ELSEVIER
Safety Science 2 1 ( 1996) 247-254
Falls from buildings and other fixed structures in
New Zealand
Sean M. Buckley, David J. Chalmers
Injury
Prevention
Research
Unit (IPRU),
Uniuersi~
Depuriment
of Otago.
P.O.
ofPreuentiue
Box 913, Dunedin,
*,
John D. Langley
und So&l
Medicine,
Me&cd
School,
New Zeulund
Abstract
Epidemiologic
studies of falls from buildings and other fixed structures have historically
focused on the urban environment. In this study, national injury mortality and hospitalisation data,
supplemented by Coroner’s investigation reports, were used to describe the epidemiology of such
falls across an entire nation, New Zealand. The overall death rate was 0.30 per 100,000 persons
per year. Ninety-three percent of cases were older than 14 years of age. Sixty-nine percent of falls
were from buildings, with 3 1% from other structures. Sixty-seven percent of fatal falls were from
a height of 10 meters or less. The incidence rate of hospitalisations
was 21.4, with the highest
rates among those aged O-9. Fifty-five percent of non-fatal falls were from buildings, with 45%
from other structures. National measures to prevent falls from structures should extend to a wide
variety of structures and environments.
Data presented on the age distributions of falls from
different types of structures and structural components (windows, etc.) provide indicators for fall
prevention.
Keywords: Structures;
Heights; Falls; Injuries; Epidemiology
1. Introduction
Epidemiologic studies of falls from buildings and other fixed structures (hereafter
referred to as falls from structures) have historically focused on the urban environment,
’ Corresponding
author
0925.7535/96/$15.00
SSDI
09257535(95)00068-2
0 1996 Elsevier Science B.V. All rights reserved
248
SM. Buckley et al. / Safety Science 2 I (I 996) 247-254
usually New York or Chicago (Baker et al., 1984;Barlow et al., 1983;Bergner et al.,
1971;Lewis et al., 1965;Meller and Shermeta, 1987;Ramos and Delany, 1986;Reynolds
et al., 1971;Sieben et al., 1971;Smith et al., 1975). These studies, all but one of which
examined falls in the aforementioned
cities, have identified falls from structures as a
substantial and preventable cause of mortality due to injury among urban dwellers,
particularly among children. In the only previous nationwide study (US) of falls from
structures (Baker et al., 19841, the data show that although the rate (per 100,000
population) of fatal falls in the largest US cities is approximately double that in other
parts of the US, the number of falls in those cities comprise less than one-third of all
fatal falls from structures in the nation. This study, by Baker et al., was limited to the
demographic parameters of fatal falls.
The purpose of this study was to describe the demographics as well as the circumstances of both fatal and non-fatal unintentional
falls from structures in an entire nation,
New Zealand. Suicides and other intentional falls were excluded from this study.
2. Method
2.1. Mortaliry
There were two sources of mortality data. One was the New Zealand
Health
Information Service’s (NZHIS) injury mortality data files for the period 1 January 1977
to 31 December 1986 inclusive. The NZHIS collects data on all deaths in New Zealand.
The data is coded according to the International
Classification
of Diseases (ICD)
“Supplementary
Classification
of External Cause of Injury and Poisoning”
(World
Health Organisation,
1977), commonly referred to as the “E codes.” The NZHIS files
also contain a free text description of the injury event. The E codes categorize injury
events by external cause, including “falls from buildings or other structures” (E code
882) and “falls from ladders or scaffolds” (E code 881). Cases for this study were
selected from each of these E code classifications.
Only falls from scaffolds, however,
were selected from cases classified under E code 881 as the focus of this study was on
fixed structures in the built environment.
The second source of mortality data was
Coroner’s investigative reports held at the Department of Justice in Wellington.
2.2. Hospitalisations
Hospitalisations
were selected from the NZHIS’s 1987 hospitalisation data file. The
NZHIS records data on all public and private hospital discharges in New Zealand.
Variables on the NZHIS hospitalisation
files include E codes, the age and sex of the
injured person, and a free text description of the injury event. Injury diagnoses are coded
according to the ICD Injury and Poisoning codes (World Health Organisation,
1977).
Cases were selected on the basis of E codes, as in the mortality series. Readmissions for
the same injury, identified by a dedicated field in the NZHIS files, were excluded from
the analysis.
SM. Buckley rt ul./ Suj>ty Science 21 (1996) 247-254
249
3. Results
3.1. Mortality
Demographics - Ninety-six fatal falls from structures were identified for the period
1977- 1986. The overall death rate was 0.30 per lOdTOO0 persons per year. The death
rate for males was 0.55, and the rate for females, 0.06.
Nature of injury - The leading categories of injury were head injuries (N = 53) and
multiple injuries (N = 33).
