Knowledge Discovery from Massive Healthcare Claims Data
advertisement

Knowledge Discovery from Massive Healthcare Claims
Data
Varun Chandola
Sreenivas R. Sukumar
Jack Schryver
Oak Ridge National
Laboratory
Oak Ridge National
Laboratory
Oak Ridge National
Laboratory
chandolav@ornl.gov
sukumarsr@ornl.gov
schryverjc@ornl.gov
ABSTRACT
a major contributor to the high national debt levels that are
projected for next two decades. In 2008, the total healthcare
spending in US was 15.2% of its GDP (highest in the world)
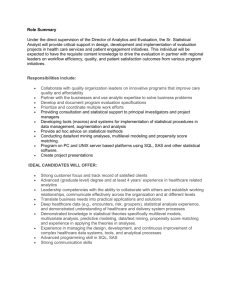
and is expected to reach as much as 19.5% by 2017 [2]. But
while the healthcare costs have risen (by as much as 131%
in the past decade), the quality of healthcare in the US has
not seen comparable improvements (See Figure 1) [24].
The role of big data in addressing the needs of the present
healthcare system in US and rest of the world has been
echoed by government, private, and academic sectors. There
has been a growing emphasis to explore the promise of big
data analytics in tapping the potential of the massive healthcare data emanating from private and government health
insurance providers. While the domain implications of such
collaboration are well known, this type of data has been
explored to a limited extent in the data mining community.
The objective of this paper is two fold: first, we introduce the
emerging domain of “big” healthcare claims data to the KDD
community, and second, we describe the success and challenges that we encountered in analyzing this data using state
of art analytics for massive data. Specifically, we translate
the problem of analyzing healthcare data into some of the
most well-known analysis problems in the data mining community, social network analysis, text mining, and temporal
analysis and higher order feature construction, and describe
how advances within each of these areas can be leveraged
to understand the domain of healthcare. Each case study
illustrates a unique intersection of data mining and healthcare with a common objective of improving the cost-care
ratio by mining for opportunities to improve healthcare operations and reducing what seems to fall under fraud, waste,
and abuse.
Figure 1: Life expectancy compared to healthcare
spending from 1970 to 2008, in the US and the next
19 most wealthy countries by total GDP [14].
Categories and Subject Descriptors
Experts agree that inefficiencies in the current healthcare
system, resulting in unprecedented amounts of waste, is the
primary driver for the discrepancy between the spending and
the returns in the healthcare domain [11]. Recent studies
estimate that close to 30% (∼ $765 billion in 2009) of total
healthcare spending in United States is wasted, which in
turn is caused by many factors such as unnecessary services,
fraud, excessive administrative costs, and inefficiencies in
the healthcare delivery.
In recent years, several experts as well as the federal government1 have stressed on the role of big data analytics in
addressing the issues with healthcare. The 2011 report by
Mckinsey Global Institute [19] estimate that the potential
value that can be extracted from data in the healthcare sector in US could be more than $300 billion per year. The
same report lists out several areas within the healthcare sector which can benefit from using big data analytics. These
include segmentation of patients based on their health profiles to identify target groups for proactive care or lifestyle
H.2.8 [Database Management]: Database Applications—
Data Mining
Keywords
Healthcare Analytics; Fraud Detection
1.
INTRODUCTION
Healthcare spending in United States is one of the key
issues targeted by policy makers, owing to the fact that it is
(c) 2013 Association for Computing Machinery. ACM acknowledges that this contribution was authored or co-authored by an employee, contractor or affiliate of the
United States government. As such, the United States Government retains a nonexclusive, royalty-free right to publish or reproduce this article, or to allow others to do so,
for Government purposes only.
KDD’13, August 11–14, 2013, Chicago, Illinois, USA.
Copyright 2013 ACM 978-1-4503-2174-7/13/08 ...$15.00.
1
http://www.whitehouse.gov/sites/default/files/
microsites/ostp/big_data_press_release_final_2.pdf
1312
changes, development of fraud resistant payment models,
creating information transparency and accessibility around
healthcare data, and conducting comparative effectiveness
research across providers, patients, and geographies.
Healthcare insurance claims have the potential of answering many of the questions currently faced by the healthcare
sector, In fact, until shareable electronic health records become a reality, healthcare claims, especially from organizations with a large spatial and demographic coverage such,
which is the case with many of the government run health
insurance programs in the country, are the most reliable resource for understanding the current healthcare landscape,
from conditions, care, and cost perspective. But the transactional format of claims data is not amenable for advance
analytics that the state of art KDD methodologies have to
offer. In this paper we explore transformations of the healthcare claims data which bridge this gap between the healthcare domain and modern data analytics.
