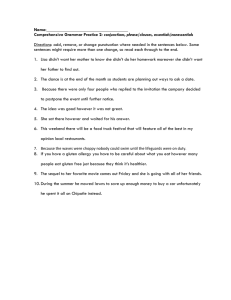
ERRATAS AND CLARIFICATION The new RR Pathology 3rd edition will be out in July or August 2009. It has been extensively revised with > 2 times more pictures and margin notes; general treatment for all diseases; and more high yield material has been added to the tables. It will not only be useful for Step 1 but also your clinical rotations and Step 2. Page 128 Under B. 3.e. Increased metabolism of 25-(OH)-D into an inactive metabolite Page 139 F. 3. Malignant tumors have up-regulation of telomerase activity Page 149 C. 1. a. Generalized catabolic reaction Page 150 Table 8-7: add to Eaton-Lambert syndrome: antibody against calcium channel Page 171 Discussion box on mitral regurgitation: a pansystolic murmur that does not increase with intensity on deep held inspiration. Also change the Margin Note right next to the box to Deep inspiration: no increase in intensity for left-sided heart murmurs and abnormal heart sounds. Margin note next to box on discussion of tricuspid regurgitation: Deep, held inspiration: Page 175 Under 4. c. (2): delete and O2 Page 189 In box discussion of Aortic regurgitation last sentence. It does not increase in intensity on deep inspiration and… Page 191 Under A. 1. a. (2) change Leishmanial forms to Amastigote forms… Under A. 2. b. add after the word infiltrate- with myocardial necrosis is highly… Page 232 Under III. A. 3. b. Acute myeloblastic leukemia (AML) Page 238 D. Acute myeloblastic leukemia Page 257 under A. 1. b b. Neutralize activated serine protease coagulation factors Factors XII, XI, IX, X, thrombin (activated prothrombin) Page 261 Under E. 2. b. Degrades factors, V, VIII, and fibrinogen Page 211 Under H. 2. b. (2) …and trap platelets, RBCs, and WBCs. Page 297 Under 6. a. Epidemiology and pathogenesis Page 300 Clarification: Chlamydia, Rickettsia, and Mycoplasma are bacteria but were separated out for discussion purposes. Will be listed under Bacteria in 3rd edition. Page 326 Under D. 3. b. (3) Trachea deviated to the ipsilateral side if the majority of the lung is collapsed. Page 335 Under M. 2. a. (2) (b) Loss of nitric oxide synthase producing (nitric oxide normally relaxes LES) Under M. 2. a. (4) Destruction of ganglion cells by amastigotes Page 347 Table 17-4 under Giardia Detected with antigen test of stool Page 348 Table 17-5 under discussion of celiac disease- Antigliadin, anti-tissue transglutaminase, anti-endomysial IgG and IgA are the best tests The pathogenesis of celiac disease has been worked out much better over the last few years. The most current concepts are included in the 3rd edition, which is available to you below. Feel free to copy it and include it in your 2nd edition. 11. Celiac disease a. Epidemiology (1) Inappropriate immune response to gluten in wheat product MN: Celiac disease: immune disease directed against gluten Also related proteins in rye and barley (2) Prevalence of 1% in North America (3) Common in whites; uncommon in blacks and Asians (4) Occurs at any age (a) Highest incidence in infancy First introduction to gluten products (b) Third decade Frequent association with pregnancy (c) Seventh decade (5) Associations MN: Celiac disease: greatest association with dermatitis herpetiformis (a) Dermatitis herpetiformis (b) Autoimmune disease Hashimoto’s thyroiditis, primary biliary cirrhosis (c) Type 1 diabetes mellitus (d) IgA deficiency (e) Down syndrome, Turner’s syndrome b. Pathogenesis (1) Multiorgan autoimmune disease (2) Inappropriate T-cell and IgA-mediated response against gluten in genetically predisposed persons Association with HLA DQ2 (95%) and HLA DQ8 (5%) (3) Timing and dose when gluten introduced in the diet is important. (4) Tissue transglutaminase (tTG; deamidating enzyme) in the lamina propria has a pivotal role. MN: Celiac disease: tTG has pivotal role (a) Deaminates mucosally absorbed gluten to produce deaminated and negatively charged gluten peptides (b) It also enhances the immunostimulatory effect of the deaminated gluten peptides (c) These peptides are phagocytosed by antigen processing cells in the lamina propria (d) They are presented in complex with HLA DQ2 or DQ8 to glutenspecific CD4 T helper cells (e) CD4 T cells produce cytokines that release matrix proteases causing cell death and degradation in the epithelial cells in the villi. c. Important diagnostic antibodies (1) Anti-tissue transglutaminase IgA (most important), IgG (a) Sensitivity and specificity 98% (b) Excellent screening test (2) Anti-endomysial IgA (a) Sensitivity and specificity 100% (b) Excellent screening test (3) Anti-gliadin IgA, IgG MN: Celiac disease: tTG, EMA, gliadin IgA antibodies (a) Sensitivity 80%, specificity 