Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacolo
advertisement

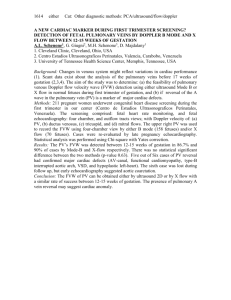
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/5241911 Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology Article in Expert Opinion on Drug Metabolism & Toxicology · July 2008 DOI: 10.1517/17425255.4.6.681 · Source: PubMed CITATIONS READS 20 224 5 authors, including: Gilles Hanton Gaël Y Rochefort GH Toxconsulting Paris Descartes, CPSC 63 PUBLICATIONS 1,376 CITATIONS 69 PUBLICATIONS 1,541 CITATIONS SEE PROFILE Jean-Marc Hyvelin Bracco Group 55 PUBLICATIONS 1,164 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Claudins and the Tight Junction View project Toxicology View project All content following this page was uploaded by Gaël Y Rochefort on 04 June 2014. The user has requested enhancement of the downloaded file. SEE PROFILE Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. Review 1. Introduction 2. The different modes of echocardiography Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology 3. Use of echocardiography 4. Application of echocardiography in preclinical safety pharmacology and toxicology 5. Value of echocardiography in experimental toxicology or safety pharmacology as a method of refinement 6. Conclusion 7. Expert opinion Gilles Hanton†, Véronique Eder, Gael Rochefort, Pierre Bonnet & Jean-Marc Hyvelin †Pfizer Global Research and Development, Department of Toxicology and Comparative Medicine, Z.I. Pocé sur Cisse, BP 159, F-37401 Amboise Cedex, France Background: Echocardiography (EC) is a method used for the investigation of cardiac morphology and function. Two-dimensional EC gives a visualisation of the morphology of the heart. M-mode EC allows heart function to be monitored. Pulsed Doppler EC is the method of choice to measure blood flows. Objective: To describe the information EC can provide for cardiovascular investigation in laboratory animals, with a special focus on the potential helpfulness of EC in preclinical toxicology and safety pharmacology. Methods: This review includes publications describing the methodology of EC and its application to several animal species used in biological experimentation. Results/conclusion: EC has been established in dogs, monkeys, rodents, rabbits and pigs. As demonstrated by experiments in different species, EC can be particularly helpful in toxicology and safety pharmacology, based on the amount of information it can give on the causes and consequences of drug adverse effects on the cardiovascular system. Furthermore, EC does not require any surgery and is therefore a key refinement compared to invasive methods generally used for investigating the cardiovascular function in laboratory animals. Despite some limitations of the method (the need for trained people, time required for an accurate EC recording, lack of current validation), EC should be further developed in preclinical toxicology and safety pharmacology. Keywords: cardiac, Doppler, echocardiography, laboratory animal, toxicity, vascular Expert Opin. Drug Metab. Toxicol. (2008) 4(6):681-696 1. Introduction Echocardiography (EC) is a method used for the investigation of cardiac morphology and function [1]. A transducer is placed on the chest of the subject and emits ultrasounds that are reflected by the cardiac structures and surrounding tissues. The reflected ultrasounds are received by the transducer and then processed by the echographic device in order to form an image on a screen. The fraction of the ultrasounds that are reflected characterises the echogenicity and depends on the physical properties of the tissues. Bones and air have a strong echogenicity and appear in white on the screen. Liquids such as blood have a weak echogenicity and appear as black areas corresponding to the cardiac cavities and lumen of large vessels. Fibrous tissues and muscles have an intermediate echogenicity and appear as grey structures corresponding to cardiac valves and the wall of heart and main vessels. 10.1517/17425250802106271 © 2008 Informa UK Ltd ISSN 1742-5255 681 Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology 5 MHz transducer Figure 1. Schematic representation of bidimensional (2-D) echocardiography in parasternal incidence, showing a longitudinal section of the heart by the ultrasound beam. Septum Aortic valves Aorta Left ventricle Mitral valves Left atrium Figure 2. Example of a 2-D longitudinal section of the heart in a dog by 2-D echocardiography. echographic device [2,3]. The transducer emits a planar beam of ultrasounds in which the cardiac structures are visualised. Depending on the position of the transducer on the chest of the animal, different heart sections are obtained. By changing the orientation of the transducer progressively, the operator can scan the heart in successive sectors from which the walls, the cavities, cardiac valves and main vessels are visualised. The changes in their structures are followed over a number of cardiac beats. An ECG that is recorded simultaneously allows one to follow the cardiac cycle. 2-D images can then be frozen either in ventricular systole, which correspond to the beginning of the QRS complex (corresponding to ventricle depolarisation) or in diastole, at the end of the T wave (corresponding to ventricular repolarisation). In 2-D sections, anatomical abnormalities can be detected and a number of measurements can be taken. 2-D EC views allow placing guidance lines for M-mode EC or Doppler EC across cardiac structures. The 2-D EC examination is usually performed in two different incidences. In parasternal incidence, the transducer is placed on the right side (dog and marmoset) or left side (rat and mice) of the sternum of the animal, generally standing or placed in a sling [2,4,5] and the cardiac structures are visualised in two different sections. A long axis (longitudinal) section is carried out across the left and right ventricles, left atrium and aorta (Figure 1). This section is used for the examination of the septum, free wall and cavity of left ventricle, mitral valves, cavity and wall of the left atrium and the aortic root (Figure 2). A short axis section allows visualisation of the heart in successive transverse sections, from the apex to the upper part of the heart (Figure 3). The section at the upper level allows visualisation of the aortic and pulmonary artery trunk and measurement of the pulmonary artery diameter (Figure 4). For apical incidence, the transducer is placed on the left side of the animal at the level of the cardiac apex [6]. The best images are obtained when the animal is lying on its left side. The four cardiac cavities are visualised simultaneously (Figure 5) and their areas can be measured in systole and diastole. The volumes of the left and right ventricles in systole (LVVs and RVVs) and diastole (LVVd and RVVd) are calculated using the Simpson method, which integrates the surfaces of the ventricles areas from apex to valve plane. The stroke volume (SV) is calculated by Equation 1: (1) There are three modes of EC, which are usually performed successively for a complete examination of the cardiac structures, their movements over time and blood flows. 