, W. Roberts, D. Yarnitsky,
and D. Simone. 1990. “Sympathetic effects on
human low threshold mechanoreceptors (abstract).”
Abstracts—Society for Neuroscience 16:1280.
Dyck, P. J., I. Zimmerman, D. A. Gillen, D. Johnson, J.
L. Karnes, and P. C. O’Brien. 1993. “Cool, warm, and
heat-pain detection thresholds: Testing methods and
inferences about anatomic distribution of receptors.”
Neurology 43:1500–8.
Dyck, P. J., J. L. Karnes, D. A. Gillen, P. C. O’Brien,
I. R. Zimmerman, and D. M. Johnson. 1990.
“Comparison of algorithms of testing for use in automated evaluation of sensation.” Neurology 40:1607–13.
Dyck, P. J., P. C. O’Brien, J. L. Kosanke, D. A. Gillen, and
J. L. Karnes. 1993. “A 4, 2, and 1 stepping algorithm
for quick and accurate estimation of cutaneous sensation threshold.” Neurology 43:1508–12.
Facer, P., D. D. Atherton, K. M. Roberts, et al. 2007. “A
new syndrome of congenital insensitivity to pain diagnosed by skin biopsy and contact heat evoked potentials.” Peripheral Nerve Society Meeting, Snowbird,
Utah, July 2007
Garcia-Larrea, L., P. Convers, M. Magnin, et al. 2002.
“Laser-evoked potential abnormalities in central pain
patients: The influence of spontaneous and provoked
pain.” Brain 125:2766–81.
Garcia-
Larrea, L. C. Perchet, C. Creac’h, et al. 2010.
“Operculo-insular pain (parasylvian pain): a distinct
central pain syndrome.” Brain 133(9):2528–39.
Gibson, S. J., S. A. LeVasseur, and R. D. Helme. 1991.
“Cerebral event-
related responses induced by CO2
laser stimulation in subjects suffering from cervicobrachial syndrome.” Pain 47:173–82.
Gold, M. S., D. M. White, S. C. Ahlgren, M. Guo, and J.
D. Levine. 1994. “Catecholamine-induced mechanical sensitization of cutaneous nociceptors in the rat.”
Neuroscience Letters 175:166–70.
Greenspan, J. D. 2001. “Quantitative assessment of neuropathic pain.” Current Pain and Headache Reports
5:107–13.
Gruener, G., and P. J. Dyck. 1994. “Quantitative sensory
testing: Methodology, applications, and future directions.” Journal of Clinical Neurophysiology 11:568–83.
Kazarians, H., E. Scharein, and B. Bromm. 1995. “Laser
evoked brain potentials in response to painful trigeminal nerve activation.” The International Journal of
Neuroscience 81:111–22.
Le Pera, D., M. Valeriani, D. Niddam, A. C. Chen, and
L. Arendt-Nielsen. 2002. “Contact heat evoked potentials to painful and non-painful stimuli: Effect of attention towards stimulus properties.” Brain Topography
15:115–23.
Levine, J. D., Y. O. Taiwo, S. D. Collins, and J. K. Tam.
1986. “Noradrenaline hyperalgesia is mediated
through interaction with sympathetic postganglionic
neurone terminals rather than activation of primary
afferent nociceptors.” Nature 323:158–60.
Low, P. A. 1993. “Autonomic nervous system function.”
Journal of Clinical Neurophysiology 10:14–27.
Maier C., R. Baron, T. R. Tölle, et al. 2010. “Quantitative
sensory testing in the German Research Network on
Neuropathic Pain (DFNS): Somatosensory abnormalities in 1236 patients with different neuropathic pain
syndromes.” Pain 150(3):439–50.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
688
Section 5: Assessment of Autonomic Function
Nygaard, O. P., R. Kloster, T. Solberg, and S. I. Mellgren.
2000. “Recovery of function in adjacent nerve roots
after surgery for lumbar disc herniation: Use of
quantitative sensory testing in the exploration of different populations of nerve fibers.” Journal of Spinal
Disorders 13:427–31.