We present a study of big data analytics on health insurance data collected by a large national social health insurance program. While previous efforts have used data
mining methods for analyzing healthcare claims data within
small organizations, we believe that this is one of the first instances where advanced data analytics and healthcare have
interacted at a national scale. In all, we approximately analyzed 2 billion insurance claims for approximately 45 million
beneficiaries and over 3 million healthcare providers.
1.1
Figure 2: Different Types of Healthcare Data
the data for payment errors [12]. Limited efforts exist that
have analyzed the healthcare claims data to understand the
inefficiencies in the healthcare system [6], but from the analytics perspective they are limited to simple summary statistics such as population means for various demographics. In
this paper we explore the application of three advanced KDD
technologies, viz. , text mining [18], social network analysis
[29], and time series analysis [20], all of which have been successful in a variety of applications but have not been applied
at a large scale to healthcare claims data.
Domains such as credit card and property insurance have
long studied the issue of fraud identification [4, 10]. But
healthcare fraud detection has unique characteristics given
that the actual beneficiary is typically not the fraud perpetrator, which is not the case for other domains. So existing
fraud detection methods cannot be directly applied to the
healthcare domain. Most of the existing fraud detection solutions in the healthcare domain are not public, primarily
because of the fact that the data is highly sensitive and is
usually not made available for research and publishing.
Our Contributions
In this paper, we make the following contributions:
1. We introduce the emerging domain of health care claims
data and identify multiple research problems that can
be solved using the existing big data analytics solutions.
2. We propose three transformations of the transactional
claims data which enables application of state of art
KDD methodologies in this domain.
3.
3. We present several approaches to identify and understand the fraud, waste, and abuse in the health care
system. The potential of each proposed approach is
demonstrated on real claims data and validated using
a true set of fraudulent providers.
4. We highlight the unique nature of healthcare data when
analyzed using methods such as social network analysis and text analysis.
2.
BACKGROUND
Healthcare data can be broadly categorized into four groups
(See Figure 2): Clinical data (patient health records, medical images, lab and surgery reports, etc.) and patient behavior data (collected through monitors and wearable devices) provide an accurate and detailed view of the health of
the population. But such data, which is increasingly being
stored electronically, can be leveraged in a big data setting
only when the owners (doctors, hospitals, and individuals)
share, which, owing to privacy concerns is still limited to
being analyzed within an organization such as a hospital or
a network of hospitals. Pharmaceutical research data
(clinical trial reports, high throughput screening results) often face privacy concerns owing to business practices. In
this paper, we focus on health insurance data, which has
been collected and stored for several years by various health
insurance agencies. While the primary justification for this
data is to track payments and address fraud, such data also
has great potential to address some of the other aforementioned issues of the healthcare system. For United States,
such data is extremely valuable, given that around 85% of
Americans use some form of insurance (private or government). Moreover, insurance data is the only source of the
cost associated with healthcare which is vital to address the
RELATED WORK
The role of big data in healthcare has been well acknowledged across government and industrial sectors23 . But only
a few published studies have analyzed such data [12]. The
primary reason is the data availability, given that the healthcare claims data has strong proprietary and privacy requirements4 . Moreover, existing studies have considered claims
data from a payment system perspective and have analyzed
2
www.eweek.com/database/emc-says-big-data-isessential-to-improving-health-outcomes/
3
www.intel.com/content/dam/www/public/us/en/
documents/white-papers/healthcare-leveragingbig-data-paper.pdf
4
http://www.hhs.gov/ocr/privacy/
1313
economic challenges associated with modern healthcare system. The strong challenge presented by insurance data on
the other hand is that it is not readily in the form to infer
strong analytic insights into healthcare, besides the payment
model. A key contribution of this paper is the transformation of the insurance data into formats that allow application
of existing analytic tools for knowledge discovery.
3.1
Speciality
~600
Providers
~4 M
Health Insurance Data
Diagnoses
~17 K
Beneficiaries
~50 M
~8 K
Figure 3: Entities and relationships in healthcare
claims data along with approximate number of entries in each entity set.
of double payments for duplicate claims, payments using
an outdated fee schedule, etc. A major cause for abuse is
due to the fact that programs such as Medicare follow a
prospective payment system for hospital care, which means
that providers are paid for services at predetermined rates.
Thus if the actual service costs more than the allowed cost,
the provider has to cover its losses. If the actual service
costs less than the allowed cost, the provider keeps the remainder. This drives the providers to charge unnecessary or
more expensive services (also known as upcoding) by making
more severe diagnosis to safeguard against any losses and to
make profit. Some of the examples listed above, e.g., double
payment for duplicate claims, can be identified by applying
business rules to the data. For others, such as upcoding or
miscoding providers, there is need for advanced algorithms
that can analyze the vast amounts of claims data.
