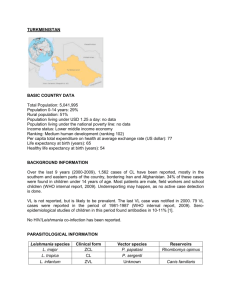
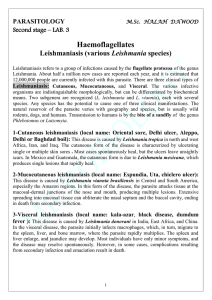
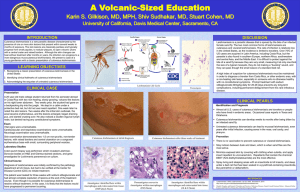
International Journal of Civil Engineering and Technology (IJCIET) Volume 10, Issue 04, April 2019, pp. 302–308, Article ID: IJCIET_10_04_031 Available online at http://www.iaeme.com/ijmet/issues.asp?JType=IJCIET&VType=10&IType=4 ISSN Print: 0976-6308 and ISSN Online: 0976-6316 © IAEME Publication Scopus Indexed CUTANEOUS LEISHMANIASIS IN AIN DFALI PROVINCE, WEST MOROCCO (2006-2015) El Alaoui Zakaria, Amayour Abdelaziz, El Aasri Aziz, EL Kharim Khadija, EL Belghyti Driss Biotechnology and Environment Laboratory (LABEL), Parasitology and Environment Team, Department of Biology, Faculty of Sciences, University, Ibn Tofail, Kenitra, Morocco ABSTRACT In the west of Morocco, between 2006 and 2014. The mean age of patients was 19.8 years with extremes from 6 months to 61 years. The sex ratio was 0.76 M / F. The mean duration of lesions was 1.6 months with extremes of 2 weeks to 10 months. Fall preponderance was noted (41.6%). The most frequent clinical appearance was that of a single ulcero-pulmonary nodule (61%) (71.9%) and was seated on the face (57.5%). Cutaneous leishmaniasis continues to pose a real public health problem in our country. The emergence of severe and resistant forms throughout the world should encourage the multiplication and strengthening of prophylactic measures. Key words: Cutaneous Leishmaniasis, Morocco Cite this Article: El Alaoui Zakaria, Amayour Abdelaziz, El Aasri Aziz, EL Kharim Khadija, EL Belghyti Driss, Cutaneous Leishmaniasis in Ain Dfali province, West Morocco (2006-2015), International Journal of Civil Engineering and Technology 10(4), 2019, pp. 302–308. http://www.iaeme.com/IJCIET/issues.asp?JType=IJCIET&VType=10&IType=4 1. INTRODUCTION Described the first time in Morocco in 1914 by Foley and Vialate (Rhajaoui et al., 2004), cutaneous leishmaniasis (CL) is a public health problem in our country. It is sharply recrudescence, due to a flagellated protozoan belonging to the genus Leishmania. The aim of our work is to describe the epidemiological, clinical and evolutionary characteristics of CL in the Ain Dfali health center. 2. METHODS Through a study conducted between Department of Parasitic Diseases and Ain Dfali Health Center, Provincial Delegation of Health Sidi Kacem, during the period from January 2006 to December 2015, including patients diagnosed with cutaneous leishmaniasis with parasitological and histological confirmation. For each patient were specified: the age, the sex, the geographical origin, the duration of evolution, the clinical aspect, the therapeutic scheme used as well as the evolution under treatment. The statistical analysis was performed using the Exel software (2010 version). http://www.iaeme.com/IJCIET/index.asp 302 editor@iaeme.com Cutaneous Leishmaniasis in Ain Dfali province, West Morocco (2006-2015) 3. FIELD OF STUDY The commune Ain Dfali Figure 1 is limited to the West by commune Sidi Azouz Sidi Kacem province, to the North commune of Rurale Bni Oual province Sidi Kacem, to the common East Ouennan province Ouazzan, and to the South by municipality Rural Mrabih province Sidi Kacem . It covers approximately 234 km2. Its population is 24181 (projection 2009). This area has a high climatic diversity in mountainous areas, the climate is moderate with a hot and dry summer with temperatures ranging from 7 ° C to 47 ° C and average winter rainfall of 500 to 700 mm. Map 1. Field of study 4. RESULT Map 2 Spatial distribution of cases