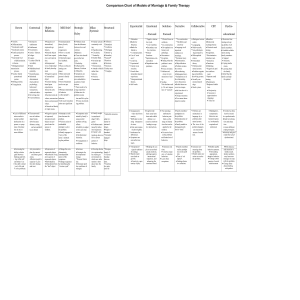
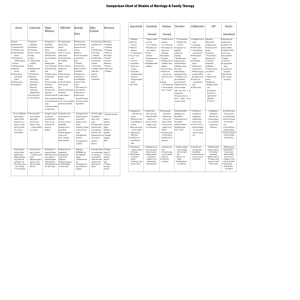
Comparison Chart of Models of Marriage & Family Therapy Bowen Contextual ♦ Anxiety. ♦ Differentiation. * Emotional cutoff. * Emotional system. ♦ Family projection process. * Functional level of differentiation. ♦ Fusion. * Multigenerational transmission process. ♦ Nuclear family promotional system. ♦ Sibling position. ♦ Triangulation. ♦ Lack of differenti ation results in marital conflict dysfunction in a spouse, or symp toms of dysfunc tion in one or more children. Object Relations Strategic Haley ♦ Projection of internalized, repressed ego objects. ♦ Internal objects built from experi ence and expecta tion. ♦ Interpersonal view of individual & family develop ment ♦ Negative aspects of internalized object ♦ Current relating based upon expectations formed in early experience. ♦ Societal norms & values, unconscious behavior. forces and personal ♦ Life cycle transition points are significant values. ♦ Unresolved family of origin issues. tion and life cycles. ♦ Focus on presenting problem. ♦ The trustworthi ness of relation ships breaks down because fairness, caring and accountabili ty are absent ♦ Negative aspects of repressed, introjected early objects are pro jected onto the spouse or children. ♦ Attempts at solu tions become the problem. ♦ Vicious cycles of mishandled attempts to solve the problem. ♦ Family engages in “more of the same”, maintain ing the problem. ♦ Symptoms main tained by family’s unsuccessful problem solving efforts. ♦ Inability to adjust to life cycle tran sitions. ♦ Dysfunctional hierarchy. ♦ Family caught up in unacknowl edged “dirty game”. ♦ Problems main tained by behav ioral sequences. ♦ Family’s old epistemology does not fit its current ♦ Triangulation or coalitions. pattern of behavior. ♦ Change the complimentarity, interdependent nature of the symptoms. ♦ Change sequences by identifying the “viscious cyde”. ♦ Increase flexibility. ♦ Strategies for developmental change. * Reassert hierar chy. ♦ Eliminate prob lem coalitions & triangles. ♦ Develop alterna tive episteraology by creating an environment in which new infor mation is intro duced into the family. . ♦ A preventative plan for current and future gener ations. ♦ Restore people’s capacity to give thru fair relating and trust. ♦ Expression of repressed objects. ♦ Resolution of neg ative aspects of repressed objects. ♦ Individuation. ♦ Detachment from the “bad” object ♦ Communication theory (levels, rules & congruence). ♦ First vs. second order change. ♦ Cybernetics/posi tive feedback loops. ♦ Focus on the pre senting com plaint ♦ Most motivated person in family is used. ♦ Unit of treatment can be one per son. ♦ Primary determinant of behavior is other people’s ♦ Problems stem from the dilemma between love and violence (Madanes). ♦ Clear rules should govern the hier archy. * Flexibility. ♦ Influenced by Bateson, Erickson & Minuchin. ♦ Symptoms are communicative acts embedded in a pattern of inter actions. * There needs to be a large repertoire of behaviors for problem resolu Milan Systemic * Destructive entitlement ♦ Entitlement ♦ Exoneration. ♦ Justice / fairness. ♦ Ledger. ♦ Legacy. * Loyalty (filial & invisible). ♦ Merit ♦ Multidirectional partiality. * Parentification. ♦ Relational determinants (facts,individ. psychology, behavioral transactions, relational ethics. ♦ Revolving slate. ♦ Trustworthiness. - ♦ Increasing the ability to distin guish between thinking and feeli. ing within self and others. Use f this skill to direct | one’s life and V solve problems. MRI Brief ♦ Family system is constantly evolv ing. ♦ Hypothesizing. ♦ Circularity. * Neutrality. ♦ Double Bind. ♦ Invariant pre scription. * Homeostasis. ♦ Attend to beliefs rather than behavior. ♦ Positive Connotation. Structural ♦ Alliances. * Boundarie * Coalitions * Disengage * Detouir^g ♦ Enmeshrj * Parentif* * Restricts ♦ Structure. * Structura * Subsy stem * Triangles. * Inflexible structure adapt to i mental m uational i lenges. ♦ Rigid or < boundari * Enmesbe engaged ships. * Reorgaa family s* * Clear aa booadac berweea tems. * Funcboa tive pata assist di Experiential * Alienation. ♦ Battle for Structure. ♦ Battle for Initiative. * Communication. ♦ Use of “crazi ness”. * Creativity. * Experiential. * Family recon struction. * Growth thru immediate shared experience. * Intergenerational themes. ♦ Self worth. Emotional Solution- Narrative - Focused Focused * Negative interac tion cyde. * Core Conflicts ♦ Secondary reac tive emotions. * Primary Emotions * Separateness-connectedness ♦ Dependence-independence. * Clinical focus on solutions. * Co-construction. ♦ De-emphasis on history and pathology. ♦ Deconstruct * Exception. ♦ Finding when the problem is not a problem. ♦ Focus on future. * Problem and cause are con structions of real ity. ♦ Scaling. * No absolute reali ty. Do not impose view of “normal”. * Co-construction. * Flexibility and creativity ♦ Language is all important emphasis on meanings. * Dominant story. ♦ Hermeneutics. ♦ Objectification. ♦ Problem creates the system. ♦ Re-authoring. ♦ Subjugated story. * Symptoms are in the relationship, not in the person. ♦ Beliefs about an event are insepa Collaborative CBT Psychoeducational ♦ Dialogical conver sation. * Languaging. ♦ Multiversatile. * Non-pathologizing perspective. ♦ Philosophical stance. ♦ Postmodern theory. * Problem-deter mined system. ♦ Problem-organiz ing and problemdissolving system. ♦ Socially con structed knowl edge. ♦ Stuck system. ♦ Couples hide their actual emo tions and exhibit defensive or coercive emotions leading to nega tive interactions. ♦ The meanings attributed to behavior puts limits on the range of alterna tives that can be applied to the solution. ♦ Excessive focus on the problem and limited set of behaviors. ♦ Family members’ partidpation in the problem. ♦ Internalization of the problem. ♦ Family unable to distinguish prob lem in “time”. ♦ “Desperation” signals readiness for change. ♦ Shared experi ence leads to growth. ♦ Creativity, spon taneity & play. ♦ Helping the cou ple to access their actual emotions, altering negative interactional sequences, and enhancing the emotional bond. ♦ Generate solu tions. ♦ Creative expan sion of solution behaviors. ♦ Learn from exceptions. ♦ Family members realize partidpa tion in the prob lem. ♦ Time is “col lapsed”. ♦ Finding alterna tive solutions. ♦ Maximize \ , ; func tioning and cop ing ability of all family members. ♦ Establish collabo ration among family members. ♦ Support ♦ Structure. ♦ Coping mecha nisms. ♦ Learning from the family. ♦ Belief that the family can help the patient ♦ Reciprocity. ♦ Successive approximation (shaping). ♦ Time-out rable from how it is experienced. ♦ Unique outcomes. ♦ You cannot know objective reality. ♦ Scapegoat pro vides relief from anxiety. * Difficulty in toler ating interperson al stress. ♦ Role and commu nication rigidity. * Intolerance for differences. ♦ Symptoms are nonverbal mes sages. ♦ Baseline. ♦ Behavioral exchange theory. ♦ Classical condi tioning. ♦ Cognitions. * Discriminative stimulus (cue). * Extinction. ♦ Functions. ♦ Modeling. * Negative & posi tive reinforce ment * Operant condi tioning. ♦ Punishment. * Redprocal inhibi tion. * Problems are maintained in language by a problem-deter mined system. ♦ The view of the problem hampers any successful means of resolu tion. ♦ Maladaptive, symptomatic behaviors are learned respons es, involuntarily acquired and reinforced. ♦ Generate new meaning about the problem. ♦ Family takes new action to resolve the problem. ♦ Modify spedfic behavior patterns. ♦ Rewarding appropriate, adaptive behavior. ♦ Change contin gencies of social reinforcement ♦ Family has beea hurt by insensi tive professionals. ♦ Need for informa tion and educa tion. ♦ Learn different coping strategies. ♦ Anxiety and grief render the lamah dysfunctional. ♦With edncascc and attention to family needs. family members may learn new strategies to cope with the problem. ♦ Change ideas about (leafing with paftrwt. Bowen * Emphasize extended family. * Entire family need not be present * Use of genogram. * Reduce anxiety ♦Increase differentiation. * Open communication, resolve triangles. Neutral. * Objective. * Coach. * Process over content * Genogram. * “I” position. * Detriangulation. * Create therapy triangle. * Often long term. * Self-reports. * Level of differentiation use of scale. * Degree of cut-off. * Level of family anxiety and reactivity. * Triangles. Contextual * Unit of treatment is chosen by therapist * Engagement * Cognitive exploration of fam. history. * Alter perceptions. * Expand trust to increase options.* * Active. * Personal. * Co-therapy. * Relational balances. * Catalyist * Advocate for all. * Multidirectional partiality. * Listening. * Observing. * Responding to unconscious material. * Therapist decides whom to see. * Couple therapy is not separate modality. ♦Focus on family resources. * Observations made on aO 4 dimensions. * Assessment is an ongoing process. * Developmental stage and interpersonal Ioy allies lead to beliefs. * Triangles assessed. Object Relations MRI Brief Strategic Haley Milan Systemic Structural Experientia l * Entire family present * Join from p« of leaders * Map underb structure. * Interventio n transform ti structure. * Short-term Solution- - Focused Focused * Engagement * Projective identification. * Confrontation. * Termination. * Often long terra. * Setup and definition of the problem. * Identify & interrupt behavior maintaining the problem. * Set goals. * Intervention. * Termination. * Short-term therapy. * Initial interview: 1. Social. 2. Problem ident 3. Interactional. 4. Goal setting. * Observation. * Intervention. * Termination. * Short-term therapy. * Non-directive^ * Observer. * Insight and understanding. * Active. * Clients are viewed as customers. * Attend to process over content. * Team and one way mirror often used. * Active and deliberate. * Join with the family. * Responsible for therapy. * Presenting problem. * Use language of the family. * Observer. * Mixed gender treatment teams. * Neutrality. * Ways to think differently. * Generate hypotheses. ♦ Most motivated person in system. * Symptom-focused. ♦ Tasks. * Paradox & reframe. ♦ Encourage interaction. ♦ Observe sequences. ♦ Define maladaptive sequences. * Problem resolution. * Non-historic. * Symptomfocused. * Sequence of symptom-main taining behaviors. ♦ Instances of circu lar causality. * Directives, direct and paradoxical. * Enactment * Feedback. * Pretending. * Ordeals. * Reframing. * Hypothesizing. * Circularity. * Neutrality. * Invariant prescription. * Rituals. * Paradox. ♦Positive Connotation. * Joining/acc t dating. * Diagnosing. * Modify intes tions. * Boundary * Unbalancing * Challenging * Enactments * Reframing. * Tasks. * Paradox. ♦ Metaphor. ♦ In-session interaction. ♦ Sculpting (Satir). ♦ Family reconstruction. ♦ Parts Party (Satir). ♦ Temperature reading. Changing interactional positions. ♦ Information learned before meeting is used in formulating the hypothesis. ♦ Hypothesis leads directly to interventions. ♦ Family stra ♦ System flerij ♦ Family maf ♦ Enmesh me disengages ♦ Family life < ♦ Family dew mental staf ♦ Observatia session. ♦Degree of anxiety. ♦ Battles for Initiative & Structure. * Therapist’s own feelings. * Degree of separateness; ability to play. ♦ Intergenerationa l themes & life cyde. ♦Desire for change. ♦ Delineate the issues presented by the coup and assess how these issues express core conflicts in the areas of separateness-connectedness and depen denceindependence. ♦ Identify the negative interaction cyde. ♦ Access unacknowledged fedings underlying interactional positions * Listening. * Observing. * Responding to unconscious material. * Interpreting. * Developing insight * Self-report * Family of origin history. * Defensive system of the family. ♦Individuation. * Intrapsychic material. ♦ Non-historic. ♦ Family life cycle transition points. ♦ Self-report ♦ Observing family ineractions. * Entire family seen. * Pre-session. * Session interview. * Hypothesis testing. * Team discussion. * Therapist presents conclusions. * Post-session. * Short-term theapy. Emotional * Active. * Involved. * Leadership. * Gather information. * Increase affect and expressiveness. * Expansion of self. * Termination upon achieving goals. * Satir: making contact, chaos, integration.* Pretreatment, middle, late phases. * Involved & active. * Self-disclosing, warm, responsive, positive. * Consultant * Alternating between provocation and support * Delineate core the negative interaction cycle. * Access underlying interactional positions. * Redefine the problem. * Promote identification with disowned needs and aspects of self„ * Promote acceptance of each partner’s experience. * Restructure the interaction. * Generate new solutions. * Consolidate new positions. * Identify Narrative Collaborative CBT Psychoeducational * Initial session: previous solutions, exceptions, goals, tasks. * Later sessions: feedback on tasks, perception of change, exceptions. * Termination: upon reaching goals. * Brief therapy. * Externalizing the problem. * Relative influence. * Collapsing time. * Raising dilemmas. * Setting experiments. * Short-term therapy- * Therapy is a continuous process. * Focus on language. * Dialogical conversation. * Termination col Iaboratively determined. * Directive. * In control. * Engage in solution oriented con versation. * Co-create system with the family. * Neither direct nor indirect * Clients have voice in treatment process. * Multipartial. * Not knowing. * Honor client’s reality. * Listener. * Responsive. * Compassionate. * Egalitarian partnership; coexplorer. * Directive. * Teacher. * Coach. * Model. * Reinforcer. ♦Active. * Learn from faash. * Direct & empathic. * Provide information. * Brief therapy. ♦ Complimenting. ♦ Formula first-session task. ♦ Scaling questions. ♦ Miracle question. ♦ More of the same. ♦ Questions and summaries. ♦ Externalizing problems. ♦ Dilemma questions. ♦ Escape meetings. ♦ Note taking/sharing. ♦ Landscape of action & meaning questions. ♦ Certificates. ♦ Therapeutic letters. * Family’s experience of the problem. * Language of the family. * Ways that family members participate in the problem. * Conversational questions. * Not-knowing approach. * Reflecting Team. * Shared inquiry. * Operant techniques (shaping, token economy, contingencies) * Respondent con ditioning (desen sitization, assertiveness, aversion). * Cognitive affective (thoughtstopping, rational emotional). ♦ Function of * Parenting training maladap tive and contracts. behaviors. * Remo e Miw ♦Unconditional positive regard. * Identify solutions. * Can family identify exceptions? * How does the family answer the miracle question? * Can family follow thru on interventions? * Degree of focus. * Shared inquiry. * Presentation of problem by client system. * Conversational questions utilized in assessment. * Identification of problem behavior. * Behavioral goals. * Behavioral interventions & homework. * Sympto m removal. * Termination. * Brief therapy. ♦ Sequences with embedded problems. ♦ Interview/self-report ♦ Observation of problem-solving & communication. ♦ Functional analysis of behavior. * Initial interview. * Information star ing. * Other resources. * Assigning tadi. * Respond to prob Iems in family structure. * FjiwinrapF * Contracting. * Survival Sk3b Workshop. * Training with family. * Lowering expectations. ♦ History of the problem * Evaluate fiat's understands^ :/ * Evaluate bash i needs for iafor maticn. ♦ Evaluate attempts at t