In the subsequent sections we describe three case studies that were conducted onhealthcare claims and associated
data. The common thread among the studies is the analysis
of the behavior and interaction between healthcare providers,
which is highly important given that they are the primary
drivers for the wasteful spending in the system.
1. Claim information captures the information about the
service transaction including the nature of the service
and the cost.
2. Patient enrollment and eligibility data that captures
demographic information about the patients (or beneficiaries of the system) and their eligibility for different
services.
3. Provider enrollment data that captures the information about the physicians, hospitals, and other healthcare providing organizations.
Health Insurance in United States
In the US, approximately 85% of the population has some
of form of health insurance. Majority of these individuals (≈
60%) obtain insurance through their employer or employer
of parent or spouse. Almost 28% of population (83 million
individuals) is covered under government health insurance
programs. These include programs such as Medicare, Medicaid, Veterans Health Services, etc.
The data managed by each of these programs is at a massive scale. Medicare alone provides health insurance to 48
million Americans and covers for hospitalization, out patient, medical equipments, and drugs. There are a few million providers enrolled with the Medicare Provider Enrollment, Chain, and Ownership System (PECOS). In 2011,
Medicare received close to 1.2 billion claims (4.8 million
claims per day) for their fee for service programs. An almost
equivalent number of claims were received in the prescription drugs program (also known as Part D). Under Medicaid, more than 60 million individuals received benefits in
2009 (one in every five). In the state of Texas alone, there
are more than 0.5 million providers within Medicaid.
4.
~50 K
Procedures
The typical health insurance payment model is a Fee-forservice (FFS) model in which the providers (doctors, hospitals, etc.) render services to the patients and are paid
for each service by the payor or the insurance agency. The
providers record the details of each service, including the
cost and justification and submit the record to the payor.
The payor decides to either pay or reject the claim based on
the patient’s eligibility for the particular service which are
determined by the policy guidelines.
The insurance agency typically maintains three types of
data for their operations:
3.2
Drugs
5.
DATA
The data used for the subsequent case studies captures
three different aspects of healthcare. First is the claims
data for close to 48 million beneficiaries for the entire US.
Second is the provider enrollment data which can be
obtained from several private organizations. The third is a
list of fraudulent providers that have been sanctioned for
fraudulent behavior in the state of Texas. The list of fraudulent providers was obtained from the Office of Inspector
General’s exclusion database5 . Note that in this paper we
will treat the rest of the providers as non-fraudulent for evaluation, even though it is evident that there are a significant
number of fraudulent actors who have not been identified.
The claims and the provider enrollment data comes from
transactional data warehouses. Each claim, consists of several data elements with information about the beneficiary,
provider, the health condition (or diagnosis), the service provided (procedure or drug), and the associated costs. Figure
3 shows the different entities and their relationships that
are present in the healthcare claims data. Note that the
providers typically are affiliated to each other through orga-
CHALLENGES AND OPPORTUNITIES
As mentioned in Section 1, fraud, waste, and abuse form
a significant amount of healthcare spending. Fraud ranges
from single providers billing the system for services that were
not provided to large scale fraud carried out by organized
criminals [27]. One form of waste happens due to improper
payments, since organizations are mandated to process payments in a short duration of time, resulting in authorization
5
https://oig.hhs.gov/exclusions/exclusions_list.
asp
1314
nizations such as hospitals. This information and additional
data about the providers is present in the provider data.
6.
LARGE SCALE TEXT ANALYTICS
Simply stated, the two ultimate goals necessary to address rising healthcare costs are: 1). a healthy population,
and 2). optimal healthcare in terms of cost and quality. To
reach these goals, the first vital step is to understand the
current landscape in terms of prevalent diseases and the resulting treatments and costs. Identifying the key disease
profiles for patients will allow segmentation of the population into groups which can then be targeted for proactive
care or lifestyle changes. For providers, typical treatment
profiles used by doctors and hospitals will be instrumental in identifying the costly areas which need to addressed
through policy changes or medicinal research. Moreover,
such profiles can also be used to compare providers across
the country and potentially across organizations to identify
fraudulent (upcoding) or wasteful providers.
In the first case study, we show how such profiles can be
generated from the claims data (See Figure 3) using advanced text analytic solutions [18]. Text data, especially
from the web domain, has been the foremost target of the big
data paradigm and a host of open-source solutions (Apache
Hadoop based Mahout library [8], MADlib for parallel databases
[9]) exist for deploying text mining algorithms on massive
text data sets. The interaction between text mining and
healthcare, for obvious reasons, has been in analyzing the
text available within the patient health records (clinical data)
[25]. But these solutions have never been applied in the context of healthcare claims data.
