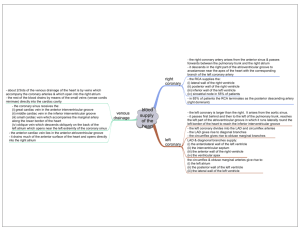
ANATOMY OF CORONARY CIRCULATION mangala_kumari@imu.edu.my Learning Outcomes To explain the origin and course of right and left coronary arteries. To name the branches of right and left coronary arteries. To name the areas supplied by the right and left coronary arteries. To describe the coronary sinus and its tributaries. To identify the right and left coronary artery branches on the coronary angiogram. To understand certain coronary artery anomalies. Coronary arteries Branches of ascending aorta Right coronary artery – arises from right coronary sinus of Valsalva which lies anteriorly (anterior sinus of Valsalva / anterior aortic sinus) Left coronary artery – arises from left coronary sinus of Valsalva (left sinus of Valsalva / left aortic sinus) Aortic valve- three leaflets, each having a cusp or cup-like configuration. Left coronary cusp (L), Right coronary cusp (R) and Posterior non-coronary cusp (N). Just above the aortic valves there are anatomic dilations of the ascending aorta, known as the sinus of Valsalva. Right coronary artery Right coronary sinus of Valsalva Between pulmonary trunk and right auricle Right A-V groove (Anterior part) (coronary groove) Winds round inferior border Right A-V groove (Posterior part) (reach the crux) Right coronary artery Branches Sinuatrial (SA) nodal br. (In 40% originate from Cx) Conus a. (In 20 -30% direct br. of aorta) Right marginal br. (acute marginal a./AM) PDA/Posterior descending a. (post. interventricular a.) – 20% cases from CX Atrioventricular (AV) nodal br. Conus a. Left coronary artery Left coronary sinus of Valsalva Passes behind pulmonary trunk Appears between pulmonary trunk & left auricle LAD/ left anterior Circumflex A. descending A. (Ant. Interventricular A.) Winds –left border (Ant. interventricular groove) Left A-V groove Left coronary arteryBranches LAD/ Left ant. descending a. (Ant. interventricular a.) Diagonal a. Circumflex br. Marginal br. Coronary Arteries Coronary Dominance Dominance refers to whether the PDA originates from the RCA (right dominant), CX (left dominant), or both (co-dominant) Approximately 80% - right dominant. RCA at crux bifurcates into the PDA and a postero-lateral branch. The PDA courses in the posterior ventricular septum giving origin to the AV nodal artery and posterior interventricular branch. In left dominance, the PDA originates from the CX. In co-dominance, there are right and left PDAs originating from the RCA and CX. Areas supplied by: Right coronary artery Right atrium Right ventricle (most part) Part of left ventricle Posterior 1/3rd of interventricular septum SA node AV node Left coronary artery Left atrium Left ventricle (most part) Part of right ventricle Anterior 2/3rd of interventricular septum AV bundle Veins of the heart From the cardiac capillaries, blood flows back to cardiac chambers through venules, which in turn coalesce into cardiac veins. 60% venous blood is collected and drained into right atrium- Coronary sinus 40% venous blood drained by Venae cordis minimi (Thebesian veins) – drain into different chambers of heart Anterior cardiac veins – directly drain into right atrium Coronary sinus 2-3 cm long, lies in the post. part of A-V groove. Begins in left part of A-V groove where it receives the great cardiac vein. Passes downwards to the right side of A-V groove. Opens into the sinus venarum of right atrium Opening is guarded by incomplete semilunar valve Coronary sinus – Tributaries Great cardiac vein - runs along anterior interventricular groove. Receives left marginal vein close to termination. Middle cardiac vein – runs along posterior interventricular groove. Small cardiac vein - lies in A-V groove between right atrium and right ventricle Receives right marginal vein. Posterior vein of left ventricle Oblique vein of the left atrium Coronary angiogram Right coronary artery http://www.youtube.com/watch?v=Eoq9yrT-Ejk Coronary angiogram Left coronary artery 70% stenosis in third obtuse marginal branch (arrow head) stenosis of proximal first diagonal branch (open arrow) Coronary anomalies Anomalous origin of the LCA from the right sinus of Valsalva and the LCA courses between the aorta and pulmonary artery. This interarterial course can lead to compression of the LCA (yellow arrows) resulting in myocardial ischemia. Coronary anomalies ALCAPA - Origin of the LCA from the pulmonary artery. Results in the left ventricular myocardium being perfused by relatively desaturated blood under low pressure, leading to myocardial ischemia. ALCAPA is a rare, congenital cardiac anomaly accounting for approximately 0.25-0.5% of all congenital heart diseases. Approximately 85% of patients present with clinical symptoms of CHF within the first 1-2 months of life. Anomalous Left Coronary Artery arising from the Pulmonary Artery Coronary anomalies Myocardial bridging Commonly observed of the LAD The depth of the vessel under the myocardium is more important that the length of the myocardial bridging. Fistula Large LAD giving rise to a large septal branch that terminates in the right ventricle (blue arrow).