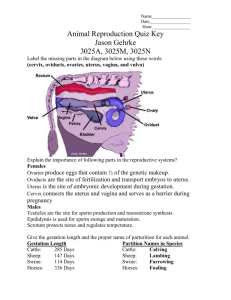
Benign Disorders & Cervical Lesions Congenital Anomalies of the Vulva & Vagina: Occur in external genitalia, vagina, and cervix Often associated with concomitant anomalies in the upper reproductive tract And anomalies in the GU tract (renal agenesis, pelvic/horseshoe kidneys, irregular collecting ds. etc.) Upper Genital Tract: Includes the endometrium, myometrium, uterus, fallopian tubes, ovaries, and peritoneal cavity Lower Genital Tract: Includes the vulva, vagina, and cervix DISORDERS OF THE LOWER REPRODUCTIVE TRACT Disorder Patho/Etiology Clinical Presentation Diagnosis Treatment NOTES Exogenous cortisol Glucocorticoid provides (-) feedback that ↓ ACTH release 21-hydroxylase deficiency CAH ↑: androgens + DHEA ↓: aldosterone + cortisol Benign Disorders of the Lower Genital Tract Labial Fusion Imperforate Hymen Transverse Vaginal Septum Causes: 1. Excess androgens: M.C.C. = EXOGENOUS androgen - OR2. Enzymatic: ↑ androgens M.C. type of error= 21hydroxylase deficiency leading to CAH Absence of opening in hymen; results in obstruction to outflow tract Anomaly occur when Müllerian tubercle is not canalized In neonates: - Phenotypically = ambiguous or masculinization of external genitalia (enlarged clitoris, labial fusion, labioscrotal masc.) ↑ 17hydroxyprogesterone ↑ Urine 17-ketosteroid ↓ Serum cortisol Exogenous Aldosterone Mineralocorticoid added for salt wasting (fludrocortisone acetate) - Metabolically = salt wasting (ADRENAL CRISIS – 75% pts), hypotension, hyperkalemia and hypoglycemia Primary amenorrhea, dysmenorrhea, abdominal pain Before menarche: hydrocolpos or mucocolpos = buildup of secretion behind hymen After menarche: hematocolpos/ hematometra: buildup of blood behind hymen in vagina or uterus (respectively) Presents similar to imperforated hymen, primary amenorrhea, cyclic pelvic pain accompanied by menstrual symptoms. Physical examination: Absence of an identifiable vaginal lumen; tense bulging hymen Usually made at the time of puberty in adolescents: Often requires reconstructive surgery Treatment Surgery to excise the extra tissue Evacuate any obstructed material Create a normal sized vaginal opening Surgical correction → only form of treatment Differentials: imperforate hymen, and vagina atresia/agenesis Occurs at junction between lower 2/3 and upper 1/3 of vagina Vaginal Atresia Vagina is abnormally closed or absent Lower vagina fails to develop (urogenital sinus failure) and is replaced with fibrous tissue Normal external female genitalia with short vagina that appears to end in a blind pouch Primary amenorrhea, cyclic pelvic pain Absence of introitus and presence of vaginal dimple Ultrasound and MRI: thickness and location of the septum. Confirm the presence of other parts of the reproductive tract Pelvic imaging w/ ultrasound and/or MRI large hematocolpos and presence of upper tract Normal ovaries, uterus, cervix, and upper vagina Vaginal Agenesis Vagina is abnormally closed or absent Mayer-Rokitansky-Kü sterHauser (MRKH): - Normal pheno/genotype - Normal ovaries and fx - Normal secondary sexual characteristics - Congenital absence of the vagina - Absence or hypoplasia of cervix, uterus, fallopian and ovaries and kidneys - Amenorrhea; normal external and abnormal internal genitalia - Rudimentary pouch of vagina may be present 10% have normal uterus with functioning endometrium associated w/ urologic and (rarely) skeletal anomalies Can also have CARDIAC issues Pelvic imaging with ultrasound and MRI to assess the: Vagina Uterus Ovaries Kidneys Surgical correction: Incision of the fibrous tissue, evac of accumulated contents, normal upper vagina sutured to hymenal ring vaginal pull-through procedure Psychosocial support Counseling