6.1
Representing Entities as Documents
To capture the behavior profiles of the providers and beneficiaries we construct several sparse matrices from a temporal aggregate of claims data, as follows:
Let the set of providers be denoted as P , set of beneficiaries be denoted as B, set of procedures as C, set of diagnoses as G, and set of drugs as D. Let the symbol XY
denote a matrix with X ∈ {B, P } representing rows and
Y ∈ {G, C, D} representing columns. For example, the matrix PG (providers vs. diagnoses) captures the nature of
diagnoses that a doctor assigns to patients. Each cell P Cij
in the matrix PC denotes the number of times the provider
Pi ∈ P uses the procedure Ci ∈ C in the given time frame.
Each of matrices thus created can be viewed as a documentterm matrix with providers/beneficiaries as documents and
drugs/procedures/diagnoses as terms. Such representation
opens up the claims data to a wide spectrum of existing text
analysis methods [18]. Given that multiple document-term
matrices can be generated for the same entity (providers),
it also allows application of methods that deal with learning
from multiple views [16].
6.2
Profiling Providers
In this study we used topic modeling using Latent Dirichlet Allocation (LDA) [5] as our text analysis tool. LDA is a
probabilistic topic model which is widely used for determining hidden topics in a set of documents. In the LDA model,
each document (provider) is represented as a mixture of a
fixed number of hidden topics and each topic is a probability
distribution over a vocabulary of words (diagnosis codes).
1315
Figure 4: Relative proportion of fraudulent and nonfraudulent providers assigned to each topic of diagnosis codes.
We applied the Mahout implementation of collapsed variational Bayesian inference (cvb) algorithm [28] for LDA on
the provider-diagnoses (PG) matrix constructed from a year
of claims data (361,117 providers, 9,378 diagnosis codes,
43,331,004 tuples). The matrix was normalized using tfidf
normalization. Using LDA we identified 20 hidden topics
from the PG matrix.
From healthcare perspective, each topic can be thought
of as a category for providers. While one would expect that
topic driven categorization should closely match the actual
specializations of the providers, we found out that this was
not always the case. While some topics were dominated by
diagnoses that belonged to same area of medicine (e.g. , oncology, ophthalmology), there were other topics which were
made up of diagnosis codes that are seemingly different from
each other. For example, one topic consisted of diagnosis
codes associated with Diabetes as well as dermatoses (skin
condition). While this might appear surprising, further research revealed a medicinal connection between the two [17].
Another possible application of the topic modeling is to
use the topic distributions as features or profiles for the
providers. To validate the discriminatory potential of topic
distributions we conducted the following analysis. For each
provider, we chose the topic with highest probability assigned by LDA. We then compared the proportion of fraudulent and the non-fraudulent providers (using the list of fraudulent providers as described in Section 5) that fall under each
topic. The relative proportions are shown in Figure 4.
The non-fraudulent providers are evenly distributed across
most topics, except for the topic 19. This particular topic
is composed of “generic” diagnoses such as follow-up surgery
and benign tumor and hence is expected to represent a large
number of providers. For the fraudulent providers, the distribution follows the non-fraudulent providers, except for
topic 5, which represents close to 25% of all fraudulent providers
as opposed to only 7% of non-fraudulent providers. Topic 5
is dominated by very distinct diagnosis codes.
From the domain perspective, this discovery is valuable
since it identifies the diagnosis codes that are used by same
providers and have historically been targets of fraud. Given
the fact that the codes in topic 5 are medicinally distinct
from each other, such discovery can only be made by methods that allow all diagnosis codes to be related to each other,
i.e. , topic models.
The promising findings in Figure 4 show that analyzing
claims data using text mining methods can reveal very in-
teresting interactions and patterns. Similar analysis can be
conducted for other matrices for additional insights.
7.
SOCIAL NETWORK ANALYSIS
As health insurance companies shift focus from fraud detection to fraud prevention, building a predictive model to
estimate the risk of a provider before making any
claims has been a challenging problem. Furthermore, substantial amount of healthcare fraud is expected to be hidden
in the relationships among providers and between providers
and beneficiaries making insurance claims. In this case study,
we present results of applying social network analysis methods [21] to understand the relationships of providers in the
healthcare system and visualizing features and patterns of
fraudulent behaviors in such a network. We describe the
construction of social-network features and the predictive
model built on those features as a solution to assessing healthcare fraud risk at the time of enrollment.
7.1
Figure 6: Snapshot of the provider network for
Texas. The width of circle at each node denotes
the number of affiliations. The large circles indicate
organizations, such as hospitals. Nodes in red are
fraudulent providers.
Constructing a Provider Social Network
disconnected graphs, the largest network being a network
of a few 100,000 providers and the smallest as little as 3,
and, (iii) the network is constructed based on self-reported
data and inferred data based on subject matter expertise
and may be subject to omissions, errors and quality issues.
