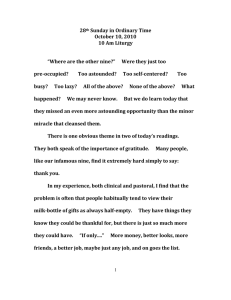
7KH/HSURV\$V\OXPLQ,QGLD૱ Jo Robertson Journal of the History of Medicine and Allied Sciences, Volume 64, Number 4, October 2009, pp. 474-517 (Article) Published by Oxford University Press For additional information about this article http://muse.jhu.edu/journals/jhm/summary/v064/64.4.robertson.html Access provided by University of California @ Berkeley (10 Oct 2014 15:37 GMT) The Leprosy Asylum in India: 1886 – 1947 JO ROBERTSON* ABSTRACT. Writing against a historical practice that situates the leprosy asylum exclusively within prison-like institutions, this article seeks to show the variation in leprosy asylums, the contingencies of their evolution, and the complexity of their designs, by devoting attention to the characteristics of the leprosy asylum in India from 1886 to 1947, in particular to the model agricultural colony. Drawing upon the travel narratives of Wellesley Bailey, the founder of the Mission to Lepers in India, for three separate periods in 1886, 1890 –91, and 1895 –96, it argues that leprosy asylums were formed in response to a complex conjunction of impulses: missionary, medical, and political. At the center of these endeavors was the provision of shelter for persons with leprosy that accorded with principles of good stewardship and took the form of judicious use of donations provided by benefactors. As the Mission to Lepers began to bring about improvements and restructuring to asylums, pleasant surroundings, shady trees, sound accommodation, and good ventilation became desirable conditions that would confer physical and psychological benefits on those living there. At the same time, the architecture of the asylum responded to economic imperatives, in addition to religious and medical aspirations, and asylums moved towards the regeneration of a labor force. Leprosy-affected people were increasingly employed in occupations that contributed to their sustenance and self-sufficiency, symbolically reincorporating the body damaged by leprosy into the economic world of productive relations. KEYWORDS: leprosy asylum, India, agricultural colony, built environment, Mission to Lepers, economy, labor. * Institut d’Histoire de la Médecine et de la Santé, Centre Médicale Universitaire (CMU), Case postale, CH – 1211 Genève 4, Switzerland and 3 Ovendean St., Yeronga, Brisbane, Queensland, Australia 4104. Email: jo.robertson@wuhmo.ox.ac.uk. This research was conducted using funding from both the Nippon Foundation and the Sasakawa Memorial Health Foundation, through WHO and the International Leprosy Association, while I was based at the Wellcome Unit for the History of Medicine at Oxford from 2001 to 2007. JOURNAL OF THE HISTORY OF MEDICINE AND ALLIED SCIENCES, Volume 64, Number 4 # The Author 2009. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oxfordjournals.org Advance Access publication on June 16, 2009 doi:10.1093/jhmas/jrp014 [ 474 ] Robertson : The Leprosy Asylum in India 475 Before us is a wide stretch of tall green trees with little buildings, red and buff and white, peeping through, and the little steeple of a church rising above all. This is the first glimpse of the asylum, splendidly situated, with open, wind-swept country all around. There are no walls to give it an air of confinement, and if one had no knowledge of the nature of the place and of the suffering that is so patiently endured within its boundaries, one might exclaim: “What a fortunate little community!”1 n contrast to this 1922 description of the leprosy asylum at Purulia, in Western Bengal, leprosy asylums in other places have garnered an impressive reputation as sites of isolation and suffering. As part of his study of insanity in the Age of Reason, Michel Foucault famously described these places of seclusion in Europe: “In the margins of the community, at the gates of cities, there stretched wastelands which sickness had ceased to haunt but had left sterile and long uninhabitable. For centuries, these reaches would belong to the non-human. . . . Leprosy withdrew, leaving derelict these low places.”2 These two descriptions, the one, reminiscent of an English village, the other, conjuring the echoing spaces of a gothic wilderness, use the economics of “space” in order to describe the places where people with leprosy lived. The Indian one presents a panorama that balances the built environment with “open, windswept country” so as to demonstrate the success of the work done by the Mission to Lepers in India; Foucault evokes the emptiness of uninhabitable wastelands in order to describe the space vacated by leprosy in the medieval period. More recently, in his analysis of institutions of “enclosure” in colonial and imperial settings, Rod Edmond has described the leprosy asylum as a “brutally literal form” of detention established I 1. Mission to Lepers, The Forty-Eighth Annual Report of the Mission to Lepers. “A Fruitful Field” (London: Botolph Printing, 1922), 12. The term “leper” carries demeaning and dehumanizing connotations that have a devastating impact on people affected by leprosy. I have attempted to avoid the use of this word in all instances except when directly quoting an historical document, the title of an organization, or the name of an asylum. 2. Michel Foucault, Madness and Civilization: A History of Insanity in the Age of Reason (New York: Random House, 1988), 3–6. Arguing metaphorically as well as literally, Foucault suggests that once the medieval lazaretto was vacated by leprosy, the space was given over to “unreason.” In spite of this argument, the disease persisted in pockets, in Europe, over the next three hundred years. Carole Rawcliffe successfully contests the historical accuracy and persistence of the nineteenth-century orthodoxies of the disappearance of medieval leprosy. At that time it was argued that the disappearance of the disease came about as a result of segregation. See Rawcliffe, Leprosy in Medieval England (London: Boydell and Brewer, 2006). 476 Journal of the History of Medicine : Vol. 64, October 2009 in an attempt to protect the metropolis and the colonizer “from the world they were colonizing.”3 As places of detention, he believes, leprosy asylums were subsequently adapted and applied to the colonized and then, in turn, to members of the imperial population.4 Edmond bases his analysis on Molokai, in Hawaii (established in 1866), Robben Island (1846), South Africa, and the islands of detention in Australia (1889, 1891, 1907) and New Zealand (1903).5 In assessing Edmond’s claim, it is important to realize that the sites on which his case is based were representative of the earliest phase of the establishment of many hundreds of leprosy asylums throughout the world. The asylums he refers to are, in fact, at one end of a historical continuum stretching into the mid-twentieth century.6 In addition, leprosy asylums that were established in any one decade, such as those built after the first international leprosy conference in Berlin in 1897, or even those after the first international leprosy congress in Cairo in 1938, were not uniform in style and character. As the Leprosy Commission of the League of Nations concluded, after an extensive world-wide survey in 1931, asylums reflected the character of the society and culture in which they were established.7 The leprosy asylum in the nineteenth and the twentieth centuries needs to be differentiated as a site, both historically and geographically. The variation in asylums, the contingencies of their evolution, 3. Rod Edmond, Leprosy and Empire: Medical and Cultural History (New York: Cambridge University Press, 2006), 20–21. 4. Ibid., 20 –22. 5. In Hawaii, legislation was introduced on 3 January 1865 to prevent the spread of the disease. Land on the island of Molokai was purchased for the first contingent of leprosy-affected people, who were shipped there on 6 January 1866. Legislation for the compulsory institutionalization of all people with leprosy was introduced into the Cape Colony in 1891. For a discussion of this see Harriet Deacon, “Racial Segregation and Medical Discourse in Nineteenth-Century Cape Town,” J. Southern Afr. Stud., 1996, 22, 287– 308. There were also sites of detention at Little Bay in Sydney, New South Wales, and Derby in Western Australia. Edmond, Leprosy and Empire, 143 –77. 6. See database search for “Leprosarium” at http://www.leprosyhistory.org. Without question, there were hellholes. For example, the Chinese who were, without benefit of the law, exiled to Dayman Island, in the Torres Straits, in 1889, almost certainly died of exposure or starvation. 7. League of Nations: Health Organization, The Principles of the Prophylaxis of Leprosy: First General Report of the Leprosy Commission (Geneva: Publications Department of the League of Nations, 1931). “The isolation of lepers should be carried out in accordance with the circumstances prevailing in the countries involved,” 6. As a result, leprosy asylums now provide eloquent indices of the specific socio-economic and cultural circumstances in which they were built. Robertson : The Leprosy Asylum in India 477 and the complexity of their designs remain to be explored. Between 1856, when the hospital asylums of Norway were established, and the first decade of the twentieth century, when the model leprosy colony of Culion, in the Philippines, was built, important changes took place in the idea of what a leprosy asylum should be. By the time of the Cairo Congress in 1938, it was clear that the focus of expertise had shifted from the imperial centers to the colonies. While this article emphasizes the geographical specificity of leprosy asylums, it will do so within an understanding of the international circulation of information about leprosy control and asylum creation. Medical and governmental authorities who were interested in leprosy shared information so that connections were made across national borders and colonial empires. For example, questionnaires on leprosy were sent to the colonies by the Royal College of Physicians of London in order to gauge the character and progress of the disease following on a request in 1862 by the Governor-in-Chief of the Windward Isles, James Walker.8 Responses were gathered from the West Indies, China, Japan, India, Africa, the Middle East, and European and Mediterranean countries and these were published in its 1867 Report on Leprosy by the Royal College of Physicians.9 This publication was then circulated throughout the British colonies. The first international leprosy conference in Berlin in 1897 drew 150 attendees, with 44 delegates representing 22 governments; the second conference in Bergen, Norway, in 1909 attracted 168 attendees from 27 countries.10 8. Correspondence of James Walker to the Duke of Newcastle, 19 February 1862, in the Report on Leprosy by the Royal College of Physicians, Prepared for, and Published by Her Majesty’s Secretary of State for the Colonies with an Appendix (London: Eyre and Spottiswood, 1867), 2. 9. The Report on Leprosy by the Royal College of Physicians contained forty responses from the following: New Brunswick, Bermuda, Bahamas, Jamaica, Tortola, St. Kitts, Nevis, Montserrat, Antigua, Dominica, St. Lucia, St. Vincent, Barbados, Grenada, Tobago, Trinidad, British Guiana, Cape of Good Hope, Sierra Leone, Tangiers (Tunis, Tripoli, Bengazi, Cairo), Jerusalem (Caiffa), Beyrout (Cyprus), Damascus, Aleppo, Rhodes, Smyrna (Scio, Mytellene, Samos), Crete, Ionian Islands (Corfu), Salonica, Monastir (Bosnia Serai, Bucharest, Varna), Dardanelles (Brussa, Samsoun), Constantinople, Tarbreez, Japan, China (Hong Kong, Canton, Shanghai, New Chwang, Kin-Kiang, Kana Gawa, Formosa) Australia (Victoria, New South Wales), Mauritius, Ceylon, Madras Presidency, Bombay Presidency, Bengal Presidency. 10. This period, between the 1867 Report on Leprosy by the Royal College of Physicians and the Berlin Conference, was a time of intense debate about the danger that leprosy represented to the metropolitan centers of Britain and Europe. 478 Journal of the History of Medicine : Vol. 64, October 2009 The main journal in the field, Lepra Bibliotheca Internationalis, an initiative of the Berlin conference, which was published up until the beginning of World War I, demonstrates an even wider circulation of information.11 Although the editorial committee was predominantly European, it also included Americans and committee members based in Jamaica and Havana. In addition, contributions came from more exotic locales such as Cambodia, Anglo-Egyptian Sudan, Arabia, South Africa, the Marquesas, Hawaii, the Dutch Antilles, British Guiana, Madagascar, Laos, New Zealand, Réunion, the Loyalty Islands, Guadeloupe, Indochina, Algeria, the highlands of West Central Africa, and British India. The journal carried reports of leprosy asylums and of differing legislation concerning people with leprosy in various countries, as well as articles of scientific and medical interest. At the time of the 1897 Berlin and also the 1909 Bergen leprosy conferences, when European medical influences were strongest, the asylums and medical practices that were considered most worthy of emulation were Norwegian, but American measures against leprosy also increasingly commanded attention.12 In Hawaii, the leprosy settlement of Kalaupapa, on the island of Molokai, admitted 5,800 people with leprosy between 1866 and 1905, with the year 1888 marking the peak in numbers of people segregated there. By 1906, the Americans had established the very modern leprosy colony of Culion in the Philippines, which had patients’ dormitories and quarters for 400 employees. This colony resembled a small township with streets and alleys, a theater, a town hall, a school, a piped water supply and reservoirs, a sewer line, docks, warehouses, dining 11. The journal was published in London, Leipzig, and Paris (and later New York). 