2. The different modes of echocardiography 2.1 Two-dimensional echocardiography and the ejection fraction (EF) of the left ventricle is derived from these volumes by Equation 2: (2) EF = SV / LVVd Two-dimensional echocardiography (2-D EC) gives a view of the morphology of the heart on the screen of the 682 SV = LVVd − LVVs EF indicates the fraction of the ventricular diastolic volume that is ejected at each beat and is therefore considered Expert Opin. Drug Metab. Toxicol. (2008) 4(6) Hanton, Eder, Rochefort, Bonnet & Hyvelin D. C. PM RV LVO LV RVO PMV AMV CH Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. E D E. C B. B A RV TV PPM RA LV LA RV NC RC LC PV APM A. LAu RV LV Figure 3. Schematic representation of bidimensional (2-D) echocardiography in parasternal incidence, showing the different levels of the transverse sections of the heart. Extracted from Thomas, 1984 [6]. RV AO PA Figure 4. Transverse 2-D section of the upper part of the heart in a marmoset, showing the right ventricle (RV), the pulmonary artery (PA) and the aorta (AO). In this view, the Doppler window can be positioned for recording the pulmonary flow. as a key indicator of the ventricular contractile function. By measuring myocardial and cavity area of the left ventricle, it is also possible to evaluate its mass [7]. These calculation of ventricle volume from a single 2-D section are based on assumption of their geometry, and the accuracy of volume evaluation can be improved using 3-dimensional EC, in which the heart is scanned in successive 2-D sections and the volume computerised by ventricular surface reconstruction [8,9]. The method is of particular interest for the evaluation of volume and contractile function of the right ventricle because its eccentric and complicated morphology does not allow accurate calculation from an unique 2-D section [10,11]. 2-D EC imaging can be improved by the use of contrast EC. Microbubbles which exhibit a high degree of echogenicity are injected intravenously and enhance the ultrasound backscatter of perfused tissues [12]. Contrast-enhanced EC can be used to image blood perfusion in the heart. It helps in detecting intracardiac shunts and valvular regurgitation, in improving endocardial border detection and in measuring cardiac output [13]. The method is Expert Opin. Drug Metab. Toxicol. (2008) 4(6) 683 Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology (5) PWTI =(PWTd – PWTs)/PWTd It is also possible to evaluate the volume (V) of the left ventricle in diastole (LVVd) and systole (LVVs) using the Teicholz formula (Equation 6). LV (6) RV V = 7D /(2.4 + D) 3 Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. RA LA Figure 5. Visualisation of the four cardiac cavities in 2-D echocardiography, apical incidence in a marmoset showing, the right ventricle (RV), the right atrium (RA), the left ventricle (LV) and the left atrium (LA). In this view, the Doppler window can be positioned for recording the mitral flow. particularly useful for quantitative evaluation of myocardial perfusion (Figure 6) [14,15]. 2.2 Time-motion EC In time-motion (M-mode), the position and movements of the cardiac structures crossed by the guidance line are displayed for a few cycles. In this way, M-mode EC allows the observer to visualise changes in heart morphology over the cardiac cycle and to monitor cardiac function [16]. M-mode EC is recorded from a 2-D view of the heart in either short axis or long-axis section [5,17,18]. In a short axis section, the upper part of the ventricle is visualised at the level of the papillary muscles close to the chordae tendinae. The guideline is positioned between the papillary muscles and the movements of the cardiac walls and septum are recorded (Figure 7). Left ventricular end-diastolic (LVDd) and end-systolic (LVDs) diameters are measured at the time of maximum diastolic and minimum systolic dimensions (Figure 8). Left ventricular fractional shortening (LVFS) is calculated by Equation 3: (3) LVFS = (LVDd − LVDs)/LVDd and gives an index of left ventricle systolic function. Thicknesses of the interventricular septum (IVSd and IVSs) and of the left ventricular posterior wall (PWTd and PWTs) are measured in diastole and systole. The thickening index is calculated for the septum (STI) and wall (PWTI) by Equations 4 and 5: (4) STI =(IVSd – IVSs)/IVSd 684 where D = LVDd or LVDs, respectively, for LVVd and LVVs. SV and EF can then be derived from LVVd and LVVs [19]. Based on the dimensions of the left ventricle cavity and thickness of its free wall and septum, the mass of the ventricle can be estimated [7]. The mean slope of the systolic wave of the free wall of ventricle is calculated between the onset and the peak of the wave, whereas the maximal slope is measured as a tangent of the wave at its onset (Figure 8). These slopes are further indices of left ventricle contractile function. In long axis section, an area of the heart giving a clear longitudinal view of the cavities and walls, in particular these of the left heart is selected, and the guidance line is usually placed at two levels. For the evaluation of the ventricular function and morphology, the guidance line is positioned at the tips of the mitral valves and the movements of the cardiac walls and septum are recorded. The same parameters as those measured or calculated from M-mode recordings in short axis section can be obtained from the long axis section. In addition, the guidance line can be placed in long axis section in the upper part of the heart, across the aortic root and left atrium, for recording of their movements (Figure 9). Aortic diameter is measured in systole and diastole (ADs and ADd). Depending on the quality of the short- or long-axis view, the movements of the right ventricular can also be assessed. The thickness of the right ventricle wall in diastole and systole (RVTd and RVTs) and diameter of its cavity (RVDd and RVDs) can be measured. 2.3 Doppler echocardiography In pulsed Doppler EC, blood velocity is measured at the level of a window selected in a 2-D section [20]. The spectrum of distribution of the velocities of the red blood cells and their variations over the cardiac cycle are recorded as successive waves produced by the pulsatile flows. The brightness of the spectrum indicates the number of red blood cells at each velocity. The waves appear positive on the screen when the blood is flowing to the transducer and the waves are negative when the blood is flowing in the opposite direction. By measuring the speed of blood motion in vessels and cardiac cavities, pulsed Doppler EC allows the assessment of flows patterns and, consequently, of the systolic and diastolic cardiac function, pressure gradients across valves and orifices, pressure changes in the cardiac chambers Expert Opin. Drug Metab. Toxicol. (2008) 4(6) Hanton, Eder, Rochefort, Bonnet & Hyvelin A. B. S Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. LV D. C. LV Figure 6. Contrast echocardiography (B and D) coupled with M-mode echocardiography (A and C) in rats. A. M-mode in a normal rat, showing the movements of the septum (S) and left ventricle posterior wall (LV). B. Bidimensional contrast echocardiography in the same rat as in (A), showing a longitudinal section of the heart with homogeneous myocardial perfusion (the whole heart appear as grey). C. M-mode in a rat with experimental infarct (coronary ligation). Movements of septum and left ventricle wall are decreased. A notching appears on the movements of the ventricle wall. D. Contrast echocardiography in the same rat as in (C). A black crescent (arrow) can be seen on the apex of the heart, indicating an ischemic area. Right ventricle Septum Mitral valve Left ventricle Left ventricle posterior wall Figure 7. Transventricular M-mode echocardiography in a dog. The guidance line has been placed at the level of the tip of the mitral valves in a longitudinal section (Figure 2) or between the chordae tendinae in a transverse section (Section C on Figure 3). The M-mode recording shows the changes over time in the right ventricle cavity, the interventricular septum, the left ventricle cavity and posterior wall of the left ventricle. and large vessels and vascular resistance. Physiological and pathological changes in pulmonary, aortic and atrioventricular flows can be investigated [1,21,22]. Doppler EC is also a reliable method for measurement of stroke volume and minute cardiac output [23-25]. The atrio-ventricular flows are assessed with pulsed Doppler from a four-cavity section obtained in apical incidence. The Doppler windows are placed downstream of the flows, below the mitral or the tricuspid valves (Figure 5). The flows are recorded and two positive waves occur at each cardiac beat (Figure 10). The rapid inflow E wave corresponds to the passive filling of the ventricle occurring during its diastole and is recorded during the