1.2.1 Exchange Surfaces & Breathing [Autosaved]
advertisement

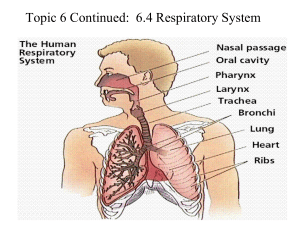
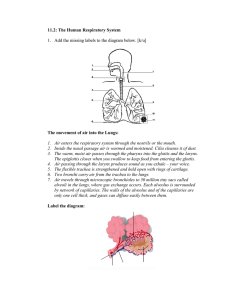
Unit 3: Exchange & Transport 3 A Exchange Surfaces & Gas Exchange Objectives • • • • • • • • Need for specialised exchange surfaces in multicellular organisms – relate to surface area to volume ratio (SA:Vol) Features of exchange surfaces Examples of exchange surfaces (lungs and alveoli) Adaptations of the lung for exchange – CO2 and O2 Ventilation and the role of lung tissues – mechanism of breathing Measuring lung capacity – spirometer; Interpretation of data 1 All living cells need to obtain certain vital substances from the external environment in which they live, and need to remove (excrete) harmful waste products of metabolism into the external environment, in order to stay alive Need to obtain from external environment Nutrients • Glucose (as a source of energy) • Proteins (for growth + repair) • Fats (for membrane structure; energy store; myelin sheath in neurones) • Water (solvent; reactant) • Minerals (for structure; water potential) • Vitamins (for metabolism) Need to remove into external environment Waste • CO2 (from respiration) • O2 (from photosynthesis) • Urea (from amino acids) • Ammonia • Excess heat • O2 – for aerobic respiration • CO2 – for photosynthesis (in plants) Cell 2 Single-celled (e.g. amoeba, bacteria, protozoa) and small organisms (e.g. flatworms) exchange materials across their cell membranes by DIFFUSION Diffusion - movement of molecules from a region of high concentration to a region of lower concentration They have large surface area to volume ratio – the exchange surface is adequate to exchange materials by diffusion Materials exchanged rapidly between external environment (water) by diffusion – external environment is in direct contact with the cell – short diffusion distance (thickness of cell membrane) Size of cube SA = Volume = SA:Volume ratio = 1 cm 6 cm2 (1x1x6) 1 cm3 (1x1x1) 6/1=6 Doubling of size causes 2 cm 24 cm2 (2x2x6) 8 cm3 (2x2x2) 24 / 8 = 3 SA to increase by 4 times Volume to increase by 8 times SA:Vol ratio to be halved Smaller organisms have a higher surface area to volume ratio 3 https://video.nationalgeographic.com/video /til/161021-sciex-til-anusha-shankarhummingbirds?source=searchvideo The Hummingbird 4 Larger multicellular organisms have lower SA : Vol ratios – they cannot rely on diffusion alone to exchange materials Increase in SA is not proportional to increase in volume as organisms get larger – volume increases much more than SA. A larger organism has a lower amount of surface in contact with the external environment in relation to its volume. ❑ Larger organisms have a greater demand for materials and produce greater amounts of toxic waste and heat, due to the large number of cells undergoing metabolism. ❑ Waste needs to be removed rapidly. Heat needs to be dissipated to prevent overheating – to prevent denaturation of enzymes ❑ Cells are distant from the external environment – materials need to travel longer distances and cross numerous barriers (membranes; fluid) Materials cannot be exchanged fast enough to maintain life ❑ Therefore, to meet the greater demands, larger multicellular organisms need efficient and specialised Exchange surfaces - intestine for absorption of digested nutrients; alveoli in lungs for gas exchange, and, Transport systems – circulatory system Some exchange surfaces may use the following to increase the efficiency of exchange further – 5 active transport (e.g. mineral uptake in root hair cells); facilitated diffusion ; bulk transport Features of efficient exchange surfaces Large surface area – large exchange surface to allow more molecules to pass through – usually achieved by structural adaptations – e.g. numerous spherical alveoli in lungs ; folding of walls and membranes - e.g. villi and microvilli in small intestine Thin – usually single cell thick - reduce diffusion distance between source and destination -e.g. wall of alveoli is composed of a single layer of squamous epithelium) Steep concentration gradient - constant supply of materials to be exchanged on one side (the supply side) to keep the concentration high (C2) and constant removal on the other side (the demand site) to keep the concentration low (C1) – in order to maintain a steep concentration (diffusion) gradient (C2 – C1) across the exchange surface –to ensure rapid diffusion - e.g. by ventilation (breathing) and circulation (blood circulatory system) Surface area X (C2 – C1) Rate of diffusion = Thickness The surface area and thickness are fixed to certain limits – the concentration gradient (C2 – C1) is the rate-limiting factor in exchange by