85% (b) Moderately good screening test d. Clinical findings (1) Steatorrhea (2) Weight loss MN: Celiac disease: steatorrhea, weight loss (3) Failure to thrive in infants and children (4) Pallor due to anemia (often combined anemias) (5) Dermatitis herpetiformis (a) Considered to be a form of celiac disease (b) Villous atrophy in 75% of cases with or without diarrhea (c) Low levels of above diagnostic antibodies (6) Findings related to water soluble and fat soluble vitamin deficiencies (refer to Chapter 7) (7) Other systemic findings (a) Bone osteoporosis, arthritis (b) CNS seizures, depression (c) Reproductive delayed puberty, miscarriages, infertility e. Diagnosis (1) Above diagnostic antibodies MN: Celiac disease: flattened villi; hyperplastic glands (2) Endoscopic biopsy (a) Flattened villi, particularly in duodenum and jejunum (b) Hyperplastic glands with intense lymphocytic inflammation f. Treatment (1) Gluten-free diet MN: Celiac disease: gluten free diet (2) Correct nutritional deficiencies All fat soluble vitamins; folate, vitamin B12; calcium (3) Corticosteroids in refractory cases Page 357 Table 17-8 under Crohn’s disease; More common in women and replace with No sex predilection Page 358 Under M. 1. c. (3) add (c) Increased risk (> 50%) for colorectal, breast, gynecologic cancers This is true even though the GI polyps are hamartomas Page 365 I. A. 1. b. (2) UCB is conjugated with glucuronic acid to produce conjugated bilirubin (CB) Page 367 Table 18-1: Discussion of Crigler-Najar syndromes: add …absent conjugating enzymes (glucuronyl transferase) Page 369 Box 18-1: under Normal bilirubin metabolism discussion: …and its conjugation with glucuronic acid to produce water-soluble conjugated bilirubin (CB+). Page 384 Box discussion of ceruloplasmin in Wilson’s disease. Begin the discussion with the following two sentences: Ceruloplasmin is an enzyme that is synthesized in the liver. It contains 6 atoms of copper in its structure. The gene defect in Wilson’s disease affects a copper transport system that produces a dual defect—decreased incorporation of copper into ceruloplasmin in the liver and decreased excretion of copper into bile. Page 449 Table 21-1 Chlamydia trachomatis: delete Most common STD HPV: add Most common STD Page 458 1. b. (1) Stimulates luteinizing hormone (LH) release (2) Stimulates follicle stimulating hormone (FSH) release (a) Positive feedback (b) Serum LH greater than FSH Page 461 I. 1. c. (2) Adrenal origin DHEA-sulfate (usually indicates adrenal origin); testosterone Recall that testosterone is synthesized in the ovaries and adrenal glands. DHT is produced by peripheral 5--reductase conversion of testosterone to DHT in various sites (skin, liver, testis, epididymis, seminal vesicles, prostate). Page 476 E. 1. b. (6) (a) change to Preeclampsia is present in 2% of patients. Page 504 Table 22-3 Pseudohypoparathyroidism: Autosomal dominant Clarification: some cases are inherited in an X-linked dominant fashion as originally stated in the book; however, most are inherited as autosomal dominant Page 505 Clarification Hypertension in hypercalcemia: Hypertension is seen with increased frequency in patients with hypercalcemia (e.g., primary hyperparathyroidism). It may be caused by renal insufficiency and/or calciummediated vasoconstriction of arterioles. Page 506 D. 3. a. Change wording to Glands become autonomous regardless of the calcium level. Page 507 Table 22-7: under Malignancy-induced hypercalcemia and serum phosphorus levels; subclassify into lytic and PTHr peptide where former (lytic) will be N for normal, and the latter (PTHr peptide) will be ; delete the sign. Under VII. A. 3. b. Converted to dihydrotestosterone (DHT) by 5-reductase, located in peripheral tissue Page 516 (not an errata; just an additional designation) C. Syndrome X (metabolic syndrome) Page 528 D. 2. a. Change to RF is an IgM antibody that has specificity against the Fc portion of IgG. b. Change to RF immunocomplexes consist of RF complexed with IgG molecules. Page 580-581 B. 1. b. Pathogenesis: there is a new pathogenesis for multiple sclerosis; below is the new 3rd edition rendering. Feel free to copy it and add it as an insert into your 2nd edition. a. Pathogenesis MN: MS: CD4 T cells react against self antigens in myelin sheath; cytokines activate macrophages that destroy myelin (1) Autoimmune disease initiated by (a) Genetic factors (e.g., HLA-DR2) (b) Environmental triggers Microbial pathogens (e.g., Epstein Barr virus, human herpes virus 6, Chlamydophilia pneumoniae), vitamin D, sun exposure MN: MS: genetic factors and environmental triggers (2) Environmental trigger activates helper T-cells whose antigen specific