12. Leprosy control in Norway, where the disease was endemic, focused on a system of medical registration, legislation, hospitalization, and research. Surveys were conducted in 1836, 1845, and 1852, and a medical superintendent for leprosy, Ove Guldberg Høegh (1814 –1863), was appointed to be responsible for a national leprosy register, established in 1856. St. Jørgen’s Hospital, three additional hospitals, and a research hospital were dedicated to leprosy. Knowledge of the disease of leprosy entered a new era through the work of Daniel Cornelius Danielssen (1815 –1894), Carl Wilhelm Boëck (1808 – 1875), and Gerhard Henrik Armauer Hansen (1841 –1912). Although nineteenth century debates about leprosy argued that the disease had disappeared from Europe because of segregation and isolation practices in the Middle Ages, views about the actual presence of the disease in Europe right up until the 1950s need to be revised. Carole Rawcliffe has begun this task. See Rawcliffe, Leprosy in Medieval England (Suffolk, UK and New York: Boydell Press, 2006). Robertson : The Leprosy Asylum in India 479 halls, a post office, a store, and a garbage disposal plant, a church, public bath-latrines and a cemetery.13 The transition from the Norwegian model of the 1850s to the American model that began in 1906 is paralleled by international exchanges of expertise that were grounded in local experience, as can be seen from papers presented at the international conferences. I have chosen India as the focus of my study because this is where in the nineteenth century the earliest extensive program of construction of asylums took place, and while there were never enough asylums in India to care for all those affected by leprosy, there were more asylums there than in any other country. From the 1870s onwards, the leprosy asylum in India incrementally changed, so that by the 1940s, it could be described as existing in three distinct forms: the well organized sanatorium for active and infective cases, with proper staff, buildings, and equipment; the asylum for crippled, deformed, and disabled cases; and the agricultural colony in which patients could maintain themselves.14 This study will focus on the emergence of the last of these forms and the rationale that sustained it. Both Sanjiv Kakar and Jane Buckingham have independently provided studies of the leprosy asylum in India. Kakar argues that in the light of medical uncertainties about transmission and causation of the disease, asylums were shaped by religious and medical intentions.15 Buckingham, as part of a larger study of leprosy in colonial 13. Secretary of the Interior, Dean C. Worcester, member of the American Cabinet in the civilian government of the American occupied Philippines, cited in Cristina Verzola Rodriguez, ed. Culion Island: A Leper Colony’s 100-Year Journey toward Healing (Philippines: Culion Foundation, Inc. and Fundacion A Nuestros Enfermos Servimos Viendo A Dios, 2003), 60. For critical articles on Culion, see Warwick Anderson, “Leprosy and Citizenship,” Positions: East Asia Cultures Critique, 1998, 6, 707 – 30; and Jo Robertson, “Culion, the ‘Island of the Living Dead’: Or Another Look at Leprosy and Citizenship,” in Politics of Prevention, Health Propaganda, and the Organisation of Hospitals, 1800 –2000, ed. Astri Andresen, Kari Tove Elvakken, and Tore Gronlie (Bergen: Rokkansenteret, 2005). 14. Government of India, Committee Appointed by the Central Advisory Board of Health (1941), Report on Leprosy and Its Control in India (New Delhi: Government of India Press, 1942), 28. 15. Sanjiv Kakar, “Medical Developments and Patient Unrest in the Leprosy Asylum, 1860 to 1940,” Soc. Sci., 1996, 24, 62–80; and Kakar, “Leprosy in British India, 1860 – 1940: Colonial Politics and Missionary Medicine,” Med. Hist., 1996, 40, 215 –30. Kakar examines “various forms of protest adopted by patients within asylums” and identifies flashpoints between patients and asylum authorities around issues of religious teaching, medical treatment, and sexual segregation. He argues that medical advances in the 1920s and 1930s provided a platform for greater militancy on the part of the leprosy affected for the improvement of asylum conditions. See Kakar, “Medical Developments,” 73. 480 Journal of the History of Medicine : Vol. 64, October 2009 south India in the period before missionary anti-leprosy activity, describes the emergence, function, and design of the leprosy hospital in Madras.16 Neither of these authors devotes an extended analysis to the regimes of value, especially the economic ones, out of which Indian asylums emerged and for which the allocation of space and the construction of the built environment were an index. In order to reconstruct a sense of the material and physical space of the leprosy asylum in India as it changed from being a refuge and a haven for the few, this article will describe how the missionary organization dedicated to supporting leprosy work in India, the Mission to Lepers, invested the unrelenting stream of donations that it received from British and Indian benefactors into land and the built environment. It will describe the extent, location, and structures of leprosy asylums in India that preceded many of the activities of the Mission, and then it will delineate the process of acquisition, improvement, and renovation that took place under the Mission. At the same time, the article will explain the rationales that governed the acquisition of new asylums and lay bare an archaeology of the spaces that governed life in these places describing the buildings, the walls, courtyards, and separations within the compounds. It thereby aims to describe the gradual processes of change out of which emerged a new form of asylum: the agricultural colony, typified by Purulia in Western Bengal. This article will do this by using the descriptions of leprosy asylums furnished in reports by Wellesley Bailey, the founder of the Mission to Lepers, on his travels on behalf of the Mission over three separate periods in 1886, 1890 –91, and 1895 –96.17 It will draw on the Mission to Lepers’ reports that were produced after meetings of leprosy asylum superintendents in Wardha in 1902, Purulia in 1908, Chandkhuri in 1911, and Calcutta in 1920.18 It will also draw upon 16. Jane Buckingham, Leprosy in Colonial South India: Medicine and Confinement (Basingstoke: Palgrave, 2002), 45 –51. 17. Wellesley Bailey, A Glimpse at the Indian Mission-Field and Leper Asylums in 1886–87 (London: John F. Shaw, 1887); The Lepers of Our Indian Empire: A Visit to Them in 1890–91 (London: John F. Shaw, 1891); A Visit to Leper Asylums in India and Burma, 1895–96 (Edinburgh: Darien Press, 1896). 18. Anon., Report of the Conference of Superintendents of Leper Asylums: The Central Provinces and the Bombay Presidency, Wardha, CP, February 1902 (Bombay: Bombay Guardian Mission Press, 1902); Anon., Report of a Conference of Leper Asylum Superintendents Held at Purulia, Bengal, from 18th to 21st February 1908 (Edinburgh: Darien Press, Bristo [sic] Place, 1908); Anon., Report of a Local Conference of Superintendents of Leper Asylums, Held at Robertson : The Leprosy Asylum in India 481 the unpublished Minutes of the Mission to Lepers and the Indian Auxiliary of the Mission to Lepers, as well as photographs, plans, and official government reports. W E L L E S L E Y B A I L E Y, I N D I A , A N D T H E M I S S I O N TO L E P E R S Wellesley Bailey, the founding father of the Mission to Lepers, was an Irishman, who after attempting to make his fortune in Australia and New Zealand, set out to India where his brother was in the Indian police force. Bailey joined the American Presbyterian Mission at Ambala, in the Punjab, and it was there that he first became aware of people with leprosy. Bailey was filled with horror, fascination, pity, and an immediate sense of purpose: “If ever there was a Christ-like work,” this was it.19 On his return to Dublin in 1874, Charlotte Pim, a friend of his wife, Alice Grahame, heard his story and began to organize small meetings in her drawing room in Dublin in order to tell others of “the terrible condition of India’s lepers, physically, mentally, spiritually, and of what we were trying to do, for just a few of them, at Ambala, in the Punjab.”20 Against all expectations, the small group found that many people were responsive to their appeal for help. They had tapped into an incremental but consistent source of funding that still supports what is today known as the Leprosy Mission International. Charlotte Pim had hoped to raise about £30 a year, but by the end of the second year, had succeeded in raising £809.21 As can be seen from the Minutes of the Meetings, the group took a keen responsibility in accounting for these donations. They apportioned small amounts of money to Protestant missionary organizations in India assisting leprosy-affected people. In turn these organizations would account for their expenditure. Every gift of money was meticulously tracked Chandkuri, Central Provinces, November 29th and 30th, 1911 (Chandkuri: W. H. P. Anderson for the Mission to Lepers, 1911); Mission to Lepers, Report of a Conference of Leper Asylum Superintendents and Others on the Leper Problem in India, Held in the Town Hall, Calcutta, from 3rd to 6th Feb 1920 (Cuttack: Orissa Mission Press, 1920). 19. Cited by John Jackson, Lepers, Thirty-Six Years Work Among Them: Being the History of the Mission to Lepers in India and the East 1874 –1910 (London: The Mission to Lepers, 1910), 12. 20. Wellesley C. Bailey, Fifty Years Work for Lepers, 1874–1924 (London: Mission to Lepers, 1924), 10. 21. A. Donald Miller, An Inn Called Welcome: The Story of the Mission to Lepers, 1874– 1917 (London: Mission to Lepers, 1965), 13. 482 Journal of the History of Medicine : Vol. 64, October 2009 and in the early years much of it went into purchasing lands and constructing and maintaining leprosy asylums in India.22 While Bailey’s awakening to the needs of the leprosy affected was expressed as concern for their spiritual well being, the work of the Mission also took material form through judicious financial investment in land and buildings. Ordinary people in Britain enthusiastically supported the work of the Mission to Lepers. Donations were given in the tradition of subscriptions for infirmaries and dispensaries that was usual in Britain in the nineteenth century.23 At public meetings held in the United Kingdom, donations of £250, £100, £50, and £30 were made towards the asylums.24 Demonstrating a keen interest and a close sense of connection with the work taking place in India, donors would sometimes specify where and on what the money was to be spent. For example, a legacy was received for the exclusive use of the Raniganj Asylum, in Bengal, “to be spent on its improvement, over and above our ordinary expenditure on that asylum.”25 In addition to British support, there was also strong Indian financial support, both from the British in India and from the Indian elite. In 1920, at the conference of leprosy asylum superintendents in Calcutta, the Reverend Frank Oldrieve announced that he had received 186,000 rupees in donations, mostly from Indians.26 Sometimes the support of inmates would be shared between the Mission to Lepers and the relevant municipality.27 When this donated money was allocated to various asylums, the Minutes of the Mission to Lepers’ meetings reveal how these small amounts of 22. Gussow, Leprosy, 206. Gussow argues that missionaries restigmatized leprosy at the end of the nineteenth century, and he refers specifically to the Mission to Lepers. A debate about stigmatization is for another article, except to note that stigmatization is always a by-product of a loss of economic status. 23. Keir Waddington, Charity and the London Hospitals, 1850 –1898 (Suffolk, UK and Rochester, NY: Royal Historical Society, Boydell Press, 2000). 24. Minutes of the Mission to Lepers, June 1890, Minute Book, 139 –140, 308, Leprosy Mission International Archives, Brentford, London. 25. Ibid. 26. Frank Oldrieve, “Survey of Present Work among Lepers in India,” Report of a Conference of Leper Asylum Superintendents, 80 –88. Buckingham has already drawn attention to the role of the Indian elite in supporting the legislation that would detain leprosy-affected paupers. 