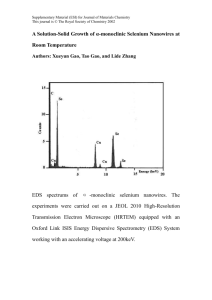
SELENIUM NOTES Introduction Selenium is incorporated into 25 selenoproteins,1 which have a broad range of functions - including contribution to the production of thyroid hormone and healthy sperm cells, as well as working as antioxidants and exerting anti-inflammatory effects. Associations between selenium status and disease risk have been made where selenium is both deficient and over-abundant, prompting the development of the theory that the relationship between selenium and disease risk is U-shaped. Health Effects 1. Viral virulence & immune function Selenium appears to play a role in suppressing viral virulence: rodent studies with influenza virus have shown more active lung inflammation in selenium-deficient mice;2 faster clearance of the polio virus was achieved in humans supplemented with selenium3 and selenium supplementation in combination with a multivitamin was shown to reduce morbidity and immune decline in HIV-infected adults4. The data demonstrating an association between low selenium status and increased mortality in HIV-infected patients is prone to confounding though, as the acute phase response seen in patients at an advanced stage of the illness has been shown to lower selenium5. A different trial demonstrated no change in CD4+ count or of HIV-1 viral load with selenium supplementation, although there was a reduction in child mortality.6 Selenium has been demonstrated to function as an immunostimulant, where supplementation in a small study of human subjects resulted in noticeably increased cytotoxic-lymphocyte-mediated tumour cytotoxicity and in Natural Killer-cell activity7, and in a separate study, where supplementation achieved the restoration of lymphocyte activity in elderly subjects to the equivalent of healthy young adults8. However, research has not all been conclusive - a large double-blind randomised placebo-controlled trial in 197 asthma patients demonstrated no benefit from selenium supplementation9, although the benefits of supplementation may have been reduced by concurrent inhaled steroid use10. 2. Fertility A very clear relationship has been established in the case of fertility; decreased sperm motility and viability has been found in men with reduced levels of the selenoproteins GPx4 and Sepp1,11,12 and selenium status was shown to be much higher in fertile men over infertile men13. In women, lower selenium status has been found in those who miscarry in the first trimester and who have recurrent miscarriages14,15, although this is not a consistent finding.15,16 A large case-control study has found that women with a particular polymorphism of selenoprotein S, which has a role in control of inflammation, had a higher risk of developing pre-eclampsia during pregnancy.17 3. Thyroid disease A number of selenoproteins are active in the thyroid, and therefore there is a high demand for selenium here. Observational studies have linked selenium deficiency with thyroid cancer18-20and goitre21, as well as autoimmune thyroid disease22,23. A meta-analysis and systematic review convincingly concluded that thyroid peroxidase autoantibody titre was significantly lowered at 3 months with selenium supplementation24. 4. Mortality & Cancer Research from 3 large prospective studies indicates that high serum selenium concentration levels are associated with decreased all cause mortality25-27, and Figure 110 displays the findings of one study, in which a clear U-shaped association between selenium status and all-cause mortality and cancer was found25. However, selenium status is higher in fit older people than those who are malnourished or unwell28, and selenium can be depleted by poor kidney function29 Figure 1: Adjusted hazard ratios for all-cause mortality according to selenium status in adult subjects of the US Third National Health and Nutrition Examination Survey, showing data for up to 18 years - 2006.25 Figure from Professor M Rayman’s paper on Selenium and Human Health.10 and in the acute phase response5 - both features of disease - and as such, the data in these studies is susceptible to confounding. Studies in relation to cancer are conflicting; a meta-analysis of prospective studies show a decreased risk of cancer with higher selenium status30, while many RCTs show no difference. As with the findings related to mortality, the results here are prone to confounding, where low selenium could potentially be a product of the disease, not a cause. Additionally, studies where selenium is supplemented in participants with already adequate selenium status (e.g. SELECT31) may push the cancer risk up, instead of down, as a result of a non-linear relationship between selenium and dis- ease risk. This demonstrates the importance of designing trials in which participants are screened for pre-existing selenium status, particularly where there are known adverse effects at both ends of the status scale. 