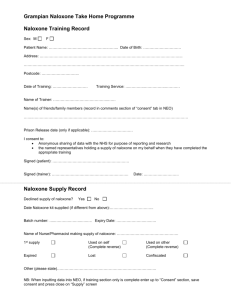
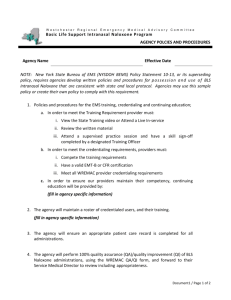
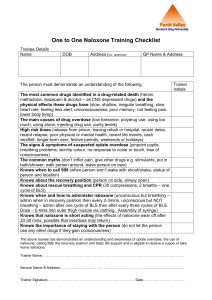
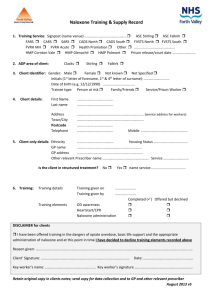
Journal of Analytical Toxicology, 2018;42:e38–e40 doi: 10.1093/jat/bkx104 Advance Access Publication Date: 28 December 2017 Letter to the Editor Letter to the Editor Movantik™ and the Frequency of Positive Naloxone in Urine 1 InSource Diagnostics, 231W Chestnut Ave, Monrovia, CA 91016, USA, and 2Ameritox LLC, 486 Gallimore Dairy Rd, Greensboro, NC 27409, USA *Author to whom correspondence should be addressed. Email: greg.mcintire@ameritox.com To the Editor: Movantik ™ (naloxegol) is a relatively new medication used to treat opioid-induced constipation (OIC). The drug is a PEGylated derivative of naloxol, a metabolite of naloxone (Figure 1); however, the literature does not support the presence of naloxone as a metabolite of naloxegol (1). In fact, the metabolites reported in the literature consist mainly of various length PEG chains attached to the core molecule (Figure 2) as well as unmodified naloxegol. It is important to note that the radiolabel used for the metabolic studies was located on the PEG chain. As such, radioactivity would not be associated with the core opioid structure. Even so, the structure that would result from loss of the entire PEG chain would be naloxol. Conversion of naloxol to naloxone would appear to be an “uphill” conversion inasmuch as naloxol is a metabolite of naloxone. Nevertheless, our respective laboratories have received calls over the past several months from patients who tested positive for naloxone, but reported only naloxegol use. Given that naloxone has not been reported as a possible metabolite of naloxegol, these results prompted an investigation into both retrospective data as well as a controlled case study with a known naloxone negative volunteer. Over the past 15 months and at physician request, 1,335 samples were analyzed for a variety of drugs from patients who were prescribed naloxegol. Fourteen of these samples had low positive naloxone results. All samples were hydrolyzed before analysis using a recombinant enzyme from IMCS® (Irmo, SC), the conditions of which have been reported elsewhere (2). Of the 1,335 samples, 209 (15.7%) were positive for buprenorphine or norbuprenorphine, making identification of the source of a positive naloxone result impossible to discern between a Suboxone™ and Movantik™ prescription for those patients. Of the remaining samples, physicians requested a result for naloxone from 187 and of those, 14 were positive for naloxone at low levels—less than 100 ng/mL—but negative for both buprenorphine and norbuprenorphine. Further, of these 14 results, two patients had repeat positive tests results for naloxone separated by 4 months and 8 months, respectively. These data suggest that as many as 7.5% (14/187) or as few as 0.8% (14/1,335) of patients prescribed naloxegol could test positive for naloxone. The actual frequency is likely between these limits. To further investigate the possibility of naloxone detection in urine after dosing with naloxegol, a 39-year-old male volunteer with no reported buprenorphine or naloxone containing prescription medications or history of illicit drug use submitted urine samples before and after dosing with Movantik™ under guidance of his physician. The volunteer was ~210 lbs and was a normal CYP 3A4 metabolizer (as determined previously and provided by request), which is the primary enzyme system for naloxegol (3). The first urine sample, before dosing, showed no detectable levels of naloxone or any other medications when analyzed by LC/MS/MS (Figure 3). The subject was then given an oral 12.5 mg dose of naloxegol on an empty stomach and submitted a sample for LC/MS/ MS analysis ~1.5 h later (Figure 4). When analyzed directly without hydrolysis, the sample showed no detectible levels of naloxone. However, when the sample was hydrolyzed using an abalone source beta-glucuronadase enzyme procedure in an acidic