isoelectric section of the ECG, between T and P waves. The A wave corresponds to the ventricular filling associated with atrial contraction and occurs at the time of the P wave. Peak velocities (Vmax) of E and A waves, their ratio (E/A), E wave deceleration and the integral of velocity over time (VTI) of the two waves together are recorded and serve as indices of ventricle diastolic and/or atrial systolic functions. In particular, E/A Expert Opin. Drug Metab. Toxicol. (2008) 4(6) 685 Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology STd LVIDd STs PWVM LVIDs Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. PWVm LVPWd LVPWs Figure 8. Schematic representation of a transventricular M-mode recording showing the different parameters measured. (7) SVPul ⫽ VTIPul ⫻ p ⫻ (DPul / 4 ) 2 (8) SVAo = VTIao × π × (D Ao / 4 ) 2 The cardiac output (CO) is calculated by Equation 9: (9) AO CO = SV × heart rate LA Figure 9. M-mode echocardiography of the upper part of the heart in a marmoset. The guidance line is positioned across the aorta and left atrium (Section E on Figure 3) The movements of aorta (AO) and left atrium (LA) marmoset, are recorded over time. gives an indication of the relative contribution of ventricular diastole and atrial systole to the ventricular filling. Pulsed Doppler EC is also used to assess arterial flows. The aortic flow is recorded from a modified section in apical incidence showing the four cavities and the aortic root. The pulmonary flow is recorded from a short axis section of the upper part of the heart, in right parasternal incidence (Figure 4). The Doppler window for aortic or pulmonary flows is placed just above (downstream of ) the sigmoid valves. For either flow, a negative wave is recorded at each beat, from which Vmax, VTI, pre-ejection time, acceleration time (AT) and ejection time (ET) can be measured (Figure 11). The SV is calculated from the pulmonary (SVPul) or aortic flows (SVAo) by Equations 7 and 8. 686 In colour Doppler EC, the flows in the cavities and great vessels are visualised in real time from a 2-D section, based on a colour code. The flow appears in blue when the blood is flowing toward the transducer or in red when blood is flowing in the opposite direction (Figure 12). The brightness of blue or red colour indicates the velocity of the blood. Colour Doppler EC shows a number of qualitative blood flow changes, for example, laminar versus turbulent flows or abnormal timing and location of blood flows. Colour Doppler is therefore a useful tool for the assessment of disturbed flow patterns associated with valve insufficiency or stenosis [21]. On a four-cavity apical view of the heart, the atrioventricular flows during ventricular diastole and atrial systole and the arterial flows during ventricular systole are observed by colour Doppler at each cardiac beat. Images can be frozen and used to determine abnormalities in the flow patterns. Doppler tissue imaging evaluates the velocity of the movements of the cardiac walls and valves and in this way gives a direct evaluation of the cardiac contractile function [26]. On an apical view of the heart in 2-D EC, the Doppler window is placed on the free wall of the ventricle at the level of the valve. On the tissue Doppler velocity spectrum, three waves are identified [27]. The positive wave (Sm wave) corresponds to ventricular systole and Expert Opin. Drug Metab. Toxicol. (2008) 4(6) Hanton, Eder, Rochefort, Bonnet & Hyvelin ventricle. The lag between Sm wave and Ea wave evaluates the time of isovolumic relaxation of the ventricle (TIVR) and the lag between Aa wave and the following Sm wave evaluates the time of isovolumic contraction (TIVC). The Tei index is then calculated by Equation 10. (10) Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. E (TIVC − TIVR )/Sm duration A Figure 10. Pulsed Doppler recording of the mitral flow in a marmoset. Presence of two waves on the velocity spectrum: E wave (E) during the isoelectric inter-beat interval of the ECG and A wave (A) at the time of the P wave of the ECG. and gives information on the global ventricular performance [28,29]. The Q-Sm time measured from the onset of Q wave of ECG to the onset of the Sm wave of the tricuspid annulus is used to evaluate the electromechanical coupling of the right ventricle [27]. In addition, the ratio of the amplitudes of the E wave of the mitral flow measured in pulsed Doppler and of the Ea wave measured in tissue Doppler (E/Ea) is a marker of the left ventricle filling pressure and is frequently used in human EC examination [30]. The E/Ea ratio can be applied in animals, although its usefulness may be limited by the fusion of the E and A waves of the mitral flow occurring as a consequence of tachycardia, mainly in small species such as rats and marmosets. 3. b d a c Figure 11. Pulsed Doppler recording of the aortic flow in a marmoset. Measurement of pre-ejection time from the Q wave of the ECG (a) to the onset of the Doppler velocity spectrum (b), acceleration time from the onset to the peak of the velocity spectrum (c) and ejection time from the onset to the end of the velocity spectrum (d). two negative waves correspond, respectively, to the early, passive filling of the ventricle due to its relaxation (Ea wave) and to the late filling of the ventricle associated with atrial contraction (Aa wave) (Figure 13). The ratio Ea/Aa is calculated as an index of the diastolic function of the Use of echocardiography EC has been widely used in humans to investigate cardiac physiology and pathology [31] and to evaluate the pharmacological effects of drugs [32,33]. EC has a number of applications in laboratory animals, in particular in dogs, but also rodents, rabbit and nonhuman primates. The frequency of the ultrasound should be adapted to the size of the animals. A 3.5 – 5 MHz transducer is used in Beagle dogs and Cynomolgus monkeys [5,9,34], 7.5 – 15 MHz transducer in rats, guinea-pigs, rabbits and small monkeys [35-38] and 15 MHz in mice [39]. In dogs, the method of EC recording is well established and has been described in a number of papers, together with values in normal subjects [4,6,18,20,40]. Changes in cardiac dimensions have been followed in growing dogs with M-mode EC [41], whilst Doppler parameters in normal dogs and influencing factors have been established [42,43]. In canine or feline veterinary practice, EC is routinely used and can assist in the diagnosis of cardiac morphological alterations or dysfunction [2,17]. M-mode and Doppler EC enabled testing the efficacy of ACE inhibition, digitalis therapy, inodilation and venodilation in the treatment of dogs affected by mitral regurgitation [44]. EC is also used as an investigational tool in dog experimentation. In particular, EC has several applications in evaluating impairment of the cardiac function in canine models of heart disease and in testing the beneficial effects of drugs. EC was applied in canine models of partial left ventriculectomy or congestive heart failure. In these animals, 2-D and M-mode EC allowed the following of drug-induced increases in size and volume Expert Opin. Drug Metab. Toxicol. (2008) 4(6) 687 Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology Figure 12. Colour Doppler image in an apical view of a marmoset heart, showing in red the blood flow from left atrium to left ventricle. Sm Ea Aa Figure 13. Doppler tissue imaging of mitral valve of a rat. Three waves are identified and correspond to the movement of the valve at the time left ventricle systole (Sm), ventricle diastole (Ea) and left atrium systole (Aa). of the cavities associated with a decrease in EF and in fractional shortening [45-48]. Effects of enalapril in dogs with doxorubicin-induced cardiomyopathy have also been assessed using EC [49,50]. In dogs with myocardial failure, treatment with milrinone at doses of 0.3, 0.5, 0.75 or 1 mg/kg produced a marked improvement of left ventricle function as indicated by a dose-related increase in fractional shortening, which at the high dose reached ∼ 1.6-fold