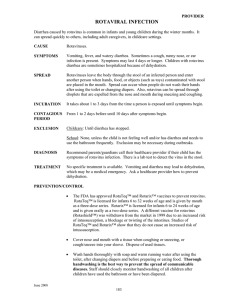
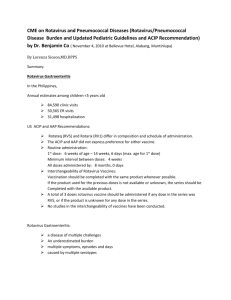
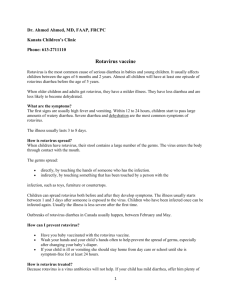
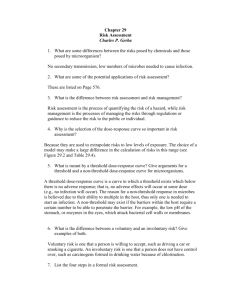
Rotavirus Prevention and Control Dr Simba Takuva, MBChB, MSc. Outline of Presentation Introduction Epidemiology and Disease Burden The Rotavirus Clinical Presentation Prevention and Control Vaccination Surveillance WHO Recommendations Conclusion Introduction Rotavirus (RV) is the commonest cause of severe diarrhoeal disease in infants and young children globally 527 000 children die each year Children under 5 most vulnerable Majority in low-income countries (85%) Country-specific data show 80-90 children die every day in Nigeria from the disease, 50-60 deaths occur daily in Cameroon, and 10-12 in South Africa Estimated cost to healthcare system: USD 264 to 318 million per year Estimated societal costs: USD 890 to 1 billion per year Epidemiology and Disease Burden Causes of Death in Children Under 5 Worldwide, 2008 15% Diarrhoea Pneumonia 37% 19% Other infections Non communicable diseases 7% 22% Neonatal causes 15% = 1.3 million deaths annually ! Black RE, Lancet 2010; 375:1969-1987 Epidemiology and Disease Burden Epidemiology and Disease Burden Transmission Primary mode of transmission is feacal to oral Highly communicable and transmissible Close person-to-person contact and environmental surfaces are common vectors of transmission Incubation period is 1 – 3 days Transmission Large quantities of virus are shed in stool from just prior to onset of symptoms until about 10 days after onset Amount of virus shed in stool: 10-100 billion virions/gram of stool ! Amount of ingested virus required to cause infection: As few as 10 infective virions ! Amount of stool that needs to be ingested to potentially result in infection: ≈ 0.000001mg ! The Rotavirus First recognized in 1973, rotavirus belongs to the viral family Reoviridae Its wheel-like shape under an electron microscope earned it the name of “rota” virus The rotavirus genome consists of 11 double-stranded RNA segments, each encoding one viral protein A triple-layered capsule surrounds the RNA Scientists have described seven rotavirus groups (A to G) Only groups A, B, and C infect humans Group A, which has multiple strains, causes the majority of childhood infections Vaccine candidates are designed to protect against Group A rotaviruses The Rotavirus The G-type and P-type define the serotype They are critical to vaccine development because they are the vaccine targets for stimulating a protective immune response SEROTYPES Source : WWW.ROTAPICTURES/BU/EDU G1P[8] is the most common serotype worldwide and accounts for over two thirds of rotavirus infections worldwide Infections with G1, G2, G3, G4, and G9 together comprise almost 95% of rotavirus serotypes observed Because the 2 gene segments that encode these proteins can segregate independently, a typing system consisting of both G and P types is used. i.e. G1P[8], G2P[4], G3P[8], G4P[8], G9P[8], and G9P[6] Clinical Presentation Timeline of Rotavirus Pathogenesis Source: Clinical Presentation Clinical Triad of Rotavirus Infection Clinical Presentation Pathogenesis The virus causes diarrhoea by three principle mechanisms: infection of villus epithelial cells causes cell destruction, decreased absorption of salt and water, and decreased disaccharidase activity, increasing the osmotic load in the gut lumen stimulation of the enteric nervous system, leading to increased fluid secretion direct enterotoxin effects of nonstructural protein 4 (NSP4), the first viral enterotoxin to be described The osmotic load in the gut and increased fluid secretion lead to diarrhoea and, if unchecked and without fluid replacement, can ultimately lead to dehydration and acidosis Clinical Presentation Complications • The major complication is the dehydration, which can lead to acidosis and eventually to circulatory collapse. Also been associated with aseptic meningitis, necrotizing enterocolitis, acute myositis, hepatic abscess, pneumonia, Kawasaki disease, SIDS and Crohn's disease Rotavirus induced gastroenteritis in children with immunodeficiency may cause persistent infection lasting weeks or months Self-limited illness in immunocompetant Clinical Presentation Diagnosis Mostly clinical Rapid antigen detection by ELISA of rotavirus in stool specimens. Isolates may be further characterized by