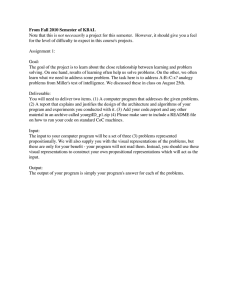
ORIGINAL ARTICLE Mentalizing in Self vs. Parent Representations and Working Models of Parents as Risk and Protective Factors From Distress and Eating Disorders Lily Rothschild-Yakar, PhD,*Þ Ariela Waniel, PhD,*þ and Daniel Stein, MD*§ Abstract: This study examined whether low developmental level of mentalization and symbolization, manifested as low ability to represent and reflect on mental states of the self and parents as well as malevolent working models of parents, may be risk factors in the genesis of eating disorders (EDs). We examined 71 female adolescent inpatients with ED and 45 controls without ED using the Object Representation Inventory and self-report measures assessing emotional distress and ED symptoms. The results indicated that the patients with ED presented with a significantly lower level of mentalization and symbolization and with more malevolent working models of their parents in comparison with the controls without ED. A more benevolent parental representation, specifically with the father, combined with better mentalization abilities, was found to indirectly predict lower ED symptoms, via the reduction of distress levels. These findings suggest that adequate mentalization and benevolent working models of parents may serve as a protective factor reducing the level of ED symptoms. Key Words: Mentalization, reflective function, symbolization, working models of parents, eating disorders. (J Nerv Ment Dis 2013;201: 510Y518) E ating disorders (EDs) reflect complex, interdependent, multidimensional causalities. Some studies ascribe the genesis of EDs as entailing a combination of psychobiological developmental deficiency manifested by low interoceptive awareness (e.g., low ability to identify and process bodily and emotional states), inaccuracy in concept development, deficient social competence, and lack of individuation (Bruch, 1988; Fassino et al., 2004). Other studies go further and tie the concrete somatic ED symptoms to a developmental deficiency in the cognitive-affective arenas of symbolization (McDougall, 1989) and mentalization (Rothschild-Yakar et al., 2010; Skårderud, 2007). The ability to put words and images to somatic experience, to transform physiological and somatic experiences into symbolic mental representations, in the service of creating psychological meaning related to these experiences was termed as the ability for mentalization or reflective functioning by Fonagy and his colleagues (Fonagy and Target, 1996; Fonagy et al., 1998, 2002). Fonagy’s use of the term combines the psychoanalytic idea of symbolization with the socialcognitive concept of ‘‘theory of mind.’’ MENTALIZATION AND REFLECTIVE FUNCTIONING Mentalization involves both a self-reflective and an interpersonal component. It refers to the capacity to reflect and interpret one’s own behavior, as well as the behaviors of others, as caused by intentional internal mental states such as thoughts, feelings, and beliefs. A well-developed ability to form and use mature mental representations *Safra Children’s Hospital, Sheba Medical Center, Tel Hashomer, Israel; †Department of Psychology, University of Haifa, Haifa, Israel; ‡Department of Education, Bar Ilan University, Ramat Gan, Israel; and §Sackler Faculty of Medicine, Tel-Aviv University, Tel Aviv, Israel. Send reprint requests to Lily Rothschild-Yakar, PhD, Department of Psychology, University of Haifa, Haifa 31905, Israel. E-mail: Lilyrot@yahoo.com. Copyright * 2013 by Lippincott Williams & Wilkins ISSN: 0022-3018/13/20106Y0510 DOI: 10.1097/NMD.0b013e3182948316 510 www.jonmd.com of the self and others enables people to think about and cope with external and internal stressors and to form good interpersonal relationships (Fonagy et al., 1998). Fixation in primitive modes of representing experience causes difficulties in identifying and acknowledging internal states, correctly perceiving and interpreting interpersonal relations, and differentiating reality from fantasy and physical from psychic reality (Fonagy et al., 2002). With regard to EDs, impaired mentalization can be conceptualized as reflecting primitive modes of experience, in which psychic reality is poorly integrated and ideas and even words mean very little. In such a condition, the body and ED symptoms may serve as concrete means to represent and enact feelings and thoughts as well as to regulate drives and emotions (Bleiberg, 2001). The few studies that have previously investigated mentalization ability in patients with ED have found low levels of reflective functioning, both in patients (Fonagy and Target, 1996; Rothschild-Yakar et al., 2010; Ward et al., 2001) and in their mothers (Ward et al., 2001). In anorexia nervosa (AN), this fixation in primitive modes of experience was also manifested as elevated use of concrete body metaphors and an inability to distinguish between a metaphor and the phenomenon it represents (Skårderud, 2007), suggesting a cognitive-developmental deficiency in symbolization. A major factor facilitating children’s attainment of the ability to mentalize is associated with the caregiver’s mirroring of the infant’s subjective experiences in a secure attachment relationship (Fonagy et al., 2002). Children’s representations of themselves and of their inner experiences are based on their parents’ capacity to represent and imagine their own minds, thus providing a secure base for the child to develop mentalization and symbolic abilities (Meins et al., 1998; Slade, 2005; Taylor, 2010). In contrast, children who lack secure attachment relationships and, thereby, attuned mirroring of their affective states cannot create representations of those experiences, likely placing them at a greater risk for remaining fixated in primitive modes for representing subjectivity (Fonagy et al., 2002). Several studies have shown that patients with AN or bulimia nervosa (BN) have a history of insecure attachment relationships (Troisi et al., 2006; Ward et al., 2001). Social-cognition research on emotion recognition has further shown that individuals with EDs show impairment in the ability to identify their own emotions and to represent and be aware of others’ emotional experiences (e.g., Bydlowski et al., 2005). Thus, at times of developmental stress, adolescents with a history of insecure attachment, lacking representations of their inner experiences, may find themselves unable to recognize and conceptualize their own subjective experiences at the level of verbal thought. They may therefore misinterpret emotional distress as a concrete bodily distress that can be relieved mainly by an excessive preoccupation with eating, appearance, or exercise (Bleiberg, 2001; McDougall, 1989). These data further highlight the theory that developed mentalization is related to the ability to form and use a developed self and other representations (Meins et al., 1998; Skårderud, 2007). SELF AND OBJECT REPRESENTATIONS The term object representations refers to the internal