Individual
Providers
7.3
Extracting Features from Provider Network
For this particular study, we focus on analyzing the network properties with respect to the fraudulent providers described in Section 5. The objective is to extract multiple features for every node in the network and use them for discriminating between fraudulent and non-fraudulent providers.
We investigated several network based features [21, 23] as
listed in Table 1.
Organizations
Centrality
Figure 5: A Sample Provider Network
Assortativity
Clustering
Providers in the US healthcare system are typically associated with multiple hospitals and health organizations. The
information about the providers can be obtained from multiple sources. Some of such data sources are public6 while
others may be purchased7 . We use data from such sources
to construct a social network in which providers (both individual and organizations) are the nodes. The edges are
between individual and organization nodes (See Figure 5).
A graph when constructed for all providers in the United
States is expected to have nearly 35 million nodes and more
than 100 million edges. In this study we construct a graph
for providers in the state of Texas with almost 1 million
nodes and close to 3 million edges.
7.2
Communities
Components
Cores
Distance Measures
Flows
Link Analysis
Rich Club
Shortest Paths
Vitality
Table 1: Network features studied for the provider
network [21].
Properties of the Provider Network
A snapshot of the provider network for the state of Texas
is shown in Figure 6. This provider network is different
from a typical “social network” in the following ways: (i)
the networks consist of both organizations and individuals.
This introduces a latent hierarchy in the network because
several individual physicians work for organizations and can
also own group practices, (ii) the network is a collection of
6
7
Degree, Closeness, Betweenness, Load
Current Flow Closeness, Communicability
Current Flow Betweenness, Eigenvector
Average Neighbor Degree
Average Degree Connectivity
Triangles, Average Clustering
Square Clustering
K-Clique
Connectivity
Core number, k-Core
Center, Diameter, Eccentricity
Periphery, Radius
Network Simplex
PageRank, Hits
Rich Club Coefficient
Shortest Path
Closeness Vitality
7.4
Relevance for Identifying Fraud
For each feature we estimated its capability to distinguish
between fraudulent and non-fraudulent nodes using the Information Complexity (ICOMP) measure [15] which compares the distribution of the features for the fraudulent and
non-fraudulent populations. The five network based features
that we found to be most distinguishing were: Node degree, Number of fraudulent providers in 2-hop network, Page rank, Eigenvector centrality, and Current-
https://nppes.cms.hhs.gov/NPPES/
http://www.healthmarketscience.com/
1316
flow closeness centrality. Figure 7 shows the distribution of each feature with respect to the fraudulent and nonfraudulent populations.
For instance, the red line in 7(a) indicates the node degree
distribution for providers previously identified as fraudulent.
The blue lines are for a random sample of non-fraudulent
providers. We observe that increase in degree of provider
correlates to a higher risk of fraud. Similar conclusions
can be drawn from analyzing the 2-hop network (See Figure 7(b)). In fact, the chance of finding other fraudulent
providers within the 2-hop network of a fraudulent provider
is ∼40% compared to the chance of finding a fraudulent
provider within the 2-hop network of a random provider
(∼2%).
Given the ability of the above features to distinguish between fraudulent and non-fraudulent providers, we plan to
utilize them within either an unsupervised multivariate anomaly
detection algorithm [7] for automatic detection of such providers
or in a binary classification algorithm that learns from the
available labeled data.
8.
This vector tracks the introduction of new beneficiaries in
the stream of claims submitted by a specific claimant, and
provides a basis for estimating whether a large number of
new beneficiaries were seen by a provider during a particular
time interval. The Bernoulli CUSUM statistics to analyze
this vector are:
St = max (0, St−1 + Lt ), t = 1, 2, . . . ,
(2)
where S0 = 0 and the chart signals if S0 > h. The values of
the log-likelihood scores are
ln 1−p1
1−p0
Lt =
ln p1
p0
TEMPORAL ANALYSIS OF CLAIMS SEQUENCES
In the context of identifying healthcare fraud perpetrated
by providers, two generic response mechanisms are possible:
1). identify and prosecute providers after claims are submitted (pay and chase), and 2). timely denial of payment for
a submitted claim based on the associated risk. Whereas
legal prosecution is expensive, time-consuming and difficult
to wage, a policy of selective denial of payment based on
statistical risk factors is much easier to implement once the
risk estimation algorithms have been developed.
In this case study we use temporal analytics to address the
following two questions: i). How can we identify the transition of a good provider into a bad actor in an online fashion
using the temporal sequence of claims?, and ii). how can
the temporal sequence be used to discriminate fraudulent
providers from others?
We pose the first question as a change-point detection
problem and employ a statistical process control methodology to identify the transition. The strength of this method
is that it can be implemented online to examine each claim
as it enters a processing queue for payment. For the second
question we compare the temporal claim submittal patterns
of every provider to estimated population norms for similar
providers (e.g., by speciality and geographic location) and
define features from these comparisons. Classifiers can subsequently be trained to learn the differences between known
fraudsters and presumed normal providers.