5. Type 2 Diabetes Mellitus (T2DM) The evidence linking T2DM to selenium status is conflicting32. Some cross-sectional studies have shown a significant association between higher selenium status and T2DM33,34, with further associations found between SeP and HbA1c33. However, longitudinal studies do not support these findings and there is only 1 RCT that has found an increased risk of T2DM with selenium supplementation35. The inconsistency of findings could be explained by an association between selenium status and T2DM that is U or S-shaped, where the risk of T2DM rises in both low and high selenium status. Intake and status Guidelines for intake vary internationally. In the UK, the reference nutrient intake is 75 µg/day for men and 60 µg/day for women36. Supplementation should be considered if patients have a selenium status of less than 122 µg/L, but no higher than this, as it is at this concentration at which the risk of cancer, non-melanoma skin cancer and T2DM increases37,38. However, it should be noted that the 130-150µg/L range is the concentraFigure 2: Combination of selenium concentration data in 2 studies (NDNS, NHANES), with associated concentration risk marker for non-melanoma cancer, cancer, and T2DM, which indicates the point at which risk increases/decreases (122μg/L), with minimal mortality indicator bracket drawn from the Third NHANES data. 25 Figure from Professor M Rayman’s paper on Selenium and Human Health10 tion associated with minimal mortality25 and this is therefore a reasonable target bracket to aim for. Conclusion The complex balance and interaction of nutrients and the multifactorial nature of disease causation can create difficulties in definitively linking individual factors to conditions, which may be why research in some areas is conflicting. Nevertheless, a range of adverse health effects have been associated with selenium status, and where single nuclear polymorphisms exist within the genes of selenoproteins. Selenium is incriminated at both ends of the status spectrum, and this supports the premise that the association between selenium status and disease risk can be illustrated by a Ushape. References 1. Kryukov GV, Castellano S, Novoselov SV, et al. Characterization of mammalian selenoproteomes. Science 2003; 300: 1439–43. 2. Beck MA, Levander OA, Handy J. Selenium defi ciency and viral infection. J Nutr 2003; 133 (suppl 1): 1463S–67S. 3. Broome CS, McArdle F, Kyle JA, et al. An increase in selenium intake improves immune function and poliovirus handling in adults with marginal selenium status. Am J Clin Nutr 2004;80: 154–62. 4. Baum MK, Campa A, et al. Effect of micronutrient supplementation on disease progressions in asymptomatic, antiretroviral-naive, HIV-infected adults in Botswana: a randomised clinical trial. JAMA 2013;310:2154-63 5. Nichol C, Herdman J, Sattar N, et al. Changes in the concentrations of plasma selenium and selenoproteins after minor elective surgery: further evidence for a negative acute phase response? Clin Chem1998; 44: 1764–66. 6. Kupka R, Mugusi F, Aboud S, et al. Randomized, double-blind,placebo-controlled trial of selenium supplements among HIV-infected pregnant women in Tanzania: eff ects on maternal and child outcomes. Am J Clin Nutr 2008; 87: 1802–08. 7. Kiremidjian-Schumacher, L., Roy, M., Wishe, H.I. et al. Biol Trace Elem Res (1994) 41: 115. https://doi.org/10.1007/ BF02917222 8. A Peretz, J Nève, J Desmedt, J Duchateau, M Dramaix, J P Famaey; Lymphocyte response is enhanced by supplementation of elderly subjects with selenium-enriched yeast, The American Journal of Clinical Nutrition, Volume 53, Issue 5, 1 May 1991, Pages 1323–1328, 9. Shaheen SO, Newson RB, Rayman MP, et al. Randomised, double blind, placebo-controlled trial of selenium supplementation in adult asthma. Thorax 2007; 62: 483–90 10. Rayman MP. Selenium and Human Health. Lancet 2012; 379:1256-68. 11. Imai H, Suzuki K, Ishizaka K, et al. Failure of the expression of phospholipid hydroperoxide glutathione peroxidase in the spermatozoa of human infertile males. Biol Reprod 2001;64: 674–83. 12. Foresta C, Floh. L, Garolla A, Roveri A, Ursini F, Maiorino M. Male fertility is linked to the selenoprotein phospholipid hydroperoxide glutathione peroxidase. Biol Reprod 2002;67: 967–71. 