models of the self and others and the relations of the self with others. These The Journal of Nervous and Mental Disease & Volume 201, Number 6, June 2013 Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. The Journal of Nervous and Mental Disease & Volume 201, Number 6, June 2013 Mentalization in ED internal models are expressions of the subjective processing of interpersonal experiences and interactions, which, in turn, plays an important role in adequately interpreting behavior, conflicts, and emotional and cognitive processes in one’s relationships with others (Blatt et al., 1997). From a cognitive psychology perspective, these representations are termed schemas and are assumed to influence social information processing in a top-down process, where previous knowledge affects the perception and organization of new social information and also plays a role in regulating behavior and decision making (Dodge and Rabiner, 2004). Blatt et al. (1993, 1992, 1979) proposed a multidimensional approach for assessing the mental representations of the self and others, in which they incorporated cognitive-developmental and affective aspects. From a cognitive-developmental perspective, the development of object representations is hypothesized as progressing from early forms on the basis of the object’s actions and need-gratifying functions to higher differentiated and symbolic object representations. This developmental path can be conceptualized according to the terms of Lieberman (2007), distinguishing between internally focused cognitions, referring to mental processes that focus on one’s own or another’s inner psychological worlds, such as thoughts and feelings, and externally focused cognitions, referring to mental processes that focus on one’s own or another’s physical and visible features and actions. This distinction has been supported by findings in social-cognitive neuroscience, in which brain imaging showed that representing psychological traits (internal) were associated with the activation of brain areas other than those activated in response to descriptions of observable behavior (external). The affective aspect of representations is examined by assessing the quality of representations of parents as attachment models. Parents may be described along several factors such as benevolent, punitive, and striving. For example, the benevolence factor measured the affective tone attributed to the parents such as being affectionate and nurturing (Blatt et al., 1992). In a summary of studies, Blatt et al. (1997) suggested that the developmental level of descriptions given by young adults of their parents was related to their quality of attachment style. For example, securely attached individuals presented more developmentally mature and symbolic representations of significant others than did their insecurely attached counterparts. This data is in line with the suggestions raised by Fonagy et al. (Fonagy and Target, 1996; Fonagy et al., 1998, 2002) proposing that developed mentalization ability is related to secure attachment relationships. the self versus mentalizing about others. In healthy development, these processes are connected, but these also involve different processes aiming to create a differentiated experience of me and not-me (Fonagy and Luyten, 2009). Moreover, the ORI allowed for assessment of the quality of working models of parents as attachment figures. As previously discussed, attachment and mentalization ability are interrelated, and both constructs have been linked to the ability to regulate affects (Taylor, 2010). In the present study, our first aim was to examine the reflective-symbolization levels in three subtypes of ED patients compared with controls without ED, as well as the affective quality of representations of parents. We hypothesized that the inpatients of all three subtypesVAN-B/P, BN, and restricting type of AN (AN-R)Vwould provide less developmentally mature descriptions of the self and of the parents with respect to the ability to reflect on internal symbolic attributes and that the affective quality of parental representations would be more malevolent and punitive compared with the controls without ED. Because the patients with AN-B/P and BN symptoms may present with more pathological personality disorders than the patients with AN-R and may exhibit more deficient impulse and affect regulation as well as less integrated perceptions of themselves and others (Klump et al., 2000), we hypothesized that the patients with AN-R would show better reflective symbolization capacities and less malevolent representations of their parents than both the patients with AN-B/P and those with BN. Inasmuch as several studies ascribe the development of ED symptoms to a deficient ability to represent, identify, and cope with emotional distress (Bleiberg, 2001; Kaye et al., 2004), our second aim was to explore how the level of mentalization and the quality of parental representations would associate with the patients’ level of distress and severity of ED symptoms. We hypothesized that a higher ability to reflect on internal symbolic characteristics of the self and parents and secure working models of the parents would serve directly to attenuate ED symptoms and indirectly as a resource for regulating distress and, thus, as a protective factor from turning to ED symptoms. To the best of our knowledge, no previous studies have examined the developmental ability to reflect on internal symbolic characteristics of the self and parents, as well as the quality of the working models provided in parental descriptions, as potential protective factors in the development of an ED. STUDY AIMS AND HYPOTHESES The research sample comprised a total of 116 female adolescents in two groups, with and without an ED. The experimental group consisted of 71 female Israeli adolescent inpatients aged 14 to 19 years who were hospitalized in an inpatient ED department located in a general hospital. All patients met the criteria for a full-blown ED diagnosis based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994). The patients were diagnosed with one of three ED subtypes: AN-R, 31; AN-B/P, 18; and BN, 22. Patients were excluded from the study if they had a lifetime or current diagnosis of bipolar disorder, schizophrenic spectrum disorder, organic brain syndrome, mental retardation, or any physical disorder with a potential to affect appetite or weight (e.g., thyroid disorders or diabetes mellitus). An analysis of the prevalence of comorbid DSM-IV axis I psychiatric diagnoses (assessed by the Structured Clinical Interview for DSM-IV Axis I DisordersYPatient Edition [SCID-I/P] version 2.0; First et al., 1995) revealed that 41 (57.75%) of the 71 patients with ED were diagnosed with a comorbid depressive disorder; and 20 (28.17%), with a comorbid obsessive-compulsive disorder. The control sample comprised 45 female high school students aged 14 to 19 years who volunteered to participate in this study. All of The