27. Minutes of the Mission to Lepers, 10 June 1890, 115, Leprosy Mission International Archives, Brentford, London. Robertson : The Leprosy Asylum in India 483 money were used judiciously, making it possible for the Mission to embark on a building program that would bring about progressive changes to the leprosy asylum in India.28 Wellesley Bailey went to India on three occasions between 1886 and 1896 in order to ascertain the needs of those affected with leprosy and of those of the Christian missions that were either already assisting leprosy-affected people or desired to do so.29 On completion of each of these tours, Bailey reported back to a committee set up by the Mission to Lepers. At the same time, his reports were published as three books that would have found readers among benefactors and those interested in joining that growing group.30 Bailey’s descriptions were filtered through his agenda, which sought to demonstrate to an audience of actual and potential benefactors the difference that the Mission to Lepers could make and was, in his view, in the process of making in the lives and to the souls of those affected with leprosy in India, in order to generate further funding. But the detailed descriptions of the leprosy asylums that he discovered in his travels and the changes that he envisaged also reveal what asylums were like between 1886 and 1896, as well as how the Mission to Lepers changed the leprosy asylum in India, by incrementally altering its built environment, at the turn of the nineteenth century. Carolyn Strange and Alison Bashford argue that places of isolation in the nineteenth century were legitimated by discourses of liberty and modernity so that their architecture reflects a paradoxical need to demonstrate humane values, while depriving individuals of their rights, in the name of public health.31 I will argue for the more determining role played by contingency in the shaping of leprosy asylums in India, one element of which was the pressing demand from those who wished to gain admittance. 28. This is evident from the painstaking details taken to account for and record expenditures. See Minutes of the Mission to Lepers, Leprosy Mission International Archives, Brentford, London. 29. For a discussion of Bailey’s using the travel literature genre to raise funds, see D. George Joseph, “‘Essentially Christian, Eminently Philanthropic’: The Mission to Lepers in British India,” História, Ciências, Saúde-Manguinhos, 2003, 10, Suppl. 1, 263 –66. 30. Bailey, A Glimpse at the Indian Mission-Field; The Lepers of Our Indian Empire; A Visit to Leper Asylums in India and Burma. 31. Carolyn Strange and Alison Bashford, eds., Isolation: Places and Practices of Exclusion (London: Routledge, 2003). 484 Journal of the History of Medicine : Vol. 64, October 2009 Leprosy reduced its victims to pauper status, irrespective of their pre-leprosy lives. In addition to leprosy altering the physical body, especially the face and hands, thereby compromising individuality, a diagnosis of the disease brought about a traumatic alteration in a person’s social status and social identity. A. T. W. Simeons’s novel, The Mask of a Lion, vividly describes these changes, both physical and social, in the life of a village tailor, Govind, who is forced by leprosy to give up his livelihood and take to the roads with a band of fellow beggars.32 Therefore a distinction must be made between those who voluntarily sought entrance to Indian leprosy asylums and those who were placed in asylums under the Lepers Act of 1898.33 Voluntary admissions were in the majority as is demonstrated in the case of the Purulia Asylum, Bengal, which in the twenty years from its inception in 1884 admitted 2,358 leprosy sufferers. Very few of these were placed in the asylum by order of the law. Although Purulia was placed under the Act in 1902, by 1908 it had only received seven people with leprosy who had been sent there under compulsion.34 Of these, one had escaped, four had died, and two were still at Purulia.35 The leprosy-affected people in institutions in India therefore were mostly voluntary admissions and as such were separately housed from those few who had been detained under the law. In addition, there were always more people in need of asylum than there was accommodation available. In Bengal, e.g., there were two leprosy mission asylums at Raniganj and Bankura, and there was one institution in Calcutta that was associated with the Mission to Lepers. By 1921, in a population of 47 million in Bengal, there were 15,550 people affected with leprosy and only 440 of these were in 32. A. T. W. Simeons, The Mask of a Lion (New York: Alfred A. Knopf, 1952). 33. The Lepers Act of 1898 (Act no. III of 1898) was passed by the Governor-General of India in Council. It was described as “An Act to provide for the segregation and medical treatment of pauper lepers and the control of lepers following certain callings.” In it a “leper” was “any person suffering from any variety of leprosy in whom the process of ulceration has commenced.” The Act is published in an Appendix in Conference Purulia, 79–87. For a discussion of the Act, its implementation, and its weakness, see Buckingham, Leprosy in South Colonial India. 34. The Lepers Act empowered local governments “to appoint places to be leper asylums for the purposes of the Act and specify the local areas from which lepers may be sent to such asylums.” It was only implemented locally and not uniformly in force throughout India. Conference Purulia, 79 –87. 35. Conference Purulia, 75. At the conference in 1908, the superintendent of Purulia complained that too few pauper lepers had been sent under the Act. Robertson : The Leprosy Asylum in India 485 asylums.36 In 1941, the government Report on Leprosy and its Control in India stated that “In India we are in the peculiar position that practically every leprosy institution in the country is full, and thousands of applicants have to be refused each year for lack of accommodation.”37 Even in the late nineteenth century, the demand for admission was so high that the Mission to Lepers had to issue a notice to the missions it supported that from June 1898, asylums were forbidden to take on more leprosy-affected people or children or construct more buildings or incur expenses on behalf of the Mission without the sanction of its Committee.38 Consequently, the changes that took place in leprosy asylums in India were incremental, continuously shaped by a balance between the values and ideals of their founders and managers who were operating with scarce financial resources that were apportioned piecemeal and by demand from those who waited “outside” in the hope of gaining entry.39 L E P RO S Y L E G I S L AT I O N A N D T H E G OV E R N M E N T O F I N D I A The tours of Wellesley Bailey were conducted against an international backdrop of growing interest in leprosy in India, as well as an intense debate within India in the ten years leading up to the Lepers Act in 1898.40 In London, the National Leprosy 36. “Map of India: Showing Leper Institutions,” in Robert G. Cochrane, Leprosy: Symptoms, Diagnosis, Treatment and Prevention, 2nd ed. (London: British Empire Leprosy Relief Association, 1927), 22. 37. Government of India, Report on Leprosy and its Control in India, 40. 38. Minutes of the Mission to Lepers, June 1898, 148, Leprosy Mission International Archives, Brentford, London. 39. Minutes of Meetings of the Mission, Leprosy Mission International Archives, Brentford, London, UK. I argue that, in India, these institutions were overwhelmed by applicants for admission. See annual reports of the Mission to Lepers, e.g., The Mission to Lepers, A Report of the Sixty-Third Year’s Work in India and Burma: September 1936-August 1937, issued by the Indian Auxiliary in India, 16, accessed in Leprosy Mission International Archives, Brentford, London, UK. This report records the need to turn away applicants for lack of space. Rev. G. C. Mackintosh is quoted as saying that “When the Purulia Leprosy Relief Association opened their new Leper Home in May we were for a time relieved of the pressure of applicants for admission. However since then they have enrolled 200 and can take no more, and once again we are having to turn people away for lack of space.” 40. In India, in the decade of the seventies, when Hansen was attempting to replicate the causative agent of leprosy, Mycobacterium leprae, in Norway, and just after Bailey saw his first leprosy-affected people, an intense exchange of information on leprosy was taking place. See Jo Robertson, “In Search of M. Leprae: Medicine, Public Debate, Politics and the Leprosy Commission to India,” in Economies of Representation, 1790 –2000: Colonialism and Commerce, ed. Leigh Dale and Helen Gilbert (Aldershot, UK and Burlington, VT: 486 Journal of the History of Medicine : Vol. 64, October 2009 Fund appointed an Indian Leprosy Commission which was sent to India on 23 October 1890.41 Its investigation coincided with Bailey’s second tour, and the commission and Bailey crossed paths in Purulia, in Western Bengal. The commissioners found that “neither compulsory nor voluntary segregation would at present effectually stamp out the disease, or even markedly diminish the leper population, under the existing conditions of life in India.”42 Their commissioning body, the National Leprosy Fund, “entertain[ed] a precisely opposite opinion” and appended recommendations for segregation to the commissioners’ report.43 Studies of leprosy in India have independently analyzed the web of interconnected interests by which leprosy legislation was introduced incrementally at the end of the nineteenth century. They reveal the reluctance of the colonial government to implement legislation, the public pressure from European and Indian elites to detain and isolate beggars with leprosy, as well as the international climate that sought to determine the threat that leprosy represented to the Empire.44 As Buckingham shows in her study of leprosy in colonial South India, the application of legislation in India was subject to negotiation at every level of government. The Lepers Act was only Ashgate, 2007); and Michael Worboys, “Was There a Bacteriological Revolution in Late Nineteenth-Century Medicine?” Stud. Hist. Phil. Biol. & Biomed. Sci., 2007, 38, 20 –42. 41. The National Leprosy Fund, began as the Committee for the Father Damien Memorial Fund, was established to pay tribute to the life and personal sacrifice of Father Damien de Veuster, who had died in April 1889 after spending sixteen years on Molokai, in Hawaii, caring for people with leprosy. The Fund assembled a cast of luminaries— members included the Archbishop of Canterbury, the Duke of Norfolk, Lord Randolph Churchill, Baron Ferdinand de Rothschild, the Bishop of London, Sir William Jenner, and the Hon. G. Curzon, as well as prominent members of the medical fraternity—and was presided over by the Prince of Wales. By the end of June, the executive committee had decided that Damien’s memory should be perpetuated in four ways: a memorial would be erected to him at Molokai; a fund would be established for lepers in the United Kingdom; two Studentships would be endowed for doctors to study the disease; and an Indian Leprosy Commission was to be appointed. 42. National Leprosy Fund, President HRH The Prince of Wales, Report of the Leprosy Commission in India (Executive Committee: William Clowes and Sons, 1893), 389. 43. Ibid., 456. See William Tebb, The Recrudescence of Leprosy and Its Causation (London: Swan Sonnenschein, 1893), 302, for a discussion of the timing of the publication of the report and the response of the National Leprosy Fund to the findings of the Commission. 44. Kakar, “Leprosy in British India”; Buckingham, Leprosy in Colonial South India; Worboys, “Was There a Bacteriological Revolution”; and Robertson, “In Search of M. Leprae.” Robertson : The Leprosy Asylum in India 487 applied selectively by district and was specifically directed at removing leprosy-affected beggars from sight.45 She indicates that, by 1898, the government was happy to hand over responsibility for leprosy institutions to, and would increasingly provide financial support for, societies or missionary groups to maintain asylums46: Since most private institutions for leprosy care existing in India by 1898 were run under the auspices of the Mission to Lepers, the passing of the Lepers Act began the process of delineating the new relationship between the Mission and the government. The Mission insisted on retaining autonomy while receiving government funding linked to their provision of accommodation under the Act. Thus, from the early twentieth century, care and treatment of leprosy sufferers substantially became the responsibility of the Mission to Lepers.47 I differ from Buckingham with respect to the timing of this shift in responsibility. Buckingham argues that “From being almost entirely a government matter, leprosy care became a missionary concern.”48 I agree with this, but I argue that activities of the Mission and the changes to asylums preceded and, in some instances, provided a model for the government institutions. Although the transition was accomplished by 1898, the process can be seen to have commenced by the time of Bailey’s first tour in 1886. It is true that the Madras Leper Hospital was established and operational when Bailey visited in 1886, but the other Presidencies had nothing comparable at this time. Acworth, which was then known as the Matunga Leprosy Asylum and was financed by subscriptions and by the Municipality of Bombay, was opened in 1890.49 This unevenness in timing is most evident in the Bengal Presidency. In 1906 the government considered which districts in the province should be brought under the Lepers Act. This was after it had spent years prevaricating about 45. Buckingham, Leprosy in South Colonial India, 191. 