the control value [51]. Using Doppler tissue imaging, it is possible to evaluate the impairment of left ventricular diastolic function in dogs with cardiac ischaemia, as indicated by a 688 decrease in Ea wave of the mitral annulus [52]. Contrast EC was used to assess the changes in regional myocardial perfusion in a dog model for coronary artery bypass surgery [13]. Performance of contrast Doppler EC also improved the measurement of haemodynamic changes associated with aortic stenosis in boxer dogs [12]. Moreover, EC is considered as a key method of investigation in preclinical toxicology in dogs [5,34,53]. In monkeys, EC can be used to evaluate the cardiac consequences of several diseases. Doppler EC showed systolic and diastolic abnormalities of both ventricles in baboons (Papio hamadryas) affected by Chagas disease [54]. Rhesus monkeys (Macaca mulata) infected with simian immunodeficiency virus had changes in indices of ventricular contractility derived from EC measurements, which correlated with postmortem evidence of myocardial pathology [55]. Development of cardiomyopathy in a colony of owl monkeys (Aotus nancymae) was monitored through echocardiographic markers of changes in size and contractile function of the left ventricle [56]. Similarly, heart failure associated with ageing in squirrel monkeys (Saimiri sp.) was assessed through the changes in left heart dimensions measured in 2-D EC [57]. The different modes of EC were also shown to allow assessment of the effects of cardiovascular compounds or irradiation [9,58]. In particular, 3-dimensional EC allowed the demonstration of a doserelated decrease in EF in Cynomolgus monkeys treated with the β-adrenergic blocker metroprolol (-19 and -24% at 10 min after treatment with 0.1 and 0.3 m/kg, respectively, when compared to pretreatment values). Less marked effects were found in monkeys receiving 0.1 and 0.3 mg/kg of the calcium channel blocker verapamil (-10 and -19% change in ejection fraction, respectively) [9]. Based on EC usefulness in primate experimentation, reference values have been established in normal Rhesus [59] and Cynomolgus monkeys (Macaca fascicularis) [60]. The authors of this article have recently set up EC in marmosets (Callithrix jacchus) [35] are considered promising species for biological research, in particular in toxicology and pharmacology [61]. The different EC modes have been established in rats and extensively used for assessing changes in heart structures and function in experimental models of cardiac disease and effects of pharmacological interventions [62]. In particular, progressive impairment of cardiac contractility and haemodynamic function has been monitored in spontaneously hypertensive (SHR) rats and in spontaneously hypertensive heart failure prone (SHHF) rats [37,62]. Progressive impairment of pulmonary artery flow patterns and right ventricle dilation occurring in rats with pulmonary hypertension (PAH), induced by chronic hypoxia or after monocrotaline treatment, have been determined using pulsed Doppler and M-mode EC [27]. These methods Expert Opin. Drug Metab. Toxicol. (2008) 4(6) Hanton, Eder, Rochefort, Bonnet & Hyvelin Table 1. Effects of candesartan and cilazapril on left ventricle function in a model of myocardial infarction in rats, after 4 weeks of oral treatment: comparison of echocardiographic and invasive method data [68]. Ratio of mean values in treated animals versus controls Candesartan 1 mg/kg/day Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. Echocardiography Cardiac catherisation 10 mg/kg/day Cilazapril 1 mg/kg/day 10 mg/kg/day FS 1.77 1.85 1.92 1.92 EF 1.29 1.39 1.32 1.32 E/A 0.31 0.30 0.33 0.29 LVEDP 0.32 0.36 0.27 0.27 E/A: Ratio of amplitudes of E and A wave of the mitral flow; EF: Ejection fraction of the left ventricle; FS: Fractional shortening of the left ventricle; LVEDP: Left ventricle end diastolic pressure. provided evidence for pulmonary outflow impairment, with a midsystolic notch of the Doppler pulmonary spectrum, a thickening of the right ventricle anterior wall, a decreased acceleration time and a reduction of right ventricle fractional shortening. Doppler tissue imaging was found to be an accurate method for evaluating the right ventricle diastolic dysfunction and the impairment of electro-mechanical coupling of the right ventricle occurring in these PAH models [27]. EC also allowed the investigation of the changes in the left ventricle systolic and diastolic function associated with myocardial degeneration in streptozotocin-induced diabetic rats, together with the beneficial effect of sulindac, an aldose reductase inhibitor [63,64]. A number of experimentations focussed on the use of EC in assessing the morphological and functional cardiac changes in rats with experimental myocardial infarction [65]. Measurement of infarct size with 2-D EC was in good agreement with histopathological examination [66]. Pulsed Doppler measurement of E/A and Doppler tissue imaging measurement of Ea/Aa at the level of the mitral valve were shown to accurately detect rats with an increased left ventricle end diastolic pressure as a marker of the cardiac failure resulting from myocardial infarction [67]. EC was used to demonstrate the protective effects of the calcium channel blocker diltiazem, the ACE inhibitor cilazapril and the angiotensin II receptor antagonist candesartan against cardiac dysfunction and morphological changes associated with experimental myocardial infarction in rats [68,69]. In this model of myocardial infarction, the treatment with cilazapril or candesartan for 4 weeks at doses of 1 or 10 mg/kg increased the left ventricle fractional shortening and EF and decreased the E/A ratio of the mitral flow, when compared to untreated rats [68]. This indicated that both the systolic and diastolic functions were improved by the treatment. The left ventricle end diastolic pressure measured by cardiac catherisation (via carotid artery) was markedly decreased in treated rats, indicating an improvement of the pumping ability of the left ventricle. Therefore, there was a good consistency between data obtain by EC or by invasive methods (Table 1). Doppler and M-mode EC monitoring also demonstrated the beneficial effects of the ACE inhibitor perindopril in preventing ventricular dilation and the decrease in cardiac contractility and cardiac output occurring in an experimental rat model of aortic regurgitation [70]. In mice, EC was also used in a number of experiments for assessing heart function and structure [71] and was demonstrated to correlate with invasive measures [39]. Left ventricle mass of the mice has been estimated from measurement of ventricle areas in 2-D EC or from measurements of cavity and wall dimensions in M-mode, the former method giving the most accurate data when compared to postmortem measurements [7]. A combination of M-mode, pulsed and colour Doppler EC allowed investigators to determine the impairment in myocardial function and intra-cardiac flows in cardiomyopathic mice [72]. Effects of ketamine, xylazine, isoprenaline, atropine and atenolol on cardiac contractility were determined with M-mode EC for assessing the importance of changes in autonomic balance during anaesthesia in mice [73]. As in other species, contrast EC is a method of choice for evaluating myocardial perfusion in mice and to assess the effects of vasodilators [74]. Using pulsed and colour Doppler, it is possible to image the major branches of the coronary arteries in mice and to measure corresponding blood flows [75]. EC was less frequently applied in other laboratory animal species than in dogs, monkeys, rats or mice. However, in rabbits, pulsed and Doppler tissue imaging have been established and can assess the depressive effects of xylazine and ketamine on cardiac function [38]. Tissue Doppler also gave an accurate evaluation of the myocardial function in a model of adriamycin-induced cardiomyopathy in rabbits [76]. Pulsed Doppler and M-mode EC were used to assess the changes in SV and ventricle contractility in rabbits with experimental thrombo-embolism [77]. Expert Opin. Drug Metab. Toxicol. (2008) 4(6) 689 Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology In guinea-pigs, impairment of cardiac function after coronary ligation was successfully assessed by 2-D and M-mode EC [36], which were applied for evaluating the effects of the calcium-sensitizer levosimendan on systolic and diastolic function [78]. The technique of EC has also been established in mini pigs [79]. Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. 4. Application of echocardiography in preclinical safety pharmacology and toxicology Adverse effects on heart morphology and function may occur with a number of drugs and have dramatic consequences or even lead to death. Therefore, it is critical to have a thorough preclinical evaluation of the cardiac risk, in which EC will find a number of applications [80]. EC is frequently used to assess toxicity of drugs in humans and in particular, Doppler EC is the gold method to assess the functional consequences of anthracycline’s cardiotoxic effects [81,82]. In contrast, this technique has not yet been routinely used for the preclinical toxicological evaluation of drugs despite its potential interest, mainly in dogs [83]. Using 2-D EC, it is possible to visualise and evaluate morphological changes induced by drug treatment, such as myocardium hypertrophy or cardiac chamber dilation [84]. Furthermore, the functional consequences of treatmentinduced arrhythmia or cardiac lesions in laboratory animals can be assessed by M-mode or Doppler EC. Changes in haemodynamic parameters (SV and flows patterns) and indicators of cardiac contraction (ejection fraction, fractional shortening and velocities of cardiac structures movements) would allow evaluation of the degree of cardiac function impairment. Doppler EC and M-mode EC were used to demonstrate the depression in cardiac contractile function and haemodynamics produced by the anaesthetics, medetomidine and xylazine, in dogs [85]. These EC techniques were also shown to be helpful in evaluating cardiac impairment in dogs treated with doxorubicin [48,86,87]. In particular, the treatment of dogs with 6 doses of doxorubicin at 3-week intervals produced a progressive decrease in mean fractional shortening, which was reduced to ∼ 25% of its initial value, at the end of the treatment and in the mean E/A ratio of the mitral flow [85]. These changes are consistent with a progressive impairment of the systolic and diastolic function of the left ventricle. In dogs treated with five doses, the changes in fractional shortening were less marked than after six doses and no change were seen in E/A ratio, showing a relationship between the total cumulative dose and the impairment of the left ventricle function. Moreover, when data from both dosing regimens were analysed at the individual level, the magnitude of the decrease in fractional shortening correlated well with the degree of myocardial damage evaluated by histopathological examination. 690 EC was also recently used to assess the effects of dex-fenfluramine, an agonist of serotoninergic 2B receptors, on PAH development in rats exposed to chronic hypoxia [88]. At the end of a 4-week treatment period, the compound had no effect on PAH associated with the hypoxic conditions. However, 2 weeks after the end of the dexfenfluramine treatment, changes in EC parameters of pulmonary flow and right ventricle function indicated an aggravation of the PAH compared to control animals exposed to hypoxia and treated with vehicle alone. Colour Doppler EC was used to visualise tricuspid, mitral, pulmonary and aortic regurgitant jets in rats with valvulopathy produced by treatment with serotonin or pergolide, a dopamine agonist. A good correlation was found between regurgitation evaluated by colour Doppler and valvular thickening measured at histopathology [89]. EC is also of prime interest in assessing the adverse effects of cardiovascular drugs. Toxic effects of such drugs on the heart or blood vessels are often due to exaggerated pharmacological effects [90-92], resulting in marked changes in the cardiovascular function. M-mode and Doppler EC can quantify drug-induced changes in the patterns of cardiac contraction, flows, SV and cardiac output and in this way help to clarify the pathogenesis of cardiac or arterial lesions. For example, M-mode and Doppler EC were used to assess the cardiac effects of the potassium channel opener minoxidil and the PDE3 inhibitors UK-61,260 and milrinone in dogs [93-96]. The changes in heart function and haemodynamics produced by these vasodilatory and/or inotropic drugs help in understanding the mechanism of development of the left ventricular and right atrial lesions that are well know adverse effects of these compounds [97]. Major effects detected by EC were a decrease in LVVd due to the decrease in diastolic time associated with tachycardia and an increase in fractional shortening and in EF characterising the reflex stimulation of the cardiac contractility in response to hypotension [93]. In addition, milrinone had a direct effect on cardiac contractility [96], which explained an increase in fractional shortening similar to that seen after minodidil, despite a smaller increase in heart rate after milrinone, indicating a lower compensatory cardiac stimulation. Overall the changes were dose related and were consistent with the pharmacological effects of the drugs (Table 2). EC was also used to evaluate the effects of minoxidil on the cardiac function of marmosets and in this way to compare the pathogenesis of the cardiac lesion induced in this species by a potent vasodilator with similar data generated in dogs [98]. As in dogs, a major effect of treatment on EC parameters consisted of an increase in fractional shortening (1.44-fold increase 1 h after dose compared to predose value) indicative of a compensatory cardiac stimulation, after treatment with 150 mg/kg. The magnitude of the change was similar to that produced by 2 mg/kg of minoxidil in dogs (Table 2) showing that the marmoset is less sensitive than the dog to the cardiovascular effects Expert Opin. Drug Metab. Toxicol. (2008) 4(6) Hanton, Eder, Rochefort, Bonnet & Hyvelin Table 2. Effects on minoxidil [93] and milrinone [96] on echocardiographic parameters in the dog. Ratio of mean values recorded after a single dose versus values recorded before treatment Minoxidil Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. Milrinone Dose (mg/kg) Heart rate LVVd FS Control 1.08 0.95 1.08 1 2.13 0.73 1.30 2 2.08 0.66 1.55 Control 0.98 0.98 0.97 0.5 1.39 0.67 1.42 1 1.46 0.77 1.49 of this compound, although the pathogenesis of the cardiac lesion is similar in both species. 5. Value of echocardiography in experimental toxicology or safety pharmacology as a method of refinement In contrast to most methods presently used in animal experimentation to investigate cardiac function or blood flows, EC is non-invasive and does not necessitate surgery. It requires only a gentle restraint and, in some species, sedation or light anaesthesia. EC does not induce any pain and no or minimal stress. It does not alter the cardiovascular function that it seeks to measure [99]. Similarly, EC has no or little interference with the measurement of other parameters recorded in toxicity or pharmacology studies and has no effect on the health status of the animal. EC measurements are easily repeatable and therefore allow subsequent follow-up in the same animal. However, rats and marmosets should be sedated or slightly anaesthetised for EC recording, and the drugs used for this purpose may have some effect on cardiac function and/or blood pressure. Therefore, sedation or anaesthesia may possibly interfere with the effects of the compound tested in the toxicology or pharmacology studies. 