aim of the present study was to assess mentalization capacities and the affective quality of internal working models of parents in patients with ED. In our research group’s previous study using other measures, including the Reflective Function (RF) Scale (Fonagy et al., 1998), we found that patients with bingeing/purging type AN (AN-B/P) demonstrated significantly lower mentalization levels and reported in a self-report measure a lower quality of current relationships with parents compared with controls without ED (Rothschild-Yakar et al., 2010). In the present study, we aimed to expand our inquiry to examine three subgroups of inpatients with ED. We also implemented a multidimensional assessment measure to examine mentalization level in line with Choi-Kain and Gunderson’s (2008) assertion that mentalization’s broad and multifaceted nature requires the use of a multidimensional approach and allows for its measurement through related constructs. Thus, in the current study, we administered the multidimensional Object Representation Inventory (ORI; Blatt et al., 1993, 1992, 1979) to examine the level of symbolization, which overlaps conceptually with cognitive aspects of mentalizing. The use of the ORI also enabled separate assessment of mentalization ability while processing representations about * 2013 Lippincott Williams & Wilkins METHOD Participants www.jonmd.com Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 511 Rothschild-Yakar et al. The Journal of Nervous and Mental Disease these students passed a screening process involving a brief interview and a questionnaire to exclude potential participants with ED symptoms or a lifetime or current psychiatric or medical illness. A comparison of the four study groups’ demographic and clinical characteristics revealed no significant differences for the percentage of mothers with an academic education (AN-R, 48.39%; AN-B/P, 61.11%; BN, 68.18%; nonpatients, 40.00%), or for the percentage of fathers with an academic education (AN-R, 64.52%; AN-B/P, 55.56%; BN, 63.64%; nonpatients, 42.22%). A significant difference did emerge for age, where the patients with AN-R were younger than the other groups (mean T SD, AN-R, 15.19 T 1.77; AN-B/P, 16.44 T 1.77; BN, 16.22 T 1.19; nonpatients, 16.11 T 1.35; F = 4.17; p G 0.01). As expected, a significant between-group difference emerged for body mass index, where the patients with BN and the controls presented a significantly higher index than the patients with AN-R and AN-B/P (mean T SD, AN-R, 15.52 T 1.62; AN-B/P, 16.00 T 1.54; BN, 20.52 T 2.23; nonpatients, 20.84 T 2.04; F(4,111) = 52.72; p G 0.001; G = 0.60). Measures This study included two independent variables (level of mentalization in the self and parent representations and affective quality of representation of parents) and two dependent variables (ED symptoms and emotional distress symptoms). Independent Variables The ORI (Blatt et al., 1993, 1992, 1979) was designed for multidimensional assessment of object representations (of the self and others), examining both cognitive-developmental and affective aspects. In the current study, using the Assessment of Self measure (Blatt et al., 1993), the participants were asked to openly and spontaneously describe themselves. Using the Assessment of Qualitative and Structural Dimensions of Object Representations measure (Blatt et al., 1992), the participants were asked to openly and spontaneously describe their mother and their father. The cognitive component of the ORI, deriving from cognitive developmental theory, enabled examination of the participants’ maturity level of reflective symbolization (mentalization), measured separately for the self and for the mother and the father. The ORI qualitative (content) scales of parental representations, deriving from attachment and psychoanalytic theory, assess the affective quality of parents’ representations. Previous interrater reliabilities for cognitive-developmental and qualitative-affective scores were good (Blatt et al., 1992, 1979). The empirical validity of the ORI has been supported; for example, low symbolization level and low benevolence level of parents’ representations were found to be associated with somatoform symptoms and stress in patients in primary care (Porcerelli et al., 2006). In the present study, the narratives provided by the participants in response to the ORI were analyzed by two coders, who were trained by the second author and were blinded to the participants’ group (ED and non-ED) and subtype (AN-R, BN, and AN-B/P) and to the other coder’s scoring. Each coder scored 40 protocols independently, 15 protocols from the control group and 25 from the ED inpatient group. The coders analyzed each narrative twice, once for the Conceptual Level (CL) scale examining the reflective symbolization level and once for the content subscales. Intraclass correlation coefficients indicated fair to excellent interrater reliability for the CL scales (0.88 for selfdescription and 0.80 for parents’ descriptions) and for the content subscales (ranging from 0.72 to 0.90). Cognitive-Developmental Aspects: Maturity of Reflective Symbolization (Mentalization) in the Self and Parent Representations. In this study, we used the CL subscales of the object (Blatt et al., 1992) and self-representation (Blatt et al., 1993) to examine the reflective symbolization level. There is an ORI subscale of reflective functioning designed only for the self-representation scales (Blatt et al., 1993). We 512 www.jonmd.com & Volume 201, Number 6, June 2013 decided to use the CL scale because it enables the assessment of the self and also others’ representations. Moreover, high correlation (0.79) was found between the self-reflective subscale and the CL scale (Blatt et al., 1993). The participants’ developmental level of reflective symbolization was coded separately for the self and for the mother and the father on the CL’s 9-point ordinal scale, ranging from 1 (developmentally immature representations) to 9 (developmentally mature representations). Level 1 (sensorimotor-preoperational) primarily reflects descriptions of parents’ activity in reference to the gratification or frustration they provide, and the parental object is not experienced as separated from the respondent. Level 3 (concrete-perceptual) indicates that the self and the object are experienced as separate. Descriptions articulate properties in concrete physical terms without ascribing any mental activity. Level 5 (external iconic) focuses on specific part properties of the self and the parents, often in terms of their functional activities. Level 7 (internal iconic) involves description of internal states, for example, what the objects think and feel rather than their activities. Level 9 (conceptual) refers to complex descriptions combining external and internal characteristics of the self and parents. Scores of 2, 4, 6, and 8 are used when criteria for a particular level are not fully achieved. The Pearson’s correlation