Chapter 9
Slides 1 – 4
Slide 5 - The most important purpose of the requisition is to give you
authorization to do the procedure. It also tells you what equipment you will need
to perform the test requested. There are many different formats and types of
requisitions; they may be a hand written doctor’s order and the lab will make up
the form for an outpatient; it may be a computer generated ticket with barcodes.
These may be waiting for you up on the floors, sent to the lab prior to collection,
or handed to you personally. It would be your job to examine them to make sure
that you have everything needed and that all orders for one patient are put
together so that you will not need to stick them again. The basic information
required would be: the patient’s name and Id number, their location, the name of
the ordering doctor, what tests are needed and the date and time to do the test.
This would include the status of the test {stat, routine, etc.}. Other information
may be required by the place that you work – patient’s date of birth, special
handling {on ice, fingerstick only,etc} as well as the number and type of tubes
to be collected. Your proper specimen collection begins with the requisition.
Slide 6 - Greeting the patient: Always knock! Introduce yourself; explain that
you are from the lab and will need a specimen of blood. Most of the time the
consent will be "implied" when the patient rolls up their sleeve or holds out their
arm. Make use of your communications skills. Always observe all signs either on
the door or over the bed.
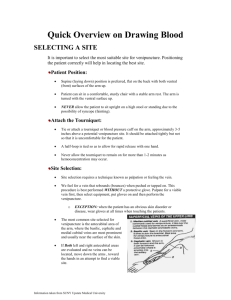
Slide 7 & 8 - The most important procedure in phlebotomy would be the proper
ID of the patient. It is now recommended that you use 2 unique identifiers. This
is vital because you could potentially kill a patient if you did not draw the right
patient. Before you start the procedure, ALWAYS check the patient’s ID band. It
should tell you their name and ID number as well as other pertinent information.
Check this against the information of the requisition and then have the patient
verbally confirm their name. Some wrist bands may even have barcodes that will
positively ID the patient. If the ID band is not on the patient’s arm – check the
ankle. Sometimes they will have an IV going in one arm and a cast on the other.
You can not use a bed sign or a wrist band lying at the bedside for ID.
Slide 9 Slide 10 - Outpatient ID is a bit different. Have the patient give you the 2 unique
identifiers verbally - stating their name or birth date, etc. Compare this with your
requisition. Usually you will not have and armband. For certain legal tests, you
may even need to have a photo ID.
Slide 11 - Technology is catching up with phlebotomy. Some institutions now
have a hand held bar code scanner that will positively ID your patient. This can
Chapter 9
even be linked to the laboratory computers and instruments. The newest
technology is the RFID. It uses radio waves to transmit data for patient ID and
sample tracking. The advantage here is that this can be updated at any time.
Slide 12 - Reassurance of a nervous patient starts with your professional
demeanor as you greet them. You never tell them that it won’t hurt but assure
them of your skills. You can briefly tell them about the procedure {what steps
you need to take, what they might need to do, etc} but do not go into an
explanation of the test. The doctor handles that. If they ask questions that you
don’t want to answer, ask them to please inquire of the physician for their
explanation. Sometimes humor helps. Make sure that any pretest variables are
completed. They may need to be fasting and some medicine may need to have
been given prior to your drawing the blood. Also ask about possible allergies.
Slide 13 –
Slide 14 - If patients know that they have trouble having their blood drawn, you
need to know this fact. You may want to have them lie down. You should never
draw a patient when they are standing. They may start to fall and the potential is
there for great injury. You should request that they remove anything that they
may have in their mouth such as gum or candy, etc. A sudden inhale could
cause them to start to choke. For outpatients, you may have a drawing chair
which will allow you to support the arm during the procedure. If a patient tells
you that they faint, have them lie down while you draw their blood and keep
talking to them!
Slide 15 - Make sure that the patient's arm is accessible and supported. If there
are bed rails in use, put them down to draw blood (uncomfortable to lean over!!)
but put them back in the up position when you are done. If you don't, that could
lead to a charge of negligence.
Slide 16 – BEFORE you leave the lab, check your requisition and make sure that
you have everything that you might need for this particular blood draw. Some
things you will not always have on your tray (ex: blood culture bottles).
Slide 17 - Do not use the bed as a place to park your tray! Placing your
equipment in close proximity to the patient is very important. You should not
have to go reaching for the items that you need. Try to place your equipment
next to the hand that you use to change tubes with. This will help eliminate
moving the needle apparatus from reaching over to get items. Lab coats have
pockets for a reason – use them as a place for extra items like tubes in case a
tube has lost vacuum, etc.
Slide 18 - In front of the patient, you should first wash your hands and then put
on clean gloves.
Chapter 9
Slide 19 - After you have asked the patient about an arm preference, you apply
the tourniquet. A tourniquet impedes the venous blood flow but NOT the arterial
flow. If you tie the tourniquet on too tightly, you can petechiae. These are small
red spots on the arm. This should be placed about 3 – 4 inches above the site
selected. This should not remain on the arm for more than 1 minute. If it stays
on longer, you can get complications such as hemoconcentration {an increased
ration of cells to plasma} or hemolysis {breaking down of the RBC’s}. These
complications can affect some lab results. Once you have found the vein,
release the tourniquet and wait 2 minutes before reapplying to stick the patient.