6. Conclusion EC is well established in different species of laboratory animals, in particular those used routinely in preclinical toxicology. A number of experiments have demonstrated that EC is a highly valuable tool for assessing the cause or the consequences of drug adverse effects on the cardiovascular system. In a number of examples, EC could replace invasive methods and complement other cardiovascular investigations, like ECG or histopathology. 7. Expert opinion EC is a key method for cardiologic examination in veterinary and human medicine, including human toxicology. It was extensively used in animal models of diseases, in particular models of cardiomyopathy induced by toxic doses of antracyclines. EC also provides a reliable tool for assessing pharmacological and therapeutic effects of drugs in animals. In contrast, EC has rarely been used in preclinical toxicology, possibly because of some technical constraints. However, a number of studies indicate that EC can accurately measure drug effects on cardiac function, their dose-relationship and time course. EC data are consistent with the known pharmacological effects of the drug and correlate well with invasive measurements. Moreover, a few experiments demonstrated that EC has successfully assessed cardiovascular adverse events in laboratory animals and have found a good consistency between morphological changes evaluated by EC and lesions seen at histopathological examination. The currently available literature on EC applications in humans and laboratory animals indicate therefore that this technology can generate key data in preclinical toxicology. Each EC examination provides a panel of quantitative and qualitative information on drug adverse effects on cardiac morphology and function. In particular, simultaneous recording of changes in cardiac structures, contractility and haemodynamics allow the establishment of correlations between the different drug adverse effects and to follow the evolution of cardiac toxic hits over time. Both the development and reversibility of cardiac adverse effects can be determined. Moreover, EC has a key ethical value, since it is a major refinement compared to invasive methods generally used to assess drug effects on the heart. We therefore strongly recommend developing EC as an investigative tool in preclinical toxicology laboratories. As EC recording investigates the same parameters of cardiac function and morphology in laboratory animals and humans, changes seen in preclinical toxicology can also be investigated in humans. When changes in EC end points are seen in animals, the clinicians can therefore select the cardiovascular examinations to be done for assessing the cardiac effects in clinical trials and ensure in this way the safety of volunteers or patients. In addition, EC will help in understanding the mechanism of development of cardiac lesions and in distinguishing cardiac toxicity due to direct action of the compound on the cardiac structures or function from adverse events due to exaggerated pharmacological effects. In this later case, the clinicians can monitor the volunteers or patients to ensure that the changes in cardiac function causing the lesions in laboratory animals do not occur in humans. The different EC modes give complementary data and are recommended to be used simultaneously for a full evaluation of drug effects. 2-D EC gives information on heart structures and allows an accurate calculation of ejection fraction. M-mode gives further information on cardiac dimensions and ventricular systolic function though calculation of fractional shortening. Thus, EF and fractional shortening, although derived from different EC modes, are both an index of cardiac contractility and changes in these parameters should be compared when assessing drug effects. Contrast Expert Opin. Drug Metab. Toxicol. (2008) 4(6) 691 Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology EC indicating the changes in myocardial perfusion can be associated to M-mode for evaluating the consequences of ischaemia on cardiac contractility (Figure 6). Doppler tissue imaging is an additional method for evaluating systolic function and has the advantage of being relatively independent of cardiac load [26]. Using pulsed Doppler it is possible to calculate a number of parameters characterising the flows through the atrio-ventricular and arterial orifices and then to evaluate the haemodynamic consequences of drug effects on myocardial function. Combination of M-mode and Doppler EC can therefore be used either to evaluate the consequences of drug-induced cardiac lesions or to investigate the pathogenesis of cardiac lesions produced by exaggerated cardiovascular pharmacological effects. Colour Doppler gives a picture of the flow patterns and has a particular interest for detecting disturbances resulting from valvular abnormalities, which are serious adverse effects of a number of drugs, in particular antiobesity compounds [100]. Contrast EC is the method of choice for evaluating changes in myocardial perfusion and therefore can be used as an application for assessing cardiac ischaemia produced by overdoses of different drugs, in particular vasodilators [97]. However, for providing reliable and accurate results, EC needs to be carried out by highly experienced and trained people who frequently perform EC examination. Therefore, some laboratories may consider it not worthwhile to ensure continuous training of staff for EC recording. In this case, it is possible to contract out EC examination in dogs to a local veterinary cardiologist who routinely uses EC in his/her practice. He/she can perform the EC examinations in the toxicology facilities of the pharmaceutical laboratory and provide data to the local scientists for interpretation. However, even when performed by experienced people, EC is overall less accurate than invasive methods and some variability in the results can be found between different experimenters or between different measurements of the same experimenter. It is therefore critical to have all EC examinations of a toxicity study carried out by the same experimenter [101]. It is also important to repeat the measurements at each experimental time point and to calculate the mean. Each measurement should be taken at least in triplicate and ideally in quintuplicate. As a consequence of the number of parameters that can be recorded and the need for repeated measurement at each time point, EC is time consuming and a complete examination takes at least 20 min. It is therefore critical to adapt the study design to the performance of the EC recording. A staggered start of the drug treatment can generally allow 692 the investigator to perform all the scheduled EC examinations in a study involving a large number of animals. At present, EC has only been used in a limited number of exploratory toxicity studies and if used in regulatory studies, it should be considered as a non-validated add-on. However, we expect that if the method is further developed as an investigative tool in toxicology, it will enter a validation process and will be recognised by authorities. For accurate EC recording, the animal involved should be quiet and motionless, standing or lying, depending on the incidence of the ultrasound beam. EC can thus be easily performed in dogs without any sedative medication, since these animals accept handling and restrain during the recording. Monkeys, rabbits and rodents should generally be anesthetised or at least sedated, which may interfere with the cardiac function and its sensitivity to drug action. It is therefore critical to establish a sedation process that has the minimum possible interaction with the cardiovascular function. The optimal method of sedation remains to be established and probably will vary in each species depending on the strain, pre-existing cardiac disease or compound to be tested [102]. EC examination without any medication in primates and rodents will require training of the animals and consequently be time consuming. Moreover, even when EC recording is technically feasible on non-sedated animals, the stress induced by restraint will probably affect the measured cardiac parameters. EC recording in