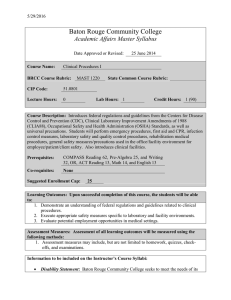
Infection Prevention & Control Training Program Islamabad Pakistan Standard And Expanded Precautions Muhammad Yaseen RN, BSN, MSc, CIC, PhD Scholar Objectives • At the end of this session attendees should be able to: 1. 2. 3. 4. Describe when to use Standard Precautions List 5 Moment for Hand Hygiene List 3 isolation categories List 2 methods of asepsis 2 DEFINITIONS Healthcare-Associated Infection Infection associated with healthcare delivery in any setting Hospital-associated or Nosocomial Infection Acquired in hospital after 48 hours of admission (not incubating nor present on admission) Community Acquired Infection Infection that is present or incubating on admission to hospital that can be traced to a community source 3 The Chain of Infection Transmission can occur when the six elements forming the Chain of Infection are present: 1. 2. 3. 4. 5. 6. An Infectious Agent Reservoir (or source) of Infectious Agent Portal of Exit Means of Transmission Portal of Entry Susceptible Host (Siegel et al. 2017) Figure M5–1 Breaking any link in the chain of infection will help prevent the spread of microorganisms (adapted from Siegel et al. 2017) The Chain of Infection • An Infectious Agent is an organism that causes disease such as bacteria, viruses, fungi, protozoa, parasites, and prions. • A Reservoir is a place where an infectious agent lives and grows (e.g., the normal flora in gastrointestinal and upper respiratory tract). There are two sources of infection: The Chain of Infection • A Portal of Exit is the way in which an infectious agent exits the source reservoir to infect a secondary source. • The Means of Transmission is how the infectious agent travels from the infected person to another person. The principle means of transmission are: contact (indirect and direct), droplet, and airborne. The means of transmission varies by type of infectious agent and some may be transmitted by more than The Chain of Infection • The Portal of Entry is any opening on the body that allows the infectious agent to enter, such as the nose, mouth, eyes, mucous membranes, a surgical or nonsurgical break in the skin, or medical devices such as urethral catheters that bypass the body’s natural defenses. • A Susceptible Host is a non-infected person who could get infected. The factors that influence who gets infected and how severe the infection is, are related to the virulence of the infectious agent and host factors such as extremes of age, underlying disease and treatment for complex diseases, immunosuppression, and recipients of organ and tissue transplants (APIC 2014; Siegel et al. 2017; GCC 2013). Modes of Transmission Mechanism for the transfer of an infectious agent from a reservoir to a susceptible host: Contact Transmission Direct and Indirect Droplet Transmission Airborne Transmission 10 Direct Contact Transmission Organisms are transferred directly from one person to another e.g. Blood borne viruses, Hep B&C and HIV transmitted under limited circumstances via percutaneous or mucous membrane exposure Herpes Simples Virus (HSV) is transmitted to patient from HCW (mouth care) 11 Indirect Contact Transmission Involves transfer of an infectious agent through a contaminated intermediate object or person Hands of HCWs most important contributors Contaminated patient surroundings Contaminated or improperly handled patient-care sterile supplies, equipment, and devices (vascular lines, gloves, catheters, bandages, etc) Inadequately reprocessed instruments (endoscopes, bronchoscopes, surgical instruments) 12 Droplet Transmission Respiratory droplets are generated by an infected person coughing, sneezing or talking. Droplets are propelled short distance Transmission occurs when droplets are deposited on conjunctivae, nasal mucosa or mouth Can also occur: During procedures (suctioning, cough induction, chest physiotherapy, etc) Microorganisms transmitted by this route are Neisseria meningitis, influenza virus 13 Airborne Transmission Airborne droplet nuclei containing very small infectious agents are generated when an infected person coughs, sneezes or talks. These tiny droplets are dispersed into the air and stay suspended in the air or move around on the air currents. Transmission is inhalation by susceptible person(s) Can also occur: During procedures such as suctioning, cough induction, extubation, or bronchoscopy Organisms transmitted by this route: Pulmonary MTB, Rubeola virus (measles), Varicella-zoster virus (chicken pox) Dangerous and exotic pathogens: SARS, Monkey pox viral hemorrhagic fever viruses 14 Standard Precautions Foundation for preventing transmission of infectious agents during healthcare woker-patients interactions Work practices required for the basic level of infection control To reduce the risk of transmission of infectious agents Apply to all body fluids, non-intact skin and mucous membranes To be used for all patient care regardless of diagnosis or presumed infectious status 15 BREAKING THE CHAIN OF INFECTION- REDUCING THE RISK OF TRANSMISSION • Standard Precautions • Hand Hygiene • PPE • Expanded Precautions • Aseptic Technique • Other recommendations 16 HAND HYGIENE • Hands can become contaminated with infectious microorganisms, which could enter the body and cause infection. • Hand hygiene is the single most effective means of preventing transmission of infectious microorganisms. 