reversetranscriptase polymerase chain reaction Clinical Presentation In infants, natural rotavirus infection confers protection against subsequent infection By the age of 2 years, nearly every child in a cohort of children in Mexico had experienced at least one rotavirus infection These children had greater protection against severe diarrhoea with subsequent infections Two natural infections were required for 100% protection against moderate-to-severe diarrhoea The first exposure to rotavirus also protected 87% (95% CI, 54%, 96%) of children from having severe disease from the second infection The protection rates observed with one natural infection are similar to those observed with vaccine-induced protection Vaccination protects 84% to 98% of children against severe outcomes of a second rotavirus infection Thus, the vaccines are mimicking the protection rates of one natural infection Source: Velazquez, FRet al. N Engl J Med. 1996;335:1022-1028 Clinical Presentation Probability of RV Infection by Age Cumulative Probability of First and Subsequent Natural Rotavirus Infections during the First Two Years of life (Source: Velazquez, FRet al. N Engl J Med. 1996;335:1022-1028.) Treatment Therapy for rotavirus-induced diarrhoea involves replacement of fluids and electrolytes lost during infection. Priorities feeding (breast milk or diluted formula in infants and lactose free carbohydrate rich foods in older children) within 24 hours after onset of illness the use of oral rehydration therapy in children with mild or moderate dehydration. Fruit juices and soft drinks are not recommended due to their high glucose content, low sodium content and high osmolarity. Antibiotics, antisecretory drugs, antimotility drugs, absorbents and antiemetics do not ameliorate acute infection, prevent reinfection or reduce fluid losses during rotavirus induced gastroenteritis, and therefore do not play a role in treatment. Children with immunodeficiency disorders may be treated with rotavirusspecific immunoglobolin preparation. Administer orally to decrease shedding and ameliorate disease . Prevention and Control Infection Control Vaccination Infection Control In the Home and Day-Care Facilities Hand-washing areas Food-preparation areas Diaper-changing surfaces Diaper disposal containers Toys In Hospital Areas and Clinics Hand-washing areas Medication-preparation areas Equipment Patient care areas Rotavirus Vaccination Rotavirus Vaccines Vaccine Efficacy Vaccine Safety Rotavirus and HIV-infected infants WHO - EPI Recommendations Rotavirus Vaccines Two oral, live, attenuated rotavirus vaccines Rotarix (GlaxoSmithKline Biologicals,Rixensart, Belgium) RotaTeq (Merck & Co. Inc., West Point, PA, USA) Available internationally Both vaccines are considered safe and effective WHO now recommends that infants worldwide be vaccinated against Rotavirus Vaccines differ in composition and dosing schedule Rotarix (RV1) is a monovalent vaccine given in a 2-dose schedule Rotateq (RV5) is a pentavalent vaccine given in a 3-dose schedule Rotavirus Vaccines Manufacturer Genetic framework Composition Genotypes Dosage Schedule Route Presentation Efficacy against severe disease Virus shedding RotaTeq Rotarix Merk & Co. GSK Bovine Rotavirus – WC3 Human Rotavirus-89-12 5 Human, Bovine reassortant Single Human rotavirus G1, 2, 3, 4 and [P8] G1 [P8] 3 doses at 2, 4 and 6 months 2 doses at 2 and 4 months oral oral liquid Lysophilized-reconstituted 85% 95% Up to 13 % 17 % - 27% Rotavirus Vaccine Clinical Trials Vaccine Efficacy Rotavirus Efficacy in Clinical Trials in Africa and Asia Vaccine RV1 (Rotarix) Region Africa RV5 (RotaTeq) Asia RV5 (RotaTeq) Africa Country South Africa, Malawi Efficacy 62% (44% - 73%) Bangladesh, 51% (13% - 73%) Vietnam Ghana, Kenya, 64% (40% - 79%) Malawi Madhi SA, et al. N Engl J Med 2010;362:289-298 Armah GE, et al. Lancet 2010;376:606-614 Zaman K, et al. Lancet 2010;376:615-623 Vaccine Efficacy Factors to Consider in Rotavirus Efficacy Efficacy of Rotavirus Vaccines by Mortality Stratum and Country Mortality rate RV vaccine Countries were studies defined by WHO efficacy estimates were performed HIGH 50 – 64 % 46 – 72 % Ghana, Kenya, Malawi, Mali Bangladesh, South Africa INTERMEDIATE 72 – 85 % Vietnam, the Americas LOW 85 – 100 % The Americas, Western Pacific and Europe Adapted from WHO. Wkly Epidemiol Rec 2009;84:533-40 Rotavirus Surveillance in South Africa