Review
Antinuclear Antibodies: Marker of Diagnosis and
Evolution in Autoimmune Diseases
Laboratory Medicine 49:3:e62-e73
DOI: 10.1093/labmed/lmy016
ABSTRACT
Antinuclear antibodies (ANAs) are autoantibodies that attack selfproteins within cell nucleus structures; their presence in serum may
indicate an autoimmune disease. Also, positive ANA test results have
been obtained in chronic infectious diseases, cancers, medicationrelated adverse events, and even healthy individuals. As a result, a
correct interpretation of the presence of ANAs is needed.
Identification of ANAs subtypes is an important part of clinical
immunology. The presence of ANAs in patient blood specimens is
detected using a cell-line substrate from human laryngeal carcinoma
(HEp-2 cells). On this substrate, ANAs will bind specific antigens,
which will lead to a suggestive fluorescent emission. The fluorescence
Antibodies are proteins produced by lymphocytes B and
play a key role in the activity of the immune system. These
proteins have the capacity to recognize foreign antigens,
or proteins from external structures such as viruses, bacteria, or other germs. In this way, antibodies are a way for
the body to defend itself from infectious organisms. After
Abbreviations
ANAs, antinuclear antibodies; SLE, systemic lupus erythematosus; SS,
scleroderma; SjS, Sjögren syndrome; MCTD, mixed connective tissue
disease; PM, polymyositis; RA, rheumatoid arthritis; PBC, primary biliary
cirrhosis; ENAs, extractable nuclear antigens; dsDNA, double-stranded
DNA; Sm, Smith antigen; CTDs, connective tissue diseases; IFA, indirect
immunofluorescence assay; ELISA, enzyme-linked immunosorbent assay;
PML, promyelocytic leukemia protein; SS-CREST, calcinosis, Raynaud
phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia;
snoRNP, small nucleolar ribonucleoprotein; NORs, nucleolar organizing
regions; RNAP I, RNA polymerase I.
The Oncology Institute, “Prof. Dr. Ion Chiricuță”,2University of Medicine
and Pharmacy “Iuliu Hațieganu”3Emergency Clinical Hospital for Children,
Cluj-Napoca—Pediatrics II Department,4Emergency Clinical Hospital for
Children, Cluj-Napoca—Pediatrics I Department, and 5Regional Institute
of Gastroenterology and Hepatology “Octavian Fodor” Cluj-Napoca, ClujNapoca, Romania
patterns visualized under the fluorescence microscope can be
correlated with certain subtypes of ANA and certain autoimmune
diseases.
Depending on the subtype of ANA present in the serum and the targeted
antigen, several staining patterns are reported, namely, nuclear patterns,
nucleolar patterns, cell cycle patterns, or cytoplasmatic patterns.
Identification of a certain pattern can lead to diagnosis of a certain
autoimmune disease.
Keywords: ANA, immunofluorescence, HEp-2, pattern,
autoimmunity, marker
recognizing the antigens, antibodies start to recruit specialized cells and proteins, which will lead to activation of the
inflammation cascade—the response of the organism to
defend itself.1,2
In some pathological conditions, some of these antibodies produced by the human body attack proteins from
self-structures. These are called autoantibodies and they
mistakenly identify normal structures as being foreign and
dangerous. This abnormal immunological response leads
to a type of systemic inflammation that leads the organism
to fight against itself. Most human bodies contain autoantibodies but in low titers, which represents a normal state of
health. In cases of high autoantibody titers, an autoimmune
disease can be suspected. Antinuclear antibodies (ANAs)
are autoantibodies that attack self-proteins within cell
nucleus structures.1-3
1
*To whom correspondence should be addressed.