46. Ibid., 188. 47. Ibid., 187. 48. Ibid. 49. Government of Bengal, “Bill to Provide for the Segregation of Pauper Lepers,” 15 September 1893, File 3-L/4 1, nos. 10 –11, 7, Municipal Department, Medical, 5/12139, Orissa State Archives, Bhubaneshwar, Orissa, includes “A Resume of the Steps Taken to Establish a Leper Asylum in Bombay and to Remove Lepers from the Public Streets;” and Government of Bengal, “Report of the Leprosy Commission – What Effect to be Given to Its Conclusions,” July 1895, File M 3-L/4, nos. 10–29, Municipal Department, Medical, 22/12134, Orissa State Archives, Bhubaneshwar, Orissa. 488 Journal of the History of Medicine : Vol. 64, October 2009 the transfer of the government funded asylum in Calcutta from Amherst Street to the new Albert Victor Asylum, only to decide that “By assisting the Mission Asylums, Government will be able to accomplish much more than it could by establishing asylums of its own.”50 It did this after it received a report on the Purulia Leprosy Asylum, which had been operating since 1888. The beginnings of this arrangement between the Mission to Lepers and the government of India started after Bailey’s 1886 tour, and negotiations probably began when he was in India in 1891 –92. Minutes of the Mission to Lepers committee note that “the Government of India have expressed their readiness to make grants in aid of leper asylums maintained by voluntary efforts” and the finance committee is instructed “to make a formal application for Government assistance for the asylums belonging to this committee . . . .”51 This would indicate that Bailey’s survey tours and reports on asylums were carried out in a climate of negotiation that would eventually lead to an arrangement agreeable to both the government and the Mission, and the changes in responsibility would have been accomplished by the time of the introduction of the Lepers Act in 1898.52 The nature of the process is demonstrated by the support provided for the Purulia asylum. It was first provided by the district and later by the provincial government, once it was decided to bring the asylum under the Lepers Act.53 Nonetheless, as a result of a measure of financial independence, with increasing support from members of the public, the Mission to Lepers took the opportunity to form asylums in a way that suited its own sense of purpose. 50. Government of Bengal, “Report of the Leprosy Commission – What Effect to Be Given to Its Conclusions”; and Government of Bengal, “Grants to Leper Asylums,” 10 March 1906, File M 3-L/8, no. 6, 2, Municipal Department, Medical, Orissa State Archives, Bhubaneshwar, Orissa. 51. Minutes of the Mission to Lepers, 13 February 1889, 112 –13, Leprosy Mission International Archives, Brentford, London. 52. Communication between the Mission and the various Presidencies was more developed in some instances than others, as is clear from Bailey’s correspondence with the Bengal government, which inquired about other provinces that were assisting the Mission. Government of Bengal (1907) Municipal Department, Medical, December, nos. 57 –64, “Grant to the Leper Asylums Maintained by the Mission to Lepers in India and the East,” Orissa State Archives, Bhubaneshwar, Orissa. 53. Government of Bengal, “Leper Asylum at Purulia and Lohardaga,” December 1895, File 3-L/5, nos. 40–49, Municipal Department, Medical File, 6/12152, Orissa State Archives, Bhubaneshwar, Orissa. Robertson : The Leprosy Asylum in India 489 These negotiations about Indian asylums would not have been independent of the deliberations at international leprosy conferences in this period, which recommended the isolation and segregation of leprosy-affected people, especially those belonging to the lower classes.54 The Berlin Conference in 1897 resolved that “Every leper is a danger to his surroundings, the danger varying with the nature and extent of his relations therewith, and also with the sanitary conditions under which he lives. Among the lower classes every leper is especially dangerous to his family and fellow workers, but cases of leprosy frequently appear in the higher social circles.”55 The Bergen Conference in 1907 would affirm the resolutions of the Berlin one and recommend the regular examination of contacts of people with leprosy, a prohibition on certain trades and occupations, and the strict isolation of leprosy-affected beggars and vagabonds.56 Country specific legislation, along with new leprosy institutions, was subsequently introduced following conferences and congresses in Strasbourg, in 1923, and in Cairo, in 1938.57 T H E E X T E N T O F L E P RO S Y A S Y L U M S I N I N D I A The descriptions that Bailey made during his three tours of Indian leprosy asylums offer an insight into the number of places in which people with the disease lived. On the first tour (1886–87), he found eleven centers where leprosy work was supported by the Mission to Lepers, three of which the Mission owned. Four years later in 1890– 91, there were twenty-one centers, six of which were outright Mission to Lepers homes, and by the 1895–96 tour, there were thirtyseven centers, fourteen of which the Mission owned (see Figure 1). The later extent of the development of asylums in India can be seen from a map produced in 1927, by Robert Cochrane, the medical director for the Mission, as a result of his own tour of inspection. This shows the institutions owned by the Mission to 54. Bailey attended the Bergen Conference and all subsequent congresses were attended by a member from the Mission to Lepers. 55. Isadore Dyer, “The Berlin Leprosy Conference,” New Orleans Med. Surg. J., 1897, 50, 361. 56. D. H. Currie, “The Second International Conference on Leprosy, Held in Bergen, Norway, August 1 to 19, 1909,” Pub. Health Rep., 1909, 24, 1357 – 61. 57. Anon., “Reports of the International Congress of Leprosy Held in Cairo, March, 1938,” reprinted for the Leonard Wood Memorial from the Int. J. Leprosy, 1938, 6, 389 – 417, first published in the J. Egyptian Med. Assoc., 1938, 21, 149 –74. 490 Journal of the History of Medicine : Vol. 64, October 2009 Fig.1. Map of Wellesley Bailey’s tour in 1886 – 87, found in Wellesley Bailey, A Glimpse at the Indian Mission-Field and Leper Asylums in 1886 – 87 (London: John F. Shaw, 1887), frontpiece to page 5. Robertson : The Leprosy Asylum in India 491 Lepers, those for which the Mission provided support, and those that were independent. This map also shows the population in each state of India, the estimated numbers of people affected with leprosy (according to the 1921 census returns), and the numbers of those who were segregated. In Bengal, e.g., there were two leprosy mission asylums at Raniganj and Bankura and one institution in Calcutta that was associated with the Mission. At the 1920 Calcutta conference of asylum superintendents, it was claimed that there were 150,000 leprosy-affected people in India and of those 5.8% were in asylums (see Figure 2). By 1886, different sorts of asylums existed simultaneously in India. One was the traditional indigenous charity shelter, or dharmashala, which accommodated leprosy-affected people among other indigents. Others were those that were managed by districts, municipalities, or provinces, as well as those run by missionary, charitable, or benevolent organizations. Traditionally, those affected with leprosy were treated in the same way as other recipients of charity who found shelter and sustenance in locally established and administered poor houses: Dharmashalas were generally situated near temples, holy places or in the larger town and cities. Such institutions therefore, traditionally accommodated all variety of needy and handicapped persons, there being no facilities, or even intention, to regard lepers as a special class of indigent requiring isolation. Dharmashalas were used as temporary or permanent abiding places or night shelters for those who might spend their days begging for alms.58 Some of these institutions had come into existence by royal decree, such as the King’s Poor House in Lucknow, which was established in 1831 by King Naseer-ood-deen Hyder. This asylum held eleven people affected by leprosy, among other recipients of charity, and was managed by a committee of European officers and Indians.59 In a remarkable contrast to this benign environment, in Bhopal State, people with leprosy were forced into the asylum founded by the Begum, at Sehore, and guarded there as prisoners.60 Princely 58. Shubhada S. Pandya, “Leprosy in the Bombay Presidency, 1840 – 1897: Perceptions and Approaches to its Control” (PhD diss., University of Bombay, 2001). 59. Bailey, Glimpse, 104 –5. 60. Bailey, Visit, 11. 492 Journal of the History of Medicine : Vol. 64, October 2009 Fig. 2. “Map of India: Showing Leper Institutions,” in Robert G. Cochrane, Leprosy: Symptoms, Diagnosis, Treatment and Prevention, 2nd ed. (London: British Empire Leprosy Relief Association, 1927), fronts on page 22. Robertson : The Leprosy Asylum in India 493 benevolence could also be inconsistent. At Chamba, Bailey found that the local prince was intent on reclaiming houses that he had originally granted as part of the asylum.61 District benevolent institutions included shelter for small numbers of leprosy sufferers. In Benares, the District Benevolent Institution housed six leprosy-affected men and two women.62 Local societies were also responsible for asylums such as that established by the Agra Local Relief Society in 1861, which in 1886 housed twenty leprosy-affected people.63 There were also asylums that were managed by the municipality, which in some instances, would appoint a board (of managers).64 Tarn Taran, in the Punjab, e.g., was a large government institution that was supported by different municipalities. These dispatched their leprosy-affected to the asylum and then contributed four rupees a month for every person sent.65 Municipal support could be a mixed blessing, as a municipality could be parsimonious or neglectful. Rawalpindi was supported by a Municipal and District Committee, but the native doctor told Bailey that no money was now being spent upon the place, as the Committee was waiting to see what the government would decide to do about an asylum.66 In addition to institutions established as a result of municipal or individual support, there were informal clusters of people affected by leprosy dwelling independently. On his first trip, Bailey discovered a group in huts by the wayside at Saharanpore, in the division of Meerut, in the North West Provinces.67 On later trips he would 61. Bailey, Glimpse, 149. 62. Ibid., 100. 63. Ibid., 170. The Dharmsala in Byculla, Bombay; the Dharmsala in Ahmedabad and the poor house at Poona, in the Bombay Presidency; the various District Charitable Association asylums at Allahabad; Benares; Amherst St., Calcutta; and Rawalpindi were all inspected by Bailey. 64. Bailey, Visit, 64. The two institutions at Saharanpore, one for men on one side of the city, and the other for women on the other side, were both supported and managed in this way. 65. Bailey, Glimpse, 153. Matunga or Acworth, in Bombay, was supported by two monthly grants of 1,000 rupees per month each from the Bombay Government and the Municipal Corporation. 66. Bailey, Lepers of Our Indian Empire, 9. This indecision in 1891 indicates the general uncertainty about who would take responsibility for the future of leprosy asylums and also prevarication that used the impending report of the Leprosy Commission as justification for indecision. 67. Bailey, Glimpse, 130. 494 Journal of the History of Medicine : Vol. 64, October 2009 seek out other groups in huts (at Neyoor, in the south, near Trivandrum; or Muzaffarnagar, in Derajat, Punjab), or in small villages (e.g., in Lodiana/Ludhiána, in Jullunder Commissionership, Punjab).68 In the Presidencies, larger hospitals, such as the JJ Hospital in Bombay, had a ward for leprosy-affected patients.69 In the Madras Presidency, the Monegar Choultry or Government Leper Hospital, in Madras was purpose built and considered a model of its kind.70 Separate asylums also existed in both British and Native States. The asylum in Bangalore belonged to the Mysore Government, and the Cochin Lazarus Hospital at Pallypuram belonged to the British government, even though it was situated in a Native State.71 Individual British benevolence could also be responsible for the establishment of an asylum such as that at Almora, in the North-West provinces, which was founded in 1840 and maintained by Sir Henry Ramsay when he was a Civil Officer in the district.72 Many establishments resulted from a combination of British and Indian local benevolence. As an example, the asylum at Bhagulpore, in Bihar and Orissa, was reconstructed in cooperation with the chairman of the municipality, Shib Chandar Banerji, Rai Bahadur. In addition, 1,000 rupees had been contributed by an Englishman who lived in the district during the winter months, and the Mission to Lepers also donated 500 rupees. As a result, a combined sum of 10,000 rupees was available for this asylum.73 68. Bailey, Lepers of Our Indian Empire, 160, 210; Bailey, Visit, 63. 