diffusion across exchange surfaces Some exchange surfaces Small intestine - villi and microvilli – increase surface area for absorption of soluble nutrients – removed and transported to cells by the circulatory system Root hairs of plants – large surface area for absorption of H2O and minerals Lungs (alveoli) – large surface area for exchange of O2 and CO2 Hyphae (fungi) – large surface area for absorption of nutrients The Need for Ventilation and Gas Exchange Cell respiration provides the energy (ATP) requirements of the organism ❑ It requires a constant supply of O2 and produces CO2 (waste – that needs to be excreted) ❑ The obtaining of O2 and removal of CO2 is achieved by the respiratory system through the processes of ventilation and gas exchange The respiratory system links the blood circulatory system with the atmosphere The structural components of the respiratory system function to move atmospheric air into and out of the lungs (alveoli) by the rhythmic physical process of ventilation Ventilation Rhythmic physical process of moving atmospheric air into and out of the lungs (the organs of gas exchange) in order to supply O2 and remove CO2 Gas exchange Gas exchange occurs between the air in the alveoli (the specialised exchange surfaces in the lungs), and blood in the lung (pulmonary) capillaries, which surround the alveoli. ❑Blood rich in CO2 (from cell respiration) is brought to the alveoli from tissues – CO2 diffuses into the alveoli down a concentration gradient; O2 (from atmospheric air in the alveoli) diffuses into the blood from the alveoli, down a concentration gradient ❑The large number of thin walled tubular capillaries provide a rich blood supply and a large surface area for gas exchange between the blood and atmospheric air ❑The large number of spherical alveoli provides a large surface area for gas exchange (approximately 80 -100 m ) between the atmospheric air and blood 7 Pulmonary vein Oxygenated blood ▪ Nitrogen does not cross the alveolar wall – nitrogen is not used or produced in the body ▪ O2 is required for cell respiration to release energy from glucose ▪ CO2 (waste) is produced in cell respiration – needs to be removed (excreted) ▪ Water vapour varies – depending on humidity of atmospheric air ▪ Exhaled air is always more humid than inhaled air Pulmonary artery Deoxygenated blood Vena cava Deoxygenated blood Aorta Oxygenated blood 8 Respiratory System Rib Internal & external intercostal muscles 9 Lungs (2) The lungs are the organs of gas exchange and are composed of a number of different tissue types – e.g. elastic, connective, epithelial, nervous, muscular - working together to achieve particular functions – i.e. ventilation (breathing) and gas exchange between the air and blood • CO2 from the blood into atmospheric air • O2 from atmospheric air into blood Air can pass into and out of the lungs, through the respiratory tree (airways), which consists of the nose, the trachea (windpipe), bronchi and bronchioles. The bronchioles end in spherical structures, termed the alveoli. Gas exchange between the air in the alveoli and blood (in the lung capillaries) takes place across the thin walls of the alveoli The lungs are a large pair of inflatable structures (organs) located in the chest (thoracic cavity) Pleural cavity contains pleural fluid ▪ Reduces friction during ventilation ▪ Defence 10 Respiratory Tree Atmospheric air Direction of air flow during inhalation Larynx (“voice box”) Trachea Bronchus (2) Bronchioles Direction of air flow during exhalation Alveoli (“air sacs”) Site of gas exchange Gases exchanged by diffusion down their concentration gradients O2 from alveoli to blood in alveolar capillaries CO2 from blood into alveoli (for excretion) Capillaries (blood) Red blood cells transport absorbed O2 from lungs to body tissues CO2 transported from tissues to lungs for excretion 11 Adaptations of Respiratory System for Gas Exchange ❑ Cleans, warms, and moistens the air entering the respiratory tract during inhalation – achieved by hairs, mucus, and blood capillaries (warm blood) in the nasal cavity and cilia in the trachea ❑ A large number of spherical alveoli (600 million) 100-300 um across – giving a large surface area of approx.80-100 m2 for rapid gas exchange between the blood and atmosphere; alveolar wall is one cell thick (squamous epithelium) – short diffusion path between alveoli and blood in the pulmonary capillaries ❑ Numerous and tubular capillaries in close contact with alveoli - wall also made of squamous epithelium and one cell thick; total diffusion distance is less than 1 um ❑ Capillaries are narrow – red blood cells are squeezed against the capillary wall – making contact with the wall to reduce diffusion