Nonsurgical and surgical correction individualized to the patient Serial vaginal dilators used on perineum or blind vaginal pouch, may be used with or without surgery Differentials: Turner’s pt’s genitalia can present with similar genitalia, imperforate hymen, transverse septum Benign Epithelial Disorders Lichen Sclerosis Age: women of all age groups Major significance: postmenopausal women in 50’s or 60’s→ associated with 4% risk of vulvar skin cancer Lichen Planus Women in their 50s or 60s and it is associated with a 4% risk of vulvar skin cancer Associated with vaginal adhesions and with erosive vaginitis. Usually asymptomatic, may cause pruritus and dyspareunia Atrophy can cause resorption of the labia minora Thinning of the vulvar skin, and skin fragility Labial fusion Occlusion of the clitoris Contracture of introitus - White coloration; often figure 8 pattern around vulva + anus Chronic eruption of shiny purple papules with white striae. Vaginal adhesions. Similar lesions are often found on the mucous membrane of the oral cavity and flexor surfaces. Histological confirmation Topical steroids: clobetasol: 0.05% 1-2x/day 6-12 weeks Biopsy if malignancy is suspected (sclerosis and planus) Types of tx for sclerosis + planus: for post-inflammatory sequela adhesions and stenosis Differentials: also includes carcinomas such as squamous cell, basal cell, melanoma, sarcoma, and Paget disease of the vulva (presents w/ eczema) High potency topical Vaginal suppositories: hydrocortisone Vaginal estrogens Surgical excision or vaginal dilators for vaginal adhesions Skin disorder leads to a scratch–itch cycle Intense pruritus → usually unilateral & circumscribed, may be due: 1. Atopic dermatitis 2. Neuropathic pain 3. Psychologic disorders It may begin with something that rubs, irritates, or scratches the skin, such as clothing. Thickened skin with skin markings and excoriations → due to chronic itching and scratching. 1) High potency topical steroids: clobetasol or halobetasol (1-2x/d for 612 weeks, then reduce to once a week 2) Low dose vaginal estrogen: Premarin - for vaginal atrophy in postmenopausal women 3) Surgical excision to enlarge the introitus and open adhesions 6 Ps: Purple, Pruritic, Papules, Plaques, Polygonal, Planar Lichen Simplex Chronicus Lesions should be biopsied in older women to rule out vulvar skin cancer 4) Vaginal Dilators: to widen the introitus Topical steroids 2x/ 4-6 weeks (medium-high potency) Vulvar Psoriasis Red, moist, scaly lesions Asymptomatic or pruritus Treatment: Topical steroids Ultraviolet light Benign Cysts or Tumors Epidermal Inclusion Cysts M.C. Tumor on the vulva Cause: Occluded pilosebaceous duct/ hair follicle Sebaceous Cysts Apocrine Sweat Gland Cysts May be found on vulva or vagina Solitary, small, mobile, nontender, filled with keratinaceous material If these become superinfected and develop into abscesses Multiple, non-tender, usually appear yellow, usually asymptomatic Filled with sebaceous material Sweat glands in the axilla, mons pubis, and labia majora can become occluded and form cysts. 1. Fox-Fordyce disease: Pruritic, inflamed, keratinplugged apocrine sweat glands Skene’s Gland Cysts Incision and drainage or complete excision 2. Hidradenitis suppurativa: apocrine + sebaceous glands; abscesses in underarms, breasts, inner thighs, groin, and buttocks. (paraurethral glands), located next to the urethra meatus Chronic inflammation obstruction of ducts + cystic dilation of the glands If they become infected and form multiple abscesses Excision or incision and drainage are the treatments of choice. If an over-lying cellulitis is present, antibiotics are indicated Cysts: generally, no treatment required if asymptomatic; if infected/abscessed, antibiotics