69. Pandya, “Leprosy in the Bombay Presidency, 1840 –1897,” 220 – 24. 70. As discussed by Buckingham, Leprosy in South Colonial India. 71. Ibid., 38. The Calicut Leper Asylum was a government institution, as was Baba Lakhan, near Siálkot, in the Punjab. 72. Mission to Lepers, Fifty Years Work for Lepers, 1874– 1924: An Account of the Funding and Growth of the Mission to Lepers (London: Mission to Lepers, 1924), 42. Similarly, the Asansol Asylum, in Bengal, was a gift to the Mission to Lepers from Georgiana, Countess of Seafield, who was inspired by the memory of a leprosy-affected Indian convert to Christianity. A note on Asansol appears in the minutes of the Mission to Lepers, which mentions plans for an asylum and requests of financial support. Minutes of the Mission to Lepers 1890, 136, The Leprosy Mission International Archives, Brentford, London; Bailey, Lepers of Our Indian Empire, 145. 73. Bailey, Lepers of Our Indian Empire, 148. The joint local project for the new Leper Asylum at Matunga, in Bombay, in 1890 would show the culmination of this form of civic cooperation: in response to Acworth’s and the city’s growing concern about leprous beggars, buildings were subscribed to by the public, and this enabled a sum of 73,000 rupees to be spent on the asylum. Robertson : The Leprosy Asylum in India 495 States were increasingly happy to hand over management of an asylum for a term to a willing and competent Western missionary. For example, the asylum at Srinagar had originally been intended to be a state concern and was to be managed by state officials, but it was subsequently offered for five years to Dr. Neve, a medical missionary.74 In 1891, he constructed buildings to accommodate thirty patients, and received 5,000 rupees from the state for the buildings and an additional 2,000 rupees a year to run the asylum. The Mission to Lepers increasingly provided support to many asylums by sharing responsibility for costs with either a District or a Municipal Association and/or another missionary group, thereby gaining more say in the new constructions. By the end of 1896, fourteen missionary organizations received funds for buildings and, in some instances, funds for the upkeep of an asylum, while the cooperating missionary organization would provide staff.75 In Allahabad, a small asylum on the Nynee road, over the Jumna bridge, had mostly been supported by the Allahabad District Charitable Association and superintended by the American Presbyterian Missionaries. In 1891, it also received an annual grant from the Mission to Lepers in India, as well as the costs of building one row of houses.76 An asylum such as that at Rurki in the Punjab came to be almost entirely supported by the Mission to Lepers in India by 1891, although it still received a small grant from the Municipality. New accommodation for this asylum was to cost about £10, and when the houses of the asylum were full to capacity, maintenance was estimated to cost about £150 per annum.77 Sometimes support was provided for a specific purpose so that the cost of the asylum was divided between benefactors. In Dehra, e.g., the support of the institution came from interest earned on trust funds, as well as from voluntary subscriptions and donations from Dehra residents, but the cost of the religious work, specifically the support of a native pastor and a subordinate Indian 74. Bailey, Lepers of Our Indian Empire, 16. 75. Bailey, Visit, 92. Almora was managed by the London Missionary Society. Bailey, Glimpse, 111; Subathu in the Punjab was established by John Newton and supported by the Mission to Lepers, Bailey, Glimpse, 137; and Chumba, which had been built by Bailey as a missionary for the Church of Scotland, Bailey, Glimpse, 148. 76. Bailey, Glimpse, 119; and Bailey, Visit 59. 77. Bailey, Glimpse, 70. 496 Journal of the History of Medicine : Vol. 64, October 2009 leprosy-affected Christian, was met by the Mission to Lepers in India.78 On his later trips, Bailey would return to many sites he had visited previously and report on their condition and development, especially if the Mission to Lepers had provided support. The two later trips were notable for reports of new establishments, including the purchase of land and the progress of construction, as well as the cost of upkeep. These new asylums were either wholly owned by the Mission to Lepers and run by a missionary organization or they were the initiative of another missionary organization and supported by the Mission to Lepers. LO CAT I O N S O F E X I S T I N G A S Y L U M S In a country as diverse as India, the locations of asylums could be expected to be mixed; nonetheless, some commonalities do emerge. The practice seems to have been to locate the asylum some distance from the city and beside a thoroughfare. The asylum in Agra, e.g., was situated two miles past the fort, on the river road.79 Proximity to a road enabled the inhabitants of the asylum to make their living by begging. In Rurki, Patiála, in the Punjab, a few huts were placed by the roadside, outside the township, and in Saharanpore, seven men found shelter in a long row of houses situated on an open plain outside the city.80 These huts appear to have been haphazardly grouped and life there proceeded with minimal or only cursory attention from outsiders. Some of these sites were quite large and very well organized. At Lodiana, e.g., a community of forty men, women, and children dwelt in a village that was well supplied with ponies, cattle, and four goats. The ponies were used for travel to locations for begging. This village was also strategically located close to the camping ground used by the British troops as they marched through Lodiana.81 In some instances, a site may have accidentally or purposefully served a therapeutic purpose; for example, the asylum at Calicut was located on the beach, close to a fishing village.82 Other 78. 79. 80. 81. 82. Bailey, Glimpse, 132 –3; and Visit, 65 –71. Bailey, Glimpse, 170 Bailey, Visit, 66–67; and Bailey, Glimpse, 130. Bailey, Lepers of Our Indian Empire, 160 – 61. Ibid., 219. Robertson : The Leprosy Asylum in India 497 situations were less appealing. Prisoners affected by leprosy in the Nagpur jail were not only imprisoned, but also isolated from other internees.83 One interesting instance of ownership and autonomy occurred as a result of sustained occupation of a particular location. At Muzaffarnagar, fourteen people, ten of whom had leprosy, who made their living by begging, occupied a few huts in a mango grove. Bailey comments that they had been there so long that they had “Marusi rights,” which forced legal recognition of land ownership so that they could not be disturbed.84 The built environment of these early sites also varied considerably both in type of structure and quality of construction. While the earliest known asylum in India, the Cochin Lazarus Hospital, Pallypuram, which had been created by the Portuguese, renovated by the Dutch, and was still in operation under the British when Bailey visited in 1886, was “clean, airy, and in good order,” in some notable instances, accommodation was clearly makeshift and inadequate.85 The shelter at Alleppey, in the Native State of Travancore, was simply one long shed made of matting and bamboo, with a sand floor that accommodated fifty people, fourteen of whom suffered from leprosy.86 Similarly, the houses at Saharanpore, which were a long row of bare houses without any verandas or shelter from the sun, seemed to have been erected and simply left to those with the disease.87 The Dharmshala in Bombay offered the worst prospect, with its narrow passages and cramped cells.88 Even specially organized accommodation had been constructed without much forethought for the comfort and health of the sick: the government-built houses at Tarn Taran were badly constructed, poorly ventilated, and had low floors that did not permit the circulation of air.89 At the same time, there were sites that were pleasant and well planned; for example, the houses in the Dharmsala in Ahmedabad 83. Major Buchanan, “The Contagiousness of Leprosy,” in Conference Wardha, 7. 84. Bailey, Visit, 64. 85. Bailey, Glimpse, 38. 86. Ibid., 41. 87. Ibid., 130. 88. Ibid., 183 –84. Pandya, “Leprosy in the Bombay Presidency, 1840 –1897,” 220 –24, offers a different perspective on this ancient refuge for the poor. 89. Bailey, Visit, 153. 498 Journal of the History of Medicine : Vol. 64, October 2009 were large and airy, and the Native Leper Asylum in Bengal was “on a nice site” and had several well-built wards.90 Bailey often remarked on the unused capacity of several asylums, particularly the asylum at Wazirabad, in northern Punjab: “The Leper Asylum was a nice little building of four rooms, capable of housing twelve lepers comfortably; but there were no lepers.”91 AC Q U I R I N G N E W S I T E S A N D I M P ROV I N G E X I S T I N G A S Y L U M S Increasingly, the Mission to Lepers established new sites for leprosy asylums, in addition to improving existing sites. Land acquisition occurred incrementally as the need arose and in response to the local conditions of purchase. In the period of Bailey’s three trips, new sites were established at Srinagar, Moradabad, Purulia, Asansol, Bhagulpore, Burdwan, Ranigunj, Jubbulpore, Wardha, Ratnagiri, and Alleppey.92 When there was no other way of securing the land, a perpetual lease was taken, as for the site for Asansol Asylum.93 Building and development progress was reported in subsequent trips by Bailey and in annual reports to the public. Improvements to existing sites took the form of providing better accommodation in more regulated spaces that catered to the physical and spiritual wellbeing of the residents and were dictated by commonly held assumptions that sound accommodation, ventilation, shade, and pleasant surroundings would benefit the health and wellbeing of the sick. As an example, the people at Rurki who were discovered living in wretched huts by the roadside were provided with an enlarged space that accorded more closely with the idea of an asylum, including new accommodations, a prayer room, and trees for shade.94 Similarly, new accommodation was provided for the people living in old huts at Neyoor, Chandag, and at Srinagar.95 90. Bailey, Glimpse, 177 –78; and Bailey, Visit, 59– 60. 91. Bailey, Lepers of Our Indian Empire, 37. 92. Srinagar (Bailey, Lepers of Our Indian Empire, 16); Moradabad (Bailey, Lepers of Our Indian Empire, 69); Purulia (Bailey, Visit, 15 –23; and Bailey, Lepers of Our Indian Empire, 122– 23); Asansol (Bailey, Visit, 26; and Bailey, Lepers of Our Indian Empire, 145 –47); Bhagulpore (Bailey, Visit, 55; and Bailey, Lepers of Our Indian Empire, 148); Burdwan (Bailey, Lepers of Our Indian Empire, 174); Ranigunj (Bailey, Visit, 28); Jubbulpore (Bailey, Visit, 13); Wardha (Bailey, Visit,14); Ratnagiri (Bailey, Visit, 87); Alleppey (Bailey, Lepers of Our Indian Empire, 216). 93. Bailey, Lepers of Our Indian Empire, 177. 94. Bailey, Lepers of Our Indian Empire, 66; and Bailey, Visit, 66. 95. Bailey, Lepers of Our Indian Empire, 17, 201 –7; and Bailey, Glimpse, 121. Robertson : The Leprosy Asylum in India 499 Sometimes the cost of these improvements was shared. In order to replace the “charity shed” at Alleppey, in which Bailey had discovered fifty people in benighted conditions, the new asylum there became a joint affair between the Mission to Lepers in India, which provided 750 rupees, and the Rajah of Travancore, who donated 500 rupees. In addition to this, “a few friends in India” promised other sums.96 The Mission to Lepers also contributed financial support for the expansion of existing and successfully run ventures, such as that at Almora. In 1890, the Mission’s committee increased their grant from 1,800 rupees to 2,400 rupees for increased numbers. They also provided 200 rupees towards repairs and continued to provide annual grants.97 When a new site for an asylum was chosen, in addition to the availability of the land, its suitability was judged on the balance between remoteness and accessibility. The site for the new asylum at Srinagar was considered to be suitable because it stood on a peninsula that extended into the lagoons, and at one point touched the Great Lake. It fulfilled the conditions both of remoteness and accessibility, for while those affected with leprosy would be well away from other people, they would be within easy reach of the town, either by land or by water. The land for the Asansol asylum was situated on a long narrow strip of land, with some rising ground that had fields for cultivation. It was located beyond the railway lines and on the opposite side of the railway station, away from other dwellings, but still within easy access.98 At Raniganj, in Bengal, a new asylum was built two miles outside the town, on a high, dry site.99 Sometimes the choice of remoteness was considered to be in the interests of those affected by leprosy. The asylum at Sabathu, in the Punjab, was at one time considered to be a suitable site for Europeans with the disease because it was in the hills.100 The suitability of a site was enhanced if there were already buildings on the property that could be adapted to asylum use. The house and property at Bhaugulpore, in West Bengal, already had a 96. 