receptors recognize CNS myelin basic protein (other antigens as well) as an antigen. (3) T cells release cytokines that activate macrophages, which also release cytokines (e.g., tumor necrosis factor-) that destroy the myelin sheath as well as oligodendrocytes that synthesize myelin (4) Antibodies directed against the myelin sheath and oligodendrocytes may also be involved. Page 582-583 VII. A. Much more is known about the pathogenesis of Alzheimer’s. The most current rendering is going to used in the 3rd edition is as follows. Feel free to copy this and put it in your 2nd edition book. B. Alzheimer’s disease (AD) 1. Epidemiology MN: AD: most common overall cause of dementia a. Most common cause of dementia (50-75% of all cases) (1) Sporadic late onset type of AD (most common) MN: AD: sporadic late onset type most common type (2) Sporadic early onset type of AD (before age 65) Related to apolipoprotein gene E, allele 4 (3) Familial early onset type of AD (< 1% of cases) (a) Mutations of amyloid precursor protein (APP) on chromosome 21 (b) Mutations in presenilin 1 on chromosome 14 (c) Mutations in presenilin 2 on chromosome 1 b. Prevalence increases with age. MN: AD: prevalence increases with age (1) It is < 1% in the 60-64 year old age group. (2) It is 40-50% by the age of 95. c. Trisomy 21 (Down syndrome) has a strong association with AD By 40 years of age, most Down syndrome patients have AD 2. Role of -amyloid (A) protein in causing AD MN: AD: neurotoxic a. A is neurotoxic and damages neurons in the following sites (1) Medial temporal lobe structures (2) Frontal cortex especially the entorhinal cortex and hippocampus b. Pivotal role of activated glycogen synthase kinase-3 (GSK) in neurotoxicity of A (1) Activation of GSK causes phosphorylation of A, which in turn, produces (a) Neuronal and synaptic dysfunction (b) Signaling for neuronal apoptosis (2) Phosphorylated A also has a positive feedback on GSK; hence, keeping the cycle of neurotoxicity in motion MN: Activated GSK-3: phosphorylates neurotoxic (3) Initial activation of GSK has been traced to dysfunction within the Wnt (Wingless integration pathway), which is a family of genes normally involved in (a) Neuronal development during embryogenesis (b) Normal neuronal function (4) Normally, the Wnt signaling pathway inactivates GSK; hence, preventing phosphorylation of A and its harmful effect on neurons (5) However, if the Wnt signaling pathway is dysfunctional, GSK remains activated leading to phosphorylation of A and it neurotoxic effects (e.g., apoptosis of neurons) MN: c. A also deposits in the wall of cerebral vessels. Important in producing amyloid angiopathy (see below) d. A stains positive with Congo red and has apple-green birefringence with polarization (refer to Chapter 3). e. A is a metabolic product of amyloid precursor protein (APP) MN: (1) APP is normally coded for on chromosome 21. (2) Defects in metabolism of APP by secretases cause an increase in A. (3) -Secretases cleave APP into fragments that cannot produce A. MN: Secretases: -secretases followed by - secretases cleave APP to produce A (4) -Secretases followed by -secretases cleave APP into fragments that are converted to A. (5) In the sporadic early onset type of AD, apolipoprotein gene E, allele 4 codes for a product that cannot eliminate A leading to early onset of neurotoxicity. MN: Insulin degrading enzyme: involved in clearance of A f. Insulin degrading enzyme (1) Involved in the clearance of A. (2) Insulin resistance syndromes (type 2 diabetes; metabolic syndrome) have increased risk for AD, because increased insulin, lowers insulin degrading enzyme, which increases A. MN: Apo gene E, allele 4: codes for product with high affinity for A; sporadic early onset AD 3. Role of Tau protein in AD a. Normal function is to maintain microtubules in neurons. Assembles and supports scaffolding important in neuron structure and function b. Activated GSK enhances hyperphosphorylation of Tau protein MN: Activated GSK-3: hyperphosphorylates Tau protein (1) This cause the protein to change shape and cluster into fibers (2) Fibers appear as neurofibrillary (NF) tangles (twisted fibers) in the cytoplasm Best visualized with silver stains MN: NF tangle: hyperphosphorylated Tau protein in neuron (3) NF tangles produce neuronal dysfunction including death of the neuron. (4) Pin 1 enzyme (prolyl isomerase) normally strips excess phosphate molecules from NF restoring it to its original shape; however, in some cases of AD, this enzyme is absent or dysfunctional. MN: PIN 1 enzyme: dephosphorylates hyperphosphorylated Tau protein; deficient in some cases of AD 4. Gross and microscopic findings a. Cerebral atrophy