Type of structure fallen from - Sixty-six falls were from buildings. Thirty-six of the
falls from a building were from the building’s roof, 13 were from a balcony, and nine
were from a window. The remaining falls included nine from bridges, eight from
scaffolding, and three from miscellaneous
structures.
Height fallen from - The estimated height fallen from was available in 60 cases
(62%), with an estimated average height of 7.3 meters. Forty of those falls (67%) were
from a height of 10 meters (approximately
two storeys) or less. An additional 15 falls
(55 total - 92%) were from a height of 20 meters or less.
Miscellaneous
circumstances
Alcohol involvement
was indicated in 13 cases,
with seven persons having measured BAC’s of greater than 80 mg/lOO ml. The most
frequently specified injury event place of occurrence was industrial place or premises
(N = 41, 21 of which were construction sites), followed by home (N = 26), and public
building (N = 11). Forty-two cases were work-related according to data contained in the
Coroner’s files.
3.2. Hospitalisations
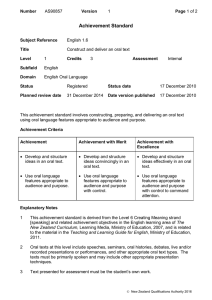
Demographics - The NZHIS hospitalisation file for 1987 contained records for 699
first admissions to hospital for injuries sustained in a fall from a structure. The overall
incidence rate was 21.4 hospitalisations
per 100,000 persons per year. The incidence rate
for males was 32.8. The incidence rate for females was 10.3. Age-specific incidence
rates are displayed in Fig. 1. The highest incidence rates were in the O-4 and 5-9 age
groups.
Nature of injury - The leading types of injuries were head injuries (intracranial
injuries and skull fractures) (29.4%), upper limb fractures (2 1.7%), lower limb fractures
(20.6%), and spine and trunk fractures (13.4%). Among those O-4 years of age, the
proportion of injuries that were intracranial
injuries was 2.9 times greater than the
comparable proportion among all older persons.
Type of structure fallen from Three hundred and eighty-five falls were from
buildings (55.1%). Of these, 41.6% were from a roof, 28.3% were from a balcony, patio,
verandah, etc., and 16.6% were from a window. Among those who fell from a roof, five
percent were O-4 years of age. Among those who fell from a balcony or window, 43.1%
and 42.2%, respectively, were O-4 years of age. Fig. 2 summarizes the age distribution
of falls from roofs, balconies, and windows.
Two hundred and forty falls (34.3%) were from miscellaneous
structures. Among
these there were 136 falls from fences and walls. Seventy percent of those who fell from
XM. Buckley et ol./Sujdy
250
Science 21 (1996) 247-254
I----MALE
EP
RO
3o
A;
20
-"FEMALE
TL 10
EA
ST
0
0 to5 to IO I5 26 25 30 35 (0 45 W 55 60 65 70 75 10 S5
49tOtototaklbtot!Jtotatntototntab
14 19 16 19 36 39 66 69 56 59 66 69 ?I 79 aI 89
AGE GROUP
Fig. I. Falls from buildings
males and females.
and other fixed structures
resulting in hospitalisation
-
Age specific incidence for
fences and walls were under 15 years of age. There were also 74 falls from scaffolds
(10.6%). Eighty-six percent of those who fell from scaffolds were 15 years of age or
older. The remaining falls in the miscellaneous category were from a wide variety of
structures including bridges, poles, wharves, tanks, silos, etc.
Miscellaneous circumstunces Forty-three percent of falls occurred at home
(N = 302). Fifteen percent occurred at industrial places or premises (IV = 104), the
second most frequently specified place of occurrence. The data indicated that 50 of the
latter falls occurred at construction sites. The data also indicated that approximately
15-25% of all 699 cases were work-related, with 25-30% of falls from roofs and
85-90% of falls from scaffolds being work-related. These figures are approximate
because there was no specific field in the data indicating whether cases were work-re-
N
U
;
50
45
E 4o
R 35
30
0 25
F 20
15
C
A lo
s
5
S
--BALCONIES
.--.WINUOWS
0 5 10 IS 1 15 30 35 60 65 50 55 60 65 70 75 60
totnbtoto~tntototntob0b~~~
6 9 16 19 24 29 16 39 66 69 i( 59 61 69 74 79 65
AGE GROUP
Fig. 2. Falls from buildings and other fixed stmctures
from roofs, balconies, and windows.
resulting
in hospitalisation
-
Age distribution
of falls
SM. Buckley et ul./ .%@ty Science 21 (19961247-254
lated. It was possible, however, to assess work-relatedness
by examining
description, place of occurrence, and victim occupation fields for each case.
251
the event
4. Discussion
4.1. Notable jindings
A substantial proportion of fatal falls were from a height of two stories or less.
