IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 55, NO. 3, MARCH 2008
1237
Gait Simulation via a 6-DOF Parallel Robot
With Iterative Learning Control
Patrick M. Aubin, Matthew S. Cowley, and William R. Ledoux*
Abstract—We have developed a robotic gait simulator (RGS) by leveraging a 6-degree of freedom parallel robot, with the goal of overcoming
three significant challenges of gait simulation, including: 1) operating at
near physiologically correct velocities; 2) inputting full scale ground reaction forces; and 3) simulating motion in all three planes (sagittal, coronal
and transverse). The robot will eventually be employed with cadaveric specimens, but as a means of exploring the capability of the system, we have first
used it with a prosthetic foot. Gait data were recorded from one transtibial
amputee using a motion analysis system and force plate. Using the same
prosthetic foot as the subject, the RGS accurately reproduced the recorded
kinematics and kinetics and the appropriate vertical ground reaction force
was realized with a proportional iterative learning controller. After six gait
iterations the controller reduced the root mean square (RMS) error between the simulated and in situ vertical ground reaction force to 35 N during
a 1.5 s simulation of the stance phase of gait with a prosthetic foot. This
paper addresses the design, methodology and validation of the novel RGS.
Index Terms—Gait simulation, iterative learning control, kinematics,
kinetics, prosthetics.
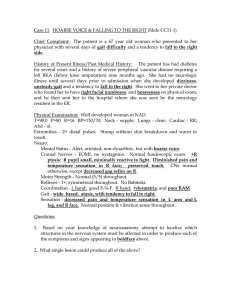
Fig. 1. The R-2000 Rotopod, with the (A) motors, (B) support frame, (C) prosthetic foot mounted to the frame, (D) force plate, and (E) mobile platform. The
inset shows a drawing of the R-2000 removed from the surrounding steel frame.
I. INTRODUCTION
Dynamic in vitro gait simulators have been useful tools for biomechanical researchers studying the foot and ankle. In contrast to modeling with living subjects, in vitro models often provide direct access
to the variables of interest. Measurement techniques too invasive for
living subjects, such as using bone pins to quantify bony motion or
strain gages to measure bone or fascia strain, are often employed. Beyond that of static models, dynamic simulators can provide additional
insight into the functional role of the foot and ankle during locomotion.
Several research teams have created dynamic in vitro foot and ankle
models that recreate the kinematics and ground reaction forces (GRFs)
of the stance phase of in vivo gait [1]–[4]. While greatly advancing the
state of the art, these gait simulators all suffer from one or more of the
following potential limitations: scaled gait simulation speeds (2–60 s)
[1]–[4], simplified rigid body motion of the tibia [1]–[4] or scaled GRFs
for cadaveric specimens (40–50%) [2]–[4]. Our research objective is to
design and implement a novel in vitro robotic gait simulator (RGS) capable of simulating the kinematics and kinetics of the foot and ankle
during the stance phase of gait. As an initial step, and for the scope of
Manuscript received November 13, 2006. This work was supported in part by
the Office of Research and Development, Rehabilitation Research and Development Service, Department of Veterans Affairs, under Grant numbers A2661C
and A3923R. Asterisk indicates corresponding author.
P. M. Aubin is with the VA RR&D Center of Excellence for Limb
Loss Prevention and Prosthetic Engineering, VA Puget Sound Health Care
System, Seattle, WA 98108 USA, and with the Department of Electrical
Engineering, University of Washington, Seattle, WA 98195 USA (e-mail:
paubin@u.washington.edu).
M. S. Cowley is with the VA RR&D Center of Excellence for Limb Loss
Prevention and Prosthetic Engineering, VA Puget Sound Health Care System,
Seattle, WA 98108 USA (e—mail: matthew.cowley@comcast.net).
*W. R. Ledoux is with the VA RR&D Center of Excellence for Limb Loss
Prevention and Prosthetic Engineering, VA Puget Sound Health Care System,
1660 South Columbian Way, MS 151, Seattle, WA 98108 USA, and the Department of Mechanical Engineering and the Department of Orthopaedics and
Sports Medicine, University of Washington, Seattle, WA 98195 USA (e-mail:
wrledoux@u.washington.edu).
