A Program Director's Guide to the Medical Student Performance Evaluation (former Dean's Letter) with a Database
advertisement
 with a Database")
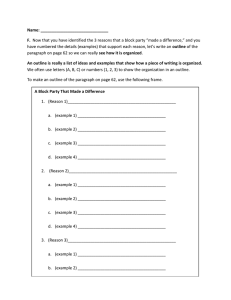
A Program Director’s Guide to the Medical Student Performance Evaluation (Former Dean’s Letter) With a Database James B. Naidich, MDa, Gregory M. Grimaldi, MDa, Pamela Lombardi, MDa, Lawrence P. Davis, MDa, Jason J. Naidich, MDa Purpose: The value of the Medical Student Performance Evaluation (MSPE) for a program director is in the information it contains comparing how a student performed in medical school relative to his or her classmates. The Association of American Medical Colleges has recommended that a student’s class ranking be included in the summary paragraph of the MSPE and that this information be repeated in a supplementary appendix. Methods: The authors reviewed the MSPEs from 1,479 applications for residency training positions. The aim was to determine to what extent and in what manner individual schools reveal how their students perform relative to their peers. The authors then set out to create a database containing this information. Results: Working from a list of 141 US members of the Association of American Medical Colleges, complete information for 107 schools (76%) and partial information for the remaining 34 schools (24%) was gathered. Only 12 schools (9%) included complete comparative information in the summary section in accordance with the guidelines of the Association of American Medical Colleges. Other schools were in partial compliance or did not comply at all. The database the authors constructed will inform users if comparative information is available, guide users to its location in the MSPE, and explain the meaning of the language different schools use to rank or classify their students. Conclusions: The authors recognize that this database is incomplete and that the individual institutions will alter their ranking system from time to time. But this database is offered in an open format so that it can be continuously updated by users. Key Words: Dean’s letter, MSPE, medical student performance, resident applications, student evaluations J Am Coll Radiol 2014;11:611-615. Copyright © 2014 American College of Radiology INTRODUCTION The Medical Student Performance Evaluation (MSPE), formerly the dean’s letter, has the potential to provide valuable information, not available elsewhere, concerning how a medical student has performed relative to his or her classmates [1]. This information is of particular importance to program directors trying to decide which applicants to invite for interviews. But despite the importance of this information, as the Association of American Medical Colleges (AAMC) wrote in its 2002 a North Shore-LIJ Health System, Hofstra North Shore-LIJ School of Medicine at North Shore University, Department of Radiology, Manhasset, New York. Corresponding author and reprints: James B. Naidich, MD, North Shore-LIJ Health System, Hofstra North Shore-LIJ School of Medicine at North Shore University, Department of Radiology, 300 Community Drive, Manhasset, NY 11030; e-mail: jnaidich@yahoo.com. ª 2014 American College of Radiology 1546-1440/14/$36.00 http://dx.doi.org/10.1016/j.jacr.2013.11.012 Guide to the Preparation of the Medical Student Performance Evaluation [2], “A common recurrent complaint of those who interpret deans’ letters of evaluation is that too often it is impossible to estimate how a candidate performed in comparison to his or her peers.” This is a problem with a long history. In 1989, Wagoner and Suriano [3] wrote a short paper titled “A New Approach to Standardizing the Dean’s Letter.” Their paper pointed out that the inconsistencies among different medical schools reduced the value of the dean’s letter and that residency program directors would benefit from a concise and comprehensive form that was consistent from school to school. That same year, the AAMC first published guidelines recommending that the dean’s letter contain information that would allow readers to understand each medical student’s performance compared with his or her peers [4]. In 1993, Hunt et al [4] published a paper titled 611 612 Journal of the American College of Radiology/Vol. 11 No. 6 June 2014 “Characteristics of Dean’s Letters in 1981 and 1992.” They reported that 45% of medical schools were not compliant with the 1989 AAMC guidelines. The authors warned that failure to provide comparative information would diminish the value of the dean’s letter, with the result that program directors would place too much emphasis on “simple-minded numerical scores from licensure examinations.” In a follow-up paper written in 2001, Hunt et al [5] reported some improvement, but 35% of schools were still noncompliant. In 2002, the AAMC [2] again addressed the issue. First, they renamed the dean’s letter the MSPE. Then the AAMC specifically recommended that the MSPE contain a summary section and that the summary section include a student’s comparative performance in medical school relative to his or her peers. The AAMC further recommended