17 Indications for hand hygiene • Hand hygiene must be performed exactly where you are delivering health care to patients (at the point of care) • During health-care delivery, there are 5 moments when it is essential that you perform hand hygiene • You must perform hand hygiene using the appropriate technique and time duration 18 When to Decontaminate Hands? Sandwich Test 20 YOUR 5 MOMENTS FOR HAND HYGIENE Clean your hands immediately before an aseptic task! Clean your hands before touching a patient-when approaching him/her! To protect the patient against harmful germs, including the patient’s own, entering his/her body! To protect the patient against harmful germs carried on your hands! Clean your hands immediately after an exposure risk to body fluids (and after glove removal)! To protect yourself and the health-care environment from harmful germs! Clean your hands after touching a patient and his/her immediate surroundings, when leaving the patient’s side! To protect yourself and the health-care environment from harmful germs! Clean your hands after touching any object or furniture in the patient’s immediate surroundings, when leavingeven if the patient has not been touched! To protect yourself and the health-care environment from harmful germs! 21 Can you identify the main examples of this indication during your everyday practice of health care? Some examples may be: • shaking hands, stroking an arm • helping a patient to move around, get washed, giving a massage • taking pulse, blood pressure, chest auscultation, abdominal palpation Can you identify the main examples of this indication during your everyday practice of health care? Some examples may be: • oral/dental care, giving eye drops, secretion aspiration • skin lesion care, wound dressing, subcutaneous injection • catheter insertion, opening a vascular access system or a draining system • preparation of food, medication, dressing sets Can you identify the main examples of this indication during your everyday practice of health care? Some examples may be: • oral/dental care, giving eye drops, secretion aspiration • skin lesion care, wound dressing, subcutaneous injection • drawing and manipulating any fluid sample, opening a draining system, endotracheal tube insertion and removal • clearing up urines, faeces, vomit, handling waste (bandages, napkin, incontinence pads), cleaning of contaminated and visibly soiled material or areas (lavatories, medical instruments) Can you identify the main examples of this indication during your everyday practice of health care? Some examples may be: • shaking hands, stroking an arm • helping a patient to move around, get washed, giving a massage • taking pulse, blood pressure, chest auscultation, abdominal palpation Can you identify the main examples of this indication during your everyday practice of health care? Some examples may be: • changing bed linen • perfusion speed adjustment • monitoring alarm • holding a bed rail • clearing the bedside table Why perform hand hygiene? • To remove/reduce the number of microorganisms on the hands • To reduce the risk of transmission of infection to patients and personnel • To reduce the contamination of the environmental surfaces 27 Methods of Hand Hygiene Hand washing a process for removal of soil and transient microorganisms from the hands Using regular or antiseptic soaps Hand Antisepsis a process for removal or destruction of transient microorganisms Using antiseptic, waterless/alcohol base rub Hand scrub a process to remove or destroy transient microorganisms and reduce resident bacterial flora from the hands Using antiseptic soap/alcohol solution with extended antimicrobial effect 28 To effectively reduce the growth of germs on hands Handwashing must last 40-60 secs and should be performed by following all steps illustrated on the left 29 To be used on visibly clean hands To effectively reduce the growth of germs on hands Hand rubbing must be performed by following all steps illustrated on the left. This takes only 20-30 seconds 30 Hand Hygiene and glove use Gloves and Hand Hygiene = clean hands Gloves with no Hand Hygiene = Germ transmission 31 HAND CARE • If you have