Digital Object Identifier 10.1109/TBME.2007.908072
this paper, we have focused on the simulation of transtibial amputee
gait. This serves two purposes: first, it provides a simple test case in
which questions regarding our methodologies and hardware can be investigated and answered, and second, it produces a system that can potentially be employed in the future to study and develop prosthetic feet,
although this is not our intended primary goal. The conclusions drawn
from the prosthetic gait simulations will be integrated into future cadaveric gait simulations.
II. MATERIALS AND METHODS
A. Living Subject Gait Data Collection
One gait trial was collected from a healthy 59–year-old male
transtibial amputee. The motion analysis system was a 12-camera
Vicon system (Vicon; Lake Forest, CA) collecting at 250 Hz. The
force plate (Bertec Corporation; Columbus, Ohio) recorded the GRF
at 1500 Hz. A certified prosthetist replaced the subject’s prosthetic
foot with a replacement foot (FS 1000 freedom, Freedom Innovations,
Inc.; Irvine CA, i.e., the same model that the subject normally wore);
this foot was used for the remainder of both the subject and robotic
tests. A tibia coordinate system (TCS) was constructed with the x-axis
pointing anteriorly, the y-axis pointing superiorly and z-axis pointing
medially (for a left leg). During a gait trial, the motion of the TCS
was recorded with respect to the lab coordinate system (LCS), an inert
reference frame located on the ground next to the force plate.
B. Robotic Gait Simulator
The RGS consists of a force plate (Kistler Instrument Corporation;
Amherst, NY) mounted to a 6-degree of freedom parallel robot named
the R-2000 (Parallel Robotics Systems; Hampton NH), which is surrounded by a steel mounting frame (Fig. 1). The R-2000 design is similar to a classic Stewart platform, with a base, six legs and a mobile
platform. Unlike a normal Stewart platform the R-2000’s legs are of
0018-9294/$25.00 © 2008 IEEE
1238
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 55, NO. 3, MARCH 2008
fixed length, and the mobile platform is positioned by moving the base
of the legs around a circular steel ring.
We described the pose of the mobile platform with six parameters,
(x y z roll pitch yaw). These parameters state the translation and
Cardan angle rotation of the tool frame (TF) with respect to the base
frame (BF). The BF is a world reference frame fixed relative to both
the laboratory and base of the robot. The TF is a body fixed coordinate
system attached to the top center of the mobile force plate.
The RGS uses relative motion to simulate the kinematics and kinetics
of a transtibial amputee gait. During a simulation the pylon was held
rigidly in place while the “ground” (a vertical force plate mounted to the
robotic mobile platform) was moved by the R-2000 in order to create
the physiologically correct relative pylon-ground motion.
To simulate gait with the R-2000, the trajectory of the LCS (ground)
with respect to the TCS (pylon) was solved for in terms of a trans~TCS LCS (n),
lation vector from the TCS origin to the LCS origin, p
and the triplet of ZXY Cardan angles, f (n); '(n); (n)g, where
n denotes the sample number. The prosthetic foot was mounted
relative to the R-2000 such that the TCS is identical to the BF.
With this configuration the discrete time trajectory given by the set
fp~TCS LCS (n); (n); '(n); (n)g will correctly position and rotate
the TF of the mobile platform with respect to the BF in the same way
the LCS translates and rotates with respect to the TCS during the in
situ stance phase of gait.
In order for the simulated vertical GRF to accurately match the in
situ vertical GRF the TCS would have to be perfectly aligned to the
R-2000’s BF. Prosthetic foot mounting inconsistencies and recorded
living subject gait data positional noise contribute to simulated vertical
GRF errors. Rather than manually fine tuning the position of the prosthetic foot, the RGS uses iterative learning control (ILC) [5] to adjust
the kinematics of the R-2000 between gait iterations to achieve the desired GRF. Real time force feedback of the R-2000 is not feasible with
the robot’s positional eight-move buffer system.