Among previous studies reporting height data (Barlow et al., 1983;Lewis et al.,
1965;Meller and Shermeta, 1987;Ramos and Delany, 1986;Reynolds et al., 1971;Smith
et al., 19751, most fatal falls have been reported to be from a height of two stories or
higher. (Note: The present discussion of height concerns fatal falls only; virtually no
height data were available for the hospitalisation
series.)
The markedly different finding in this study concerning height fallen from can be
explained as follows. First, three of the previous studies reporting data on height
(Barlow et al., 1983;Meller and Shermeta, 1987;Smith et al., 1975) examined paediatric
falls only. Children, being lighter and more resilient than adults, are less likely to die
from a fall of two stories or less. Second, the other three studies reporting height data
(Lewis et al., 1965;Ramos and Delany, 1986;Reynolds et al., 1971) which included falls
among persons of all ages, examined a mixture of unintentional
and intentional falls.
Obviously, people trying to commit suicide rarely jump from a height of two stories or
less. Third, all of the aforementioned
studies have examined urban falls only. The
preponderance
of residences and other buildings exceeding two stories in New York
City and Chicago naturally skews the distribution
of structures from which falls
occurred.
Another notable finding of this study was that a substantial proportion of both fatal
and non-fatal falls from structures involved structures other than buildings. These
included a variety of miscellaneous structures such as fences, walls, tanks, and silos. The
emphasis of previous studies of falls from structures has been on falls from high-rise
buildings.
An implication of these findings is that national measures to prevent falls from
structures should extend to all buildings including single family homes and, in addition,
structures other than buildings.
4.2. Prevention
Falls from windows One peak in the age distribution of non-fatal falls from
windows (Fig. 2) occurred in the O-4 age group. The New Zealand Code ofpracticefor
Safer House Design (New Zealand Standard, 1990), a national building standard,
includes a provision (9.5.4) designed to prevent childhood falls from upper-level
windows. It states that “upper level windows that allow a clear opening of over 100 mm
square, where the sill is under 1200 mm from the floor, should be fitted with removable
security stays for child safety.” Such a method of preventing falls from windows among
children met with success in New York City, where a law was passed requiring
252
SM. Buckley et ul./Sujhy
Science 21 (1996) 247-254
landlords of high-rise dwellings to provide window guards (Barlow et al., 1983). Health
education efforts making parents aware of the potential fall hazard of windows, and how
such falls could be prevented, were also shown to be effective in New York City
(Spiegel and Lindaman, 1977). Another peak in the age distribution of non-fatal window
falls occurred among those aged 15-29. Among fatal falls from windows, most occurred
among those 15 or older. Many falls among older persons could be prevented by making
windows difficult to fall through by reducing their size, modifying their placement, or
by the interposition of screens or other barriers. The windows must still be usable for
emergency egress, however. Architects, engineers, and ergonomists should incorporate
fall prevention considerations
into the design of windows.
Fulls frombalconies - As with falls from windows, peaks in the age distribution of
those who sustained non-fatal falls from balconies were found at O-4 and 15-29 years
of age. Falls among those O-4 years of age can be prevented by providing railings on all
kinds of balconies (i.e., verandas, patios, terraces, sundecks, etc.), and by making the
railings difficult to climb, and with openings too small for a child to pass through. Falls
among older persons can be prevented by providing railings and by making them high
enough that overbalancing
is unlikely. The New Zealand Code of Practice for Safer
House Design (New Zealand Standard, 1990) includes a provision (2.8.1) requiring
railings at least 900 mm high around exterior decking and balconies over 1200 mm
above the ground. The railings must be detailed to prevent climbing and have openings
not exceeding 80 mm.
Fulls from roofs - Most falls from roofs, both fatal and non-fatal, occurred among
persons 15 years of age and older. Many of these falls were work related. Work related
falls from roofs can be prevented by use of safety nets or platforms, safety belts, guard
rails, and by the use of temporary surfaces and walkways for roofs under construction
(International
Labour Organisation,
1983). Twenty-nine
percent of non-fatal falls from
roofs occurred among those 0- 14 years of age. Limiting structural access to roofs (by
way of windows, ledges, etc.) could prevent some of these falls.
Fulls on construction sites and from scufsolds A substantial proportion of fatal
falls, and a smaller proportion of non-fatal falls, occurred at construction
sites. The
majority of falls from scaffolds occurred at construction sites. Falls at construction sites
1986) and falls from scaffolds in the US (Scaffold
in New Zealand (Anonymous,
Industry Association,
1978) have been identified as a serious injury problem. The
occupational safety community has given considerable attention to methods of preventing falls at construction sites. The large variety of prevention strategies available to the
safety practitioner and others will not be addressed here. For more information,
the
reader is referred to the Encyclopaedia of Occupational Health and Safety (International
Labour Organisation,
1983) as a starting point.