During this time you would gather your equipment.
Slide 20
Slide 21 – The most likely place where you will find a vein is in the antecubital
fossa {just below the elbow}. 3 major veins in order of choice are: the median
cubital, which is the most well anchored and runs down the middle of the arm;
the cephalic – located on the thumb side, it is the not as well anchored and
many times is a rolling target; median cephalic - sometimes found in the "M"
pattern and the basilic – located on the inner arm but closer to the brachial artery
that lies near it. You can also look at the veins in the hands and wrists.
Slide 22 & 23
Slide 24 - Palpating the vein will give you the dimensions – how wide and how
deep the vein is – as well as the direction it is going. A good vein should feel
spongy. Sometimes older people have veins that feel more rigid because they
have lost their elasticity. You must be careful not to confuse these with a tendon
which feels like a rigid cord. It will help to find a vein if you have tied the
tourniquet properly and if the patient can clench their fist. Pumping the fist can
cause hemoconcentration so this should be avoided. When palpating a vein,
always use your index finger. Try it with your non-dominant hand because it may
be less used than your dominant one. Never use your thumb because it has a
pulse of its own and you may think that you have found an artery. Sometimes
you can use landmarks (freckles, moles, scars, etc.) to help you map our and
remember where the vein is.
Slide 25 - Once you have found the vein, release the tourniquet and start to
cleanse the site. This is done with 70% isopropyl alcohol and is done in a
circular motion and working outward. Always allow the site to dry for 30 - 60
seconds prior to sticking. Do not blow, fan, or wipe the site with unsterile gauze.
Slide 26 - While the alcohol is drying, you can assemble everything. Make sure
that all of your equipment is close by but do not place your tray on the patient’s
bed. They could move and send everything flying and it just does not appear
Chapter 9
professional. Connect the needle to the adapter but do not remover the needle
cap.
Slide 27 - Reapply the tourniquet and then uncap the needle and observe it for
any flaws. Hold the adapter in your dominant hand with the thumb on top and
fingertips on the bottom in an East - West position. You anchor the vein to
prevent “rolling”. In general, the closer the vein is to the surface of the arm, the
more likely it is that it will roll. When you are ready to enter the vein, make sure
that the bevel of the needle is up and that your insertion angle is between 15
and 30 degrees. According to the book, anchor the vein with your thumb below
the venipuncture site. This is a change for me because I always have anchored
above and below and that is the way that I will be showing you.
Slide 28 - Using the wings of the adapter, use your thumb to push the tube on.
If you are in the vein, blood should start to flow. At this point, the patient can
release their fist and the tourniquet can be removed. If the procedure will not last
more than the 1 minute time, I would not mess with it. The more moving you do,
the more chance that something will go wrong. Your hand holding the adapter
should have your fingers forming a brace to provide stability for the needle. The
tubes should be held at a downward angle to prevent blood refluxing. When you
remove an anticoagulant tube from the assembly, always mix it gently PRIOR to
putting on the next tube. Any specimen requiring special handling would be
collected LAST. When you have drawn the last tube, withdraw it and mix it
completely. You do not want a tube still on there when you withdraw from the
arm because you could drip blood on the patient.
Slide 29 – This would be the order of actions once you have removed the last
tube and are ready to finish the venipuncture. Removing the tourniquet helps to
prevent a hematoma from forming. Place gauze over the puncture site and
remove the needle quickly. Activate the safety device. Apply pressure
immediately AFTER you have withdrawn the needle. If you put pressure on while
the needle is still in the arm, it hurts and can cause leaking around the enlarged
hole thus causing a hematoma. That is the same reason why patients no longer
bend their arm up. If the patient is able, he may apply the pressure but if not –
you must do it. Before applying a bandage, you must ascertain that the bleeding
has stopped. If you do not, a hematoma might form.
Slide 30 - You must dispose of the whole needle assembly immediately into a
sharps container. Never recap the needle!
Slide 31 - While the patient is applying pressure, you may then label your tubes.
You must never manually pre-label a tube. Sometimes you may have bar-coded
Chapter 9
tubes to use but these must be very carefully checked for the proper
identification. Learn to write the time in military time. Make sure that all
information needed is on the tube.
Slide 32 - After you have labeled the tubes, go back and check to make sure
that your patient has stopped bleeding. Most people will stop within 5 minutes. If
your patient is allergic to band aids, use paper tape. If you feel that additional
pressure is needed, fold up a gauze square and put the bandage over that. This
bandage should be removed within an hour and patients should avoid carrying
heavy objects during that time.
Slide 33 - Anything that might be contaminated or that has touched the patient
needs to be disposed of in a biohazard container. All paper trash – wrappers,
etc.- may be thrown into the regular trash.
Slide 34 - After this is done, you can de-glove and wash your hands. Make sure
that the bed is in the same position in which you found it. Always thank the
patient. Good manners go a long way to help in patient satisfaction.
Slide 35 - You must make sure that you deliver the specimens to the lab in a
timely manner and make sure that they are handled in the proper manner
{immediately separated, stored in freezer, etc.} Some tests will be affected
adversely if they are not properly processed. It can also affect the workflow. The
job is not done until the paperwork is finished.
Slides 36 - 47 Pictorial review