between the self, mother, and father scale scores showed only moderate correlations (between mother and father, r = 0.62, p G 0.001; between the self and mother, r = 0.52, p G 0.001; between the self and father, r = 0.39, p G 0.001). Thus, we analyzed the reflective symbolization level of the representations separately for the self, mother, and father. Affective Aspects: Quality of Representations of Parents (Attachment Models). The qualitative aspects of parental representations were assessed from the ORI narratives using content analysis by the Qualitative Dimensions of Parental Representations for the three factors identified by Blatt et al. (1992): benevolent, punitive, and striving representations. In the present study, we examined only the benevolence factor because 112 participants related to themes of maternal benevolence and 109 related to themes of paternal benevolence, but only 26 related to themes of maternal punitive attributes; 37, to paternal punitive attributes; 43, to maternal strivings; and 40, to paternal strivings. Low benevolence scores indicated that the respondent viewed the father or the mother as malevolent, threatening, abusive, and abandoning (e.g., ‘‘My parents don’t get along. My father is always drinking and sometimes beats my mother up’’). High scores showed that the individual holds a spectrum of supportive and beneficial emotional attributions of that parent (e.g., ‘‘My mother is a loving mother. We are very close, turn to each other for help’’). The Pearson’s correlations calculated between the mothers’ and fathers’ benevolence subscales revealed only a moderate correlation, r = 0.31, p G 0.001; hence, we used the mother and the father scores separately. As previously discussed, mentalization ability and attachment are interrelated. The Pearson’s correlations between the different CL scales (the self, mother, and father) and the benevolence subscales (mother and father) were tested, both within each group (ED and nonED) and across groups (see Table 1). The data show that, across all participants and within the nonpatient group, consistency emerged in the level of reflective symbolization, evident in the significant correlations for the conceptual scores (CLs) of all three representations. In the patients with ED, by contrast, a significant correlation emerged only between the CL for the mother and the CL levels for the self and the father but not between the CL of the father and the self. Across all participants, the affective quality of the mother’s representation did not correlate significantly with the reflective symbolization level of representations, whereas the quality of representation of the father did, indicating that a higher level of paternal benevolence correlated positively with the CL level of all three representations. Positive * 2013 Lippincott Williams & Wilkins Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. The Journal of Nervous and Mental Disease & Volume 201, Number 6, June 2013 Mentalization in ED TABLE 1. Pearson’s Correlations for the ORI Conceptual and Benevolence Scales for Representations of the Self and Parents Quality of Representation (Benevolent Content) Reflective Symbolization (CL) Scale Mother Father CL Self CL Mother benevolencea Father benevolenceb 0.53** 0.40** 0.01 0.20 Father CL Self CL Mother benevolence Father benevolencec 0.64*** 0.55*** 0.10 0.16 Father CL Self CL Mother benevolenced Father benevolencee 0.62*** 0.52*** 0.15 0.35*** Father Self Patients with ED (n = 71) 1.00 0.22 0.22 1.00 0.04 0.11 0.30* 0.08 Nonpatients (n = 45) 1.00 0.51** 0.51** 1.00 j0.11 j0.10 0.00 0.12 Total sample (N = 116) 1.00 0.40*** 0.40*** 1.00 0.12 0.15 0.38*** 0.25** Mother Father 0.04 0.11 1.00 0.07 0.30* 0.08 0.07 1.00 j0.11 j0.10 1.00 0.42** 0.00 0.12 0.42** 1.00 0.12 0.15 1.00 0.31** 0.38*** 0.25** 0.31** 1.00 a n = 67. n = 66. c n = 43. d n = 112. e n = 109. *p G 0.05. **p G 0.01. ***p G 0.001. b correlations also emerged in the patients with ED between paternal benevolence and CL level for fathers. Dependent Variables ED Symptoms. The Eating Disorders InventoryY2 (EDI-2; Garner, 1991) is a self-report measure assessing core ED-related symptomatic and personality attributes. It includes 91 items grouped into 11 subscales, each rated on a 7-point Likert scale ranging from never (0) to always (6). We used 2 of the 11 subscales. The 7-item drive for thinness (DT) subscale assessed excessive concern with dieting, pursuit of thinness, and preoccupation with weight. The 9-item body dissatisfaction subscale (BD) assessed dissatisfaction with weight and physical appearance. The Pearson’s correlations among the two EDI-2 subscales revealed a high significant correlation between the EDI-2YDT and EDI2YBD subscales (r = 0.85, p G 0.001). Thus, we constructed a combined self-report ED measure (SR-ED), comprising the standardized scores of the DT and BD subscales to examine the second hypothesis (Cronbach’s > = 0.90 for this combined measure). Emotional Distress Measures. We collected self-report data on the participants’ state anxiety and depressive symptoms. Self-reported state anxiety. We used the 20-item state anxiety subscale of the State-Trait Anxiety Inventory (STAI-S; Spielberger et al., 1970) to measure the participants’ self-reported anxiety at the time of evaluation. The participants rated items on a 4-point scale ranging from never (1) to very much (4). Self-reported depressive symptoms. The 21-item self-reported Beck Depression Inventory (BDI; Beck et al., 1961) was used to measure the severity of depressive symptoms. The participants rated items on a 4-point scale ranging from rarely (1) to often (4). The Pearson’s correlation between the two distress measures was 0.80. Thus, a combined self-report emotional distress variable (SR-distress) was constructed, comprising the standardized scores of * 2013 Lippincott Williams & Wilkins the BDI and STAI-S subscales to examine the second hypothesis (Cronbach’s > = 0.89 for this combined measure). Procedure All participants, and their parents in the case of minors younger than 18 years, gave their written informed consent to participate in this study. This study was approved by the Ethics (Helsinki) Committee of the Sheba Medical Center. Two experienced child and adolescent psychiatrists independently interviewed the inpatients. ED diagnosis was established using the Eating Disorders Family History Interview (Strober, 1987) and the SCID-I/P version 2.0 within 14 days of admission, when the patients were considered medically stable as determined by routine comprehensive physical, neurological, and laboratory examinations. For the control group, a first session was held individually to screen out potential participants with ED symptoms. In this session, the control participants completed the self-reported Eating Attitude Test (EAT-26; Garner et al., 1982) and reported their weight and height. Only those 45 control participants with no pathological scores (i.e., G20) on the EAT-26 and with a