surgenel@yahoo.com
e62
A positive test result for ANAs may indicate the presence
of a systemic autoimmune disease, such as systemic lupus
erythematosus (SLE), drug-induced lupus, scleroderma (SS),
Sjögren syndrome (SjS), mixed connective tissue disease
(MCTD), polymyositis (PM)/dermatomyositis, rheumatoid
arthritis (RA), oligoarticular juvenile chronic arthritis, polyarteritis nodosum, or an organ-specific autoimmune disease
© American Society for Clinical Pathology 2018. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Lucia M. Sur, PhD,2,4 Emanuela Floca, PhD,2,5 Daniel G. Sur, PhD,1,2
Marius C. Colceriu, BSc,2 Gabriel Samasca, MD,3 Genel Sur, MD, PhD2,3,*
Review
such as Grave disease, Hashimoto thyroiditis, autoimmune
hepatitis, primary biliary cirrhosis (PBC), inflammatory bowel
disease, or idiopathic pulmonary fibrosis.
Types of ANA
The many known subtypes of ANA can be grouped in 2
main categories, namely, autoantibodies against DNA and
histones, and autoantibodies against extractable nuclear
antigens (ENAs). The first group includes antibodies against
dsDNA (double-stranded DNA) and against histones.
Antibodies against dsDNA in high titers are considered to
confirm SLE diagnosis. Antibodies against histones indicate
drug-induced SLE. The second group includes antibodies
against Smith antigen (Sm), wich are specific for SLE, anti–
SS-A/Ro, and anti–SS-B/La (these 2 types are specific for
Sjögren syndrome, subacute cutaneous SLE, and neonatal
lupus syndrome), anticentromere (considered specific for
limited cutaneous SS), Jo-1 (considered specific for PM),
anti–U3-RNP, and Scl-70 (these final 2 are considered specific for SS). In recent years, more antigens attacked by
ANA, such as topoisomerase-I, centromere protein B, and
RNA-polymerase I-III, have been described in the literature.4-7 Even if most of them are disease specific, a statistically significant overlap still exists.
Tests for ANA Detection
Screening tests are used for detection of ANAs in patient
serum. The presence of ANAs in blood represents an important
criterion for the diagnosis of connective tissue diseases (CTDs).
Also, identifying ANA subtypes may be useful in determining
a specific CTD. Despite that there are many tests available
for detection of ANAs, the ones most commonly used in daily
www.labmedicine.com
The ELISA test is based on the interaction between antibodies existing in the blood specimen, a preprepared antigen,
and special antibodies that are able to stick to the previous 2 components of the final complex, which leads to a
color change in the final solution that is proportional to the
quantity of ANAs. The results can be positive, equivocal, or
negative, based on the determination of the optical density
value of the solution.4,8,10,11
IFA is the standard ANA testing method because it is easy
to perform, inexpensive, and has high specificity and sensitivity. The presence of ANAs in patient blood specimens is
detected using a cell-line substrate from human laryngeal
carcinoma (HEp-2 cells). Microscope slides are coated with
a monolayer of Hep-2 cells because those cells are a sensitive substrate for ANAs. Those cells confer the following
advantages: they are the most sensitive substrate used at the
moment, they offer the possibility to identify many patterns,
they have better specificity than other methods due to their
human origin, they have large nuclei so more details can
be seen, all nuclei can be seen, antigens that are produced
only in cell division can be more easily identified due to high
cell-division rates, and the distribution of antigens is uniform.
These slides are incubated with blood specimens, and if the
antibodies are present, they will bind to the nuclear antigens.
The antigen-antibody complex can be visualized as a distinct
pattern in fluorescence microscopy, after adding a fluorescent-labeled antibody that is able to adhere to the complex.