that the summary section define the school-specific categories used in differentiating among the levels of student performance. The AAMC also recommended that the MSPE contain a supplementary appendix D containing a graphic representation of the student’s overall performance relative to his or her classmates, with numerically defined boundaries for the individual medical school’s specific categories. In 2007, in our first paper [6], we documented deans’ continued indifference to compliance with the AAMC recommendations. We echoed the concern of Hunt et al [4,5] that the lack of evaluation accuracy of the MSPE resulted in de facto ceding of this task by the deans of American medical schools to the United States Medical Licensing Examination. The problem with this, we thought, is that the licensing examination scores, however objective, are a thin statistic that offers no insight into a student’s interpersonal or communication skills, medical professionalism, or other domains beyond medical knowledge. This kind of information can be included in a well-written dean’s letter and is information not found elsewhere in the application. Shea et al [1], in a paper published in 2008, shortly after ours, reached many similar conclusions. Importantly, they found that the summary paragraph provided comparative information in only 17% of cases, contrary to the 2002 AAMC guidelines. Most recently, in December 2012, Green et al [7] wrote an op-ed piece in Virtual Mentor: American Medical Association Journal of Ethics titled “Standardizing and Improving the Content of the Dean’s Letter.” Note how similar this title is to that used by Wagoner and Suriano [3] 23 years earlier. Not only the title but the issues discussed have remained the same. Clearly little has changed in the intervening years. Too often it remains difficult to judge a student’s performance from reading the MSPE. To try a new approach to remedy the situation, we set out to develop a database. Our purpose was to create a tool to enable program directors to quickly extract the useful information from the MSPE. METHODS Institutional review board approval was obtained for this project. We reviewed the Electronic Residency Application Service submissions of students from the US AAMCaccredited medical schools [8]. The submissions were for students applying for graduate medical education positions in diagnostic radiology at 3 institutions: North Shore University Hospital (Manhasset, New York), Northwestern University (Chicago, Illinois), and Long Island Jewish Medical Center (New Hyde Park, New York) for the 2012e2013 academic year. There were 239 applicants to the North Shore program, 544 to Northwestern, and 224 to Long Island Jewish. We then reviewed an additional 472 applications to the Northwestern program for the 2013e2014 academic year. The MSPE accompanying each of these 1,479 applications formed the basis for our investigation. We set out to create a comprehensive database. Our intent was that a program director reading an application from an unfamiliar school might access our database and quickly learn what comparative information the individual medical school offered and where in the MSPE, whether in the summary paragraph, an appendix, or another location, this information was located. Furthermore, when comparative information was not included in the MSPE, the database would so inform the user, to prevent fruitless searches. The first column of the database is an alphabetized list of the 141 US AAMC member schools [8], including their full names and their city and state addresses, for easy identification. We next examined the summary paragraphs of the MSPEs to determine what comparative data they included. A rare summary paragraph would contain the exact class ranking of a student. Somewhat more often, the summary paragraph would contain a numerically defined category, perhaps the student’s performance quartile. Most often, the student’s performance was categorized using a descriptor. The most frequently used descriptor was excellent. Often, but not always, the descriptor was used in a defined hierarchy. The most commonly used hierarchy, in descending order, was some variant of outstanding, excellent, very good, and good. The schools would often assign numeric boundaries for each of the descriptor categories. Although the descriptor was frequently included in the summary paragraph, its definition was not. Sometimes this information was located in Appendix D in accordance with the AAMC guidelines. Sometimes the information was included in another location in the MSPE. Sometimes the schools used undefined descriptors. Sometimes there were no comparative data whatsoever. Sometimes the schools would inform readers that it was their intent to offer no comparative data, and other times they would not. Regardless, we searched the MSPEs for whatever school-specific comparative data they might Naidich et al/Medical Student Performance Evaluation 613 contain, and this information was included in a cell next to the school’s name. In this manner we created our database. The design of our database is thus two columns wide. The first column contains the alphabetized medical school names and other identifying information. The second column contains the corresponding data we collected concerning the content of the MSPE (Table 1, online only). Once the database was constructed, it provided the means to investigate a number of interesting questions: 1. We identified the number of schools from which we had no data. 2. We identified the schools from which we had incomplete data. These were schools for which we thought that more examples (larger sample sizes) might be helpful in better understanding the descriptors used in the summary paragraph. 