with dilation of ventricles (hydrocephalus ex vacuo) (1) Due to loss of neurons in the temporal, frontal, and parietal lobes (2) Occipital lobe is usually spared. b. Presence of NF tangles in the cytoplasm of neurons (1) Best visualized with silver stains (2) They may occur in other disorders. • Elderly patients without dementia, Huntington’s disease, NiemannPicks MN: AD: density of NF tangles and senile (neuritic) plaques in the brain c. Senile (neuritic) plaques (1) Core of A surrounded by neuronal cell processes containing Tau protein, microglial cells, and astrocytes Located in the gray mater. (2) A stains with Congo red (refer to Chapter 3). (3) Best visualized with silver stains (4) Are also normally present in the brains of elderly people MN: Senile (neuritic) plaques: core of A surrounded by neuronal cell processes with Tau protein d. Amyloid angiopathy (1) A is present in cerebral vessels. (2) Causes weakening of vessels with increased risk for hemorrhage MN: Amyloid angiopathy: risk for cerebral hemorrhage e. Confirmation of Alzheimer’s disease (1) Requires postmortem examination of the brain (2) Must be widespread presence of NF tangles and senile plaques MN: Confirmation of AD: must be made at autopsy 5. Clinical findings a. Prominent early sign is the decline in short term memory b. Another early sign is loss of smell Dysfunction in entorhinal cortex c. Patients with mild to moderate disease only have cognitive defects d. Additional deficits accumulate including changes in behavior, judgement, language, and abstract thought MN: AD: prominent early sign is decline in short term memory e. Even later in the course, functional deficits manifest in the patient not being able to care for themselves. f. No focal neurologic deficits are present early in the disease. g. Patients usually die of an infection. • Example—intercurrent bronchopneumonia 6. Presumptive diagnosis is made with mental status testing; tests for MN: AD: presumptive diagnosis with mental status testing; rule out all other causes of dementia a. Orientation b. Attention c. Verbal recall d. Language e. Visual-spatial skills 7. Positron-emission tomography (PET) is useful the differential of dementia 8. Treatment a. Cholinesterase inhibitors Increase synaptic transmission b. Memantine (blocks NMDA glutamate receptors) QUESTION 10 (Page 642 has question, page 657 has discussion) A 9-month-old girl has an infection on her face that began as erythematous macules. She later develops pustules that rupture and cause honey-colored crusted lesions. The girl's 5year-old brother develops similar lesions. Which of the following is the causal agent? A. B. C. D. E. Staphylococcus aureus Herpes simplex virus type 1 Malassezia furfur Propionibacterium acnes Trichophyton rubrum A (Staphylococcus aureus) is correct. The child has impetigo, which causes honeycolored crusted lesions that cover shallow ulcerations of the skin. Staphylococcus aureus is the most common cause of this superficial skin lesion. Streptococcus pyogenes is the second most common cause of impetigo. Impetigo is highly contagious, which explains why the child's brother develops similar lesions. B (herpes simplex virus type 1) is incorrect. Herpes simplex virus type 1 produces vesicles and pustules on the vermilion border of the lip. It does not produce honeycolored crusted lesions on the face. C (Malassezia furfur) is incorrect. M. furfur, a superficial dermatophyte, causes tinea versicolor and seborrheic dermatitis (dandruff). It does not produce honey-colored crusted lesions on the face. D (Propionibacterium acnes) is incorrect. P. acnes is an anaerobe involved in producing the inflammatory reaction associated with acne vulgaris. It does not produce honeycolored crusted lesions on the face. E (Trichophyton rubrum) is incorrect. T. rubrum, a superficial dermatophyte, causes tinea corporis (body), tinea cruris (groin), and tinea pedis (foot). It does not produce honeycolored crusted lesions on the face. QUESTION (I do not know where this question is) Picture of 1-Antitrypsin deficiency Which of the following clinical disorders is most compatible with the distribution of affected patients shown in this pedigree? A. B. C. D. E. 1-Antitrypsin deficiency Hemophilia A Sickle cell trait Type 2 diabetes mellitus Vitamin D–resistant rickets DISCUSSION OF QUESTION 35 Option A (1-antitrypsin deficiency) is incorrect. 1-Antitrypsin deficiency is an autosomal dominant (codominant) disorder that involves a defect in either the synthesis of 1-antitrypsin in the liver or its secretion from the liver. In co-dominant disorders, both alleles express themselves. The pedigree does not show this inheritance pattern.