The amount of ANAs in the serum specimen is established by
determination of antibody titers. ANA titer is determined by
diluting the specimens in a buffered solution. Screening tests
for ANAs use 1:40 and 1:160 dilutions. If the pattern can be
seen in both dilutions, the specimen will continue to be diluted
until staining can no longer be seen. The end dilution corresponds to the antibody titer. It is generally considered that a
titer of 1:160 is significant for the diagnosis of CTDs. The fluorescence patterns visualized under fluorescence microscope
can be correlated with certain autoimmune diseases.2,4,8,11-14
Hep-2 Nuclear Patterns
These staining patterns appear as a result of the adhesion
of autoantibodies to certain nuclear antigens. Although
ANAs are specific to nuclear antigens, in some cases, cytoplasmic patterns correlated with autoantibodies against
Lab Medicine 2018;49;e62–e73 DOI: 10.1093/labmed/lmy016
e63
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
ANAs also have been detected in chronic infectious diseases, including viral infections (parvovirus, hepatitis C),
tuberculosis, parasitic infections (schistosomiasis), and bacterial endocarditis. Other factors that yield ANA-positive test
results include cancers, markers of the future development
of autoimmune disease, certain medications, and having
relatives with an autoimmune disease. Also, some healthy
persons test positive for ANA: 2% of healthy young women
can have a positive test result.1-3
practice are the indirect immunofluorescence assay (IFA) and
enzyme-linked immunosorbent assay (ELISA).4,8,9
Review
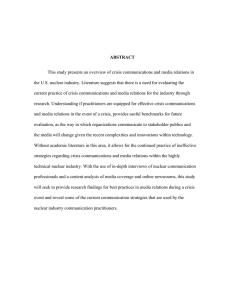
Smooth nuclear membrane pattern in serum of patient with polymyositis.
cytoplasmic antigens can also be visualized. Sometimes, a
mixed pattern can be observed. Cases in which mitosis-associated patterns may be observed are less common.
Smooth nuclear membrane pattern
This pattern is characterized by an intense linear fluorescence represented by the nuclear membrane and a less-intense homogeneous fluorescent appearance of the nucleus.
In anaphase and metaphase, the chromatin plate result is
negative, and greater fluorescent intensity can be seen at
the contact between cells. In this pattern, the nucleoli cannot
be seen. A fine membranous fluorescence surrounds newly
formed nuclei in telophase. The antigens associated with this
pattern are lamins A, B1, B2, and C, as well as lamin-associated proteins such as LAP 1A and LAP 2. This pattern has
been observed in SLE (Image 1), SS, chronic active hepatitis,
seronegative arthritis, and chronic fatigue syndrome.14-16
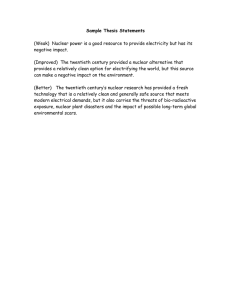
Punctate nuclear membrane pattern
In this pattern, also known as nuclear membrane pores,
the nuclear membrane presents granular staining in interphase cells. In anaphase and metaphase, no chromosomal
staining can be visualized. The contact surfaces of adjacent
e64 Lab Medicine 2018;49;e62–e73
DOI: 10.1093/labmed/lmy016
nuclear membranes emit more powerful fluorescent signals.
Frequently, this aspect is associated with mitochondrial
antibodies. This pattern can be observed in polymyositis
(Image 2) and PBC. In patients with PBC, if testing for
anti-Gp210 antibodies yields a positive result, the disease
is more aggressive. The most frequent antigen is Gp210,
which is a glycoprotein of 210 kDa from nuclear pore complexes. These pores play an important role in substances
movement between the cytoplasm and the nucleus. Another
antigen identified in this pattern is nucleoporin p62.14,17-19
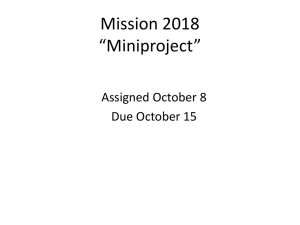
Homogeneous nuclear pattern
Uniform staining across all nucleoplasm is seen in this
pattern. The intensity of fluorescence depends on the titer
of antibodies in the serum. Sometimes, the nuclear rim can
be visualized as a more intense fluorescent emission of
the nucleus inner edge. In mitotic cells, chromatin mass is
often more intensely stained. Nucleolar staining may yield
a positive or negative result and, in some cases, a peripheal nucleolar emission can be observed. Autoantibodies
are directed against antigens from dsDNA, histones,
or nucleosomes. Although anti-Ku antibodies are more
commonly associated with a speckled pattern, in some
cases, they are able to show a homogeneous aspect. This
www.labmedicine.com
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 1
Review
Punctate nuclear membrane pattern in serum of patient with polymyositis.