3. We counted the number of schools for which we had complete data. These were schools for which we were confident we had a complete understanding of the MSPE content. 4. We counted how many medical schools would inform readers in the summary paragraph of their students’ comparative performance in order to compare this number to the 17% statistic reported by Shea et al [1]. 5. We looked at use of the descriptor excellent. We counted how many schools used excellent in their summary paragraphs. We looked for schools that used excellent in hierarchies with defined numeric boundaries. For schools meeting this criterion, we then graphed the range of excellent for 2013 (Fig. 1) and compared it with a similar graph reproduced from our 2007 data (Fig. 2). 6. Finally, we looked at the descriptor outstanding. We counted how often schools would use outstanding as a category descriptor for something less than their best performers. Note that we knew from the outset that there would be duplicate submissions for academic year 2012e2013 because the same student might easily apply to 2 or all 3 Fig 1. 2013 Medical Student Performance Evaluation range of excellence data, 41 medical schools. Fig 2. 2007 Medical Student Performance Evaluation range of excellence data, 35 medical schools. Three schools defined the upper but not the lower boundary (blurred) for their descriptors of excellent. programs. We made no effort to correct for this because we thought that repetition would improve accuracy. Subsequently, we did cross-check our lists to determine the number of unique applicants. RESULTS The chief outcome of this project is the database (Table 1). As planned, the database is only two columns wide. It is simple to use. With the database open, a program director or coordinator using the keyboard search function can rapidly locate a medical school of interest. The adjacent cell will detail all the comparative information we were able to find and where these comparative data are located in that school’s MSPE. There were 141 medical schools listed as US members of the AAMC [8]. We had data from all 141 schools. We had incomplete data from 34 medical schools (24%). These were schools that did not define their descriptors. The amount of information we had from these schools varied. At one end of the spectrum were schools from which we had available enough examples to know some but not all of the descriptors used in the summary paragraph. For example, if one school described a student as very good and another student from the same school as outstanding, most probably the second student had performed better than the first. For other schools, we had access to enough student applications to form reasonable estimates of the school-specific category hierarchies, but because the schools did not formally define their hierarchies, we were not completely confident of our estimates. We think that with more examples of the MSPEs from these 34 schools, our database could better describe how these schools stratify their students’ levels of performance. Regardless of our opinion, all we did was label the information cell in the second column of the database “Incomplete Data.” We then included in the cell whatever information we had available concerning each school’s ranking system to allow users to form their own opinions. 614 Journal of the American College of Radiology/Vol. 11 No. 6 June 2014 There were 107 medical schools (76%) for which our data were complete. Of these 107, 13 medical schools were explicit about not ranking their students’ performance. These schools offered no comparative information in their MSPEs. The database will readily identify these schools. There were 88 medical schools that fully described their ranking systems and used well-defined category descriptors with numeric margins. Finally, there were 8 new medical schools that have not yet published MSPEs. Because Shea et al [1] found that 17% of medical schools provided comparative data in the summary paragraph we looked at our own numbers. We found in our survey that only 10 schools (7%) would routinely include comparative information in the summary paragraph. Add the 2 other schools that placed this information next to but not in the summary paragraph, and there were 12 schools (9%) in compliance with this AAMC recommendation. Three additional schools offered this information in the summary section, but only for their better students. Concerning the