Ochoa, J. 1986. “The newly recognized painful ABC
syndrome: Thermographic aspects.” Thermology
2:65–107.
Ochoa, J. L., D. Yarnitsky, P. Marchettini, R. Dotson, and
M. Cline. 1993. “Interactions between sympathetic
vasoconstrictor outflow and C nociceptor-
induced
antidromic vasodilatation.” Pain 54:191–96.
Ochoa, J., M. Cline, W. Comstock, et al. 1987. “Painful
syndrome newly recognized: Polymodal hyperalgesia
with cross modality threshold modulation and rubor
(abstract).” Abstracts—
Society for Neuroscience
13:189.
Pazzaglia, C., C. Vollono, D. Ferraro, et al. 2010
“Mechanisms of neuropathic pain in patients with
Charcot–Marie–Tooth 1A: A laser-evoked potential
study.” Pain 149:379–85.
Peripheral Neuropathy Association. 1993. “Quantitative
sensory testing: A consensus report from the Peripheral
Neuropathy Association.” Neurology 43:1050–52.
Price, D. D. 1988. Psychological and neural mechanisms of
pain, 18–49. New York: Raven Press.
Price, D. D., P. A. McGrath, A. Rafii, and B. Buckingham.
1983. “The validation of visual analogue scales as ratio
scale measures for chronic and experimental pain.”
Pain 17:45–56.
Roberts, W. J. 1986. “A hypothesis on the physiological
basis for causalgia and related pains.” Pain 24:297–311.
Rommel, O., M. Tegenthoff, U. Pern, M. Strumpf,
M. Zenz, and J. P. Malin. 1995. “Sympathetic skin
response in patients with reflex sympathetic dystrophy.” Clinical Autonomic Research 5:205–10.
Rossi, P., M. Serrao, G. Amabile, L. Parisi, F. Pierelli,
and G. Pozzessere. 2000. “A simple method for estimating conduction velocity of the spinothalamic
tract in healthy humans.” Clinical Neurophysiology
111:1907–15.
Sandroni, P., P. A. Low, T. Ferrer, T. L. Opfer-Gehrking,
C. L. Willner, and P. R. Wilson. 1998. “Complex regional
pain syndrome I (CRPS I): Prospective study and laboratory evaluation.” The Clinical Journal of Pain 14:282–89.
Sato, J., and E. R. Perl. 1991. “Adrenergic excitation of
cutaneous pain receptors induced by peripheral nerve
injury.” Science 251:1608–10.
Sato, J., S. Suzuki, T. Iseki, and T. Kumazawa. 1993.
“Adrenergic excitation of cutaneous nociceptors
in chronically inflamed rats.” Neuroscience Letters
164:225–28.
Schmelz, M., R. Schmid, H. O. Handwerker, and
H. E. Torebjork. 2000. “Encoding of burning pain
from capsaicin-treated human skin in two categories
of unmyelinated nerve fibres.” Brain 123:560–71.
Schmidt, R., M. Schmelz, C. Forster, M. Ringkamp,
E. Torebjork, and H. Handwerker. 1995. “Novel
classes of responsive and unresponsive C nociceptors
in human skin.” Journal of Neuroscience 15:333–41.
Schmidt, R., M. Schmelz, H. E. Torebjork, and
H. O. Handwerker. 2000. “Mechano-
insensitive
nociceptors encode pain evoked by tonic pressure to
human skin.” Neuroscience 98:793–800.
Serra, J., H. Bostock, R. Sola, et al. 2012. “Micro­
neurographic identification of spontaneous activity in
C-nociceptors in neuropathic pain states in humans
and rats.” Pain 153:42–55.
Shahani, B. T., J. J. Halperin, P. Boulu, and J. Cohen. 1984.
“Sympathetic skin response—A method of assessing
unmyelinated axon dysfunction in peripheral neuropathies.” Journal of Neurology, Neurosurgery, and
Psychiatry 47:536–42.
Spiegel, J., C. Hansen, and R. D. Treede. 2000. “Clinical
evaluation criteria for the assessment of impaired
pain sensitivity by thulium-laser evoked potentials.”