at the province of west morocco. During the studied period, 132 patients were collected. The age of our patients ranged from 6 months to 63 years with an average of 19.5 years. Female predominance was noted (56%) (Figure 2) http://www.iaeme.com/IJCIET/index.asp 303 editor@iaeme.com El Alaoui Zakaria, Amayour Abdelaziz, El Aasri Aziz, EL Kharim Khadija, EL Belghyti Driss 140 120 ffectif 100 80 60 40 20 0 00-09 10 - 19 20-29 30-39 40-49 50-59 ≥ 60 ans TOTAL Masculin 20 27 4 3 1 1 1 57 Féminin 23 24 3 11 6 6 2 75 Total 43 51 7 14 7 7 3 132 Figure 2. Age and Sex Distribution of Cutaneous Leishmaniasis Cases in Ain Dfali (2006-2015). Fall preponderance was noted (41.6%) (Figure 3) 60 50 40 30 20 10 0 Effecctif Figure 3. Distribution by month of diagnosis of cutaneous leishmaniasis cases in Ain Dfali (2006-2015) The average consultation time was 1.6 months (2 weeks -10 months) (Figure 4). 100 Effectif 80 0-1 mois 60 1-2mois 40 2-3mois 4+ 20 0 Délai de consultation Figure 4. Distribution according to the consultation time of cutaneous leishmaniasis cases in Ain Dfali (2006-2015) http://www.iaeme.com/IJCIET/index.asp 304 editor@iaeme.com Cutaneous Leishmaniasis in Ain Dfali province, West Morocco (2006-2015) Lesions were unique in 71.9% with an average of 1.39 lesions per patient (Figure 5). Unique Deux Trois Quatre et plus Figure 5. Distribution by number of lesions of cutaneous leishmaniasis cases in Ain Dfali (20062015) The lesions sitting on the face in 71.9% of the cases, on the upper limbs in 14.39%, on the lower limbs in 13.63% of the cases (Figure 6). 35 30 25 20 15 10 5 0 nez nombre 32 bras pied paup main joue front oreill lévre iére e 2 18 6 17 19 24 9 5 Figure 6. Distribution by site of lesions of cutaneous leishmaniasis cases in Ain Dfali (2006-2015) The clinical features found were 48% ulcero-crust (Photo A), 34% papulo-nodular form (Photo B), 11% erythematous-squamous form (Photo C) and 7% unspecified (Figure 7). Non spécifié 7% érythémato-squameuse 11% papulo-nodulaire 34% ulcéro-croûteuse 48% 0% 10% 20% 30% 40% 50% 60% pourcentage Figure 7. Distribution by lesion aspects of cutaneous leishmaniasis cases in Ain Dfali (2006-2015) http://www.iaeme.com/IJCIET/index.asp 305 editor@iaeme.com El Alaoui Zakaria, Amayour Abdelaziz, El Aasri Aziz, EL Kharim Khadija, EL Belghyti Driss 5. DISCUSSION Cutaneous leishmaniasis has a circum-terrestrial geographical area. According to the WHO, the population at risk of leishmaniasis is estimated at 350 million people (WHO, 2010). The global incidence of LC, in all clinical forms, is between 1 and 1.5 million / year. More than 90% of LF cases come from Afghanistan, Iran, Saudi Arabia and Syria for the old world, Brazil and Peru for the new world (Momeni, 1994). Morocco is an endemic country of the LC. Infection occurs in three noso-geographic forms: the zoonotic LC to Leishmania major in the south, the anthroponotic LC to Leishmania tropica in the center with emergence of new outbreaks in the north and the sporadic LC to Leishmania infantum in the north whose first Moroccan case has revealed in 1996 (Rhajaoui 2004, Guessous 1994, Chihab 1999). Between 2007 and 2011, 27457 cases of CL were identified (Ministry of Health Morocco, 2012). The analysis of the epidemiological data revealed a control of the LC profile at L. major in the majority of the old foci with a reactivation observed during the year 2010. Moreover, the LC to L. tropica has experienced outbreaks epidemic (El Assri, 2016). LC affects all ages and the child can be exposed to the disease in the first