choice of summary paragraph descriptors, 77 medical schools (55%) used excellent as a descriptor in the summary paragraph, of which 41 (29%) used excellent in a defined hierarchy with defined numeric boundaries. Figure 1 graphically represents the range of excellent used by 41 medical schools in 2013. Figure 2 graphs the range of excellent for 35 medical schools in 2007. Qualitatively, they are similar. Twelve schools used outstanding as their second best category, supplanted 3 times by exceptional, 3 times by distinguished, twice by superior, and once each by most outstanding, top student, superb, and recommend with distinction. Of the 1,479 applications we surveyed, 329 were duplicated or triplicated because the same student applied to more than one program. There were 1,150 unique applications. DISCUSSION There is an inherent conflict of interest between medical school deans trying to make their graduating medical students look as attractive as possible to place them in the best graduate medical education programs available and residency program directors trying to recruit the best performing medical school graduates for their postgraduate programs. Probably this is the reason deans are reluctant to reveal their students’ comparative performance in the summary paragraph or sometimes not reveal it at all. Shea et al’s [1] finding of 17% compliance was based on a survey of students graduating in 2005. Eight years later, we find that compliance has dropped to 9%. Deans may become even more hesitant to provide easily accessible comparative data in the future. The growth of new medical schools is exceeding the expansion of residency training programs [9]. This will make it increasingly difficult for medical schools to place their graduates in the specialty training programs of their choice. Medical schools have adopted a number of approaches to circumvent the AAMC recommendation that the MSPE provide readily accessible data to program directors. One such strategy, used more frequently by the more prestigious schools, is to not rank their students. We found 13 schools (9%) adopting this strategy. Examples include Stanford University and Yale University. Our database can rapidly identify these schools to save readers the effort of searching for nonexistent data. The database cannot, of course, offer insight into applicants’ performance at such medical schools. The drawback of not ranking students is that although it may veil a poorer student’s performance, at the same time, it does not reveal who the better performing students are. To get around this difficulty, some schools will include students’ performance only when it is favorable. Examples include the University at Albany and Northeast Ohio Medical University. Albany uses 3 descriptors in the summary paragraph; recommend highly for the top third of their students, recommend without reservation for the middle third, and recommend as a positive presence for the bottom third. When a student is in the top third of the class, the dean will indicate this in the summary paragraph. However, the dean will not inform the reader in the summary paragraph that recommend without reservation designates the middle third or recommend as a positive presence the bottom third of the class. For most students from Northeast Ohio Medical University, comparative information was not included in the summary paragraph, an explanatory appendix, or elsewhere in the MSPE. However, an exception was made for one student. His standing in the top quartile of the class was proclaimed in boldface type on the first page of the MSPE. A variant of this strategy is to omit from the summary paragraph the student’s ranking when it is at the bottom of the class. Examples are Stony Brook University and Indiana University. The database identifies this tactic. A puzzling strategy used by some schools is to deny ranking their students even when they do use defined categories with numeric margins. Two examples are the University of Chicago and Georgetown University. The database provides the descriptor categories used by these schools and their numeric boundaries. Many schools will use attractive descriptors in the summary paragraph and either not define the descriptors or, more commonly, define their meanings in some location remote from the summary paragraph. The most frequently used descriptor is excellent, a word with a pleasant connotation and ordinary English-language definitions including “exceptionally good” and “of superior merit” [6]. However, MSPE writers assign very different meanings to this word. Figures 1 and 2 show that no school used excellent to describe its very best Naidich et al/Medical Student Performance Evaluation 615 students and also show how frequently excellent was used to describe students in the bottom half of their classes. Whereas the University of Chicago used excellent to describe students ranking between the 5th and 43rd percentiles, The Ohio State University used the same descriptor for students in the 71st to 90th percentiles, and Vanderbilt University used outstanding to describe the top quarter