with incision/drainage (I&D) or excision Bartholin’s Duct Cysts and Abscesses Mucous-secreting glands that provide lubrication to the vagina; opens just external to hymenal ring Location: at 4 and 8 o’clock positions near the vaginal introitus Gartner’s Duct Cysts Can be asymptomatic if the cyst remains small (1-2cm) – may resolve on its own 1. Warm sitz baths several times per day: pain relief and to ↓ healing time. Cysts can become large and cause localizes pain, dyspareunia, and pain with walking can lead to infection (Bartholin abscess) 2. Adjunct antibiotic therapy: If Neisseria gonorrhoeae (10%) (Azithro, Doxy); If cellulitis or an abscess, tx for S. aureus Result from polymicrobial infections, and is also associated with STDs Word Catheter (w/balloon): emergent setting or office For drainage: 4-6 weeks Obstruction Cystic Dilation Marsupialization: Indications: 1. Recurrent cysts 2. Abscesses (infected cyst) 3. Word Cath failed prevents reformation of the abscess 1. Bartholin Abscess 2. Bartholin Cyst 3. Bartholin Cyst carcinoma: < 1% Remnants of Wolffian system. Most common location: anterior lateral aspects of the upper part of the vagina Most asymptomatic May present in adolescence with dyspareunia or difficulty inserting tampon Excision: potential for significant bleeding during excision use vasopressin to maintain hemostasis If needs to be removed, IVP (IV pyelogram) and cystoscopy locate bladder and urethra Benign Cervical Lesions Nabothian Cysts Dilated retention cysts <1cm Intermittent blockage of mucinous endocervical glands Normal variant Clinical presentation: M.C. in menstruating women; most are asymptomatic. No tx needed for most Woman over 40 = risk for Bartholin gland cancer biopsy cyst wall Differentials 1. Urethral diverticula 2. Ectopic ureters 3. Vaginal and cervical cancer Endometriosis Cysts Cervical Polys Cervical Fibroids Cervical Stenosis Can implant on/near cervix Benign pedunculated or broad-based (sessile) growth from endocervix or endometrium Rarely: obstructs canal Very rarely: (<1%) contain Squamous Cell Carcinoma or adenocarcinoma Can arise In cervix or be prolapsing from the endometrial cavity 1. Congenital 2. Infection 3. Scarring (surgery, cryosurgery, radiation) 4. Atrophy: secondary to lack of estrogen 5. Obstruction: neoplasm, polyp, fibroid (less common) Cysts tend to be red or purple in color Endometriosis symptoms cyclic pain and dysperunia Intermenstrual/ postcoital bleeding No tx needed Hysteroscopy distinguish cervical and endometrial polyps No pain Removal to prevent masking of abnormal bleeding done easily in office: twist off with ring forceps in office Not considered premalignant lesion Dilation and curettage (D&C) May need electrocautery Dyspareunia, bladder pressure, rectal pressure, pregnancy problems (dilation, hemorrhage, malpresentation, obstruction) Typically asymptomatic Does not affect menstruation or fertility unless passage from uterus is completely blocked Can cause difficult birth; of obstruct certain procedures DISORDERS OF THE UPPER REPRODUCTIVE TRACT Congenital Anomalies Surgical removal if symptomatic Hysterectomy rather than myomectomy may be required depending on location and desire to preserve fertility Generally, no tx necessary Can use cervical dilators can leave catheter in cervical canal for few days until stenosis relieved Obstructive lesions should be removed Rule out possibility of cervical cancer PATHOGENESIS: Female Reproductive Organs Arise From: 1. Genital ridge: ovaries 2. Mü llerian system: Formed by fusion of paramesonephric (mü llerian) ducts: superior vagina, cervix, uterus, fallopian tubes 3. Urogenital diaphragm: Lower one-third of the vagina EPIDEMIOLOGY: Uterine anomalies are