8.1
Suppose we have a time-ordered sequence of claims X =
x1 , x2 , . . . , xn . This sequence could represent all insurance
claims submitted by a single provider over a fixed time interval (e.g., one year). One of the simplest SPC statistics is
the Bernoulli CUSUM [26], where X is simply a vector of
zeros and ones. For example, we can define xi according to
the following:
1
if the ith claim has a new beneficiary number
xi =
0
otherwise
if Xt = 0
(3)
if Xt = 1
A more common form of fraud occurs when providers start
taking patients with conditions different from their past profile. Given that the condition codes can have multiple categories, the above method needs to be generalized to a multinomial case. The multinomial CUSUM statistic [13] can be
applied here as follows:
pi1
when Xt = i
(4)
Lt = ln
pi0
Change-point Detection with Statistical Process Control Techniques
The statistical process control (SPC) literature [20] has
evolved into a fairly mature technology for implementation
of a temporal approach to processing data sequences.
A number of methods have been proposed in SPC theory to monitor processes for exceedance of control limits.
One popular metric is the cumulative sum (CUSUM) statistic [22]. Here we illustrate an application of CUSUM to identify changes in the patient enrollment. A useful assumption
in this approach is that a fraudulent providers often start
“taking” more patients than usual [27].
Where pi1 is the ith alternative hypothesis, and pi0 is the ith
null hypothesis. A typical multinomial/categorical CUSUM
for a “presumed normal” is shown in Figure 8(a). The CUSUM
statistic spikes when the provider uses different condition
codes than the typical, but falls back to 0 since the atypical
behavior is sporadic. On the other hand, Figure 8(b) shows
the CUSUM statistic for an unusual (potentially fraudulent)
physician who uses many condition codes that are not typical for his speciality; the CUSUM statistic captures this
unusual behavior.
A complete set of out-of-control probabilities are selected
for the multinomial CUSUM. In the absence of a specific
alternative hypothesis, a simple method of formulating the
out-of-control probabilities is to assume that every probability reverses direction to become less extreme, i.e., probabilities migrate in the direction of the grand mean. We
specify a proportional change constant to compute the exact probabilities. The alternative hypothesis p0 is then
p1 = p0 + c ∗ (m − p0 ) where c is the proportional constant
and the mean m is simply the reciprocal of the number of
categories.
8.2
Anomaly Detection using CUSUM Statistic
One promising metric for screening anomalies is the maximum value of a CUSUM statistic over a fixed time interval.
However, this statistic is biased by the number of claims
submitted by a provider during that interval. Some outlier providers exhibit continuously anomalous behavior, even
1317
(1)
(a) Node Degree
(b) Fraud in 2-hop Network
(d) Eigenvector Centrality
(c) Page Rank
(e) Current-flow Closeness Centrality
0.8
60
80
80
60
40
20
0
0
Time
Multinomial CUSUM
600
400
300
Diagnosis Code
0.2
100
Diag−Lo
Diag−Hi
multiCUSUM
500
0.6
40
0.0
0.4
20
Multinomial CUSUM
600
200
400
Diagnosis Code
800
700
Diag−Lo
Diag−Hi
multiCUSUM
0
100
1000
800
120
1.0
Figure 7: Distribution of top distinguishing features for fraudulent (red) vs. non-fraudulent providers (blue).
200
400
600
800
Time
(a) Normal Provider
(b) Potentially Fraudulent Provider
Figure 8: Multinomial CUSUM chart to track time ordered condition codes from insurance claims. Green
squares indicate the typical codes and blue squares indicate the atypical codes for the given speciality.
over a large time interval, and their CUSUM statistics often resemble a linear function. This pattern suggests another metric that is not similarly biased by the length of the
claims sequence - the average CUSUM rate. Figure 9 shows
a scatterplot using these metrics for a typical provider population color-coded by speciality. The scatterplot displays
a cornucopia-shaped pattern with the tail originating at the
lowest CUSUM values, and the mouth arcing upward toward the highest CUSUM rates. Anomalies are separated
from the main cluster near the top of the scatterplot. Further analysis is required to determine whether these anomalies are normal in a statistical sense, or whether they are
more likely members of an anomalous cluster. A horizontal
line boundary is drawn at a CUSUM rate of about 0.35 to
suggest a possible division of outliers from normals.
8.3
Temporal Feature Construction
The previous section explored the possibility that a provider
presumed to be normal up to some position within a temporal claims sequence is diverted either temporarily or permanently to anomalous behavior. Additionally we expect that
some providers are either fraudsters from the moment they
1318
Figure 9: Distribution of CUSUM metrics for a
provider population.