normal reported body mass index (body weight divided by height squared) of at least 18.5 kg/m2 continued with the study procedure, as administered to the ED group. The self-report questionnaires and the ORI were administered individually by trained licensed clinical psychologists and interns in clinical psychology, who were blinded to the patients’ self-report outcomes. RESULTS Before examining the study hypotheses, we determined the extent to which the study groups (inpatients with ED and controls without ED) differed in ED symptoms (EDI-2) and emotional distress symptoms (STAI-S and BDI). Thus, we conducted two analyses of covariance (ANCOVAs) on the self-report EDI-2 scales (EDI2YDT and EDI-2YBD) and two ANCOVAs for the emotional distress www.jonmd.com Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 513 The Journal of Nervous and Mental Disease Rothschild-Yakar et al. measures, with age as a covariate. The univariate ANCOVAs and the significant between-group contrasts in ED and distress symptoms according to post hoc Tukey’s tests are presented in Table 2. The analyses revealed, as expected, a significant between-group difference in ED and in emotional distress symptoms. Tukey-Kramer’s post hoc comparisons of the four groups (AN-R, BN, AN-B/P, and non-ED) showed that the significant between-group differences were caused by the nonpatient group’s significantly lower scores on the EDI-2YDT and EDI-2YBD subscales and lower scores on the reports of distress levels, in comparison with each of the three ED subgroups ( p G 0.001). No significant contrast emerged between any of the ED subgroups (see Table 2). Reflective Symbolization Level and Parents’ Benevolence in the Three ED Subtypes and Controls The first hypothesis, asserting that the reflective symbolization level of the representations and the level of benevolence of parents’ representations would be lower among the ED groups than the controls, was examined with a between-group multivariate analysis of variance for the CL scales of the ORI and with two separate betweengroup ANCOVAS for the benevolence scales, with age as a covariate. The univariate ANCOVAs and the significant between-group contrasts revealed by the Tukey’s test are presented in Table 2. As expected, a significant between-group difference was found, in which all three ED groups showed lower levels of reflective symbolization in their representations of the self and of their parents, F(9,265) = 3.57, p G 0.001, and also ascribed their parental representations (mother and father) with a lower level of benevolence. Tukey-Kramer’s post hoc comparisons of the four groups showed that the reflective symbolization level in the description of both parents in the nonpatient group was significantly higher than in each of the ED subgroups. The reflective symbolization level for mothers revealed contrasts with AN-R and BN at p G 0.01, and the contrast with AN-B/P was p G 0.05; the reflective symbolization level for fathers revealed contrasts with AN-B/P and BN at p G 0.05 and a contrast with AN-R at p G 0.01. The reflective symbolization level for the self revealed significant contrasts with patients with AN-R & Volume 201, Number 6, June 2013 and BN ( p G 0.01). No significant contrasts emerged between the ED subgroups. Because of the lack of differences between the ED subgroups in most dependent and independent variables, we combined all ED subgroups into one group of patients with ED when examining the second study hypothesis. Reflective Symbolization Level and Parents’ Benevolence as Predictors of Emotional Distress and ED Symptoms Before examining the research hypothesis concerning the predictive value of the independent research variables, we computed the Pearson’s correlations between the independent variables (the ORI’s CL scales for the self, mother, and father and the benevolence subscales for mother and father) and the dependent variables (SR-ED and SR-distress measures). These correlations were tested both within each group separately and across the research and control groups (see Table 3). As expected, the analyses across all participants yielded significant negative correlations between the SR-ED symptoms and the benevolence level attributed to both parents. Nonetheless, a negative correlation between SR-ED and the cognitive-developmental measures (ORI-CL) was found only for representations of the mother but not for representations of the father or the self. These data showed that the higher symbolization level evident in mothers’ descriptions and the higher benevolence ascribed to both parents were correlated with lower ED symptoms. Self-reported emotional distress symptoms (SR-distress) revealed significant negative correlations with the reflective symbolization representations and the benevolence scales of both parents but not with the CL score for self-representation (see Table 3). A significant positive correlation also emerged between the SR-distress and SR-ED symptoms, indicating that a higher emotional distress level was correlated with more ED symptoms. Path analysis was conducted for all four groups using SAS’s Proc CALIS (SAS, 2004), to examine the second research hypothesis regarding the direct contribution of the ORI to the explained between-group variance in ED-related symptoms and the indirect effect of the ORI on ED symptoms mediated by the level of distress. TABLE 2. Two-Way Analyses of Variance of the Study Variables for the ED Subgroups and the Nonpatient Controls Variable ED symptoms DT BD Emotional distress symptoms Depression State anxiety Representations Reflective symbolization Mother Father Self Quality of representation Mother benevolencea Father benevolenceb A B C D Nonpatients (n = 45) AN-R (n = 31) AN-B/P (n = 18) BN (n = 22) Mean (SD) Mean (SD) Mean (SD) Mean (SD) F(4,111) G2 Contrasts 3.08 (4.85) 5.80 (6.74) 12.86 (8.04) 16.31 (11.69) 15.09 (8.31) 18.50 (11.83) 12.83 (6.50) 16.76 (9.66) 22.33*** 12.78*** 0.37 0.25 A G B, C, D A G B, C, D 5.67 (5.80) 34.50 (8.66) 23.01 (15.17) 51.49 (14.80) 29.97 (16.32) 55.13 (12.95) 29.95 (16.45) 54.91 (15.08) 26.95*** 21.39*** 0.42 0.37 A G B, C, D A G B, C, D 5.13 (1.20) 5.05 (1.27) 5.59 (1.09) 3.86 (1.55) 3.79 (1.59) 4.59 (1.15) 4.03 (1.71) 3.83 (1.60) 5.19 (1.43) 3.68 (1.85) 3.78 (2.01) 4.30 (1.28) 6.73*** 5.74** 7.25*** 0.16 0.13 0.16 A 9 B, C, D A 9 B, C, D A 9 B, D 5.60 (1.17) 5.59 (0.82) 4.92 (1.10) 4.22 (1.29) 4.45 (1.55) 3.58 (1.70) 4.41 (1.23) 4.21 (1.29) 6.34*** 16.26*** 0.15 0.31 A 9 C, D A 9 B, C, D a n = 112, df = 3,107. n = 109, df = 3,104. **p G 0.01. ***p G 0.001. b 514 www.jonmd.com * 2013 Lippincott Williams & Wilkins Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. The Journal of Nervous and Mental Disease & Volume 201, Number 6, June 2013 Mentalization in ED TABLE 3. Pearson’s Correlations Between Self-reported Symptoms of EDs and Emotional Distress and the Conceptual and Benevolence Scales for Representations of the Self and Parents Self-reported Symptom Scales ORI EDs Reflective