Diarrhoea sentineal surveillance programme implemented in April 2009 by the NICD Five hospitals in four provinces (Gauteng, North-West, Kwazulu Natal and Mpumalanga) The aim of the programme is to evaluate the prevalence of rotavirus in diarrhoea cases and to monitor the effect of the introduction of the Rotarix vaccine into the EPI The rotavirus vaccine was introduced in August 2009 Children < 5 years admitted (slept overnight in hospital) to one of the sentinel hospitals for acute diarrhoea (3 loose stools in 24 hour period and onset within 7 days) are eligible for enrolment in the surveillance Stool specimens are collected and tested at the NICD/NHLS and at the Diarrhoeal Pathogens Research Unit, MEDUNSA, using the Rotavirus ELISA kit Rotavirus Surveillance in South Africa In the first year, coverage was less than 50%; data from early 2010 indicated uptake of 50-75% Rotavirus in South Africa is a very seasonal disease, usually peaking in May, with a second smaller peak a few months later In summer months there is little rotavirus but quite a bit of other diarrheal disease Data collected from the sentinel sites through June 2010 showed a major decline in RV-positive stool samples in the 2010 rotavirus season, the first following the vaccine’s introduction In vaccinated children, rotavirus was detected in 11% of stool samples during the surveillance period, while in the unvaccinated children the rate was 20% Rotavirus Surveillance in South Africa Cumulative number of specimens tested rotavirus positive and total number of samples collected by hospital - Reporting period: 04/01/2010 to 30/12/2010. Hospital Rotavirus Positive Total Samples Chris Hani Baragwanath 128 541 Edendale 16 84 George Mukhari 46 232 Mapulaneng 10 67 Matikwane 41 218 Total 241 1142 Rotavirus also has a distinct seasonality with peaks in the winter months in temperate climates serotype G1 accounts for approximately 50% of infections in South Africa. Other serotypes causing infection in South Africa include G2, G8, G9 and G12 Data courtesy of NICD Epidemiologic Report; ROTA Surveillance, 2011. Rotavirus Surveillance in Africa 25-40% of African children hospitalized with diarrheal illness are infected with rotavirus By 18 months of age, 83% of children will have contracted the virus G1 is most prevalent strain in Africa, estimated 50% of cases, followed by G3 at 30% G2 strain occurs in “waves” every 3 to 4 years G4 and G8 strains occur in sporadic isolation G9 is emerging in countries across the continent Mixed serotypes are increasingly common Of the P genotypes, P6 is the most common, accounting for 50-60% of cases, followed by P8 (35-40% of cases). An unusual VP4 serotype has also been detected African Rotavirus Surveillance Network (AFRSN) – www.afro.who.int/en Rotavirus Surveillance Other Effects of Rotavirus Vaccination Health Impact decrease in all-cause diarrhoea Herd Immunity protection extends to the unvaccinated Age specific incidence of disease change in age of exposure Season specific incidence of disease shift in onset of epidemics. Helps guide surveillance systems Long-term interaction of rotavirus vaccination and strain ecology Strains may changes post-vaccination Rotavirus Herd Immunity Rotavirus in HIV-infected Infants HIV infected children with RV diarrhoea have similar shortterm clinical course and outcome. HIV infected children 4.7 fold more likely to have ongoing, prolonged asymptomatic shedding of RV four weeks post-diarrhoeal illness. RV IgG and IgA seroconversion post wild type RV illness similar between HIV-infected and -uninfected children RV infection does not affect blood HIV viral load or CD4cell counts RV vaccine not associated with progression of immunedeficiency in HIV infected children. Cunliffe NA et al. The Lancet; 2001; 358: 550-555 ; Jere C et al. AIDS 2001; 15: 1439-42 Rotavirus Vaccine Safety Intussuseption Currently NO data supports hypothesis of increased risk of intussuseption with RV vaccines Rotavirus vaccines are safe • Reviewed safety data from phase III efficacy studies of Rotarix and RotaTeq, as well as postmarketing safety data from Australia, Latin America and the United States • Previous association with the now withdrawn vaccine, RotaShield Rotavirus Vaccine Safety Contraindications Severe Combined Immunodeficiency Syndrome History of: severe allergic reaction to a prior dose of RV Severe allergic reaction