1.0
enroll in an insurance program, or that they revert to fraudulent activity permanently at some time before the beginning
of a limited claims sequence. In this case the availability
of provider ground truth affords the analyst an opportunity
to go beyond anomaly detection as a method of identifying
potential bad actors. In particular, if every provider can
be labeled as either “bad actor” or “presumed normal”, we
can discriminate between temporally stable characteristics
of normal and bad actors. Here we assume that providers
naturally cluster into a main normal group and a main bad
actor group. This assumption may only be approximately
correct, especially for the class of bad actors if multiple paths
exist to fraudulent behaviors.
In this section we extract 10 temporal features for each
provider based on their submitted claims. Given the fact
that some of these features might “help” real providers
to adapt and avoid future identification, we are not
disclosing the actual features in this paper. In general,
we consider a set of temporally stable features are defined
over observed fields in a claims sequence. Features may either be direct functions of elements of the claims sequence
or goodness-of-fit statistics that compare empirical distributions to normative distributions. While some features are
conditioned on the provider speciality (denoted as Spec features) other are independent (NonSpec features).
To assess the value of such features, we train two weighted
binary logistic regression classifiers [3] for the Spec and NonSpec feature sets, respectively. We use a labeled training set
with 8557 instances constructed using several million Medicaid claims. Less than 1% of the labeled set contained 1% of
known fraudulent providers using the fraud data discussed
in Section 5. Since the bad actor group was comparatively
small, and because we had greater confidence in their labels, the logistic regression was weighted toward the bad
actor group by a 10:1 ratio.
We calculated the sensitivity and specificity of both classifiers along with the area under the curve (AUC). Figure 10
shows that including speciality in the model significantly
improved performance (DeLong’s test; Z=7.22, p<.0001) of
the Spec model over the NoSpec model, yielding an AUC of
0.814.
0.8
With Specialty
Without Specialty
AUC=.814
0.0
0.2
0.4
Sensitivity
0.6
AUC=.716
1.0
0.8
0.6
0.4
0.2
tive data is available. An immediate next step is to try
semi-supervised methods on provider feature vectors so that
providers that are not labeled “fraudulent” can be treated as
unlabeled.
9.
CONCLUSIONS AND FUTURE DIRECTIONS
This paper showcases the relevance of advanced big data
analytics in the emerging domain of healthcare analytics using claims data. Our main contribution is the translation of
some of key challenges faced by the healthcare industry as
knowledge discovery tasks. The three case studies presented
in this paper attack the problem of identifying fraudulent
healthcare providers in three independent ways, using state
of art KDD methodologies, which have never been previously used in this context. Our results on real fraud data
highlight the promise that advanced data analytics hold in
this important domain. The analysis for these case studies
was conducted using the Hadoop/Hive data platform and
used open source software such as Mahout, R, and Python
networkx8 and hence are repeatable in other contexts.
In each case study we identified the potential and challenges associated with the existing analytic solutions. Treating providers and beneficiaries as text documents opens the
possibility of using the vast text mining literature and the
highly sophisticated text mining tools that have been developed specifically for big text data, and can lead to valuable
discoveries as shown in Section 6. Studying affiliations between providers as social networks is valuable, given that
organized fraud is rampant in the healthcare system, and
can be identified by analyzing the relationships between the
providers using network science methods. However, we identified certain differences between the provider network and
a traditional “social network” which researchers should bear
in mind before applying these methods. Temporal analysis
methods are also useful because they do not require trained
classifiers to identify anomalies, and are sensitive enough
to be employed as timely online techniques for detection of
transient billing practices that are anomalous. In future, we
intend to combine the features generated from each of the
case studies in a multi-view learning framework to better
identify fraudulent providers.
An important conclusion from these analyses is that while
insurance claims data are typically considered as payment
records, they contain valuable information that can be used
to answer many other healthcare related questions. For instance, studying topics of diagnosis or drug codes (see Section 6) can be done in the context of beneficiaries to understand the major behavior modes of the population in terms
of health indicators. Networks that capture interaction between beneficiaries and providers can be constructed from
claims data and can be used in conjunction with the provider
network to better understand the healthcare system.
0.0
Specificity
10.
Figure 10: ROC curves for Spec and NoSpec classifiers using weighted logistic regression
ACKNOWLEDGEMENTS
Prepared by Oak Ridge National Laboratory, P.O. Box
2008, Oak Ridge, Tennessee 37831-6285, managed by UTBattelle, LLC for the U. S. Department of Energy under
contract no. DEAC05-00OR22725.
Thus we show that supervised learning methods can be
effective in discriminating between bad actors and those presumed normal if the features are well-designed and norma-
8
1319
http://networkx.github.com/
11.