distance. The blood cells are also slowed down – increasing the time for exchange ❑ Constant ventilation - replacing the air in the alveoli to maintain a concentration gradient between the alveolar air and the blood ❑ Alveoli are surrounded by a large number of capillaries – a rich blood supply, replaces the blood constantly, to maintain a concentration gradient between the blood and alveolar air. ❑ Haemoglobin (Hb) in red blood cells carries oxygen and has a high affinity for oxygen – helps in maintaining a steep concentration gradient for oxygen ❑ Moist exchange surface – allows gases to dissolve ❑ Water in the alveoli contains a surfactant (phospholipid) – reduces surface tension – prevents collapse of alveoli ❑ Alveoli contain phagocytic cells - for defence 12 O2 from the atmospheric air entering the alveoli enters the blood by diffusion across the alveolar wall down its concentration gradient Total barrier to diffusion is less than 1 um CO2 from the blood enters the alveoli by diffusion across the alveolar wall down its concentration gradient Oxygenated blood to heart via pulmonary vein Low CO2 concentration Surfactant produced by alveoli – reduces cohesive surface tension forces between H2O molecules in film of H2O ST forces may cause collapse of alveoli during exhalation – prevented by surfactant Diffusion gradient maintained by rhythmic ventilation (replaces air in alveoli) and a rich blood supply high [O2] on supply side (alveoli); low [O2] on demand side (capillaries) – vice versa for CO2 Squamous (flattened) epithelium Plasma – carries 85% of CO2 as hydrogen carbonate ions, 5% dissolved in plasma, and 10% in combination with haemoglobin O2 CO2 Deoxygenated blood from heart via pulmonary artery High CO2 concentration Capillaries Close contact with alveolar wall 1 cell thick – short diffusion distance Narrow – space enough for passage of single RBC – allows close contact with capillary wall Large surface area – numerous and tubular Alveoli – spherical and numerous (600 million); large surface area (c.70 m2) Film of H2O – dissolves gases - evaporates Alveolus wall Capillary wall Each 1 cell thick RBC’s – contain haemoglobin carries O2 as oxyhaemoglobin Ventilation – movement of air into and out of lungs The ribcage, intercostal muscles and diaphragm all work together to move air into and out of the lungs, where gas exchange occurs across the thin (single-celled) walls of the alveoli Ventilation is a physical process, relying on the principle of Boyle’s Law – which state “Pressure is inversely proportional to volume” The mechanism can be illustrated using a bell jar model of the respiratory system – however, the model does not illustrate involvement of the rib cage and the intercostal muscles in ventilation Breathing out (expiration / exhalation) Internal intecostals contract in forced expiration Breathing in (inspiration / inhalation) 15 INSPIRATION EXPIRATION Atmospheric pressure = 760 mmHg External intercostals contract raising the rib cage ❑ ❑ ❑ ❑ ❑ Diaphragm & external intercostals contract Rib cage raised (upwards and outwards) Diaphragm lowered (becomes flatter) Volume of chest cavity increases Pressure in chest cavity drops to below atmospheric pressure to 758 mmHg • • Air moves into lungs from atmosphere Active process ❑ ❑ ❑ ❑ ❑ External intercostals relax lowering the rib cage Diaphragm & external intercostals relax Rib cage lowered Diaphragm raised (dome shape) due to push from abdominal organs Volume of chest cavity decreases Pressure in chest cavity increases to above atmospheric pressure to763 mmHg Air forced out of lungs into atmosphere Aided by elastic recoil and abdominal organs Passive process Structural components of the respiratory system Trachea Smooth muscle Contracts and relax to allow diameter of airways to be controlled; During exercise the muscle relaxes – making the airways wider – reduces resistance to air flow – aids ventilation Muscles contracts to narrow the airways when challenged with foreign material (e.g. pollen) to protect airways and alveoli Elastic fibres Stretch to allow expansion during inhalation and recoil during exhalation; prevent over expansion C-shaped rings of cartilage Provide structural support Prevent collapse of airway during inhalation Allows flexibility during movement without narrowing of airways Allows oesophagus to expand during swallowing Inside surface of trachea – epithelial lining Goblet (mucus) cells Secrete mucus – traps particles (e.g. dust, pollen, bacteria) – reduce risk of infection & inflammation Ciliated epithelium Cilia beat in a synchronised pattern to move (waft) mucus (with particles) towards throat – to be swallowed (stomach acid kills bacteria) or expectorated; prevents