Image 3
Homogeneous nuclear pattern in serum of patient with systemic lupus erythematosus.
pattern is common in SLE (Image 3), RA, lupus induced
by hydralazine and procainamide, juvenile chronic arthritis,
and SS.14,20-22
Nuclear matrix/large speckled pattern
A network of large speckles with a sponge-like aspect characterizes this pattern. Chromatin is not stained in mitotic
cells (anaphase, telophase, or metaphase). Nucleoli can
be stained or unstained. The nuclear matrix represents a
www.labmedicine.com
structure made from insoluble proteins resistant to RNAase,
DNAase, and high salt treatment. In this pattern, the antigens are heterogeneous ribonuclear proteins. In patients
with SLE (Image 4), MCTD, and RA, the autoantigens are
represented by hnRNP-A1, hnRNP-A2, hnRNP-B1, and
hnRNP-B2. In SS, autoantigens hnRNP-C1, hnRNP-C2, and
hnRNP-I have been detected. Usually, nuclear matrix pattern is reported in MCTD but it may also occur in RA, SS,
and SLE.14,23,24
Lab Medicine 2018;49;e62–e73 DOI: 10.1093/labmed/lmy016
e65
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 2
Review
Nuclear matrix/large speckled pattern in serum of patient with systemic lupus erythematosus.
Coarse speckled
This pattern is characterized by the presence of dense,
intermediate-sized speckles and large speckles. The nucleoli are unstained. Cells in mitosis are without staining of
the chromatin mass. The antigens identified in this pattern
are ribonucleoproteins Sm (U2, U4, U5, U6) and U1RNP.
Sm autoantibodies and U1-snRNP (small nuclear ribonucleoprotein) are markers for SLE and MCTD. U2-RNPs
are presented in SS-PM overlap, MCTD, SLE, psoriasis
(Image 5), and Raynaud phenomenon. In SS and SjS,
researchers have identified U4-snRNP and U6-snRNP
autoantibodies.14,25,26
Fine speckled
Also known as fine granular, this pattern is characterized by
fine, tiny speckles emission of interphase nuclei, with a uniform distribution. Nucleoli are mainly unstained; however, in
cases of positive anti–SS-B or anti-Ku, some nucleoli may
be visualized. Chromatin is not observed in mitotic cells.
e66 Lab Medicine 2018;49;e62–e73
DOI: 10.1093/labmed/lmy016
Antigens identified in this pattern are nuclear proteins such as
SSA, SSB, Ku, Ki, RNA polymerases II and III, and Mi-2. The
diseases associated with this pattern are SLE, SjS, myositis, MCTD, and SS. As many as one-fourth of patients with
dermatomyositis (Image 6) present autoantibodies against
Mi-2.14,27-29
Dense fine speckled
In interphase, characteristic for this pattern are speckles
of various size, distribution, and brightness (Image 7).
Nucleoli present no staining. Another highly characteristic aspect is the presence of some denser and looser
areas of speckles. Mitotic cells present intense speckled
fluorescence of the chromosomes. Associated antigens
may be LEDGF-p75 (lens epithelium–derived growth factor
75). The exclusive presence of LEDGF-p75 antibodies in
the specimen may be useful to identify patients who have
no rheumatologic disease, even if the IFA test result is
positive.14,30
www.labmedicine.com
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 4
Review
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 5
Coarse speckled pattern in serum of patient with psoriasis.
Image 6
Fine speckled pattern in serum of patient with dermatomyositis.
www.labmedicine.com
Lab Medicine 2018;49;e62–e73 DOI: 10.1093/labmed/lmy016
e67
Review
Dense fine speckled pattern in interphase in patient serum.