months of life (6 -10). We note a predominant impairment of school-aged children, especially those over ten years of age (38.6% of cases). The distribution of LC by sex is variously appreciated in the literature (EL Aasri, 2015). There does not seem to be any significant difference in our series. Clinically, our results are superimposable to those of the literature. The predominance of the ulcero-crustal form in our series, noted also in the other studies carried out in North Africa, is explained by the frequency of LC to L. Major (Guessous, 1999). The latter form is characterized by multiple lesions, localization at the level of the regions discovered especially at the level of face and limbs as well as the short duration of evolution (Aoun, 2012). The long consultation time found in our work is explained by the slowly insidious, indolent and benign nature of the lesions. In our context, the diagnosis is often made in autumn or winter away from the contamination that occurred in summer (after a stay in endemic area). Numerous clinical presentations are possible during LC, the impetigo, warty, vegetative, lupoidal, pseudotumoral, psoriasiform, lichenified, ulcerous, echtymatous, lymphangitic, abortive, sporotrichoid and nodular forms. This clinical polymorphism does not only depend on the genetic characteristics of the parasite, but also on the immunological status of the host. Indeed, the balance of functional phenotypes of CD4 T lymphocytes plays an important role in the determinism of this affection; schematically the Th1-type response corresponds to a benign localized lesion, the Th2 response involves extensive severe injury. Leishmania-HIV co-infection is currently considered an emerging disease, especially in southern Europe (Dedet, 2000). WHO estimates that 1.5 to 9% of AIDS patients have visceral leishmaniasis (Momni, 1994). The cutaneous form is more and more described during HIV infection (Durant, 1998). The diagnosis of LC is evoked clinically, confirmation is based on the detection of the parasite. The direct examination on the smear or the colored puncture with the MGG seems to be the best examination for the diagnosis because economic, easy, fast and without danger. However, it lacks sensitivity. Special Environment (NNN) culture improves the sensitivity of parasitological examination by 16% (Belhadej 2005, Grevlink 2003)]. Pathological examination also contributes to the diagnosis. The enzymatic identification of species is a reference technique, reserved for specialized laboratories, as well as for PCR, the results of which seem very promising (98% sensitivity versus 80% with conventional diagnostic means) (Chergui, 2003; Matsumoto, 1999). This makes discuss the interest of this new method in our http://www.iaeme.com/IJCIET/index.asp 306 editor@iaeme.com Cutaneous Leishmaniasis in Ain Dfali province, West Morocco (2006-2015) context in front of an evocative clinical presentation without isolation of the parasite with the usual techniques. In our experience other arguments have been taken into account: the notion of stay in an endemic zone, the slow evolution and the non-response to other therapies (antibiotics, antimycotics). The therapy of leishmaniasis has only changed for many years. Glucantime is the standard treatment for cutaneous leishmaniases (Buffet, 1994). However, this treatment exposes many side effects, and resistance is increasingly reported in several countries. For single or infrequent LC, intralesional infiltration has proved its effectiveness (100% success in our series) The