REFERENCES
[19] J. Manyika, et al. Big data: The next frontier for
innovation, competition, and productivity, May 2011.
[20] D. C. Montgomery. Introduction to Statistical Quality
Control. John Wiley and Sons, 4th. edition, 2001.
[21] M. Newman. Networks: An Introduction. Oxford
University Press, Inc., New York, NY, USA, 2010.
[22] E. S. Page. On problems in which a change can occur
at an unknown time. Biometrika, 44(1-2):248–252,
1957.
[23] L. Page, S. Brin, R. Motwani, and T. Winograd. The
pagerank citation ranking: Bringing order to the web.
Technical Report 1999-66, Stanford InfoLab, 1999.
[24] S. H. Preston and J. Ho. Low life expectancy in the
United States: Is the health care system at fault? In
National Research Council (US) Panel on
Understanding Divergent Trends in Longevity in
High-Income Countries. 2010.
[25] U. Raja, T. Mitchell, T. Day, and J. M. Hardin. Text
mining in healthcare. Applications and opportunities.
Journal of healthcare information management :
JHIM, 22(3):52–56, 2008.
[26] M. Reynolds and Z. Stoumbos. A cusum chart for
monitoring a proportion when inspecting continuously.
Journal of Quality Technology, 1999.
[27] M. Sparrow. License to steal: how fraud bleeds
America’s health care system. Westview Press, 2000.
[28] Y. W. Teh, D. Newman, and M. Welling. A collapsed
variational bayesian inference algorithm for latent
dirichlet allocation. In NIPS, 2006.
[29] S. Wasserman and K. Faust. Social Network Analysis.
Methods and Applications. Cambridge University
Press, 1994.
[1] National health expenditure projections 2009–2019.
Center for Medicare and Medicaid Services, 2010.
[2] World health statistics. WHO Library
Cataloguing-in-Publication Data, 2011.
[3] A. Agresti. Categorical Data Analysis, chapter 5.
Wiley-Interscience, Hoboken, New Jersey, second
edition, 2002.
[4] E. Aleskerov, B. Freisleben, and B. Rao. Cardwatch:
A neural network based database mining system for
credit card fraud detection. In Proceedings of IEEE
Computational Intelligence for Financial Engineering,
pages 220–226, 1997.
[5] D. M. Blei, A. Y. Ng, and M. I. Jordan. Latent
dirichlet allocation. J. Mach. Learn. Res., 3:993–1022,
Mar. 2003.
[6] Y. M. Chae, et al. Data mining approach to policy
analysis in a health insurance domain. International
Journal of Medical Informatics, 62(2-3):103–111, 2001.
[7] V. Chandola, A. Banerjee, and V. Kumar. Anomaly
detection – a survey. ACM Computing Surveys, 41(3),
July 2009.
[8] C. T. Chu, et al. Map-Reduce for Machine Learning
on Multicore. In B. Schölkopf, J. C. Platt, and
T. Hoffman, editors, NIPS. MIT Press, 2006.
[9] J. Cohen, et al. Mad skills: new analysis practices for
big data. Proceeding of VLDB Endowment,
2(2):1481–1492, Aug. 2009.
[10] T. Fawcett and F. Provost. Activity monitoring:
noticing interesting changes in behavior. In
Proceedings of the 5th ACM SIGKDD International
Conference on Knowledge Discovery and Data Mining,
pages 53–62. ACM Press, 1999.
[11] A. M. Garber and J. Skinner. Is american health care
uniquely inefficient? Working Paper 14257, National
Bureau of Economic Research, August 2008.
[12] R. Ghani and M. Kumar. Interactive learning for
efficiently detecting errors in insurance claims. In
Proceedings of the 17th ACM SIGKDD, pages
325–333. ACM, 2011.
[13] M. HÃűhle. Online change-point detection in
categorical time series. In T. Kneib and G. Tutz,
editors, Statistical Modelling and Regression
Structures, pages 377–397. Physica-Verlag HD, 2010.
[14] L. Kenworthy. AmericaâĂŹs inefficient health-care
system: another look.
http://lanekenworthy.net/2011/07/10/americasinefficient-health-care-system-another-look/,
2011.
[15] S. Konishi and G. Kitagawa. Information Criteria and
Statistical Modeling (Springer Series in Statistics).
Springer, 2007.
[16] B. Long, P. S. Yu, and Z. Zhang. A General Model for
Multiple View Unsupervised Learning. In Proceedings
of the SDM, 2008.
[17] C. B. Lynde and M. D. Pratt. Acquired perforating
dermatosis: association with diabetes and renal
failure. Canadian Med ‘Association Journal, 181(9),
2009.
[18] C. D. Manning, P. Raghavan, and H. Schtze.
Introduction to Information Retrieval. Cambridge
University Press, New York, NY, USA, 2008.
1320