infection Cells contain numerous mitochondria (energy for ciliary movement) Loose tissue Inside surface of cartilage – glandular tissue, connective tissue, 17 elastic fibres, smooth muscle and blood vessels Bronchi ▪ Two narrower branches arising from the trachea – the right is more vertical and wider than the left – protective function – allows material entering the airways by accident to be directed into the right side, keeping the left functional Similar in structure to trachea – cartilage provides mechanical strength, and prevents collapse ▪ Cartilage is less regular Bronchioles ▪ Branches arising from the bronchi - much narrower than bronchi ▪ Some cartilage in larger ones – none in smaller ones ▪ Mainly smooth muscle and elastic fibres – terminal bronchioles have clusters of alveoli at their ends, where gas exchange takes place Smooth muscle ▪ Contracts involuntarily to constrict the airways – narrows lumen – most obvious in bronchioles; restricts airflow to and from the alveoli Defensive to prevent entry of foreign material and agents triggering contraction (e.g. in asthma). – leads to difficulty in breathing – drugs termed bronchodilators may be used to alleviate symptoms Elastic fibres ▪ Smooth muscle cannot reverse the effect of narrowing of the airways. Elastic fibres in the loose tissue are deformed when smooth muscle contracts. As the muscle relaxes, the elastic fibres recoil to their original size and shape – helping to dilate the airways. ▪ Elastic fibres in the lungs aid recoil of lung tissue during exhalation. Phagocytic cells ▪ Mostly in alveoli - defence 18 Cross section of bronchiole Alveolus wall ▪ Thin - single cell thick ▪ Squamous epithelium ▪ Reduces diffusion distance Bronchiole wall ▪ Ciliated epithelium (cilia move mucus upwards) ▪ Goblet cells (secrete mucus) Blood capillary ▪ Close to alveoli ▪ Thin - single cell thick ▪ Squamous epithelium ▪ Reduces diffusion distance Pulmonary vein ▪ Carries oxygenated blood to heart 19 Bronchiole (a) and trachea(b) in transverse section 20 Ciliated epithelium ▪ Composed of cells that possess cilia and mucus secreting goblet cells and glands ▪ The exposed part of the cell surface (luminal surface) is covered with cilia Cilia are hair like projections of the cell membrane – similar in structure to flagella, but much smaller ▪ Found in the trachea, bronchi, and in larger and medium-sized bronchioles ▪ Cells can be columnar or cuboidal ▪ Move fluid or mucus (with trapped material) upwards in the trachea by the mucociliary escalator; able to filter out particles between 2-10 microns (um) in diameter Nicotine in cigarette smoke paralyses cilia; tar also damages cilia 21 Part of lung Cartilage Smooth muscle Yes Elastic fibres Goblet cells Epithelium Trachea Large Cshaped rings Yes Yes Ciliated Bronchi Smaller pieces Yes Yes Yes Ciliated Larger bronchiole Some Yes Yes Yes Ciliated Smaller bronchiole None Yes Yes None Ciliated Smallest (terminal) bronchiole Alveoli None Yes Yes None No cilia Yes Recoil after deformation to dilate (widen) the airway None Secrete mucus – traps tiny particles (e.g. pollen; bacteria) from the inhaled air No cilia Cilia move in a synchronised pattern to waft the mucus up the airway to the back of the throat, to be swallowed. The acidity of the stomach kills any bacteria None Structural Supports trachea and bronchi – holding them open None Contracts to constrict the airways – restricting the flow of air In the lungs – recoil to reduce lung volume in expiration 22 Measuring Lung Volumes - Spirometry Lung volumes can be measured using a spirometer and recorded as a spirometer trace (spirogram). Used to assess lung function under various conditions) • • • • to evaluate respiratory impairment to aid diagnosis by identification of particular disease to assess changes with time and/or treatment to help assess fitness for anaesthesia and surgery Larger volumes Smaller volumes males Females taller people shorter people non-smokers heavy smokers athletes non-athletes people living at high altitudes people living at low altitudes ▪ A chart recorder is used to produce a graph (spirogram) ▪ Soda lime (sodium hydroxide)– absorbs CO2 from exhaled air ▪ The chamber does not rise to the same height with each breath – since, O2 is consumed and the CO2 produced is absorbed by the soda lime ▪ Depending on the design, in some respirometers, the float rises during inspiration and falls during expiration – the inspiration peak is longer than the expiration peak 23 Spirogram Inspiratory reserve volume – larger than expiratory reserve volume Expiratory reserve volume – less than inspiratory reserve volume Normal breathing rate = 12-18 breaths per minute One breath = Inspiration + Expiration Two factors determine ventilation of the lungs – RATE and DEPTH of breathing 24 Volume Definition Tidal Volume (TV) 0.5 L ▪ Volume of air moved into and out of lungs with each breath at rest. ▪ Provides body with enough O2 for its resting needs while removing enough CO2 to maintain a safe level Vital Capacity (VC) 5 L (male) 4.5 L (female) ▪ Largest volume of air that can be moved into and out of the lungs in any one breath (IRV + TV + ERV); varies (age, sex, gender, disease). ▪ Regular exercise increases VC Inspiratory Reserve Volume (IRV) 3L ▪ How much more air that can be inhaled over and above the normal TV when taking a deep breath. ▪ Utilised when exercising, defecating, playing musical instruments, etc Expiratory Reserve Volume (ERV) 1.2 L ▪ How much more air that can be exhaled over and above the amount that is expired in a normal TV breath Residual Volume (RV) 1.5 L Dead Volume (DV) ▪ Volume of air remaining in the lungs, even after forced exhalation ▪ Volume of air in the bronchioles, bronchi and trachea – does 25 not take part in gas exchange Using a spirometer 1.Subject - relaxed and allowed to establish a breathing pattern 2.A sterile mouthpiece is placed into the mouth; and a nose clip worn– nose clip ensures all air breathed in comes from the chamber and also prevents entry or exit of air through the nose 3.Subject breathes normally and the kymograph started; a data logger may be used 4.A spirometer trace (spirogram) is obtained - this is the TIDAL VOLUME 5.After a few minutes of relaxed breathing, the subject performs maximum expiration (by forcing all the air out of the lungs) and then performs a maximum inspiration, before returning to a normal breathing pattern. This gives a record the EXPIRATORY RESERVE VOLUME, INSPIRATORY RESERVE VOLUME, and VITAL CAPACITY Precautions ∙ ∙ ∙ ∙ ∙ ∙ ∙ Ensure subject is not on medication related to respiratory illness Ensure subject is not suffering from respiratory problems (e.g. asthma) Ensure fresh supply of soda lime for each investigation Ensure equipment is sterile and disinfect mouthpiece Use medical grade O2 and ensure adequate amount of O2 is available Ensure equipment is functioning correctly Maintain constant temperature – temperature affects volume of gases 26 Calculations involving lung volumes Respiratory Minute Volume (RMV) The RMV (or minute volume) is the volume of air inhaled or exhaled from a person’s lungs in one minute – it is also known as pulmonary ventilation (PV) It is the product of the tidal volume and the breathing rate Normal - 5-8 dm3 per minute Example Abnormal – e.g. in asthma – up to 14 dm3 per minute Tidal volume = 0.5 dm3 Breathing rate = 12 breaths /minute RMV = TV x breathing rate = 0.5 x 12 = 6 dm3 /minute Breathing rate from a spirogram 1Count the number of peaks (tidal volumes) in a given time 3 peaks in first 20 seconds 2Calculate the number of peaks in one minute No of peaks in 1 minute = 3 x 60 / 20 = 9 peaks per minute Breathing rate = 9 breaths per minute (bpm) 27 O2 uptake per minute from spirogram Example If x (decrease in volume) = 0.8 dm3 y (time) = 130 – 20 = 110 sec In 110 s, 0.8 dm3 of O2 is used up x / y = 0.8 / 110 x 60 = 0.44 dm3of O2 used per minute Breathing rate = 22 / 110 = 0.2 breaths/second = 0.2 x 60 = 12 breaths/ minute ❑ The volume of air inspired is the same as the volume expired. ❑ Soda lime absorbs the CO2 exhaled – causing the total volume of air to go down. ❑ This total reduction is equal to the volume of O2 breathed in – allowing the estimation of O2 use under different conditions. 28 Exercise and pulmonary ventilation The interdependence of the circulatory and the respiratory system in supplying O2 to tissues for respiration and the removal of CO2 (waste) for excretion requires an increase in pulmonary ventilation during exercise – to ensure that the demand for extra O2 and the removal of the excess CO2 during exercise are met Effects of exercise on PV Exercise causes an increase in PV (as well as cardiac output) This is to deliver greater amounts of O2 faster to the blood and therefore the respiring muscle cells and to remove CO2, lactic acid, and excess heat Chemoreceptors in the medulla oblongata, the carotid and aortic bodies detect the decrease in pH during exercise due to the increase in CO2 produced Signals are sent to the respiratory centre in the medulla to increase the frequency of impulses to the diaphragm and intercostal muscles to increase the breathing rate (breaths per minute) and depth (tidal volume) of breathing to increase PV This allows gaseous exchange to speed up – causing CO2 levels to drop and the demand for extra O2 to be met 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49