results obtained in our patients are similar to those of the literature, with an efficacy of Glucantime without general adverse effects nor pigmented scars. Many products have been tried in the literature (amphotericin B, fluconazole, disulone, rifampicin), as well as the laser, bleomycin intra-lesional. Currently, hopes are placed in allopurinol, aminosidine sulfate (paromomycin) or triazoles, or even in some hydroxynaphthoquinones, such as atovaquone. Immunostimulation with interferon has been the subject of convincing clinical trials that have unfortunately no future (Buffet, 1994, Morizot, 2007). 6. CONCLUSION Cutaneous leishmaniasis continues to pose a real public health problem in our country. The emergence of severe and resistant forms throughout the world should encourage the multiplication and reinforcement of prophylactic measures through the fight against the reservoirs and vectors of the parasite. Therapeutic optimization, standardized protocol monitoring and consensual repository remain necessary. REFERENCES [1] Bettaieb J, Siala E, & Ben Abdallah R (2012). Caractérisation comparative des trois formes de leishmaniose cutanéo endémiques en Tunisie. Ann Dermatol Venereol; 139(67):452–458. [2] Belhadj S, & Chaker E (2005). Place de la culture dans le diagnostic parasitologique des leishmanioses viscérales et cutanées. Rev Franc Labo. (369): 41–5. [3] Buffet P, Caumes E, & Gentilini M. (1994). Traitement des leishmanioses cutanées localisées. Ann Dermatol. Vénéréol. 121(6-7):503–11. [4] Chargui N, Haouas N, & Babba H. (2003). Apport de la PCR dans le diagnostic de la LC (203 cas) Ann Dermatol Venereol; 130:4S53. [5] Chiheb S, Guessous Idrissi N & Hamdani A (1999). Leishmaniose cutanée à leishmania tropica dans un foyer émergent au nord du Maroc: nouvelles formes cliniques. Ann Dermatol Venereol; 126(5):419–22. [6] Dedet JP, & Pratlong F (2000). Taxonomie des leishmania et distrubition géographique des leishmanioses. Ann Dermatol Venereol;127(4):421–4. [7] Durand I, Beylot-Barry M, Weill FX, Doutre MS, & Beylot C (1998). Leishmaniose cutanée diffuse révélatrice d'une infection par le virus de l'immunodéficience humaine. Ann Dermatol Venereol; 125(4): 268–70. [8] El Aasri A, El Alaoui Zakaria, EL Kharim Khadija & EL Blghyti Driss (2016). Profil Epidemiologique De La Leishmaniose Cutanée Dans La Region Du Gharb- Maroc De 2006 À 2014 . European Scientific Journal; 247-250 [9] Grevelink SA, & Lerner EA. (1996). Leishmaniasis. J Am Dermatol Acad. 34(2 pt 1):257–72. http://www.iaeme.com/IJCIET/index.asp 307 editor@iaeme.com El Alaoui Zakaria, Amayour Abdelaziz, El Aasri Aziz, EL Kharim Khadija, EL Belghyti Driss [10] Guessous N, Riyad M, & Chiheb S. (1996). Les leishmanioses au Maroc: Actualités épidémiologiques et diagnostiques. Bul SMSM. 7:31–35. [11] Matsumoto T. & Mimori T. (1999). Comparison of PCR results using scarpe/exsudate and biopsy samples for diagnosis of cutaneous leishmaniasis. Trans R Soc Trop Med Hyg. 93(6):606–7. [12] Ministère de la Santé (2012). Bulletin épidémiologique. Maroc: Avril. Ministère de la santé. Direction de l’épidémiologie et de lutte contre les maladies. [13] Momeni AZ, & Javaheri MA. (1994). Clinical picture of cutaneous leishmaniasis in Asfahan. Int J Dermatol;33(4):260–5. [14] Morizot G, Del Giudice P, Caumes E, Laffitte E, Marty P, & Dupuy A. (2007). Healing of old world cutaneous leishmaniasis in travelers treated with fluconazole: drug effect or spontaneous evolution. Am J Trop Med Hyg. 76(1):48–52. http://www.iaeme.com/IJCIET/index.asp 308 editor@iaeme.com