symbolization (CL) Quality of representation (benevolence) Reflective symbolization (CL) Quality of representation (benevolence) Reflective symbolization (CL) Quality of representation (benevolence) Patients with ED (n = 71) Mother Father Self Mothera Fatherb Nonpatients (n = 45) Mother Father Self Mother Fatherc Total sample (N = 116) Mother Father Self Motherd Fathere Emotional Distress j0.10 0.13 0.19 j0.01 j0.15 j0.25* j0.03 0.09 j0.17 j0.25* 0 0.02 0.06 j0.11 j0.34* j0.07 j0.10 0.16 j0.11 j0.30* j0.28** j0.12 j0.07 j0.23* j0.43*** j0.40*** j0.27** j0.15 j0.34*** j0.51*** The self-reported symptom scale for EDs combined the means for the DT and the BD subscales. The self-reported symptom scale for distress combined the means for state anxiety and depression. a n = 67. b n = 66. c n = 43. d n = 112. e n = 109. *p G 0.05. **p G 0.01. ***p G 0.001. The path model, presented in Figure 1, constructed common factors of the measured scales yielding 22 df, with the chi-square goodnessof-fit (GFI) statistic, which compares the predicted and observed covariance matrices, reaching a nonsignificant value indicating good fit, W2 = 30.31, p = 0.11. The GFI index was 0.94 and the adjusted GFI was 0.88, indicating acceptable fit. The root mean square error of approximation, proposed by Browne and Cudeck (1989) to test the null hypothesis of close fit as a more meaningful approximation than the null hypothesis of perfect fit, was 0.059, indicating fair fit. Standardized estimates for the model are presented in Figure 1. The proposed direct path from the ORI to ED symptoms was not found to be significant. Nonetheless, the indirect path from ORI through emotional distress symptoms was supported by the model’s parameter estimates (A = j0.71). The data showed that the ORI factor had a significant attenuating effect on emotional distress. Examining the loading of each general scale (benevolence and CL) on the ORI factor and the loading of each ORI subscale on each general scale yielded the following: the level of benevolence in the parents’ representations had a higher load on the general ORI factor than the reflective symbolization (CL) level of the self and parent representations. In addition, father’s benevolence had a higher loading than mother’s benevolence on the general benevolence factor. Reflective symbolization level for mother had the highest loading on the general reflective symbolization factor, whereas the level of symbolization of self-representation had the lowest loading. DISCUSSION The first aim of this study was to examine several aspects of mentalization in patients with ED through analysis of their narrative * 2013 Lippincott Williams & Wilkins descriptions about the self and their parents. We examined the cognitive-developmental level of the self and other representations by investigating the participants’ maturity of reflective symbolization. We also studied the affective quality of these female adolescents’ working models of their attachment figures. The second aim of this study was to examine whether mentalization ability and the quality of working models of parents may a) directly serve to protect these adolescents from turning to psychosomatic ED symptoms and b) indirectly serve as a protective factor by facilitating the participants’ ability to regulate and cope with emotional distress, thus reducing the risk for developing ED symptoms. In accordance with the first research hypothesis, the patients with ED demonstrated a lower developmental capacity for mentalization than the controls without ED, expressed in the ORI descriptions of the self and parents. The average reflective symbolization (CL) level of between 5 and 6 found in our control group for the three types of representations (father, mother, and the self ) indicates an adequate capacity for mentalization in functional and internal mental states. By contrast, the patients with ED showed an average level of 4 for the description of the self and of 4 or lower in their descriptions of their parents. This indicates that the inpatients are mainly externally focused, referring to their parents mostly in terms of their concrete physical attributes. These findings reflect a developmental impairment in the cognitive capacity of the adolescent patients with ED for reflecting symbolically on the self and others. A similar finding emerged for the adolescents’ affective quality of parents’ representations: the nonpatients presented significantly more benevolent and secure representations of both the mother and the father than did the patients with ED. This result coincides with studies www.jonmd.com Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 515 Rothschild-Yakar et al. The Journal of Nervous and Mental Disease & Volume 201, Number 6, June 2013 FIGURE 1. Reflective symbolization level and parents’ benevolence as direct and indirect protective resources from ED symptoms. showing high prevalence of insecure attachment relationships in patients with ED (Troisi et al., 2006; Ward et al., 2001). Attachment theories (Slade, 2005) and studies in the framework of social-cognition models (Bydlowski et al., 2005) assume the likelihood of a congruence in developmental symbolization level between representations of the object and the self. However, the findings in our total sample seemed to contradict this claim. For one, the reflective symbolization level of representations of the self was only moderately correlated with the level of parents’ representations. Second, a significant but low correlation emerged in the reflective symbolization level between the self and father’s benevolence but not between the self and mother’s benevolence. Nonetheless, our data may lend support to the contention of Fonagy et al. (1998) that mentalization ability may vary because of conflicting relations across different situations and different persons. Thus, although adolescents, primarily those diagnosed with an ED, demonstrate an ability to internally focus on themselves, they are more externally focused and concrete in their descriptions of their parents. The lack of correlations between mother benevolence and the three CL scales may correspond with Drodge (1997), who found no association between the CL scale and the affective tone of adolescents’ relationships with parents. The second part of the first hypothesis, concerning differences among the subtypes of ED with respect to reflective symbolization level and parental perception, was not confirmed. Several explanations can be suggested to explain these data. Our data supported recent claims that patients with ED of all subtypes share many core personality traits and tend to move across different diagnostic categories during the course of their illness (Eddy et al., 2008). Moreover, most studies assessing personality in EDs have been undertaken in adults. Perhaps the relations between maladaptive personality attributes and ED subtype (overcontrol-restricting versus undercontrol-B/P, Kaye 516 www.jonmd.com et