Fulls from fences and walls Most falls from fences and walls occurred among
children. Most of these children were probably climbing or simply playing when they
fell. Limiting access to the tops of outdoor walls (e.g., earth retaining walls) could
prevent some of these falls. Preventive measures identified above for balconies may also
be applicable to fences and walls.
Fulls from other structures - In general, structures on or in which people must work
should be designed with consideration given to the prevention of falls. Designs should
S.M. Buckley et al./Safety
Science 21 (1996) 247-254
253
include slip-resistant surfaces, ergonomically designed handholds, and railings and other
barriers. In addition, measures should be taken to prevent access to such structures by
unauthorized persons. Power poles, for example, should be designed so that they cannot
be climbed without special equipment.
In closing it is noted that falls from structures is a complex problem and cannot be
addressed by the public health sector alone. In the spirit of the Ottawa Charter for
19861, diverse but complementary
Health Promotion (World Health Organisation,
efforts, including efforts from outside the public health sector, are needed to adequately
address the problem. In New Zealand, a notable example of such a measure is the Code
of Practice for Safer House Design which addresses the problem of domestic falls while,
moreover, addressing domestic safety as a whole. It was developed by people of diverse
backgrounds including engineers, architects, and health professionals, and was publicly
promoted by the New Zealand Accident Rehabilitation
and Compensation
Insurance
Corporation, an injury compensation organization. It will be implemented by builders as
enforced by appropriate regulatory bodies. The Code, however, addresses residences
only, and much more work remains to be done in New Zealand and elsewhere to prevent
unintentional
falls from buildings and other structures.
Acknowledgements
This paper was prepared under contract to the New Zealand Accident Rehabilitation
and Compensation Insurance Corporation. The authors are grateful to the New Zealand
Health Information Service for the provision of data.
The advice and assistance of the following persons is gratefully acknowledged. Dr.
Barry Borman, Mr. Jim Dearsly, Ms. Maree Drury, Ms. Avery Jack, Mr. Craig Leahy,
Dr. Barbara Lovie, Dr. Robyn Norton, Ms. Val O’Sullivan, Mr. Ian Shepherd, and Dr.
Philip Silva.
This research was funded by the New Zealand Accident Rehabilitation and Compensation Insurance Corporation. The Injury Prevention Research Unit is funded jointly by
the latter and the New Zealand Health Research Council.
References
Anonymous,
1986. Falls: biggest killer on construction.
Labour and Employment
Gazette, 36(4): 17-2 I.
1984) p.
Baker,S.P.,O’Neill, B. and Karpf, R.S., 1984. The Injury Fact Book (Lexington Books, Lexington,
Barlow, B., Niemirska, M., Gandhi, R.P. and Leblanc, W., 1983. J. Ped. Surgery, 18:509-51 I.
Bergner, L., Mayer, S. and Harris, D., 1971. Falls from heights: A childhood epidemic in an urban area. Am.
J. Public Health, 61:90-96.
International Labour Organisation,
1983. Encylopaedia of Occupational Health and Safety.
Lewis, W.S., Lee, A.B. and Grantham, S.A., 1965. Jumpers syndrome. J. Trauma, 5:812-818.
Meller, J.L. and Shermeta, D.W., 1987. Falls in Urban Children. Am. J. Dis. Child., 141: 1271-1275.
Ramos, S.M. and Delany, H.M., 1986. Free falls from heights: a persistent urban problem. J. Nat. Med. Ass..
78(2): I I I-l 15.
Reynolds, B.M.. Balsano, N.A. and Reynolds, F.X., 1971. Falls from heights: a surgical experience of 200
consecutive cases. Ann. Surgery, 174:304-308.
2.54
S.M. Buckley ef al./Sajdy
Science 21 (1996) 247-254
Scaffold Industry Association,
1978. Survey of scaffold accidents. Scaffold Industry Association,
14039
Sherman Way, Van Nuys, CA. Undated, circa 1978.
Sieben, R.L., Leavitt, J.D. and French, J.H., 1971. Falls as childhood accidents: An increasing urban risk.
Pediatrics, 47:886-892.
Smith, M.D., Burrington, J.D. and Woolf, A.D., 1975. Injuries in children sustained in free falls: An analysis
of 66 cases. J. Trauma, 15:987-991.
Spiegel, C.N. and Lindaman, F.C., 1977. Children can’t fly: a program to prevent childhood morbidity and
mortality from window falls. Am. J. Public Health, 67: 1143-l 147.
New Zealand Standard,
1990. Code of practice for safer house design (New Zealand Standard 41021.
Wellington: Standards Association of New Zealand, 1990.
World Health Organisation. 1977. International classification of diseases. Geneva: World Health Organisation,
1977.
World Health Organisation,
1986. The Ottawa charter for health promotion. Geneva: World Health Organisation. 1986.