Few nuclear dots pattern
Centromere pattern
An average of 2 (1–6) discrete dots are visualized in
interphase. Frequently, these dots are presented near
the nucleolus and are known as coiled bodies or Cajal
bodies. Those dots represent a distinct pattern from the
multiple nuclear dots pattern, despite being found in similar clinical conditions. Antigens identified in this fluorescent aspect are proteins (80 kDa) designated p80-coilin.
Particles are associated with fibrillarin and are presumed
to have a role in snRNP maturation and transport.
Clinical associations: chronic active hepatitis, PBC
and, in rare occasions, collagen vascular diseases
(Image 8).14,31,32
In interphase, discrete coarse speckles (40–60/cell) spread
over the entire nucleus are observed. A block of closely
associated speckles is found in the chromatin mass of
mitotic cells. Antigens targeted by autoantibodies found in
the centromere pattern include CENP-A, -B, -C, -D, -E, -G,
and -H. This pattern can be present in limited cutaneous
SS-CREST (calcinosis, Raynaud phenomenon, esophageal
dysmotility, sclerodactyly, and telangiectasia; Image 10),
PBC and, in rare instances, SjS.35,36
Multiple nuclear dots
This pattern is similar to the few-nuclear-dots pattern, but
the number of dots is variable, namely, from 6 to 20 per cell
(an average of 10/cell). Also, the dots are of variable size. In
mitotic cells, the emission is visualized in the cell periphery.
More than 30% of patients with PBC are associated with
this pattern. Other pathological conditions associated are
SjS (Image 9) and, in rare occasions, SLE. Autoantibodies
are directed against nuclear multiprotein complexes that
include promyelocytic leukemia protein (PML), Sp-100 protein, and NDP53.33,34
e68 Lab Medicine 2018;49;e62–e73
DOI: 10.1093/labmed/lmy016
Hep-2 Nucleolar Patterns
Nucleolar homogeneous
This pattern involves diffuse, homogeneous fluorescence of
the entire nucleolus, with weak, fine granular staining of the
nucleoplasm. In mitotic cells, chromatin mass is unstained;
however, diffuse cytoplasmic emission is seen. PM-Scl 75
and PM-Scl 100 represent antigens associated with this
pattern and are found in patients with myositis-scleroderma
overlap syndrome (25%–50% of patients). Another antigen
identified is Rpp25, which is a part of the Th/To complex
and is associated with SS (Image 11), (4%–10% of patients
with limited cutaneous form). Rpp25 have also been
reported in SLE, RA, and polymyositis.14,35,37,38
www.labmedicine.com
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 7
Review
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 8
Few-nuclear-dots pattern in serum of patient with collagen vascular disease.
Image 9
Multiple-nuclear-dots pattern in serum of patient with Sjögren syndrome.
www.labmedicine.com
Lab Medicine 2018;49;e62–e73 DOI: 10.1093/labmed/lmy016
e69
Review
Centromere pattern in serum of patient with limited cutaneous SS-CREST (calcinosis, Raynaud phenomenon, esophageal dysmotility,
sclerodactyly, and telangiectasia).
Image 11
Nucleolar homogeneous pattern in serum of patient with scleroderma.
e70 Lab Medicine 2018;49;e62–e73
DOI: 10.1093/labmed/lmy016
www.labmedicine.com
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 10
Review
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Image 12
Nucleolar clumpiness in serum of patient with scleroderma.
Image 13
Nucleolar speckled/punctated pattern in serum of patient with systemic lupus erythematosus.
www.labmedicine.com
Lab Medicine 2018;49;e62–e73 DOI: 10.1093/labmed/lmy016
e71
Review
Nucleolar clumpiness
Nucleolar speckled/punctated
Distinct grains with dense distribution are visualized in the
nucleoli and are frequently associated with fine speckled
nucleoplasmic emission. In metaphase cells, bright spots
corresponding to nucleolar organizing regions (NORs) are
usually seen within the chromatin body. Regarding antigens (RNAP I/NOR), RNAP I (RNA polymerase I) complex is
located inside the nucleoli, and RNAP II and III are located
in the nucleoplasm. Due to certain common polypeptides, a
cross-reaction between RNAP I, II, and III may by possible.