97. 98. 99. 100. Bailey, Glimpse, 42. Bailey, Lepers of Our Indian Empire, 136. Ibid., 177. Bailey, Visit, 29. Ibid., 73 –74. 500 Journal of the History of Medicine : Vol. 64, October 2009 good pucca house and some out-offices that were ready for use.101 Similarly, the site at Wardha, in the Central Provinces, had several good buildings and also others in need of repairs.102 At Ratnagiri, Konkan, in the Bombay Presidency, a piece of ground of about two and a quarter acres by the river recommended itself because it already had one small hut on it and the site seemed suitable for further permanent buildings.103 Often negotiations for suitable land had to take into account competition with other interests. At Ranigunj, it was necessary to negotiate with the General Manager of the Bengal Coal Company to ask if he would try to secure a site for an asylum.104 There were sometimes difficulties in finding a site. At Bhandara, near Nagpore, the search for a site was a prolonged affair. Bailey described the process: In the evening I drove out with Drs Revie and Sandilands, and Mr Rango Harri, Secretary to the Municipal Committee, and a pleader. Sandilands was interested in an asylum, and the Mission to Lepers had promised him a grant for building and an annual grant for maintenance, but a site had to be found first. One possibility was located on the other side of the river, which Mr Harri had offered as a gift to the Leper Mission, but it was decided that during the rainy season it would become flooded.105 The next day another site was inspected and was considered favorably because it had a mango grove, a small tank, and a few good fields, but it belonged to some local people, and they would have to be persuaded to sell it. Two days later, the group was still looking and had not found anything suitable.106 Similarly, at Jubbulpore, a site that was suitable was not for sale, and although some native Christians offered a site on their own property, it was not considered suitable.”107 101. Pucca housing referred to permanent solidly-built constructions made of kilnburnt brick, stone, or mortar. Bailey, Lepers of Our Indian Empire, 148. 102. Bailey, Visit, 14– 15. 103. Ibid., 87. 104. Bailey, Lepers of Our Indian Empire, 175. 105. Ibid., 180 –81. 106. Ibid., 183. 107. Bailey, Visit, 13– 14. Robertson : The Leprosy Asylum in India 501 T H E I D E A L A S Y L U M : WA L L S A N D CO U RT YA R D S In most instances, before the Mission to Lepers began constructing asylums, dwellings for people with leprosy were enclosed by a wall. Walls did not necessarily make the shelters prison-like, and they may have served to provide seclusion just as walls did in private dwellings in India at that time. Thomas Metcalf points out that the British in India also built themselves bungalows that were situated in courtyards.108 The already-existing asylums usually had some sort of central area, in which huts, small houses, or a building, containing several small rooms, provided shelter for men and women. In 1886, the Cochin Lazarus Hospital was in a large enclosed compound, as was the Native Leper Asylum at Baidyanath, Bengal, and in Agra, the asylum, albeit laid out in a large quadrangle, was enclosed by a high wall.109 The asylum at Dehra and the Dharmsala in Ahmedabad were surrounded by high walls, and the Calicut Leper Asylum was enclosed by a wooden fence on the front part that faced the sea.110 Missionary-built asylums that pre-existed the Mission to Lepers varied in character. One of the most remarkable asylums at Almora, which was constructed by Sir Henry Ramsay in 1849 and run by the London Missionary Society, was built on terraces.111 At Chumba, the asylum, which Bailey himself had built, was divided into two parts; the first set of buildings, forming two sides of a square, consisted of low huts; and the second set of buildings was of a single row of huts, about 400 yards further down the river.112 The site does not seem to have been enclosed in any way. Buckingham traces the history of the politics of contestation that was brought about by the walls of the Madras Leper Asylum. There the walls around the asylum highlighted the ambiguous status of the leprosy-affected person: “Many leprosy sufferers were not entirely convinced of their status as patients in the Madras Leper Hospital and feared that once they had entered the asylum they would be 108. Thomas R. Metcalf, “Architecture and the Representation of Empire: India, 1860–1910,” Representations, 1984, 6, 37– 65, 38. 109. Bailey, Visit, 59– 60; and Bailey, Glimpse, 170. 110. Bailey, Glimpse, 312 –13; Bailey, Visit, 79; Bailey, Lepers of Our Indian Empire, 219. 111. Bailey, Visit, 32. 112. Bailey, Glimpse, 149; and Bailey, Lepers of Our Indian Empire, 41 –42. 502 Journal of the History of Medicine : Vol. 64, October 2009 prevented from leaving. . . . Rumours had already gone abroad that the hospital was indeed a prison for incarceration of the leprosy sufferers in Madras.”113 Additionally, the contest between medical authorities and the government over the height of the wall “reflected the complexity and incoherence of British notions of confinement and charitable care for leprosy sufferers in Madras.”114 Surrounding walls seemed to become increasingly necessary for the construction of new asylums. But, if the example of the asylum at Pui can be relied upon, the nature of the wall could vary. When the Collector of the District wanted this asylum fenced, the Mission to Lepers planned to plant a prickly pear hedge around it at a cost of about ten rupees an acre.115 At the Chandag asylum, which was acquired by the Mission to Lepers, a row of nine houses was built a little down the hill and to the north of the main bungalow.116 Once again, there seems to have been no attempt at enclosing the site. Nonetheless, it seems that the general practice was to erect a surrounding wall, and when the Mission to Lepers constructed the new asylum at Alleppey, they built a surrounding brick and mortar wall, and the new shelters for the people at Rurki were enclosed in a courtyard.117 While the inmates of Purulia were strictly prohibited from going to the town, there were no guards or walls or fences of any kind. Reverend Hahn, the Superintendent of Purulia, reported that the aim was to manage the asylum by attracting people rather than by using “forcible detention.”118 Courtyards were also remarked upon as offering a pleasant space and as forming a focal point for an asylum. Early sites that preexisted the Mission to Lepers were described by Bailey as having pleasant courtyards. The courtyard to the Agra Asylum was described as cool and shaded by several fine trees.119 The Dharmsala Leper Asylum in Ahmedabad was a large open place 113. Buckingham, Leprosy in Colonial South India, 54. 114. Ibid., 59. 115. Bailey, Visit, 85. 116. Bailey, Glimpse, 121 –22. 117. Bailey, Lepers of Our Indian Empire, 216; and Bailey, Visit, 66. 118. Conference Purulia, 71. Independently of the Mission to Lepers, the new Acworth asylum at Matunga, in Bombay, constructed by the Municipality, was surrounded by a barbed-wire fence. (Bailey, Lepers of Our Indian Empire, 222; Pandya, “Leprosy in the Bombay Presidency,” chap. 9.) 119. Bailey, Glimpse, 170. Robertson : The Leprosy Asylum in India 503 with large trees and surrounded by a wall.120 The compound at Bhagulpore was considered to be very beautiful and suitable as an asylum.121 A line of graceful plantain trees grew between the two rows of huts in the middle of the Cochin enclosure.122 Under the direction of the Mission to Lepers, courtyards became increasingly structured. The modest huts by the wayside at Rurki became part of a larger establishment with a courtyard and a large shady tree.123 On Bailey’s third trip, it is described as being an enclosed space with a large shady tree, seven houses, a church, and gardens.124 When the Mission rebuilt Alleppey, they constructed a courtyard one hundred yards square with coconut trees in the center.125 S E PA R AT I O N S W I T H I N T H E CO M PO U N D In 1889, the British government required that asylums separate men and women stating that: His Excellency in Council expressed the opinion that in such institutions the necessity of strictly segregating the sexes should invariably be kept in view, and desired that this condition should be enforced in the case of every institution for the relief of lepers receiving aid from public funds, and that every effort should be made to induce the supporters of institutions of the kind maintained by voluntary contributions to adopt a similar rule.126 The reason for this requirement was expressed by Gavin Milroy in 1874 in response to Carter’s report on Norwegian measures to deal with leprosy. Speaking for the Royal College of Physicians of London, he stated: The fact that Leprosy is transmitted by parent to child is indisputable, and as Leprosy by descent is often through a natural error (mistaken for Leprosy by contagion, the members of one family being naturally in 120. Ibid., 177 –78. 121. Bailey, Visit, 55– 56. 122. Bailey, Glimpse, 37. 123. Bailey, Lepers of Our Indian Empire, 66. 124. Bailey, Visit, 66. 125. Bailey, Lepers of Our Indian Empire, 216. 126. The original opinion of 1889 is reproduced in Government of Bengal, “Segregation of Pauper Lepers,” 1895, File 3-L/4 16, no. 30, 1, Municipal Department, Medical, 1/12135, Orissa State Archives, Bhubaneshwar, Orissa. 504 Journal of the History of Medicine : Vol. 64, October 2009 contact, it is important that this fact should be borne in mind. It is a fact which points also to the expediency of placing asylums for females at a distance from asylums for males when circumstances permit, and when the numbers are such to justify separate establishments.127 Nevertheless, in structures that existed before the changes brought about by the Mission to Lepers, there were inconsistencies in the application of these policies. In the Agra asylum, men and women occupied different sides of the courtyard, but the Dharmsala in Bombay, which was roundly condemned by Bailey, made no such distinction.128 At Dehra and Sehore, Bhopal State, there were separate large courtyards for men and women, and at Moradabad, the men were in one yard and the women were in another, with a line of houses back to back acting as a division and a barrier.129 On a larger scale and breaking with the courtyard enclosure structure, in the asylum run by the London Missionary Society at Almora, the women’s terraces were separated from the others by a wall running the whole length of the terrace.130 Kakar states that many features of the medieval European leprosy asylum were reproduced in India and, as a result, practices such as sexual segregation and sexual abstinence were implemented without question, but there were other pressures that reinforced this imperative.131 Benefactors of the Mission to Lepers were adamant that men and women be kept apart: first, there was no intention of supporting leprosy-infected men and women in dubious moral conditions, but the possibility of births and the chance of infecting children with leprosy became an equally strong reason for separation. Increasingly, the Mission constructed asylums that would keep men and women separate. By 1895, at Alleppey, a wall was added down the middle of the enclosure, and at Asansol, at the same time, the length of the new site was considered advantageous because it would be possible to have men’s quarters at one end and women’s at the other.132 127. Gavin Milroy to the Honourable R. H. Meade, 8 September 1874, vol. 35, 1875, 191– 99, General Department, Maharashtra State Archives, Mumbai, India. 128. Bailey, Visit, 170; and Bailey, Glimpse, 10. 129. Bailey, Glimpse, 312 –13; Bailey, Visit, 11; and Bailey, Lepers of Our Indian Empire 69–70. 130. Bailey, Glimpse, 111. 131. Kakar, “Medical Developments,” 65 –66. 