non-sedated primates or rodents does therefore not appear to be recommended in toxicity studies. Despite some limitations, EC can therefore be considered a key method for preclinical investigation of drug adverse effects and has a major ethical value. Pharmaceutical companies and contract research operations should develop and validate EC in the laboratory animal species they use in toxicology. Due to its technical constraints, EC can probably not be recorded routinely in all toxicity studies. As a first step, the method can be applied to exploratory studies assessing the mechanism of development of cardiac lesions or their consequences on the cardiac function. As a later step, when the echocardiographic technology is adequately validated, it could be used in regulatory studies, when there is a possible risk of cardiovascular adverse effects. Acknowledgements We thank J Leaney for her critical review of the manuscript and F Besse for his help in formatting the figures in this article. Expert Opin. Drug Metab. Toxicol. (2008) 4(6) Hanton, Eder, Rochefort, Bonnet & Hyvelin Bibliography 11. Papers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers. 1. • Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. 2. • 3. 4. • 5. Waggoner AD, Pérez JE. Principles and physics of Doppler. Cardiol Clin 1990;8:173-90 A detailed review of Doppler technology. Bonagura JD, O’Grady MR, Herring DS. Echocardiography. Principles of interpretation. Vet Clin North Am Small Anim Pract 1985;15:1177-94 A review of EC in dogs. Schiller NB, Shah PM, Crawford M, et al. Recommendation for quantitation of the left ventricle by two-dimensional echocardiography. J Am Soc Echocardiogr 1989;2:358-67 Bonagura JD, Miller MW. Veterinary echocardiography. Echocardiography 1989;6:229-64 A full description of EC application in dogs. Hanton G, Geffray B, Lodola A. Echocardiography, a non-invasive method for the investigation of heart morphology and function in laboratory dogs: 1. Establishment of the method and reference values for M-mode parameters. Lab Anim 1998;32:173-82 6. Thomas WP. Two-dimensional real-time echocardiography in the dog. Vet Radiol 1984;25:50-64 7. Youn HJ, Rokosh G, Lester SJ, et al. Two-dimensional echocardiography with a 15-MHz transducer is a promising alternative for in vivo measurement of left ventricular mass in mice. J Am Soc Echocardiogr 1999;12:70-5 8. 9. 10. Gopal A, Shen Z, Sapin P, et al. Assessment of cardiac function by three-dimensional echocardiography compared with conventional non-invasive methods. Circulation 1995;92:842-53 Tsusaki H, Yonamine H, Tamai A, et al. Evaluation of cardiac function in primates using real-time three-dimensional echocardiography as applications to safety assessment. J Pharmacol Toxicol Methods 2005;52:182-7 Jiang L, Samuel C, Handschumacher MD, et al. Myocardial imaging: three-dimensional echocardiography: in vivo validation for right ventricular volume and function. Circulation 1994;89(5):2342-50 12. 13. 14. 15. • Shiota T, Jones M, Chikada M, et al. Real-time three-dimensional echocardiography for determining right ventricular stroke volume in an animal model of chronic right ventricular volume overload. Circulation 1998;97(19):1897-900 Höglund K, Bussadori C, Domenech O, et al. Contrast echocardiography in boxer dogs with and without aortic stenosis. J Vet Cardio 2007;9:15-24 Aronson S, Bender E, Feinstein SB, et al. Contrast echocardiography: a method to visualize changes in regional myocardial perfusion in the dog model for CABG surgery. Anesthesiol 1990;72:295-301 Oshita A, Ohmori K, Kondo I, et al. Myocardial blood flow measurements in rats with simple pulsing contrast echocardiography. Ultrasound Med Biol 2002;28:459-66 Thibault H, Lafitte S, Timperley J, et al. Quantitative analysis of myocardial perfusion in rats by contrast echocardiography. J Am Soc Echocardiogr 2005;18:1321-8 Application of contrast EC for investigation of cardiac perfusion in rats. 16. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation 1978;58:1072-83 17. Bonagura JD. M-mode echocardiography. Basic Principles. Vet Clin North Am Small Anim Pract 1983;13:299-319 18. Lombard CW. Normal values of the canine M-mode echocardiogram. Am J Vet Res 1984;45(10):2015-8 19. Belenkie I, Nutter DO, Clark DW, et al. Assessment of left ventricular dimensions and function by echocardiography. Am J Cardiol 1973;31:755-62 20. •• 21. Bonagura JD, Miller MW, Darke P. Doppler echocardiography I. Pulsed-wave and continuous-wave examination. Vet Clin North Am Small Anim Pract 1998;28:1325-59 A thorough review of Doppler EC in veterinary clinic. Brown DJ, Knight DH, King RR. Use of pulsed wave Doppler echocardiography to determine aortic and pulmonary velocity and flow variables in clinically normal dogs. Am J Vet Res 1991;52:543-50 Expert Opin. Drug Metab. Toxicol. (2008) 4(6) 22. Gramiak R, Holen J, Mose AJ, et al. Left coronary arterial blood flow: noninvasive detection by Doppler US. Radiology 1986;159:657-62 23. Ihlen H, Myhre E, Amlie JP, et al. Change in the left ventricle stroke volume measured by Doppler echocardiography. Br Heart J 1985;54:378-83 24. Darke PGG, Bonagura JD, Miller M. Transducer orientation for Doppler echocardiography in dogs. J Small Anim Pract 1993;34:2-8 25. Dubin J, Wallerson DC, Cody RJ, Devereux RB. Comparative accuracy of Doppler echocardiography methods for clinical stroke volume determination. Am Heart J 1990;120:116-23 26. Shimizu M, Konstantinov IE, Suess AM, et al. Noninvasive analysis of myocardial function using high-resolution Doppler Tissue echocardiography in rats. J Am Soc Echocardiogr 2005;18:461-7 27. Boissiere J, Gautier M, Machet M-C, et al. Doppler tissue imaging in assessment of pulmonary hypertension-induced right ventricle dysfunction. Am J Physiol Heart Circ Physiol 2005;269:H2450-5 28. Tei C, Ling, LH, Hodge DO, et al. New index of combined systolic and diastolic myocardial performance: a simple and reproducible measure of cardiac function – a study in normals and dilated cardiomyopathy. J Cardiol 1995;26:357-66 Detailed publication on tissue Doppler recording and measurements. • 29. • Tei C, Dujardin KS, Hodge DO, et al. Doppler index combining systolic and diastolic myocardial performance: clinical value in cardiac amyloidosis. J Am Coll Cardiol 1996;28:658-64 Detailed publication on tissue Doppler recording and measurements. 30. Sharma R, Pellerin D, Gaze DC, et al. Mitral peak Doppler E-wave to peak mitral annulus velocity ratio is an accurate estimate of left ventricular filling pressure and predicts mortality in end-stage renal disease. J Am Soc Echocardiogr 2006;19:266-73 31. Pombo JF, Troy BL, Russel RO. Left ventricular volumes and ejection fractions by echocardiography. Circulation 1971;43:480-90 32. Jones SE, Ewy GA, Groves BM. Echocardiographic detection of adriamycin heart disease. Proc Am Assoc Cancer Res 1975;16:228 693 Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology 33. 34. Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. •• 35. • 36. 37. 38. 39. Kraunz RF, Ryan TJ. Ultrasound measurements of ventricular wall motion following administration of vasoactive drugs. Am J Cardiol 1971;27:464-73 Crippa L, Ferro E, Melloni E, et al. Echocardiographic parameters and indices in the normal Beagle dog. Lab Anim 1992;26:190-5 A reference article for echocardiographic measurement of cardiac parameters in Beagle dogs. Hanton G, Eder V, Bonnet P, Rochefort GY. Echocardiography in marmosets: a non-invasive method for the assessment of cardiovascular toxicology and pharmacology. In: Weinbauer GF, Vogel F, editors, Novel approaches towards primate toxicology. Münster, Germany: Waxmann Publishing Co.; 2006. p. 27-45 The first description of the establishment of EC in marmosets. Horackova M, Arora R, Chen R, et al. Cell transplantation for treatment of acute myocardial infarction: unique capacity for repair by skeletal muscle satellite cells. Am J Physiol Heart Circ Physio 2004;287:H1599-1608 Kokubo M, Uemura A, Matsubara T, Murohara T. Noninvasive evaluation of the time course of change in cardiac function in spontaneously hypertensive rats by echocardiography. Hypertens Res 2005;28:601-9 Stypmann J, Engelen MA, Beithardt AK, et al. Doppler echocardiography and tissue Doppler imaging in the healthy rabbit: differences of cardiac function during awake and anaesthetised examination. Int J Cardiol 2007;115:164-70 Syed F, Diwan A, Hahn HS. Murine echocardiography: a practical approach for phenotyping genetically manipulated and surgically modeled mice. J Am Soc Echocardiogr 2005;18:982-90 40. Boon J, Wingfield WE, Miller CW. Echocardiographic indices in the normal dog. Vet Radiol 1983;24:214-21 41. Sisson D, Schaeffer D. Changes in linear dimensions of the heart, relative to body weight, as measured by M-mode echocardiography in growing dogs. Am J Vet Res 1991;52:1591-6 42. 