EXTREMELY RARE Incidence increased in women exposed to DES from 1940-1973 DES: Diethylstilbestrol: synthetic non-steroidal estrogen - Given to woman with risk of spontaneous abortion (also given for postpartum laceration, atrophic vaginitis, menopausal symptoms, adv breast cancer, etc.) - Female children later developed congenital anomalies Isolated congenital anomalies of the cervix are rare Can cause uterine didelphys with a double vagina, a double cervix (bicollis) may be found, but not isolated. Women who were exposed in utero to DES (25%) have an associated abnormality of the cervix, including: 1. Cervical hypoplasia 2. Cervical collars (fig. 13-11) 3. Cervical hoods 4. Cock’s comb cervix 5. Pseudopolyps Other risks of DES: 1. Increased risk of cervical insufficiency in pregnancy. 2. A very rare clear cell adenocarcinoma of the cervix and vagina. Cell adenocarcinoma of the cervix and vagina: Seen in young women <20; only occurs in 0.1% of DES-exposed pts Non-Drug Related Cause = M.C. septate uterus due to: malfusion of müllerian ducts Also associated with: Unilateral renal agenesis, pelvic/horseshoe kidneys, and irregularities in collecting system CLINICAL MANIFESTATIONS: Anomalies usually asymptomatic and most are discovered incidentally during OBGYN visits at onset of menarche, coitus, or when attempting pregnancy Symptoms associated with anomalies of the uterus include: Menstrual abnormalities Dysmenorrhea Dyspareunia Cyclic and noncyclic pelvic pain Infertility Recurrent miscarriages Mullerian Anomalies (CLASS): Class I – Hypoplasia/Agenesis: failure in müllerian duct fusion; can affect, vagina, cervix, fundal, tubal, or combined - associated with Mayer-Rokitansky-Hauser-Kauser Syndrome (MRHK): absent vagina and uterus - presents with amenorrhea and urinary tract anomalies Class II – Unicornuate uterus: may have communicating/non-communicating endometrial cavity or absent cavity; müllerian ducts fail to form incomplete horn (banana shape) Class III – Uterine didelphys: double uterus; ducts fail to fuse and each become a separate uterus Class IV – Bicornuate uterus = M.C. can be complete, partial or arcuate (bow shape); ducts fail to fuse on top, resulting in two separate single horns sharing one cervix Class V – Septate Uterus: medium septate persists in the uterus; lacks adequate blood supply to facilitate placentation and maintain pregnancy; RISK = recurrent 1st trimester miscarriage Class VI – Arcuate uterus/partial septate: normal in shape, small indentation in fundus; medium septum fails to dissolve completely; no negative effects in pregnancy Class VII – DES Related DIAGNOSIS: Primary investigative tools for uterine abnormalities are: 1. Pelvic ultrasound 2. CT scan 3. MRI 4. Sonohistogram 5. Hysterosalpingogram 6. Hysteroscopy 7. Laparoscopy TREATMENT: Many uterine anomalies require no treatment. Treatment: when the defect causes significant symptoms such as: Pain Menstrual irregularities Infertility Uterine septa: Can be excised with operative hysteroscopy Bicornuate uterus has to be ruled out first. Bicornuate uterus When a viable pregnancy cannot be achieved: - Surgical unification procedures is indicated. - Viable pregnancies have been achieved after these surgeries. - These pts will require cesarean to ↓ the risk of uterine rupture. Many women are able to carry a pregnancy to fruition, with risk ↑ of: - Preterm labor - Preterm delivery Benign Disorders of the Upper Genital Tract Leiomyoma (uterine myoma, uterine fibroid) PATHO/ EPIDEMIOLGY: Proliferation of the smooth muscle cells of the myometrium; vary in size It is unclear if fibroid have malignant potential; however, leiomyomas and leiomyosarcomas typically exist concurrently (with rare exception) Leiomyosarcoma thought to be new neoplasms and not a degeneration of an existing benign fibroid Factors that play a role in the formation and growth of uterine fibroids: 1. Genetic predisposition 2. Steroid hormone factors 3. Growth factors 4. Angiogenesis Responsive to both estrogen & progesterone but the relationship is complex. 