132. Bailey, Lepers of Our Indian Empire, 177, 217 –18. Robertson : The Leprosy Asylum in India 505 Although Bailey was troubled by the separation of elderly married couples in particular and married couples in general because it went against Christian principles, it is without doubt one of the features of asylums that he never fails to remark on. He approved of the situations in which the sexes were separated, and strongly disapproved of the instances where men and women were free to mix with each other. Debates about segregation were on the agenda of meetings of superintendents of the asylums well into the early twentieth century. In 1908, superintendents still debated whether to separate leprosy-affected people, who were already married, from each other, and the Conference at Purulia was reminded by Bailey, the Chairman of the Conference, that “many subscribers at home refused to assist the Mission unless assured that all lepers were carefully segregated,” but practices in asylums still varied.133 In the Punjab, married couples were allowed to live together. In the United Provinces, segregation was still in the process of being introduced in 1908, and couples who had been in residence for some time were permitted to live together.134 Further south, segregation was strictly enforced. When Bailey visited Purulia in 1891, the men’s quarters and women’s quarters were separated by a high wall, with a door that was locked at night.135 In the same year, Dr. Hilson, the Surgeon-General and Inspector-General of Civil Hospitals, from Bengal, visited Purulia and reported that he was pleased with arrangements for the segregation of the sexes. He also noted that children were housed in separate buildings “and while allowed to see their parents occasionally, do not have any close or intimate connection with them.”136 This process of segregation continued unevenly, but irrevocably, with the 1908 conference of leprosy asylum superintendents recommending the segregation of the sexes, except in exceptional circumstances.137 Even in 1941, the government of India’s report stated that it was desirable for married 133. Conference Purulia, 20. 134. Ibid. 135. Bailey, Lepers of Our Indian Empire, 122 –23; Rev. K. W. Nottrott, “Segregation of the Sexes; and of Untainted Children,” Conference Wardha, 26. Discussion of the segregation of children is outside the scope of this article. 136. Hilson cited in Bailey, Lepers of Our Indian Empire, 128. 137. Conference Purulia, 21. 506 Journal of the History of Medicine : Vol. 64, October 2009 life in leprosy institutions to be forbidden unless the woman was beyond child-bearing age.138 S T RU C T U R E S W I T H I N T H E CO M PO U N D The constructions within the asylum compound were often arranged in rows and barracks, and their placement was governed either by the terrain upon which they were built or the availability of local building materials. Under the supervision of the Mission to Lepers, these constructions became more standardized. The intention of the overall design was to provide shared accommodation for living, rather than to create a hospital, although something of the character of a monastic retreat is retained by having small rooms. In 1886, the Cochin Lazarus Hospital was in a large compound, with two sets of fourteen houses arranged in two rows of seven: one row for men and the other for women. These were placed back to back and parallel with each other, and each row was enclosed with a railing and a gate. The structures at the government institution at Tarn Taran were also arranged in two long rows of double houses that were placed back to back.139 At Sehore in Bhopal State, a long row of houses opened into each of the two separate courtyards.140 Some asylums such as the asylum at Almora were designed as barracks, with three barracks of five houses each, on each of the three central terraces.141 At Baba Lakhan, too, there were three barracks parallel to each other containing twenty-four rooms each (twelve on either side, back to back), and providing accommodation for seventy-two inmates.142 Eventually barracks gave way to cottage accommodations that were described in the Central Provinces (Champa) as a preferred example in 1920 to the attendees at the Calcutta conference, when the Superintendants from the various asylums gathered to confer with each other, pool their experiences, and standardize their practices.143 These cottages were 48 feet long and 31 feet wide, with walls 14 feet high and one and a half feet thick. Each had three 12 by 14 feet living rooms and corresponding 138. 139. 140. 141. 142. 143. Government of India, Report on Leprosy and its Control in India, 43. Bailey, Glimpse, 154. Bailey, Visit, 11. Bailey, Glimpse, 111. Bailey, Visit, 82– 83. Conference Calcutta, 91–94. Robertson : The Leprosy Asylum in India 507 7 by 14 feet veranda rooms. Each of the three main rooms could accommodate four people, and the veranda rooms were for cooking or for sleeping. Ventilation was provided by transoms, two end windows, and also by low partition walls that did not reach to the roof of the building. Local materials and local building practices had a determining influence over the built environment of the leprosy asylums in India. The structures within the new courtyard at Rurki consisted of seven small mud houses with tiled roofs and a church made of the same material.144 The asylum at Pui in the Kolaba district of the Bombay Presidency consisted of a pucca building, made of stone and lime, with a roof of Mangalore tiles. It had two rows of five rooms that were placed back to back, with a verandah in front of each set of rooms. The partitions between the rooms were of rods covered in plaster.145 New structures were invariably grafted onto what was already standing. At Bhagulpore, e.g., in addition to the already-existing old bungalow, five wards were added so that each ward had three large rooms each and each room accommodated four people.146 By 1920, superintendents of the asylums were directed by the Mission that accommodation be constructed from substantial materials such as bricks that were either pointed or plastered. All wood work was to be of sawn timber and the doors and windows were to be made of seasoned timber. The roof had to be built out of materials that would be rainproof. Floors could vary with location. In Calicut, floors were of glazed tiles, in Cuttack, floors were of cement, and in the Central Provinces, mud floors were preferred because they were not so cold and could be cleaned daily with disinfectant.147 The surroundings of asylums were often described by Bailey, and many asylums were considered to be situated in particularly beautiful settings. The emphasis on gardens and trees served to soften the impression of the asylum and to create a sense of a garden retreat.148 Before improvements by the Mission to Lepers, the 144. Bailey, Lepers of Our Indian Empire, 66. 145. Bailey, Visit, 74. 146. Ibid., 55 –56. 147. P. A. Penner, “The Best Type of Ward,” Conference Calcutta, 88. 148. The effect of settings for the leprosy asylum on Robben Island, in South Africa, is discussed in Harriet Deacon, “Landscapes of Exile and Healing: Climate and Gardens on Robben Island,” South Afr. Archaeol. Bull., 2000, 55, 147 –54. 508 Journal of the History of Medicine : Vol. 64, October 2009 asylum at Ahmedabad was described as being beautifully situated in a grove of fir trees and next to a tea garden, and the women’s huts at Saharanpore were near some old gardens and close to a mango grove.149 The asylum at Dehra also stood in the middle of a green plain, with groves of mango trees, and it was approached by a long road lined with trees.150 Bailey described the asylum at Chumba, which he built himself in 1875, as being beautifully situated on one side of the Ravi river, about two miles from the city. This asylum was to be found down “a lovely road” that followed “the right bank of the river.”151 The area around the asylum at Chandag, which had originally belonged to a European settler and then to the Mission to Lepers, was also described by Bailey as spectacular: In front of the houses and to the east, there was a fine row of blue gum trees, and this was expected to provide shade in the warm weather. There was a well-cut path from the main road up to the house, lined with young cedar trees; and on the left on the approach, a piece of ground was laid out for a garden, and some hundreds of English fruit trees of different sorts were growing. The whole stands on the top of a ridge, with a beautifully fertile valley sloping away to the west . . . in the midst of a great amphitheatre of hills, stands Pithoragarh. There are high hills all round, while to the north are to be seen several peaks of the “Snows.” On the north end of the ridge on which Chandag stands, and on a tableland, is a temple, at which a great mela [explain] is held every August. Altogether, this place is beautifully situated.152 If the surroundings of the asylum were unappealing, every effort was made to improve them, especially by planting trees to provide shade. While the new Moradabad asylum was situated away from the city and close to the lake, it was not wholeheartedly endorsed by Bailey because it was situated on a bare stretch of ground without shade and he thought that one of the few disadvantages of the site chosen for the new asylum at Asansol was a lack of trees, but there were plans to plant some immediately.153 Generally, the new establishments took the need for having surrounding trees into account so that, e.g., the new asylum at Neyoor was built on 149. 150. 151. 152. 153. Bailey, Glimpse, 131, 177 –78; and Bailey, Lepers of Our Indian Empire, 64 –65. See quotation from Bailey, Glimpse, 312 –13. Bailey, Lepers of Our Indian Empire, 41– 42. Bailey, Glimpse, 121 –22. Ibid., 69, 177. Robertson : The Leprosy Asylum in India 509 elevated ground which ran down towards a large piece of water, fringed by Palmyra palms and other trees, and the new asylum at Srinagar was built near a magnificent crimson flowering chunar tree. This emphasis on aesthetic surroundings cannot be disregarded. It was obviously important to demonstrate that the new asylums were well situated in ways that would soothe the inmates. Additionally, the beauty of the physical landscape was often an occasion for a meditation on the contrast between the beauty of the surroundings and the condition of the people affected with leprosy. AG R I C U LT U R A L CO LO N I E S By degrees the asylums sponsored or owned by the Mission focused upon providing garden plots needing to be tended in order to occupy the inhabitants, and also to allow the asylum to become increasingly self-sufficient. The courtyard of the newly enlarged asylum at Rurki included some small gardens with shrubs and trees in the center, and adjoining land with shady trees.154 Bailey noted the blossoming peach and apricot trees in front of the houses at Subathu Leper Asylum. At this asylum, the inmates also cultivated their own gardens.155 At Tarn Taran, one of the improvements influenced by the Mission to Lepers was the laying out of small plots for those who were able to use them: The surroundings of the asylum are much improved; nice little plots of ground having been laid out, and given to the inmates capable of cultivating them. There is an abundant supply of water, so that the plots are easily worked, and the lepers take great pleasure in them, besides which the work is very good for them. 156 The Leprosy Investigation Commission of the British National Leprosy Fund initially suggested the idea of “experimental leper colonies or farms in rural districts” for people affected by leprosy, in its report of 1891, and this idea was reiterated by the government of India in 1895: 154. Bailey, Lepers of Our Indian Empire, 96– 98; and Bailey, Visit, 66. 155. Bailey, Glimpse, 138. 156. Bailey, Visit, 76. 510 Journal of the History of Medicine : Vol. 64, October 2009 it may, it appears to His Excellency in Council, be found desirable to establish lepers asylums or farms in remote places outside municipal areas and within the jurisdiction of a Local Board. The Bill might provide for the sending of pauper lepers to such asylums or farms without bringing into operation the powers of arresting pauper vagrants within the areas from which lepers may be permitted to be sent to them.157 Influenced by this and developing what had already begun, sites for asylums with the potential for farming and gardening were increasingly sought out. The Mission to Lepers’ acquisition of Chandag was considered favorably by Bailey because it had extensive grounds, some of which were laid out in terraced fields of wheat and rice.158 There were also plans at Subathu for larger agricultural projects.159 At Asansol, fields suitable for cultivation were included in the site, and at Rawalpindi, little plots of ground were laid out for cultivation. By 1934, the asylum at Raniganj, in Bengal, was referred to as a “model garden-town.”160 In concert with attempts to persuade the government of India to amend the 1898 Lepers Act by widening the definition of “the leper” from applying to those “in the process of ulceration” to include “any person suffering from any variety of leprosy,” the idea of large leprosy settlements or agricultural colonies was developed.161 The practicality of this idea was canvassed at the 1920 Conference of Superintendents in Calcutta. The Reverend Frank Oldrieve, the Secretary for India for the Mission to Lepers, expressed the aspirations of the conference when he stated that “The compulsory segregation of all lepers in India is not, in my opinion, a practical question, but the segregation of even 20,000 or 30,000 pauper lepers, if there should be so many, is certainly a thing that can be attempted, and if it can, then the attempt should most 157. National Leprosy Fund, Report of the Leprosy Commission in India (Executive Committee: William Clowes and Sons, 1893), 389; and Government of Bengal, “Bill to Provide for the Segregation of Pauper Lepers: From J. P. Hewett, Offg. Sec. to the Government of India to the Secretary to the Gov. of Bengal, Municipal Government,” 7 February 1895, 12/132, File 3-L/4 14, no. 28, Municipal Department, Orissa State Archives, Bhubaneshwar, Orissa. 