Clinical Neurophysiology 111:725–35.
Stanton-Hicks, M., W. Janig, S. Hassenbusch, J. D. Haddox,
R. Boas, and P. Wilson. 1995. “Reflex sympathetic
dystrophy: Changing concepts and taxonomy.” Pain
63:127–33.
Tarkka, I. M., and R. D. Treede. 1993. “Equivalent electrical source analysis of pain-related somatosensory
evoked potentials elicited by a CO2 laser.” Journal of
Clinical Neurophysiology 10:513–19.
Torebjork, E. 1993. “Human microneurography and intraneural microstimulation in the study of neuropathic
pain.” Muscle and Nerve 16:1063–65.
Torebjork, H. E., L. E. Lundberg, and R. H. LaMotte.
1992. “Central changes in processing of mechanoreceptive input in capsaicin-
induced secondary
hyperalgesia in humans.” The Journal of Physiology
448:765–80.
Treede, R. D., and B. Bromm. 1988. “Reliability and validity
of ultra-late cerebral potentials in response to C-fibre
activation in man.” In Proceedings of the Vth World
Congress on Pain, eds. R. Dubner, G. F. Gebhart, and
M. R. Bond, 567–73. Amsterdam: Elsevier.
Treede, R.-D., J. Lorenz, K. Kunze, and B. Bromm. 1995.
“Assessment of nociceptive pathways with laser-
evoked potentials in normal subjects and patients.”
Advances in Pain Research Therapy 22:377–92.
Truini, A., F. Galeotti, E. Pennisi, F. Casa, A. Biasiotta,
and G. Cruccu. 2007. “Trigeminal small-fibre function assessed with contact heat evoked potentials in
humans.” Pain 132(1–2):102–7.
Valeriani, M., D. Le Pera, D. Niddam, A. C. Chen, and
L. Arendt-Nielsen. 2002. “Dipolar modelling of the
scalp evoked potentials to painful contact heat stimulation of the human skin.” Neuroscience Letters.
318:44–48.
Valeriani, M., C. Pazzaglia, G. Cruccu, and A. Truini.
2012 “Clinical usefulness of laser evoked potentials.”
Clinical Neurophysiology 42:345–53.
Vallbo, A. B., K. E. Hagbarth, H. E. Torebjork, and B.
G. Wallin. 1979. “Somatosensory, proprioceptive, and
sympathetic activity in human peripheral nerves.”
Physiological Reviews 59:919–57.
Verdugo, R., and J. L. Ochoa. 1992. “Quantitative somatosensory thermotest. A key method for functional
evaluation of small calibre afferent channels.” Brain
115:893–913.
Wahren, L. K., and E. Torebjork. 1992. “Quantitative sensory tests in patients with neuralgia 11–25 years after
injury.” Pain 48:237–44.
Wahren, L. K., E. Torebjork, and B. Nystrom. 1991.
“Quantitative sensory testing before and after regional
guanethidine block in patients with neuralgia in the
hand.” Pain 46:23–30.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
40 Electrophysiology of Pain
Yarnitsky, D., D. A. Simone, R. M. Dotson, M. A. Cline,
and J. L. Ochoa. 1992. “Single C nociceptor responses
and psychophysical parameters of evoked pain: Effect
of rate of rise of heat stimuli in humans.” The Journal
of Physiology 450:581–92.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Willis, W. D., Jr. 1995. “From nociceptor to cortical activity.” Advances in Pain Research and Therapy 22:1–19.
Wu, Q., L. Garcia-
Larrea, P. Mertens, A. Beschet, M.
Sindou, and F. Mauguiere. 1999. “Hyperalgesia with
reduced laser evoked potentials in neuropathic pain.”
Pain 80:209–14.
689
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
Copyright © 2016. Oxford University Press, Incorporated. All rights reserved.
Clinical Neurophysiology, Oxford University Press, Incorporated, 2016. ProQuest Ebook Central,
http://ebookcentral.proquest.com/lib/waketech-ebooks/detail.action?docID=4545340.
Created from waketech-ebooks on 2020-11-21 18:12:40.
")