The nucleolar speckled pattern has high specificity for SS
(4%–20%), which is often associated with kidney and heart
involvement. Other clinical associations are SLE (Image 13),
MCTD, and RA.35,41,42
As many as 100 autoantibodies are incriminated in the determination of overt 35 IFA patterns. In addition to nuclear
and nucleolar patterns, cytoplasmic patterns have also
been described. In several cases, these patterns are mixed
due to similar antigenic structures.14
Positive results of ANA testing must be interpreted only in a
clinical context because of the possibility of a positive test
result in a healthy person, especially in elderly people or in
pathological conditions other than autoimmune diseases. In the
future it will be important to develop IF methods, to improve the
accuracy of discrimination between healthy people who test
ANA positive and patients with autoimmune disease LM.
References
1. Antinuclear Antibodies (ANA). American College of Rheumatology website.
https://www.rheumatology.org/I-Am-A/Patient-Caregiver/DiseasesConditions/Antinuclear-Antibodies-ANA. Accessed April 28, 2018.
2. Medical definition of antinuclear antibody. MedicineNet website. https://
www.medicinenet.com/script/main/art.asp?articlekey=6709. Accessed
April 28, 2018.
3. Patient education: Antinuclear antibodies (ANA) (Beyond the Basics).
Uptodate website. https://www.uptodate.com/contents/antinuclearantibodies-ana-beyond-the-basics. Accessed April 28, 2018.
4. Kumar Y, Bhatia A, Minz RW. Antinuclear antibodies and their detection
methods in diagnosis of connective tissue diseases: a journey revisited.
Diagn Pathol. 2009;4:1.
5. Kavanaugh A, Tomar R, Reveille J, Solomon DH, Homburger HA.
Guidelines for clinical use of the antinuclear antibody test and tests
for specific autoantibodies to nuclear antigens. American College of
Pathologists. Arch Pathol Lab Med. 2000;124(1):71–81.
6. Fishbein E, Alarcon-Segovia D, Vega JM. Antibodies to histones in
systemic lupus erythematosus. Clin Exp Immunol. 1979;36(1):145–150.
Conclusions
IFA is the standard ANA testing method because it is easy
to perform, inexpensive, and offers high specificity and
sensitivity. Also, it has the advantage that the patterns visualized under fluorescence microscope using this method
can be correlated with certain autoimmune diseases. These
patterns are a result of the adhesion of ANAs to nuclear
antigenic structures—this is why they may be associated
with certain autoantibodies and certain clinical conditions.
Although the IFA presents no organ specificity, it is an
important step in the investigation and diagnosis of
e72 Lab Medicine 2018;49;e62–e73
DOI: 10.1093/labmed/lmy016
7. Tan EM, Kunkel HG. Characteristics of a soluble nuclear antigen
precipitating with sera of patients with systemic lupus erythematosus. J
Immunol. 1966;96(3):464–471.
8. Antinuclear Antibody. Medscape website. https://emedicine.medscape.
com/article/2086616-overview#a4. Accessed April 28, 2018.
9. Granito A, Muratori P, Quarneti C, Pappas G, Cicola R, Muratori L.
Antinuclear antibodies as ancillary markers in primary biliary cirrhosis.
Expert Rev Mol Diagn. 2012;12(1):65–74.
10. González-Buitrago JM, González C. Present and future of the
autoimmunity laboratory. Clin Chim Acta. 2006;365(1-2):50–57.
11. Emlen W, O’Neill L. Clinical significance of antinuclear antibodies:
comparison of detection with immunofluorescence and enzyme-linked
immunosorbent assays. Arthritis Rheum. 1997;40(9):1612–1618.