al., 2004) are greater in adult populations than in adolescents such as those included in our study. The current findings did confirm our second study hypothesis. Accordingly, the presence of secure benevolent working models with parents and of better-developed reflective symbolization ability of the self and parents was found to indirectly predict lower levels of ED symptoms, by reducing the level of distress. Interestingly, secure working models with parents had greater value in predicting emotional distress than did reflective symbolization level. In the absence of internalization of calming, benevolent parental representations that could assist in coping with negative moods, patients may turn to ED-related preoccupations and behaviors as a means to escape emotional distress. These data coincide with the association found between body dissatisfaction and an insecure style of attachment in women with AN and BN (Troisi et al., 2006). Our findings further show that, for the participants both with and without ED, the representation of the father as secure, but not the mother, correlated negatively with emotional distress (SRdistress) and with ED symptoms (SR-ED). This suggests that, for female teens, whether ill or healthy, secure relationships with the father are crucial. Female adolescents experience the developmental process of separation-individuation and identity integration, which are associated with conflicting relationships, mostly with the mother. In the case of the female patients with ED, these data may further underscore the importance of a secure father-child relationship as protecting the adolescent from distress (Mountford et al., 2007) and hence, indirectly, as reducing the severity of ED symptoms. In line with Mountford et al. (2007), the current data suggest that insecure, negative childhood experiences, with the father seen as ignoring or responding negatively to the communication of negative emotions, are a key factor leading to the development of an ED, with emotional distress intolerance as a mediating factor. * 2013 Lippincott Williams & Wilkins Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. The Journal of Nervous and Mental Disease & Volume 201, Number 6, June 2013 An important finding of this study is the lack of significant correlations in the adolescent sample as a whole between the ability to mentalize and symbolize self-experiences and ED psychopathology. This stands in contrast to the significant correlations found in the total sample between both parents’ reflective symbolization level and distress and between mother’s symbolization level and ED symptoms as well as between mother’s reflective symbolization level and distress in the inpatients with ED. These findings may suggest that, in the developmental phase of adolescence, a developed symbolic understanding of the attachment figures’ ideas and experiences is a regulating, calming, and crucial predictor of the ability to cope with stress and to protect against the development and maintenance of ED symptoms. Moreover, these findings may highlight the importance of the interplay between two domains of relating to the self and others: the domain of mentalization of the self and others and the domain of investment in the self versus others. Thus, a higher reflective symbolization level and a developed awareness to attributes of the self do not necessarily mean an investment in self needs. In addition, our data show that, in the group of patients with ED, a developed awareness to the mental attributes of the mothers but not of the fathers may protect from distress. These data may be in line with studies of EDs within the framework of self-psychology (Goodsit, 1997), family therapy (Minuchin et al., 1978), and recent empirical self-psychology findings (Bachar et al., 2010, 2008), suggesting that attunement to the mother’s needs and characteristics and not to one’s own perspective may be associated with the development and maintenance of an ED. Note that self-psychology examines the extent of selflessness and of the readiness to ignore one’s own needs and to serve as selfobject for others, as either a predisposing (in higher levels of selflessness) or a protective (in normal and lower levels of selflessness) factor in EDs. Similarly, our paradigm suggests that different reflective symbolization levels may act as either predisposing (low reflective symbolization levels) or protective (high reflective symbolization levels) factors in the development and maintenance of an ED. Future studies should examine the interplay between these two domains: the developmental reflective symbolization domain and the selflessness domain in the predisposition to an ED. Conclusions and Clinical Implications Recent clinical observations and empirical research emphasize that secure attachments in childhood and adulthood and well-developed capacities for symbolization and mentalization promote resilience to stressful events (Taylor, 2010). Our study has shown that these capacities are also of considerable relevance in the development and maintenance of an ED. As noted earlier, our findings likely have important implications for prevention and treatment. For example, the contribution of high symbolization and mentalization to a reduction in ED symptoms may suggest that treatment strategies focused on the development of mentalization should be integrated alongside interventions addressing ED symptoms. Our findings also point to the importance of treatment of adolescent patients with ED, to address relationships not only with the mother but also, most importantly, with the father. This is particularly relevant in the case of adolescents who are hospitalized because of an ED, who likely show considerable difficulties in separation from their primary parental figures. Thus, therapeutic interventions in EDs may do well to focus on promoting secure relationships with the father, to enhance regulation ability and reduce ED symptoms. Limitations and Recommendations for Further Research First, our research design is cross-sectional and performed in acutely ill patients, which allows for inferences about associations but not causation. Second, we assessed mentalization abilities and working models of parents only via the ORI because this multidimensional tool * 2013 Lippincott Williams & Wilkins Mentalization in ED is a highly acceptable measure in the study of symbolization and the affective quality of representations, as well as in separately examining reflective ability about the self versus significant others. Although the ORI thereby permitted assessment of several components of mentalization, future studies should, nevertheless, implement additional measures of mentalization components. Third, our inclusion of only inpatients in our sample does not enable direct generalization of our results to outpatients with less severe ED pathology. Future research should be longitudinal and prospective and should examine whether improvement in mentalization ability and the quality of working models of parents influence the process and outcome of an ED. DISCLOSURE The authors declare no conflict of interest. REFERENCES American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders (4th ed). Washington, DC: American Psychiatric Association. Bachar E, Gur E, Canetti L, Berry E, Stein D (2010) Selflessness and perfectionism as predictors of pathological eating attitudes and disorder: A longitudinal study. Eur Eat Disord Rev. 18:496Y506. Bachar E, Kanyas K, Latzer Y, Canetti L, Bonne O, Lerer B (2008) Depressive tendencies and lower levels of self-sacrifice in mothers, and selflessness in their anorexic daughters. Eur Eat Disord Rev. 16:184Y190. Beck AT, Ward CH, Mendelson M, Mock JE, Erbaugh JK (1961) An inventory for measuring depression. Arch Gen Psychiatry. 