During each gait simulation the R-2000’s motion was controlled via
a closed loop PID position feedback controller. After a gait simulation
the recorded vertical GRF was automatically analyzed and the motion
of the R-2000 was adjusted with the purpose of altering the vertical
GRF during the stance phase of the simulated gait. These new motion
commands were saved and used in the next gait iteration. The only
trajectory parameters that were changed between iterations by the ILC
algorithm were p
~TCS LCS (n) (i.e., the x, y, and z translations of the
TF), while (n); '(n); (n) remained constant. An increase in the
vertical GRF at time step n was accomplished by changing the location
of the TF origin at time step n. Incremental motion of the TF origin
between iterations was prescribed only in the direction normal to the
force plate surface. This normal direction was unique for each time step
n. This technique decoupled changes to the vertical GRF from changes
to the shear GRF.
To prove stability and iteration domain tracking of the target vertical
GRF during a simulation, we modeled the vertical component of the
force developed between the force plate and the prosthetic foot by a
simple time-varying linear spring
1
FGRE j = Kreal uj
(2)
where Kreal is a diagonal matrix defined as
kreal (1)
Kreal =
0
..
.
0
0
kreal (2)
...
0
...
0
..
.
0
..
.
...
(3)
kreal (i)
where i is the number of time steps in the gait simulation.
The iterative control law is then written in the iteration domain as
C. Iterative Learning Control
FGRF (n) = kreal (n) 1 [ 0
where p
~BF TF (n) is a translation vector from the BF origin to the TF
origin with respect to the BF. We define, p
~0 (n) by creating a special trajectory fp
~0 (n); (n); '(n); (n)g such that at every instant
n the force plate is just touching the plantar surface of the prosthetic
foot but not exerting any force. This trajectory uses the rotation angles
( (n); '(n); (n)) recorded from the living subject. These rotation
angles also define the rotation matrix RTF BF (n), (i.e., RTF BF (n) =
T
T
RBF
TF (n) = (Rz ( )Rx (')Ry ( )) ). The spring constant of the
prosthetic foot at time step n is given as kreal (n). The vertical GRF due
to the compressed prosthetic foot at discrete time step n is FGRF (n).
The error between the desired and actual vertical GRF at time step
n is defined as e(n) = FGRF (n)target 0 FGRF (n)actual . Let u(n) =
[ 0 1 0 ] 1 RTF BF (n) (p
~BF TF (n) 0 p~0 (n)) and further define, uj ,
FGRF j and ej as column vectors giving the complete history of the
input u(n), output FGRF (n) and error e(n) for iteration j . This allows
us to write the output vertical GRF at iteration j as
0]
1 RTF BF (n) 1 (p~BF TF (n) 0 p~0 (n))
(1)
uj = uj 01 + Lej 01
(4)
where L is the learning gain matrix. After manipulating (2) and (4) the
iteration domain error in the vertical GRF is given as
ej = (I 0 Kreal L)j e0 :
(5)
The requirement for iteration domain stability and vertical GRF
tracking is based on the eigenvalues of [I 0 Kreal L], namely
ji [I 0 Kreal L]j < 1:
(6)
Assuming the learning gain matrix L is diagonal reduces the stability
criterion to
j1 0 kreal (n)Lnn j < 1
for n = 1 . . . i:
(7)
An optimal control gain such as, Lnn = 1=kreal (n) was not attempted because we do not want the determination of kreal (n) to be a
prerequisite for gait simulation. Rather a learning gain of Lnn 0:07
for all n was shown to be effective.
D. Inertial Compensation
During a simulation the force plate is accelerating and decelerating
its mass in order to reproduce the in situ ground kinematics. Thus the
output measured by the force plate is actually the sum of both the force
from the prosthetic foot and forces resulting from the acceleration and
deceleration of the force plate mass. Mathematically, the force plate
output (Fmeasured j ) can be written as
Fmeasured j = FGRF j + maj :
(8)
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 55, NO. 3, MARCH 2008
Fig. 2. Comparison of the in situ vertical GRF to the simulated vertical GRF
for a 1.5 s simulation. The GRF is always less than body weight due to abnormal
center of mass acceleration caused by the prosthetic limb.
Where FGRF j is a column vector containing the entire vertical GRF
for iteration j ; m is the mass of the force plate; and aj is a column
vector containing the y-axis component of the acceleration of the TF
with respect to the BF as expressed in the TF coordinate system for
iteration j .