12. Lightfoote MM, Chirmule N, Homburger HA, et al. Quality Assurance
of Laboratory Tests for Autoantibodies to Nuclear Antigens: (1)
Indirect Fluorescence Assay for Microscopy and (2) Microtiter Enzyme
Immunoassay Methods. Approved Guideline–Second Edition. Wayne,
PA: Clinical and Laboratory Standards Institute. 2006;26:13.
www.labmedicine.com
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
Clustered granules are observed in the nucleoli.
Nucleoplasm is not stained; however, coiled bodies may
be seen as nuclear dots. In mitotic cells, chromatin mass is
stained. This pattern has a high specificity (5% of patients)
for SS (Image 12) and may be detected in pulmonary
hypertension. It has been also associated with hepatocellular carcinoma. The identified antigen is fibrillarin, which is a
component of snoRNP (small nucleolar ribonucleoprotein)
that includes U3snoRNP.39,40
autoimmune diseases. ANAs can also be considered
markers of evolution and prognosis, which is why the
possibility of correlation between IF patterns and certain autoantibodies conveys a major advantage in clinical evaluation. For example, it has been observed that
patients with juvenile idiopathic arthritis who test ANA
positive present similar disease characteristics and more
frequently develop iridocyclitis, compared with those who
test ANA negative.
Review
15. AC-11 – Smooth nuclear envelope. International Consensus on ANA
Patterns (ICAP) website. https://www.anapatterns.org/view_pattern.
php?pattern=11. Accessed April 28, 2018.
30. AC-2 – Nuclear dense fine speckled. International Consensus on ANA
Patterns (ICAP) website. https://www.anapatterns.org/view_pattern.
php?pattern=2. Accessed April 28, 2018.
16. Konstantinov K, Foisner R, Byrd D, et al. Integral membrane proteins
associated with the nuclear lamina are novel autoimmune antigens of
the nuclear envelope. Clin Immunol Immunopathol. 1995;74(1):89–99.
31. Fujimoto M, Kikuchi K, Tamaki T, et al. Distribution of anti-p80-coilin
autoantibody in collagen disease and various skin diseases. Br J
Dermatol. 1997;137(6):916–920.
17. AC-12 – Punctuate nuclear envelope. International Consensus on ANA
Patterns (ICAP) website. https://www.anapatterns.org/view_pattern.
php?pattern=12. Accessed April 28, 2018.
32. Ogg SC, Lamond AI. Cajal bodies and coilin–moving towards function.
J Cell Biol. 2002;159(1):17–21.
18. Dagenais A, Bibor-Hardy V, Senécal JL. A novel autoantibody causing a
peripheral fluorescent antinuclear antibody pattern is specific for nuclear
pore complexes. Arthritis Rheum. 1988;31(10):1322–1327.
19. Nesher G, Margalit R, Ashkenazi YJ. Anti-nuclear envelope antibodies:
clinical associations. Semin Arthritis Rheum. 2001;30(5):313–320.
20. Holborow EJ, Weir DM, Johnson GD. A serum factor in
lupus erythematosus with affinity for tissue nuclei. Br Med J.
1957;2(5047):732–734.
21. van Venrooij W, Maini R. Manual of Biological Markers of Disease.
Dordrecht: Springer Netherlands; 1996.
22. Isenberg D, Smeenk R. Clinical laboratory assays for measuring antidsDNA antibodies. Where are we now? Lupus. 2002;11(12):797–800.
23. Salden MH, Van Eekelen CA, Habets WJ, Vierwinden G, Van de Putte
LB, Van Venrooy WJ. Anti-nuclear matrix antibodies in mixed connective
tissue disease. Eur J Immunol. 1982;12(9):783–786.
24. Staněk D, Vencovský J, Kafková J, Raška I. Heterogenous nuclear RNP
C1 and C2 core proteins are targets for an autoantibody found in the
serum of a patient with systemic sclerosis and psoriatic arthritis. Arthritis
Rheum. 1997;40(12):2172–2177.