4:561Y571. Blatt SJ, Auerbach JS, Levy KN (1997) Mental representations in personality development, psychopathology, and the therapeutic process. Rev Gen Psychol. 1:351Y374. Blatt SJ, Bers SA, Schaffer C (1993) The assessment of self (Rev ed). Unpublished manual, Yale University, New Haven, CT. Blatt SJ, Chevron ES, Quinlan DM, Schaffer CE, Wein S (1992) The assessment of qualitative and structural dimensions of object representations (Rev ed). Unpublished manual, Yale University, New Haven, CT. Blatt SJ, Wein SJ, Chevron ES, Quinlan DM (1979) Parental representations and depression in normal young adults. J Abnorm Psychol. 88:388Y397. Bleiberg E (2001) Treating personality disorders in children and adolescents: A relational approach. New York: Guilford Press. Browne M, Cudeck R (1989) Single sample cross-validation indices for covariance structure. Multivariate Behav Res. 24:445Y455. Bruch H (1988) Conversations with anorexics. London: Jason Aronson. Bydlowski S, Corcos M, Jeammet P, Paterniti S, Berthoz S, Laurier C, Chambry J, Consoli SM (2005) Emotion processing deficits in eating disorders. Int J Eat Disord. 34:321Y329. Choi-Kain LW, Gunderson G (2008) Mentalization: Ontogeny, assessment, and application in the treatment of borderline personality disorder. Am J Psychiatry. 165:1127Y1135. Dodge KA, Rabiner DL (2004) Returning to roots: On social information processing and moral development. Child Dev. 75:1003Y1008. Drodge EN (1997) Parental representations, self-view, and interpersonal functioning of older adolescents. J Pers Assess. 68:152Y164. Eddy KT, Dorer DJ, Franko DL, Tahilani K, Thompson-Brenner H, Herzog DB (2008) Diagnostic crossover in anorexia nervosa and bulimia nervosa: Implications for DSM-V. Am J Psychiatry. 165:245Y250. Fassino S, Pierò A, Gramaglia C, Abbate-Daga G (2004) Clinical, psychopathological and personality correlates of interoceptive awareness in anorexia nervosa, bulimia nervosa and obesity. Psychopathology. 37:168Y174. First MB, Spitzer RL, Gibbon M, Williams JBW (1995) Structured Clinical Interview for DSM-IV Axis I Disorders: Patient Edition (SCID-I/P, version 2.0). New York: New York State Psychiatric Institute. Fonagy P, Gergely G, Jurist EL, Target M (2002) Affect regulation, mentalization, and the development of the self. New York: Other Press. Fonagy P, Luyten P (2009) A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder. Dev Psychopathol. 21:1355Y1381 Fonagy P, Target M (1996) Playing with reality: Vol. I. Theory of the mind and the normal development of psychic reality. Int J Psychoanal. 77:217Y233. www.jonmd.com Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 517 Rothschild-Yakar et al. The Journal of Nervous and Mental Disease Fonagy P, Target M, Steele H, Steele M (1998) Reflective-functioning manual (version 5) for application to Adult Attachment Interview. London: Sub-Department of Clinical Health Psychology, University College. Garner DM (1991) Eating Disorders InventoryY2: Professional manual. Odessa, FL: Psychological Assessment Resources. Garner DM, Olmsted MP, Bohr Y, Garfinkel PE (1982) The Eating Attitudes Scale: Psychometric features and clinical correlates. Psychol Med. 12:871Y878. Goodsit A (1997) Eating disorders: A self psychological perspective. In Garner D, Garfinkel PE (Eds), Handbook of psychotherapy for eating disorders (pp 55Y82). New York: Guilford Press. Kaye WH, Strober M, Jimerson D (2004) The neurobiology of eating disorders. In Charney DS, Nestler EJ (Eds), The neurobiology of mental illness (pp 1112Y1128). New York: Oxford Press. Klump KL, Bulik CM, Pollice C, Halmi KA, Fichter MM, Berrettini WH, Devlin B, Strober M, Kaplan A, Woodside DB, Treasure J, Shabbout M, Lilenfeld LR, Plotnicov KH, Kaye WH (2000) Temperament and character in women with anorexia nervosa. J Nerv Ment Dis. 188:559Y567. Lieberman MD (2007) Social cognitive neuroscience: A review of core processes. Annu Rev Psychol. 58:259Y289. McDougall J (1989) Theatres of the body: A psychoanalytic approach to psychosomatic illness. London: Free Association Books. Meins E, Fernyhough C, Russell J, Clark-Carter D (1998) Security of attachment as a predictor of symbolic and metalizing abilities: A longitudinal study. Soc Dev. 7:1Y24. Minuchin S, Rosman BL, Baker L (1978) Psychosomatic families: Anorexia nervosa in context. Cambridge, MA: Harvard University Press. 518 www.jonmd.com & Volume 201, Number 6, June 2013 Mountford V, Corstorphine E, Tomlinson S, Waller G (2007) Development of a measure to assess invalidating childhood environments in the eating disorders. Eat Behav. 8:48Y58. Porcerelli JH, Huprich SK, Binienda J, Karana D (2006) Object representations and their relationship to psychopathology and physical health status in African-American women in primary care. J Nerv Ment Dis. 194:838Y844. Rothschild-Yakar L, Levi-Shiff R, Fridman-Balaban R, Gur E, Stein D (2010) Mentalization and relationships with parents as predictors of eating disordered behavior. J Nerv Ment Dis. 198:501Y507. SAS Institute Inc (2004) SAS Software\ 9.1.2. Cary, NC: SAS Institute Inc. Skårderud F (2007) Eating one’s words: Part I. ‘‘Concretized metaphors’’ and reflective function in anorexia nervosa. An interview study. Eur Eat Disord Rev. 15:163Y174. Slade A (2005) Parental reflective functioning: An introduction. Attach Hum Dev. 7:269Y281. Spielberger CD, Gorsuch RL, Lushene RE (1970) STAI manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Clinical Press. Strober M (1987) The Eating Disorders Family History Interview. Los Angeles: University of California. Taylor GJ (2010) Affects, trauma, and mechanisms of symptom formation: A tribute to John C. Nemiah, MD (1918Y2009). Psychother Psychosom. 79:339Y349. Troisi A, Dilorenzo G, Alcini S, Nanni RC, Dipasquale C, Siracusano A (2006) Body dissatisfaction in women with eating disorders: Relationship to early separation anxiety and insecure attachment. Psychosom Med. 68:449Y453. Ward A, Ramsay R, Turnbull S, Steele H, Steele M, Treasure J (2001) Attachment in anorexia nervosa: A transgenerational perspective. Br J Med Psychol. 74:497Y505. * 2013 Lippincott Williams & Wilkins Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.