In order to track the target vertical GRF and perform the simulations
at 1.5 s our approach was to first perform slow speed simulations at 6.0 s
until good vertical GRF tracking with the ILC was observed (i.e., after
N iterations). Then the kinematics were held constant and, with the ILC
turned off, the simulation was sped up to 1.5 s and Fmeasured N +1 was
obtained. After removing the prosthetic foot the same N +1 kinematics
and kinetics were performed for iteration (N + 2) and the inertial force
(maN +2 ) was measured repeatedly nine times and averaged. Because
the target (N + 1)th kinematics are the same as the target (N + 2)th
kinematics we can assume that, maN +1 maN +2 . Finally the vertical GRF for the (N + 1)th iteration simulation was determined by
F
GRF N +1 = Fmeasured N +1 0 maN +1
Fmeasured N +1 0 maN +2 :
(9)
The vertical GRF for the N th + 1 iteration simulation was then compared to the in situ vertical GRF and an RMS error calculated.
III. RESULTS
A. Living Subject Gait Data
The living amputee GRF curve with three peaks all below body
weight is somewhat unusual as compared to non-amputee gait (Fig. 2).
Tracking this arbitrary shape demonstrates the RGS’s ability to simulate patient specific gait data. The sagittal, frontal and transverse angular rotations that describe the TCS with respect to the LCS were determined (Fig. 3).
B. Simulation Results
The living subject gait data (Fig. 3) were used as the inputs to the
RGS. Due to motor velocity constraints the fastest possible simulation
with our device in its current configuration was 1.5 s, rather than 0.75 s.
During the six iterations of learning the RMS error was reduced from
78.73 N to 9.42 N (Fig. 4). The exponential decay of the error was
expected and consistent with the derivation for the iteration domain
1239
Fig. 3. Rotation of the pylon during the stance phase of in situ gait. Positive
sagittal rotation is defined as the proximal end of the tibia moving posteriorly.
Positive frontal rotation is defined as the proximal end of the tibia moving medially. Positive transverse rotation is defined as the forefoot moving laterally
(external rotation).
Fig. 4. RMS error history for the iterative learning control (ILC).
convergence of tracking, ej = (I 0 Kreal L)j e0 . Once the RMS error
between the simulated and in situ vertical GRF was minimized, the
kinematics were held constant and the simulation speed was increased
to 1.5 s for iteration seven; the force plate output was again measured
and the RMS was recalculated as 39.2 N (Fig. 2).
This increase in RMS error from 9.42 to 39.2 N was due to increased
inertial forces. After measuring the force plate output for iteration 7, the
prosthetic foot was removed and nine inertia only force curves were
recorded. The mean inertia only force curve was calculated (Fig. 5).
The inter-iteration standard deviation of the inertia only force curves
was between 1.0 N and 15.0 N, with a mean of 3.0 N.
To estimate the vertical GRF (i.e., the force “felt” by the prosthetic
without the inertial forces) the mean inertial force was subtracted from
the force plate output as shown in (9). The RMS error between the
estimated vertical GRF and the in situ vertical GRF was 35.0 N (Fig. 2).
IV. DISCUSSION
In order to compare and contrast different gait simulators it is useful
to have a set of performance metrics. The performance characteristics
of interest are: simulation DOF, velocity, inter-simulation kinematics
adjustability and fidelity of the GRF. By fidelity of the simulated GRF,
we mean whether or not the GRF is scaled and how well the simulated
GRF tracks normative data.
1240
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 55, NO. 3, MARCH 2008
While the performance of the RGS is promising, we must acknowledge in our comparison that cadaveric gait simulation is far more complex then prosthetic gait simulation. Prosthetic gait simulation has a
simple and repeatable system under load while cadaveric gait simulation has a complex and variable system that also requires muscle tendon
actuation.
V. CONCLUSION
Fig. 5. Inertial force for a 1.5 s simulation. The zoomed in view provided as an
inset shows the repeatability of the nine inertial force curves.
Currently most gait simulators allow for two tibia translations and
one sagittal plane tibia rotation [1], [3], [4]. Hurschler et al.’s simulator
also has a total of 3-DOF, i.e., one translation, superior and inferior and
two tibia rotations, sagittal and transverse [2]. In comparison, the RGS
simulates three tibia translations and three tibia rotations.
The working velocity of some gait simulators are much slower than
are physiologically correct [1], [2], [4] making them quasi dynamic.