1 Reproductive age women: fibroids can grow and shrink at differing rates During menopause the tumors: Usually stop growing May atrophy in response to naturally ↓endogenous estrogen levels Risks to develop leiomyoma by age 50. Whites: 70% African American: > 80% 5x more likely (also more likely to be diag. younger, have larger or more fibroids, bleed heavily, and develop severe anemia) CLINICAL MANIFESTATIONS: Fibroids become problematic only when their location results in: Heavy or irregular bleeding Reproductive difficulties. Large enough to cause a mass effect on other structures resulting in: 1. Pelvic pain and pressure 2. Urinary frequency 3. Constipation ANY OF THESE CONDITIONS CAN COEXIST WITH FIBROIDS: 50-65% → Have no clinical symptoms M.C. symptom = abnormal uterine bleeding: Typically presents as: Menorrhagia: increasingly heavy periods of longer duration Postcoital spotting: spotting after intercourse. Metrorrhagia: bleeding between periods Menometrorrhagia: heavy irregular bleeding Blood loss from fibroids can lead to: 1. Chronic iron-deficiency anemia 2. Dizziness 3. Weakness 4. Fatigue Pelvic Pain: Present if vascular compromise is present. Most common in subserosal pedunculated fibroids. Secondary dysmenorrhea: when menorrhagia or menometrorrhagia are present. Pressure-related symptoms: Vary depending on the number, size and location of leiomyomas. Pelvic pressure Constipation Hydronephrosis Venous stasis Urinary frequency Urinary retention ON PHYSICAL EXAM: Depending on their location and size: Leiomyomas can sometimes be palpated on: 1. Bimanual Pelvic examination: a nontender irregularly enlarged uterus with “lumpy-bumpy” or cobblestone protrusions that feel firm or solid on palpation. 2. Abdominal examination. (3) Types of Uterine Fibroid Subserosal: can impact implantation, placentation & ongoing pregnancy; resection of submucosal fibroids in pts diagnosed with infertility does lead to increased conception rates. Intramural & Submucosal: are both unlikely to affect conception or pregnancy loss except when multiple fibroids are present. DIAGNOSIS: 1. Differentials: depends on the pt symptoms 2. Pelvic ultrasound: M.C. – can be seen as areas of hypoechogenicity among normal myometrial material Valuable tools in identifying submucosal fibroids and in distinguishing fibroids from polyps: 3. Hysterosalpingogram (HSG) 4. Sonohysterogram (saline infusion sonogram) 5. Hysteroscopy 6. MRI: especially helpful in distinguishing fibroids from adenomyosis as well as for surgical planning. TREATMENT: 1. Expectant therapy: Most cases with close follow up, they ↓ size after menopause Pts with actively growing fibroids: Follow every 6 months to monitor the size and growth. 2. Nonhormonal options - Nonsteroidal anti-inflammatory drugs - Anti-fibrinolytics: tranexamic acid - Are limited at treating: Dysmenorrhea Heavy prolonged bleeding Anemia 3. Hormonal options: Combined oral contraceptive pills Progestins (medroxyprogesterone acetate Mirena IUD Norethindrone acetate Mifepristone Androgenic steroids: danazol and gestrinone GNRH agonists: nafarelin acetate, leuprolide acetate depot 4. Uterine Artery Embolization Less invasive, for treating symptomatic fibroids. Interventional radiologist catheterizes the femoral artery under local anesthesia in order to inject an embolizing agent into each uterine artery. Goal: decrease the blood supply to the fibroid. 