13.Eroglu, M., Sahin, S., Durukan, B. et al. Blood Serum and Seminal Plasma Selenium, Total Antioxidant Capacity and Coenzyme Q10 Levels in Relation to Semen Parameters in Men with Idiopathic Infertility. Biol Trace Elem Res 2014:159: 46. 14.Barrington JW1, Lindsay P, James D, Smith S, Roberts A. Selenium deficiency and miscarriage: a possible link? Br J Obstet Gynaecol. 1996 Feb;103(2):130-2. 15. Rayman MP. The importance of selenium to human health. Lancet 2000; 356: 233–41. 16. Rayman MP. Selenium and adverse health conditions of human pregnancy. In: Hatfi eld DL, Berry MJ, Gladyshev VN, eds. Selenium: its molecular biology and role in human health, 3rd edn.New York: Springer Science and Business Media, 2011: 531–46. 17.Moses EK, Johnson MP, T.mmerdal L, et al. Genetic association of preeclampsia to the inflammatory response gene SEPS1. Am J Obstet Gynecol 2008; 198: 336 e1–5. 18. Glattre E, Thomassen Y, Thoresen SO, et al. Pre-diagnostic serum selenium in a case-control study of thyroid cancer. Int J Epidemiol 1989; 18: 45–49. 19. Schmutzler C, Mentrup B, Schomburg L, Hoang-Vu C, Herzog V, K.hrle J. Selenoproteins of the thyroid gland: expression, localization and possible function of glutathione peroxidase 3. Biol Chem 2007; 388: 1053–59. 20. Mara Ventura, Miguel Melo, and Francisco Carrilho, “Selenium and Thyroid Disease: From Pathophysiology to Treatment,” International Journal of Endocrinology, vol. 2017, Article ID 1297658, 9 pages, 201 21. Derumeaux H, Valeix P, Castetbon K, et al. Association of selenium with thyroid volume and echostructure in 35- to 60-year-old French adults. Eur J Endocrinol 2003; 148: 309–15. 22. Nacamulli D, Mian C, Petricca D, et al. Infl uence of physiological dietary selenium supplementation on the natural course of autoimmune thyroiditis. Clin Endocrinol (Oxf) 2010; 73: 535–39. 23. Van Zuuren et al. Cochrane Database Syst Rev. 2013 Jun 6;6:CD010223; 24. Toulis KA, Anastasilakis AD, Tzellos TG, Goulis DG, Kouvelas D. Selenium supplementation in the treatment of Hashimoto’s thyroiditis: a systematic review and a meta-analysis. Thyroid 2010; 20: 1163–73. 25. Bleys J, Navas-Acien A, Guallar E. Serum selenium levels and all-cause, cancer, and cardiovascular mortality among US adults. Arch Intern Med 2008; 168: 404–10. 26. Akbaraly NT, Arnaud J, Hininger-Favier I, Gourlet V, Roussel AM, Berr C. Selenium and mortality in the elderly: results from the EVA study. Clin Chem 2005; 51: 2117–23. 27. Ray AL, Semba RD, Walston J, et al. Low serum selenium and total carotenoids predict mortality among older women living in the community: the women’s health and aging studies. J Nutr 2006; 136: 172–76. 28. Bates CJ, Thane CW, Prentice A, Delves HT. Selenium status and its correlates in a British national diet and nutrition survey: people aged 65 years and over. J Trace Elem Med Biol 2002; 6: 1–8. 29. Schiavon R, Guidi GC, Biasioli S, De Fanti E, Targa L. Plasma glutathione peroxidase activity as an index of renal function. Eur J Clin Chem Clin Biochem 1994; 32: 759–65. 30. Vinceti et al. Cochrane Database Syst Rev 2014 (5):CD00519 31. Lippman SM, Klein EA, Goodman PJ, et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2009; 301: 39–51. 32. Steinbrenner H, Speckmann B, Pinto A, Sies H. High selenium intake and increased diabetes risk: experimental evidence for interplay between selenium and carbohydrate metabolism.J Clin Biochem Nutr 33. Misu H, Takamura T, Takayama H, et al. A liver-derived secretory protein, selenoprotein P, causes insulin resistance. Cell Metab 2010;12: 483–95 34. Yang SJ, Hwang SY, Choi HY, et al. Serum selenoprotein P levels in patients with type 2 diabetes and prediabetes: implications for insulin resistance, infl ammation, and atherosclerosis. J Clin Endocrinol Metab 2011; 96: E1325–29. 35. Stranges S, Marshall JR, Natarajan R, et al. Effects of long-term selenium supplementation on the incidence of type 2 diabetes: a randomized trial. Ann Intern Med 2007; 147: 217–23. 36. Department of Health . 8th ed. Stationery Office; London, UK: 1991. Dietary reference values for food, energy and nutrients for the UK: Report of the panel on dietary reference values of the committee on medical aspects of food policy; pp. 1–210 37. Bates C.J., Thane C.W., Prentice A., Delves H.T. Selenium status and its correlates in a British National Diet and Nutrition Survey: People aged 65 years and over. J. Trace Elem. Med. Biol 38. Allen N.E., Appleby P.N., Roddam A.W., et al. Plasma selenium concentration and prostate cancer risk: Results from the European Prospective Investigation into Cancer and Nutrition (EPIC) Am. J. Clin. Nutr. 2008;88:1567–1575. doi: 10.3945/ajcn.2008.26205