of its class and excellent to describe everyone else. Although an MSPE reader will usually be correct in assuming that outstanding is a category reserved for a school’s best performing students, we found 13 examples (9%) for which this was not true. A program director encountering a descriptor that is undefined in the summary paragraph can reference the database with the expectation that it usually will make clear the school’s idiosyncratic use of the word. One limitation of our database is that it is not complete. We have only partial data concerning 34 medical schools. However, even for these 34 schools, usually there is enough information for the database to be helpful. On the other hand, for the remaining 107 schools, although our data are complete, there are 13 schools for which all the database will reveal is that these schools elect not to offer comparison information concerning their students’ performance. And there are 8 new schools that have not yet begun to write letters. Despite these limitations, we think this is a good start. Another concern is avoidable errors. There is just too much information included in this database for it not to contain some errors. To some extent, our methodology worked in our favor to reduce errors. We reviewed 1,497 MSPEs from 3 different programs. This ensured that there would be multiple different student applications from the same medical school. Furthermore, we were unconcerned that for academic year 2012e2013, the same student might easily apply to 2 or all 3 programs. We welcomed the repetition. We thought the more applications we reviewed, the fewer would be our errors. In all, we had 1,150 unique applications. A third limitation is that what had been true for 2012e2013 may no longer be true for the future. Deans may change their policies from year to year. New schools will begin submitting Electronic Residency Application Service applications. This database might best be looked upon as a work in progress requiring continuous updating. However, if it proves as useful a tool as we hope, as better data become available, users can fill in the gaps and correct the mistakes. If the AAMC, medical school deans, and program directors were ever able to reach a consensus concerning the use of well-defined category descriptors with numeric boundaries, this would enhance the value of the MSPE. Ideally, a student’s class ranking should be based not only on grades but also on nonclinical categories of achievement, including professionalism, research, and community service. The AAMC’s mission [10] does include “supporting the entire spectrum of education, research and patient care activities.” Activities that contribute to this goal, we think, deserve more credit in evaluating a student’s performance. However, for the interim, this database is our solution to medical school deans’ reluctance to provide easily understandable comparative information concerning the performance of their graduating students. The database should speed users’ ability to locate relevant information within an MSPE and to understand an applicant’s performance relative to his or her peers. TAKE-HOME POINTS The summary paragraph of an MSPE should describe a student’s performance in medical school relative to that of his or her peers. Most often, this comparative information is not included in the summary paragraph. Too often, this information is not included anywhere in the MSPE. Accessing the attached database will describe what information is made available from different medical schools. SUPPLEMENTARY DATA Supplementary data can be found online at: http://dx. doi.org/10.1016/j.jacr.2013.11.012. REFERENCES 1. Shea JA, O’Grady E, Morrison G, Wagner BR, Morris JB. Medical Student Performance Evaluation in 2005: an improvement over the former dean’s letter. Acad Med 2008;83:284-91. 2. Association of American Medical Colleges. A guide to the preparation of the medical student performance evaluation. Report of the Dean’s Letter Advisory Committee. Washington: District of Columbia: Association of American Medical Colleges; 2002. 3. Wagoner NE, Suriano JR. A new approach to standardizing the dean’s letter. Acad Med 1989;64:688-9. 4. Hunt DD, MacLarean CF, Scott CS, et al. Characteristics of dean’s letters in 1981 and 1992. Acad Med 1993;68:905-11. 5. Hunt DD, MacLarean CF, Scott CS, et al. A follow-up study of the characteristics of dean’s letters. Acad Med 2001;76:727-33. 6. Naidich JB, Lee JY, Hansen EC, Smith LG. The meaning of excellence. Acad Radiol 2007;14:1121-6. 7. Green MM, Sanguino SM, Thomas JX. Standardizing and improving the content of the dean’s letter. Virtual Mentor 2012;14:1021-6. 8. Association of American Medical Colleges. Member directory search result—medical school. Available at: https://members.aamc.org/eweb/ DynamicPage.aspx?site¼AAMC&webcode¼AAMCOrgSearchResult& orgtype¼Medical%20School. Accessed December 9, 2013. 9. Iglehart JK. The residency mismatch. N Engl J Med 2013;369:297-9. 10. Association of American Medical Colleges. About the AAMC. Available at: https://www.aamc.org/about/. Accessed December 9, 2013.