5. Surgery: Myomectomy: preserves fertility 1. Laparoscopy 2. Laparotomy Hysterectomy: definitive treatment for leiomyomas when fertility is completed 1. Abdominal: TAH 2. Vaginal: TVH GnRH agonists may be used to: Presurgical shrinkage: GnRH agonist for 3-6 months. Stop bleeding ↑ the hematocrit prior to surgical treatment of uterine fibroids PROGNOSIS: Unfortunately, the tumors usually resume growth after the medications are discontinued. Women nearing menopause: txs may be used as a temporizing measure until their own endogenous estrogens decrease naturally NOTES: More commonly associated with: 1. African American heritage 2. Early menarche 3. Nulliparity 4. Perimenopause 5. Nonsmoking 6. Increased alcohol use 7. Hypertension Disorder Endometrial Polyps Patho/Etiology Localized benign overgrowths of endometrial glands and stroma. Clinical Presentation Diagnosis Diagnostic Evaluation 1. They vary in size from millimeters to several centimeters May be: Ultrasound 2. Sonohysterogram 3. Hysteroscopy Treatment Treatment recommendations: Any polyp will be removed in postmenopausal pts Premenopausal women require removal of symptomatic polyps NOTES Pedunculated or sessile Benefit of hysteroscopy: Single or multiple • Location: Is the possibility of immediate treatment. Women’s age ≥ 45 with abnormal bleeding from endometrial polyps should be Within the endometrial cavity prolapse through the endocervical canal. evaluated with endometrial biopsy prior to removal. Most commonly in women 4050 years old Women taking tamoxifen are at risk for developing polyps Most commonly present symptom: metrorrhagia: bleeding between menstrual cycles. Any bleeding in a postmenopausal woman needs investigation Definition: Abnormal proliferation of both elements of the endometrium: 1. Glandular Prolonged exposure to exogenous/endogenous estrogen in absence of progesterone Classification of Hyperplasia and Endometrial Cancer (EC) Progression: Majority are benign Polyps can be malignant or premalignant in: Depends on the: Stromal Pathogenesis: Cause: 3. Risk of infertility Endometrial hyperplasia Endometrial cancer D Hx: 2. 1. 2. 5% of postmenopausal women 1% to 2% of premenopausal women Fast facts about Endometrial Polyps Endometrial Hyperplasia Asymptomatic polyps that should be removed: those at: Long periods of oligomenorrhea or amenorrhea followed by irregular or excessive uterine bleeding. Uterine bleeding in a postmenopausal woman should raise suspicion of endometrial Diagnosis: Method of choice for evaluation of abnormal uterine bleeding: Endometrial biopsy When an office endometrial biopsy cannot be obtained: Do a D&C in the operating room 1. Histologic variant of the disease why an endometrial biopsy cannot be obtained; Control abnormal bleeding Simple and complex 2. Age of the patient. Goal of treatment: Prevent progression of disease Endometrial hyperplasia is clinically important because it is: A source of abnormal uterine bleeding Link to endometrial cancer. Simple Hyperplasia: no atypical cytology; 1% risk to become EC Complex Hyperplasia: no atypical cytology; 3% risk Atypical Simple: cytologic atypia present; 10% risk Atypical Complex: cytologic atypia present; 30% risk Risk factors 1. Chronic anovulation 2. Obesity 3. Nulliparity 4. Late menopause 5. Unopposed estrogen use 6. Hypertension: independent risk factor 7. Diabetes mellitus: independent risk factor 8. Lynch II syndrome: hyperplasia or carcinoma until proven otherwise. Physical Examination: • Pelvic examination is unremarkable • Pts may also have signs associated with chronic anovulation such as: Abdominal obesity Acanthosis Acne Hirsutism because: 1. Insufficient tissue hyperplasia without atypia: Progestin 3 to 6 months 2. Patient discomfort 3. Cervical