Nester et al.’s gait simulator is the fastest, simulating the stance phase
of gait in 2 s [3]. The RGS operates currently at 1.5 s, slower than what
is physiologically correct, but an order of magnitude faster than most
other simulators.
Inter-simulation kinematics adjustability is important if one wants to
simulate a variety of gait patterns. In order to do so, the gait simulator
must have the ability to prescribe different tibia kinematics between
simulation trials. Currently only the RGS and Hurschler et al.’s gait
simulator [2] have the ability to do this easily because their kinematics
are specified in software rather then dictated by hardware. (This issue
has also been addressed with Sharkey et al.’s newest gait simulator,
which no longer requires that the tibia move along a fixed cam profile
[6].) The range of rotational motion of the R-2000, 615 in both the
transverse and frontal plane, and 360 in the sagittal plane provides the
ability to simulate a wide range of gait patterns.
Some gait simulators have relatively good GRF fidelity for prosthetic
feet [4] and for cadaveric feet [1], while other systems scale the GRF
[2]–[4]. In some cases, this is a result of frail cadaveric specimens rather
then hardware limitations [4] or due to a stated goal of matching kinematics rather than kinetics [3]. Gait simulators (including the RGS) that
have performed experiments with prosthetic feet are able to prescribe
full GRFs.
The RGS’s vertical GRF fidelity is limited by our inertial cancellation method. At slow speeds, (i.e., 6.0 s) the vertical GRF fidelity
is very high (9.42 N RMS, approximately twice the noise floor). As
the simulation speeds increase our inertial estimate becomes worse resulting in larger vertical GRF RMS error. Close examination of the data
reveals that the large inertial spikes at heel strike and toe off were accurately subtracted out, but that the error in midstance was increased.
Also the inertial cancellation resulted in only a marginal reduction in
the vertical GRF error, from 39.2 N RMS to 35.0 N RMS. In summary,
an improved inertial estimation algorithm will result in improved GRF
fidelity.
The ability to perform a prosthetic gait simulation is a logical first
step towards the more pursued goal of cadaveric gait simulation. The
prosthetic gait simulations acted as a test bed to investigate the feasibility of our methodologies. Based on our simulation results, we conclude that if future cadaveric simulations are to be performed at simulation speeds faster than 1.5 s, then an improved inertial compensation algorithm is required. Another possibility would be to perform experiments at the slower speed and focus on effects that are not highly
sensitive to loading rate in the cadaveric specimens. Although many aspects of ILC are advantageous including its fast implementation, simple
stability criteria, and minimum required iterations until tracking, ILC
cannot be the final force tracking control solution for cadaveric simulations because in contrast to the prosthetic foot GRF the cadaveric
GRF cannot be prescribed by changing the ground kinematics alone
but must be accompanied by a change in the applied extrinsic muscle
tendon forces. However, our group did gain valuable experience implementing living subject data collection with embedded coordinate systems, configuring the R-2000 and prosthetic foot, and inverting the relative kinematics via a fixed tibia.
REFERENCES
[1] N. A. Sharkey and A. J. Hamel, “A dynamic cadaver model of the
stance phase of gait: Performance characteristics and kinetic validation,” Clin. Biomech., vol. 13, no. 6, pp. 420–433.
[2] C. Hurschler, J. Emmerich, and N. Wulker, “In vitro simulation of
stance phase gait, part I: Model verification,” Foot Ankle Int., vol. 24,
no. 8, pp. 614–22, 2003.
[3] C. J. Nester et al., “In vitro study of foot kinematics using a dynamic
walking cadaver model,” J. Biomech., vol. 40, no. 9, pp. 1927–1937,
2007.
[4] K. J. Kim et al., “In vitro simulation of the stance phase of gait,” J.
Musculoskel. Res., vol. 5, no. 2, pp. 113–121, 2001.
[5] Z. Bien and J. X. Xu, Eds., Iterative Learning Control: Analysis, Design, Integration and Applications. Boston, MA: Kluwer Academic,
1998, vol. 372.
[6] Y. M. Kirane, J. D. Michelson, and N. A. Sharkey, “The potential role
of flexor hallucis longus stenosis in the pathogenesis of hallux rigidus:
A dynamic cadaver model,” in Proc. 53rd Annu. Meeting Orthopaed.
Res. Soc., San Diego, CA, 2007, Poster No. 1200. On CD.