25. Beck J. Variations in the morphological patterns of “autoimmune”
nuclear fluorescence. Lancet. 1961;277(7188):1203–1205.
26. Craft J, Mimori T, Olsen TL, Hardin JA. The U2 small nuclear
ribonucleoprotein particle as an autoantigen. Analysis with sera from
patients with overlap syndromes. J Clin Invest. 1988;81(6):1716–1724.
27. AC-4 – Nuclear fine speckled. International Consensus on ANA
Patterns (ICAP) website. https://www.anapatterns.org/view_pattern.
php?pattern=4. Accessed April 28, 2018.
28. Wang J, Satoh M, Kabir F, et al. Increased prevalence of autoantibodies
to Ku antigen in African American versus white patients with systemic
lupus erythematosus. Arthritis Rheum. 2001;44(10):2367–2370.
www.labmedicine.com
33. Zuber M, Heyden TS, Lajous-Petter AM. A human autoantibody
recognizing nuclear matrix-associated nuclear protein localized in dot
structures. Biol Cell. 1995;85(1):77–86.
34. Sternsdorf T, Guldner HH, Szostecki C, Grötzinger T, Will H.
Two nuclear dot-associated proteins, PML and SplOO, are often
co-autoimmunogenic in patients with primary biliary cirrhosis. Scand J
Immunol. 1995;42(2):257–268.
35. Buchner C, Bryant C, Eslami A, Lakos G. Anti-nuclear antibody
screening using HEp-2 cells. J Vis Exp. 2014;88:e51211.
36. AC-3 – Centromere. International Consensus on ANA Patterns (ICAP)
website. https://www.anapatterns.org/view_pattern.php?pattern=3.
Accessed April 28, 2018.
37. Raijmakers R, Renz M, Wiemann C, et al. PM-Scl-75 is the main
autoantigen in patients with the polymyositis/scleroderma overlap
syndrome. Arthritis Rheum. 2004;50(2):565–569.
38. Reichlin M, Maddison PJ, Targoff I, et al. Antibodies to a nuclear/
nucleolar antigen in patients with polymyositis overlap syndromes. J Clin
Immunol. 1984;4(1):40–44.
39. Yang JM, Hildebrandt B, Luderschmidt C, Pollard KM. Human scleroderma
sera contain autoantibodies to protein components specific to the U3 small
nucleolar RNP complex. Arthritis Rheum. 2003;48(1):210–217.
40. Ochs RL, Lischwe MA, Spohn WH, Busch H. Fibrillarin: a new
protein of the nucleolus identified by autoimmune sera. Biol Cell.
1985;54(2):123–133.
41. Whitehead CM, Winkfein RJ, Fritzler MJ, Rattner JB. ASE-1: a novel
protein of the fibrillar centres of the nucleolus and nucleolus organizer
region of mitotic chromosomes. Chromosoma. 1997;106(8):493–502.
42. Imai H, Fritzler MJ, Neri R, Bombardieri S, Tan EM, Chan EK.
Immunocytochemical characterization of human NOR-90 (upstream
binding factor) and associated antigens reactive with autoimmune
sera. Two MR forms of NOR-90/hUBF autoantigens. Mol Biol Rep.
1994;19(2):115–124.
Lab Medicine 2018;49;e62–e73 DOI: 10.1093/labmed/lmy016
e73
Downloaded from https://academic.oup.com/labmed/article-abstract/49/3/e62/5032495 by guest on 21 March 2020
14. Bradwell A, Hughes R. Atlas of HEp-2 Patterns. Birmingham, England:
Binding Site; 2007.
29. Mimori T, Akizuki M, Yamagata H, Inada S, Yoshida S, Homma M.
Characterization of a high molecular weight acidic nuclear protein
recognized by autoantibodies in sera from patients with polymyositisscleroderma overlap. J Clin Invest. 1981;68(3):611–620.
13. Greidinger EL, Hoffman RW. Antinuclear antibody testing: methods,
indications, and interpretation. Lab Med. 2003;34:113–118.