1577124538221 1577124533275 1577124493215 1577124493026 1577124492245 1577124488889 193565109948067 me
advertisement

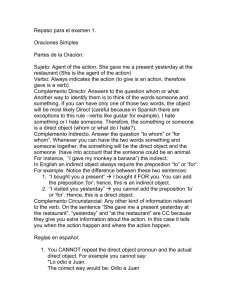
Hospital Discharge Form Monday, December 23, 2019 Basic Information Complete this form for all hospital discharges. Refer to Hospital Discharge Summary Form Instructions for information on how to complete this form. Patient's Name Patient's I.D. # Phone Number: Minni Luciano Integer non velit. +45 (18) 528-5168 Attending Physician Facility Name Minni Luciano Integer non velit. Date Services should end Saturday, September 15, 2012 Elements that need to be put in place prior to discharge (verify that the following information is documented in the record, if applicable) Nulla justo. Aliquam quis turpis eget elit sodales scelerisque. Mauris sit amet eros. Suspendisse accumsan tortor quis turpis. Medical Information Fill in detailed and speci c information about the patient’s current medical condition and the reasons why services are no longer reasonable or necessary for this patient or are no longer covered according to Medicare or Medicare managed care coverage guidelines. (Use full sentences, plain language and no abbreviations) a. You were admitted to (see facility above) on the following date Saturday, September 15, 2012 b. At admission you presented with the following symptoms Pellentesque ultrices mattis odio. 1 Create your own automated PDFs with JotForm PDF Editor Medical Information Continues... c. You were diagnosed with Pellentesque ultrices mattis odio. d. You were treated with Pellentesque ultrices mattis odio. e. Your tests were (include results) Pellentesque ultrices mattis odio. 2 Create your own automated PDFs with JotForm PDF Editor Medical Information Continues... f. You were evaluated by Pellentesque ultrices mattis odio. g. You are now (list current treatment plan and/or state the medical issue is resolved) Pellentesque ultrices mattis odio. h. Your provider feels that your condition has improved and that the care you need now could safelybe provided in/at Pellentesque ultrices mattis odio. i. Your discharge plan and follow-up care includes Pellentesque ultrices mattis odio. Other Information Printed name of person completing the form Minni Luciano Phone Number +45 (18) 528-5168 Signature of person completing the form Pellentesque ultrices mattis odio. 3 Create your own automated PDFs with JotForm PDF Editor