any existing skin problems or develop skin breakdown following repeated hand hygiene, you must seek medical assistance • Any concerns with latex allergy must seek medical assistance 32 Hand Lotions / Moisturisers • Prevent dehydration and damage to barrier properties of skin, skin shedding, loss of skin lipids • Use regularly if washing hands • Use individual tube or pump dispenser to prevent contamination Products used for hand Hygiene • Soap and water • Antimicrobial soaps • Alcohol hand rubs • Hand Lotions / Moisturisers Which Product When? Risk assess: What are you about to do? What have you just done? Are your hands visibly soiled? Is this a high risk procedure or a vulnerable patient? Soap and Water • Mechanical removal of soil and contaminants • Minimal microbial kill • No sustained activity • Suitable for most clinical activities • Removes 99% of transient organisms Antimicrobial Soaps • Reduce resident and transient organisms • May have sustained activity • Use only when higher level of kill required • i.e. when skin contaminated or sterile gloves to be worn • Surgical scrubbing • Kills and removes 99.9% of transient organisms Alcohol Handrubs • Very rapid kill • No residual effect • Contain emollients • Use on visibly clean hands only • Emollients residue can build up over time • Wash hands when sticky • Useful where facilities not available or time short • Kills 99.99% of transient organisms Alcohol Handrubs There are some special considerations while using Alcohol Handrubs that include: • Alcohol handrub dispensers should be away from electric sockets • The bottles should be stored in metal cupboards • The use of alcohol handrub should be discouraged while looking after patients with infections with spore forming bacteria especially Clostridium difficille related diarrhea. UK Department of Health (2005) Are Alcohol-Based Hand Rubs Really Effective? • Numerous published studies have shown that alcohol-based hand rubs remove bacteria from hands more effectively than washing hands with plain soap and water • In most studies, alcohol-based hand rubs removed bacteria from the hands to a greater degree than did washing hands with an antimicrobial soap and water • It can be used at the point of care Boyce JM, Pittet D et al. MMWR 2002;51 (RR-16):1-45 Definition of Point of Care Point of care - refers to the place where three elements occur together: the patient, the health-care worker, and care or treatment involving patient contact. Application time of hand hygiene (handwashing and handrubbing) and reduction of bacterial contamination Hand hygiene with: Handwashing Handrubbing Pittet and Boyce, Lancet Infectious Diseases 2001 More Tips on How to Use an AlcoholBased Hand Rub • If you feel a “build-up” of emollients on your hands after cleaning your hands 5 to 10 times with an alcohol-based hand rub, wash your hands with soap and water • If you clean your hands with an alcohol-based hand rub before putting on gloves, make sure the alcohol has dried completely before putting on gloves Won’t Frequent Use of Alcohol Dry Out My Skin? • Several studies have proven that nurses who routinely cleaned their hands between patients by using an alcohol-based hand rub had less skin irritation and dryness than nurses who washed their hands with soap and water • Alcohol-based hand rubs contain skin conditioners (emollients) that help prevent the drying effects of alcohol Boyce JM et al. Infect Control Hosp Epidemiol 2000;21:442 Winnefeld M et al. Br J Dermatol 2000;143:546 BREAKING THE CHAIN OF INFECTION REDUCING THE RISK OF TRANSMISSION • Standard Precautions • Hand Hygiene • PPE • Expanded Precautions • Aseptic Technique • Other recommendations 47 PRESONAL PROTECTIVE EQUIPMENT • PPEs should be worn when exposure to body fluids is likely. • PPE is used to create a barrier between HCW and patient, substance, or surface. • The use of one or more of these is based on the degree and risk of exposure anticipated. • These include the use of gloves, gowns, plastic aprons, eye protection and resuscitation devices. 48 GLOVES • Gloves are used as a barrier • Gloves are for single patient use only • Perform hand hygiene before wearing gloves • Wear gloves when handling: • Blood and other body fluids • Mucous membranes • Non-intact skin • Contaminated surfaces and items • Select gloves for the particular task to be undertaken, i.e. sterile/unsterile procedures 49 GLOVES • Change gloves when they become contaminated: • Between patients • Between procedures • Between different procedures on the same patient • Gloves are to be worn at the bedside • Do not leave patient room with gloves on • Remove and discard gloves promptly: • After use before leaving the area of activity • Before touching environmental surfaces • Wash hands immediately 50 