buffer, naloxone was observed at 12.1 ng/mL, just above the reporting limit of the assay (10 ng/mL). The presence of naloxone in the urine of patients prescribed naloxegol was not predicted from the metabolic study from Bui et al. (1). While the possible metabolic route for this conversion to naloxone has not yet been delineated, these data support the observation of a significant number of patients with positive naloxone test results after taking naloxegol. The actual quantitative values are generally low, <100 ng/mL, as demonstrated both by the retrospective data analysis and the single case study. For comparison, naloxone concentrations derived from Suboxone™ dosing have been reported by Cummings et al. (4) to average 240 ng/mL. These data are in concert with those from Heikman et al. (5) who found an average concentration of 299 ng/mL in substance abuse patients. Furthermore, two patients prescribed naloxegol tested positive repeatedly for naloxone in urine samples that were submitted and analyzed several months apart, pointing towards a unique metabolic pathway. This pathway may be minor but results in positive naloxone results as noted above. Thus, the observation of naloxone post dosing naloxegol is both possible and present in a significant percentage of patients. © The Author(s) 2017. Published by Oxford University Press. All rights reserved. For Permissions, please email: journals.permissions@oup.com e38 Downloaded from https://academic.oup.com/jat/article-abstract/42/3/e38/4780786 by guest on 26 February 2020 Justin Wotring1, Sky Countryman1, Frank N. Wallace2, Erin C. Strickland2, Oneka T. Cummings2, and Gregory L. McIntire2,* Letter to the Editor e39 Figure 1. Structure of Movantik™. Figure 3. Pre dosing control sample showing hydrolyzed results using a beta glucuronidase enzyme and analyzed using a validated LC/MSMS method. The upper image represents the quantitative peak while the lower image represents the qualitative peak. Downloaded from https://academic.oup.com/jat/article-abstract/42/3/e38/4780786 by guest on 26 February 2020 Figure 2. Reported metabolites of Movantik™ (1). e40 Letter to the Editor When monitoring patients who are taking naloxegol for opiate induced constipation, physicians should be aware that they may test positive for low levels of naloxone. Inasmuch as naloxone may also be given in an emergency situation during a suspected opioid overdose event, it is important to know the source of naloxone detected in a patient’s urine sample. Further research is required to determine guidelines and possible mechanism for the detection of naloxone in patients taking naloxegol. References 1. Bui, K., She, F., Hutchison, M., Brunnström, Å., Sostek, M. (2015) Adsorption, distribution, metabolism and excretion of [14C]-labeled 2. 3. 4. 5. naloxegol in health subjects. International Journal of Clinical Pharmacology and Therapeutics, 53, 838–846. Cummings, O.T., Strickland, E.C., McIntire, G.L. (2016) A rapid, selective, and sensitive method for the analysis of naltrexone and 6β-naltrexol in urine. Current Trends in Mass Spectrometry, 14, 17–20. Movantik™ package insert. https://www.accessdata.fda.gov/drugsatfda_ docs/label/2014/204760s000lbl.pdf (accessed June 15, 2017). Cummings, O.T., Wallace, F., Strickland, E.C., McIntire, G.L. Urine naloxone levels in patients prescribed combination dosage forms: buprenorphine/naloxone, 2016 SOFT Annual Meeting, Dallas, TX. Heikman, P., Hakkinen, M., Gergov, M., Ojanpera, I. (2014) Urine naloxone concentration at different phases of buprenorphine maintenance treatment. Drug Testing Analysis, 6, 220–225. Downloaded from https://academic.oup.com/jat/article-abstract/42/3/e38/4780786 by guest on 26 February 2020 Figure 4. Post dosing urine sample comparing (a) hydrolyzed and (b) un-hydrolyzed results analyzed using a validated LC/MSMS method. A beta glucuronidase enzyme was used hydrolyze urine samples. In both (a) and (b) the top image represents the quantitative peak while the bottom image represents the qualitative peak.