stenosis Depo-Provera Oral (Provera) medroxyprogesterone megestrol (Megace) norethindrone (Aygestin) Followed by resampling of the endometrium D&C is also recommended for women ≥ 45 Younger women with risk factors for hyperplasia and cancer Pts with atypical complex hyperplasia on biopsy (30% will have endometrial cancer Atypical complex hyperplasia treatment of choice = hysterectomy Ovarian masses can be divided into: 1. Functional cysts 2. Neoplastic growths Follicular Cysts < 2.5 cm simple cysts are physiologic, but they size vary from 3-8 cm When > 4 cm can: occurs during the proliferative (estrogen-dominant) phase of the cycle Unopposed estrogen stimulation may be from two sources: Exogenous: M.C. source = estrogen hormone replacement without progesterone Endogenous: M.C. seen in obese women: excess adipose tissue results in ↑ peripheral conversion of androgens: androstenedione and testosterone to estrogens: estrone and estradiol by aromatase in the adipocytes. This excess endogenous estrogen stimulation can then stimulate overgrowth of the endometrium resulting in: endometrial hyperplasia and even cancer. Hereditary nonpolyposis colorectal cancer Have>10-fold ↑ lifetime risk of endometrial hyperplasia & cancer. Ovarian Cysts Endometrial proliferation is a normal part of the menstrual cycle that Diagnositc Work Up: 1. Pregnancy test 2. UA 3. CBC 4. Pelvic US Follicular Cysts Management: Functional cysts of the ovaries: Most common types of ovarian cysts: no treatment necessary Results from normal physiologic functioning of the ovaries Divided into: 1. Follicular cysts → most common functional cyst 2. Corpus luteum cysts Follicular Cysts MC functional cyst Results from unruptured follicles during the follicular phase of the cycle. Usually unilateral and resolve spontaneously in 6090 days Estrogens dominate the follicular phase of menstruation Corpus luteum cysts Functional cysts that occur during the luteal phase of the menstrual cycle. Corpus luteum fails to regress after 14 days and becomes either: Enlarged ˃ 3 cm Hemorrhagic (corpus hemorrhagicum) Theca Lutein Cysts Large bilateral cysts filled with clear, straw-colored fluid. Result from stimulation by Cause a tender palpable ovarian mass 5. Culdocentesis Lead to ovarian torsion Differential Diagnosis: 1. Ectopic pregnancy 2. PID 3. Torsed ovary 4. Endometriosis Corpus luteum cysts A delay in menstruation and dull lower quadrant pain. A ruptured corpus luteum cyst can present with: 5. Appendicitis 6. UTI 7. Tubo-ovarian abscess 8. Renal stone 9. Fibroids 10. Ovarian neoplasms 1. Observation for 8-12 weeks 2. Oral Contraceptives Pills: to suppress future cyst formation 3. Repeat pelvic ultrasound Corpus luteum cysts Management Signs of hemoperitoneum late in the luteal phase. Pain meds Cysts usually resolve spontaneously May be suppressed with oral contraceptives if recurrent Cysts that do not resolve spontaneously in 60 to 90 days Physical Exam: Bimanual exam Require further evaluation and treatment Acute pain Follicular cysts usually < 8 cm, simple or unilocular in structure Lutein cysts: Usually larger than follicular cysts Feel firmer or more solid on palpation. A ruptured cyst can cause: Pain on palpation Acute abdominal pain Rebound tenderness. abnormally ↑ ß-human chorionic gonadotropin eG: From a 1. Molar pregnancy 2. Choriocarcinoma 3. Ovulation induction therapy Endometriomas; Arise from the growth of ectopic endometrial tissue within the: Ovary Adnexa Cul-de-sac. Also called “chocolate cysts” from the thick brown old blood contained in them. Findings: symptoms of endometriosis such as: Pelvic pain Dysmenorrhea Dyspareunia Infertility Torsed adnexa, the classic presentation is: Nausea and vomiting Waxing and waning pain