GOWN/PLASTIC APRON • Gown/plastic apron (clean/non-sterile) • Wear during procedures and patient-care activities that are likely to generate splashes or sprays of body fluids • Worn to protect bare skin • To prevent soiling of clothing 51 GOWN/PLASTIC APRON • Select a gown/plastic apron that is appropriate for the activity and the amount of fluid likely to be encountered. • Secure the strings to keep the gown or apron in place • Remove soiled gown/plastic apron promptly and wash hands to prevent transfer of microorganisms to other patients and environmental surfaces. • Untie strings and fold away from you in an inside out manner to prevent transfer of microorganisms to yourself 52 MASKS • Wear a surgical mask to prevent exposure of the mucous membranes of your mouth and nose during procedures that are likely to generate aerosol droplets or splashes of blood or other body fluids. • Wear an N95 Respirator mask to enter the room of any patient room in Airborne Isolation (unless it is known that you have immunity to that disease, e.g. Chickenpox). 53 MASKS • Wear the mask to fully cover the nose and mouth so that you are breathing through it. • Discard surgical mask before leaving the area of activity. • N95 respirator mask must be removed outside of the patients’ room. 54 PROTECTIVE EYEWEAR • Wear protective eyewear such as glasses, goggles or shields to protect your eyes, and in conjunction with a mask to protect your face, during procedures where splashes of blood or body fluid are likely to occur. • Ensure that protective eyewear is readily available anywhere there is a risk of splashes of body fluid e.g. ER, Endoscopy, O.R, ICU, L&D, cardiac arrest carts. 55 PPE use in non-patient care areas • The concepts of who, when, and how to wear PPEs are the same in non-patient care areas • Applies to areas where patients receive diagnostic testing and specimen are processed • Medical imaging • Laboratory • Physiotherapy, etc 56 Putting PPEs on safely Put on in this order: 1. Hand hygiene 2. Mask, goggles or face shield 3. Gown 4. Gloves 57 Removing PPEs safely Remove in this order: 1. Gloves 2. Wash or cleanse hands 3. Mask, face shield or goggles (not N95 respirator) 4. Gown 5. Cleanse hands N95 respirator is remove when outside of the Airborne Isolation room 58 BREAKING THE CHAIN OF INFECTION REDUCING THE RISK OF TRANSMISSION • Standard Precautions • Hand Hygiene • PPE • Expanded Precautions • Aseptic Technique • Other recommendations 59 EXPANDED PRECAUTIONS Transmission Based Precautions Isolation Precautions EXPANDED PRECAUTIONS • Used when infectious status of patient is known or suspected with epidemiologically significant organism (e.g. highly transmissible, difficult to treat) • Determined by the modes of transmission of the infecting agent • 3 Categories of precautions (Isolation) 1.Contact 2.Airborne 3.Droplet 61 Contact Isolation • Contact isolation is designed to interrupt transmission of infection transmitted by contact route. • Must be used in conjunction with Standard Precautions. • Requires a single room • Used for patients known or suspected to be infected or colonized with resistant, epidemiologically important or highly transmissible pathogens (MRSA, VRE, RSV, etc.) 62 Droplet Isolation • To prevent transmission of infectious agents, spread by droplet contact route to mucous membranes, conjunctiva, nose and mouth • Must be used in conjunction with Standard Precautions • Droplets generated by coughing, sneezing and suctioning • Requires close contact (patient surroundings) for transmission Pertussis Mumps Influenza Rubella Invasive Neisseria meningitidis 63 Airborne Isolation • To prevent transmission of organisms spread by airborne route that remain suspended in the air • Must be used in conjunction with Standard Precautions • Requires a single room with negative pressure ventilation • Used for patients known or suspected to be infected with Measles Varicella Pulmonary Tuberculosis 64 When to isolate? • Type and duration of precautions (Contact, droplet, or airborne isolation) needed for selected microorganisms and diseases 1. For the duration of hospital stay 2. For the duration of illness 3. For time specified in hours or days of antimicrobial therapy 4. Until lesions are crusted 5. Until there are negative culture or cultures 1. 2. Guidelines from Association for Professionals in Infection Control and Epidemiology 2009 (APIC) 3 rd Edition (HICPAC 2007) 65 When to isolate and how long? • Patients that are: A. RSV (+)? B. Chickenpox? C. Query Neisseria meningitis? D. Query or rule out pulmonary tuberculosis? 