158. Bailey, Glimpse, 121 –22. 159. Bailey, Visit, 74. 160. Bailey, Lepers of Our Indian Empire, 7 –8, 177; Mission to Lepers, Sixty Years of Service, 1874 – 1934, on Behalf of the Lepers and Their Children (London: Mission to Lepers, 1934), 31. 161. Mission to Lepers, Conference Calcutta, ii, 141. Robertson : The Leprosy Asylum in India 511 certainly be made.”162 This was to be achieved by establishing large settlements throughout India. The 1920 Conference of Superintendents in Calcutta was told that the new idea of “the settlement” was to be “a place where there is as much as possible the idea of community life.”163 It was to be so attractive that the pauper would be willing to remain there without restraints, with the best wards that could be designed and the best medical attention available. The buildings would include a central hall, a hospital for advanced cases, a dispensary where treatment would be given, school buildings for the young people in the asylum, and recreation rooms where people could amuse themselves. There would be work available, beside plantation work, which would receive remuneration: “in this way the inmates would be kept from thinking too much about their miseries, while it would help keep down the cost of maintenance if a good many of their needs were supplied by themselves.”164 In a study of model agricultural colonies in the Netherlands and Indonesia, Albert Schrauwers claims that such utopian spaces (in the service of a form of socialist idealism) were designed “as a means of eliminating pauperism in a wide variety of settings, in radically divergent forms, throughout the early nineteenth century.”165 They sprang from a common regime of value: Whether through the colonies of the Benevolent Society in the Netherlands, Fourier’s phalanxes in France, Robert Owens’ New Harmony, or a variety of religious sects such as the Shakers and the Oneida perfectionists in America, the idiom of charity and pauper relief inspired a spate of intentional communities marked by communal production for the market.166 162. Ibid., 70 –71. 163. Ibid., 70. 164. Ibid. This movement was not only confined to India. In 1906, Colombia and Venezuela developed their own agricultural colonies for leprosy-affected people, and the hospital and agricultural colony of Fontilles in Spain was established in 1907. J. Bernabeu-Mestre and T. Ballester-Artigues, “Disease as a Metaphorical Resource: The Fontilles Philanthropic Initiative in the Fight against Leprosy, 1901 –1932,” Soc. Hist. Med., 2004, 17, 409– 21. 165. Albert Schrauwers, “The ‘Benevolent’ Colonies of Johannes van den Bosch: Continuities in the Administration of Poverty in the Netherlands and Indonesia,” Compar. Stud. Soc. Hist., 2001, 43, 298 – 328, 319. 166. Ibid., 319. 512 Journal of the History of Medicine : Vol. 64, October 2009 He argues that these colonies presented a solution to poverty at a time when global commodity markets were restructuring productive relations around the world.167 In concert with this solution to pauperism, as the asylums that were sponsored by the Mission to Lepers changed their structure, provision for the leprosy-affected inmates to engage in gardening and farming and other productive activities that would enable a degree of self-sufficiency emerged more and more strongly, until the asylum that was set up as an agricultural colony became one of the preferred options. Frank Oldrieve’s grand idea was never completely realized, as in a total of ninety-five institutions in India, both Mission and State, only 13,676 people were institutionalized in 1941, but certain asylums developed into large settlements with many hundreds of inmates.168 By 1941, the largest institutions (over 500) were Purulia, in what was then Bihar, with 805 people; Chandkhuri and Champa in the Central Provinces, with 554 and 550, respectively; Chingleput, in the Madras Presidency with 800; Naini (Allahabad) in the United Provinces with 500; and Dichpali in Hyderabad (the Nizam’s Dominions) with 800 (see Figures 3 and 4). The idea of the agricultural colony for leprosy-affected people never really died out. In 1937, rehabilitated inmates of an asylum had begun to clear virgin forest land in the Central Provinces. They were referred to as “pioneers” and “settlers-to-be.” The intention was to give “ex-patients a stake in the land, a healthy occupation carried on under sympathetic oversight, and such necessary support as may be required until the settler has won for himself resources for times of difficulty.”169 Again in 1942, colonies were recommended as the center of anti-leprosy work for the districts in Orissa and Bihar, by the Indian Council of the British Empire Relief Association, for infectious cases or for those who needed treatment other than that provided by clinics. The colonies could also serve for the cultivation of Hydnocarpus wightiana trees as a source of income, and the Forest and Agricultural departments were to be consulted for suitable sites for colonies with 100 acres of 167. Schrauwers, “Benevolent Colonies,” 320. 168. Government of India, Report on Leprosy and its Control in India, 60. 169. The Mission to Lepers, A Report of the Sixty-Third Year’s Work in India and Burma: September 1936-August 1937, issued by the Indian Auxiliary in India, 4– 5, accessed in Leprosy Mission International Archives, Brentford, London, UK. The Leprosy Asylum in India Fig. 3. “Our Purulia Leper Asylum, Bihar (From a photograph of a model),” in Wellesley C. Bailey, Fifty Years Work for Lepers, 1874 – 1924 (London: Mission to Lepers, 1924), 24. Robertson : 513 514 Journal of the History of Medicine : Vol. 64, October 2009 Fig. 4. “Women at Work in the Rice Fields at Purulia Asylum,” in Rev. Frank Oldrieve, The Mission to Lepers: A Statement of Its Work in India with Financial and other Information (Cuttack: Orissa Mission Press, 1921), opposite page 9. arable land each.170 The feudatory states of Orissa were considered ideal as they possessed “plenty of lands which can be spared for the colonies.”171 The Dewan of Baudh State was instructed to set aside 640 acres, five miles from Baudh. The patients were to produce at least half of their food and to this end they were to be offered “a few acres of land.” They were also to be encouraged to bring their own bullocks and agricultural implements. In this instance, families 170. See John Parascandola, “Chaulmoogra Oil and the Treatment of Leprosy,” Pharm. Hist., 2003, 45, 47 –57; Shubha Pandya, “Ridding the Empire of Leprosy: Sir Leonard Rogers FRS (1868 –1962) and the Oil of Chaulmoogra,” unpublished paper presented at “Health and Medicine in History: East-West Exchange: Third Conference of the Asian Society for History of Medicine,” Jawaharlal Nehru University, New Delhi, 2 –4 November 2006, copy supplied by author; and G. Verghese, “Epidemiological Features of Leprosy in Orissa,” Leprosy in India, 1942, 14, 4, 135. 171. Isaac Santra, Report to the Political Agent, Orissa States, 1105/1 BELRA, 9 April 1946, Orissa State Archives. Robertson : The Leprosy Asylum in India 515 were to be welcomed into the colony. Doing this would also serve medical ends: “This is a good idea as it will make their life comfortable and give us the opportunity to observe the contacts, especially the children. Those who bring their families may be given separate cottages and separate pieces of land.”172 At the 1934 Jubilee Celebrations of the Mission to Lepers in India, messages of gratitude from the residents of leprosy asylums in India were included in the celebration booklet. The message from Purulia, Bihar, was written in Hindi by one of the elders called Bibhabati. Describing the leprosy asylum at Purulia as an ashram, he referred to “the beautiful hospital buildings and the good nursing and doctor’s arrangements” that had grown out of what had been established in 1884.173 An ashram usually means “a place of religious retreat, sanctuary, or hermitage,” and it carries the connotation of spiritual healing.174 Thinking of a leprosy asylum as an ashram complicates this meaning by suggesting a tension between physical and spiritual healing. At a time when a cure for leprosy was so uncertain, an ashram provided a place that could, at the very least, soothe the spirit. When Bibhabati referred to the asylum as an ashram and in the same breath commented on its medical arrangements, he linked both sets of aspirations expressed in the architecture of the leprosy asylum at Purulia: the aspiration both to soothe the spirit and to heal the body. What he does not express are the economic regimes of value which made these asylums possible and within which they developed and changed their identity. The built environment of these asylums was highly structured and was as responsive to economic imperatives as missionary and medical values. While these asylums functioned as shelters for bodies and also as places that would at the very least soothe sufferers, they also provided their inmates with useful occupations. As the architecture of the asylum was changed, the aim also was to provide work. In a manner that fitted perfectly with the values of a Protestant Missionary organization, people with leprosy were 172. Isaac Santra, “Isolation of Leprosy Cases in the Baudh State,” 1105/2, 9 April 1946, Orissa State Archives. 173. Bibhabati, prachina (elder) “A Message from Purulia, Bihar,” trans. Rev. E. B. Sharpe, in Mission to Lepers, Sixty Years of Service 1874 –1934 (London: Mission to Lepers, 1934), 12. 174. See entry for “asylum” in Oxford English Dictionary, 2nd ed. (1989; Oxford, Oxford University Press, 2009), accessed online at http://www.oed.com (accessed 12 May 2009). 516 Journal of the History of Medicine : Vol. 64, October 2009 increasingly offered productive occupations that contributed to the sustenance and self-sufficiency of their asylums. Their labor symbolized their economic and their psychological rehabilitation, and found one form of expression, among others, in the self-sustaining, agriculturally based leprosy settlement. CO N C L U S I O N In conclusion, in order to begin to differentiate the variety of leprosy asylums built throughout the world, this article has devoted its attention to the characteristics of the leprosy asylum in India from 1886 to 1947. There, leprosy asylums were restructured by the activities of the Mission to Lepers in India, and the changes financed out of a tradition of subscription and benevolence that coincided with British and Indian practices. This response was incremental and piecemeal and expressed in the appropriation of land and the development of the built environment. It was enabled by a political situation that opened a space for missionary participation so that spiritual, medical, and economic regimes of value coincided at a time when little could be done to alleviate the suffering of those with leprosy. Consequently, pleasant surroundings, shady trees, sound accommodation, and good ventilation became desirable components of an asylum that would confer physical and psychological benefits for residents. In addition, while it was never necessary forcibly to isolate inmates, men, women, and children were increasingly segregated in such institutions. Gradually, the spaces of the asylum became more highly structured: walls provided seclusion, courtyards were cool and shaded, and buildings were provided to ensure a degree of self-sufficiency. Increasingly, emphasis was placed on the need to occupy the inhabitants so that larger colonies were developed where inmates produced their own food and made their own clothes, rather than sustaining themselves by begging. One form of the leprosy asylum in India found expression in the agricultural colony, which symbolically reincorporated the body damaged by leprosy into the economic world of productive relations. E P I LO G U E This is not the place for an extended analysis of the ways in which leprosy-affected people were both coerced and enabled by leprosy Robertson : The Leprosy Asylum in India 517 asylums, but it is important to realize that the complexities of this process of incorporation do not end in the asylum and cannot be relegated to the past. Today, in India, people whose lives were connected to these asylums, whether as past leprosy sufferers or as the adult offspring of leprosy-affected parents, seem to function as a self-enclosed “caste.” Many still dwell in a multitude of self-formed communities, in villages, clustered around the old colonies.175 It seems to be impossible to disentangle the degree to which colonialism and missionary activity or leprosy, as a socially stigmatized and self-stigmatizing disease, is responsible for this complex process of identity formation. While the structures of colonialism seem less apparent today and the changes wrought by Christianity are still apparent, it is the taint of leprosy that seems to linger longest. 175. These views were formed from three field trips over three years to leprosy colonies in order to meet people still living in or adjacent to colonies in Orissa, Chhattisgarh, Tamil Nadu, Madhya Pradesh, Uttar Pradesh, and Maharashtra.