to latex Intussuseption Some congenital GI malformations e.g. Meckel diverticulum Vaccine-vaccine interactions RV vaccines have been found not to interfere significantly with the immunogenicity or safety of other childhood vaccines However, OPV appears to have an inhibitory effect on the immune response to the first dose of RV vaccine WHO - EPI Recommendations RV vaccine should be included in all national immunization programmes In countries where diarrhoeal deaths account for ≥10% of mortality among children aged <5 years, the introduction of the vaccine is strongly recommended WHO recommends that the first dose of either RotaTeq or Rotarix be administered at age 6–15 weeks The maximum age for administering the last dose of either vaccine should be 32 weeks. It is recommended that 2 doses of Rotarix be administered with the first and second doses of DTP rather than with the second and third doses This ensures maximum immunization coverage and reduces the potential for late administration beyond the approved age window This schedule will be reviewed as new data become available 6 and 14 weeks in RSA EPI schedule Conclusions Rotavirus vaccines are not the solution to controlling this disease Disease Control involves an integrated approach Zinc treatment Improved oral rehydration solution (ORS) Exclusive breastfeeding Improved nutrition Community education Safe water, adequate sanitation and hygiene These can complement the impact of vaccines and together have a huge impact in reducing the burden of diarrhoea – one of the largest killer of young children. References • • • • • • • • • • • • • • • • • • • • • • WHO Weekly Epidemiological Record 2008; 83 (47), 27 November 2008 Global networks for surveillance of rotavirus gastroenteritis, 2001-2008. Wkly Epidemiol Rec 2008;83:421-428. Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI. Global illness and deaths caused by rotavirus disease in children. Emerg Infect Dis 2003;9:565-72. Chin, J. (Ed.). (2000). Control of Communicable Disease Manual. Wash. DC: American Public Health Association. American Academy of Pediatrics. (1997). Rotavirus. In Red book: Report of the committee on infectious diseases. (24th ed., pp.454 - 456). Elk Grove Village, IL:Author. Velazquez F, Matson DO, Calya JJ, et al. Rotavirus infections in infants as protection against subsequent infections. N Engl J Med. 1996;335:1022-1028. Offit, P. A. & Clark, M. F. (2000). In G. L. Mandell, J. E. Bennett, & R. Dolin (Eds)., Principles and practice of infectious diseases. (5th ed., pp.1696 -1703). Philadelphia, PA: Churchill Livingstone Estes M. Rotaviruses and their replication. In: Howley PM, ed. Fields Virology. 3rd ed. Vol. 2. Philadelphia, PA: Lippincott-Raven; 1996:162555. Estes MK, Cohen J. Rotavirus gene structure and function. Microbiological Reviews 1989;53:410-49. Glass RI, Bhan MK, Ray P, et al. Development of candidate rotavirus vaccines derived from neonatal strains in India. J Infect Dis 2005;192(Suppl):S30-S5. Ward RL, Bernstein DI. Lack of correlation between serum rotavirus antibody titers and protection following vaccination with reassortant RRV vaccines. Vaccine 1995;13:1226-32. Green KY, Taniguchi K, Mackow ER, Kapikian AZ. Homotypic and heterotypic epitope-specific antibody respones in adult and infant rotavirus vaccinees: implications for vaccine development. J Infect Dis 1990;161:667-79. Madhi S, Cunliffe NA, Steele D, Witte D, Kirsten M, et al. N Engl J Med 2010: 362: 289-98 Vesikari T, Matson DO, Dennehy P, et al. Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med 2006;354:23-33. CDC. Withdrawal of rotavirus vaccine recommendation. MMWR 1999;48:1007. Peter G, Myers MG. Intussusception, rotavirus, and oral vaccines: summary of a workshop. Pediatrics 2002;54:110. WHO. Report of the Global Advisory Committee on Vaccine Safety, December 1-2, 2005. Wkly Epidemiol Rec 2006;2:13-20. African Rotavirus Surveillance Network (AFRSN) – www.afro.who.int/en Rotavirus (ROTA) Surveillance: Rotavirus Report, National Institutes of Communicable Diseases, 2 March 2011. WHO Weekly Epidemiological Record. No. 51-52, 2009, 84, 533-540. Diarrhoea: why children are still dying and what can be done. Geneva, UNICEF and World Health Organization, 2009 (available from: http://www.who.int/child_adolescent_health/documents/9789241598415/en/index.html; accessed November 2009). CDC, unpublished data, 2006. THANK YOU