66 When to discontinue isolation? A. Isolate patient for duration of illness: 1. RSV: Contact Isolation and Standard Precautions • For the duration of illness (2-5days) 2. Chickenpox: Airborne and Contact Isolation and Standard Precautions • Until lesions are crusted/dried (usually 5 days) • Infection Control Practitioner should review patient status before removing patient from isolation. • Signs and symptoms (subsided respiratory illness or no new lesion eruption) • In these cases (re)screening is not necessary 67 B. Isolate patient for time specified in hours or days of antimicrobial therapy 1. Neisseria meningitidis: Droplet Isolation and SP • Only discontinue droplet isolation after completion of 24 hours of effective antibacterial therapy • Infection Control Practitioner should review patient status before removing patient from isolation. 68 When to discontinue isolation? C. Isolate patient until there are negative culture(s) 1. Query (R/O) pulmonary Tuberculosis: Airborne Isolation and SP • Discontinue isolation: If another diagnosis is made that explains the clinical syndrome or review of patient shows TB infection is negligible OR 3 negative AFB stain are required • obtained on 8-24 hours • one must be morning specimen 69 2. Patient in Airborne Isolation for (+)AFB sputum smear (pulmonary Tuberculosis) • Discontinue isolation: • After patient receive ≥14 days of effective anti-TB therapy • AND 3 negative AFB stain • obtained on 8-24 hours • one must be morning specimen • Infection Control Practitioner should review patient status/results before removing patient from isolation. OTHER RECOMMENDATIONS OTHER RECOMMENDED PRACTICES TO FURTHER REDUCE THE RISK OF TRANSMISSION OF INFECTION IN HEALTHCARE SETTING New Standard Precautions • Respiratory Hygiene/Cough Etiquette was added in 2004 for the purpose of source containment of respiratory tract pathogens (e.g., severe acute respiratory syndrome (SARS) variant Co-V, avian influenza H5N1, human influenza. • Procedure: • Use tissues cover the nose and mouth when coughing or sneezing to contain respiratory secretions • Dispose them in the nearest waste disposal then perform hand hygiene. 72 RESUSCITATION DEVICES • Avoid the need for emergency mouth-to-mouth resuscitation by using mouthpieces, resuscitation bags or other ventilation devices. • Ensure that this is available in your work area and any area where the need for resuscitation is predictable. • Know where and how to use the equipment. 73 HANDLING CONTAMINATED ITEMS • Proper and safe handling of the following items in the patient care areas is crucial to reduce the risk of exposure to and transmission of infectious microorganisms • Needles and Sharps • Linen • Medical waste • Patient care equipment • Laboratory specimen 74 AVOIDING INJURIES • • • • YOU USE IT YOU DISPOSE OF IT DO NOT discard needles/sharps in the garbage or linen bag DO NOT leave used needles/sharps unattended on open surfaces DO NOT overfill sharps containers • Containers must be replaces when it is at the full-line • DO NOT recap used needle 75 LINEN • Handle soiled linen in a manner that prevents skin and mucous membrane exposures, contamination of clothing, and transfer of microorganisms to other patients and the environment. • Wrap soaked linen so that the heavily soiled area is in the middle and immediately after removing from the patient’s bed. 76 CONT’D • Do not overfill laundry bags - remove from the laundry hamper when bag 2/3 full and securely tie the mouth. • Do not put soiled linen on the floor. Avoid repeated handling, to minimize agitation that will cause contamination of the air. • Wash hand after handling soiled linen. 77 WASTE MANAGEMENT Medical waste is those items soaked with blood stained fluid, which are judged to have a relative risk of disease transmission and therefore special handling is indicated for their disposal. 78 Medical waste include • Sharps/Needles and syringes • Fluid filled disposable suction devices/canisters that cannot be emptied • Blood soaked items from any area • Dialyzersdialysis bags and lines • Large volume urine/stool collections • Laboratory specimens and their disposable containers • Body part (human and animals) • Disposable patient care items (heavily soiled with blood) 79 Cont’d • Dispose of infectious waste in the appropriate containers. • Ensure that garbage containers are lined with color-coded bags to effect proper disposal. • Wear the appropriate protective apparel when handling medical waste. • Wash hands after handling medical waste and containers. 80 SUMMARY • Standard Precautions must be used for all patient care regardless of their known or suspected infectious status. • Standard Precautions is designed to reduce the risk of exposure to potentially infectious microorganisms in body fluids. • Applied universally, it will improve the standard of care for all patients rather than focusing special attention on the few patients with identified infections/infectious diseases. 81 THANK YOU