694 Kirberger RM, Bland-van den Berg P, Darazs B. Doppler echocardiography in the normal dog: part I. Velocity findings and flow patterns. Vet Radiol Ultrasound 1992a;33:370-9 43. 44. 45. 46. 47. 48. 49. Kirberger RM, Bland-van den Berg P, Grimbeek RJ. Doppler echocardiography in the normal dog: part II. Factors influencing blood flow velocities and comparison between left and right heart blood flow. Vet Radiol Ultrasound 1992b;33:380-6 Nakayama T, Nishijima Y, Miyamoto M, Hamlin RL. Effects of 4 classes of cardiovascular drugs on ventricular function in dogs with mitral regurgitation. J Vet Int Med 2007;21:445-50 Christiansen S, Redmann K, Scheld HH, et al. Adriamycin-induced cardiomyopathy in the dog- an appropriate model for research on partial left ventriculectomy? J Heart Lung Transplant 2002;21:783-90 Christiansen S, Stypmann J, Jahn UR, et al. Partial left ventriculectomy in modified adriamycine-induced cardiomyopathy in the dog. J Heart Lung Transplant 2003;22:301-7 Monnet E, Orton C. A canine model of heart failure by intracoronary adriamycin injection: hemodynamic and energetic results. J Card Fail 1999;5:255-64 Murphy MP, Smith WJ, Aklog L, et al. A canine model of adriamycin-induced left ventricular dysfunction. Abstract from the 66th Scientific Sessions, American Health Association Congress, Atlanta, USA 1993. Circulation 1993;88:I-257 Allen DG. Echocardiography as a research and clinical tool in veterinary medicine. Can Vet J 1982;23:313-6 50. Vaynblat M, Chivarelli M, Ramdev G, et al. Enalapril prophylaxis of doxorubicin-induced cardiomyopathy. J Mol Cell Cardiol 1996;28:A201 51. Kittleson MD, Pipers FS, Knauer KW, et al. Echocardiographic and clinical effects of milrinone in dogs with myocardial failure. Am J Vet Res 1985;46:1659-64 52. Naguieh SF, Rao L, Jackson P, et al. Hemodynamic insight into the effects of ischemia and tachycardia on the tissue Doppler derived annular velocities. Scientific session of American Heart Association. Anaheim, CA, USA (2001). Circulation 2001;104:II-564 53. Hug M-C, Singer T. Echocardiography as a new tool in toxicology. 35th Eur Congress Toxicol, Alicante, Spain 1996. Toxicol Lett 1996;88(Suppl 1):105 54. Zabalgoitia M, Ventura J, Anderson L, et al. Morphologic and functional characterization of chagasic heart disease Expert Opin. Drug Metab. Toxicol. (2008) 4(6) in non-human primates. Am J Trop Med Hyg 2003;68:248-52 55. Shannon RP, Simon MA, Mathier MA, et al. Dilated cardiomyopathy associated with simian AIDS in nonhuman primates. Circulation 2000;101:185-93 56. Rishniv M, Schiavetta AM, Johnson TO, Erb HN. Cardiomyopathy in captive owl monkeys (Aotus nancymae). Comp Med 2005;55:162-8 57. Brady AG, Watford JW, Massey CV, et al. Studies of heart disease and failure in aged female squirrel monkeys (Saimiri sp). Comp Med 2003;53:657-62 58. Wondergem J, Persons K, Zurcher C, et al. Changes in circulating atrial natriuretic peptide in relation to the cardiac status of rhesus monkeys after total-body irradiation. Radiotherapy Oncol 1999;53:67-75 59. Korcarz CE, Padrid PA, Shroff SG, Lang RM. Doppler echocardiographic reference values for healthy rhesus monkeys under ketamine hydrochloride sedation. J Med Primatol 1997;26:287-98 60. Morita H. Ventricular wall thickness and blood pressure values in normal cynomolgus monkeys. J Vet Med Sci 1995;57:1045-8 61. Smith D, Trennery P, Farningham D, Klapwijk J. The selection of marmoset monkeys (Callithrix jacchus) in pharmaceutical toxicology. Lab Anim 2001;35:117-30 62. Reffelmann T, Kloner RA. Transthoracic echocardiography in rats. Evaluation of commonly used indices of left ventricular dimensions, contractile performance, and hypertrophiy in a genetic model of hypertrophic heart failure (SHHF-Mcc-facp-rats) in comparison with Wistar rats during aging. Basic Res Cardiol 2003;98:275-84 63. Hoit BD, Castro C, Bultron G, et al. Noninvasive evaluation of cardiac dysfunction by echocardiography in streptozotocin-induced diabetic rats. J Card Fail 1999;5:324-33 64. Krishna KM, Gopal GS, Chalam CR, et al. The influence of sulindac on diabetic cardiomyopathy: a non-invasive evaluation by Doppler echocardiography in streptozotocin-induced diabetic rats. Vasc Pharmacol 2005;43:91-100 65. Ferreira Cury A, Bonilha A, Saraiva R, et al. Myocardial performance index in female rats with myocardial infarction: relationship with ventricular function parameters by Hanton, Eder, Rochefort, Bonnet & Hyvelin Doppler echocardiography. J Am Soc Echocardiogr 2005;18:454-60 66. Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. Nozawa E, Kanashiro RM, Murad N, et al. Performance of two-dimensional Doppler echocardiography for the assessment of infarct size and left ventricular function in rats. Braz J Med Biol Res 2006;39:687-95 Saraiva RM, Kanashiro-Takeuchi RM, Antonio EL, et al. Rats with high left ventricular end-diastolic pressure can be identified by Doppler echocardiography one week after myocardial infarction. Braz J Med Biol Res 2007;40:1557-65 Yoshiyama M, Takeuchi K, Omura T, et al. Effects of candersartan and cilazapril on rats with myocardial infarction assessed by echocardiography. Hypertension 1999;33:961-8 Yoshiyama M, Takeuchi K, Omura T, et al. Effects of diltiazem on cardiac remodelling in rats assessed by Doppler echocardiography and mRNA expression. Cardiovasc Drug Ther 1999;13:249-58 Murakami K, Mizushige K, Noma T, et al. Effects of perindopril on left ventricular remodelling and aortic regurgitation in rats assessed by echocardiography. Angiology 2000;51:943-52 Pollick C, Hale SL, Kloner RA. Echocardiography and cardiac Doppler assessment in mice. J Am Soc Echocardiogr 1995;8:602-10 Tsujita Y, Kato T, Sussman MA. Evaluation of left ventricular function in cardiomyopathic mice by tissue Doppler and color M-mode Doppler echocardiography. Echocardiography 2005;22:245-52 Tan TP, Gao XM, Krawczyszyn M, et al. Assessment of cardiac function by echocardiography in conscious and anesthetized mice: importance of the autonomic nervous system and disease state. J Cardiovasc Pharmacol 2003;42(2):182-90 77. 78. 79. • Li J, Duan YY, Chen HM, et al. Left ventricular function of a rabbit model with acute thrombo-embolic pulmonary hypertension monitored by echocardiography [English abstract]. Chinese J Med Imaging Technol 2007;23:613-5 Bódi A, Szilágyi S, Edes I, Papp Z. The cardiotonic effects of levosimendan in guinea pig hearts are modulated by beta-adrenergic stimulation. Gen Physiol Biophys 2003;22:313-27 Hanton G. Preclinical Cardiac Safety Assessment of Pharmaceutical Compounds. Drug Res Develop 2007;8:213-28 81. Marchandise B, Schroeder E, Bosly A, et al. Early detection of doxorubicin cardiotoxicity: interest of Doppler echocardiographic analysis of left ventricular filling dynamics. Am Heart J 1989;118:92-8 An example of the usefulness of EC in clinical toxicology. • 82. 83. • 84. hypertrophy, myocardial contractility and load conditions in hemodialysis patients: an echocardiographic study. Am J Kidney Dis 1997;30:780-5 85. Rand JS, Reynolds WT, Priest J. Echocardiograpic evaluation of the effects of medetomidine and xylazine in dogs. Aust Vet J 1996;73:41-4 86. Hanai K, Takaba K, Manabe S, et al. Evaluation of cardiac function by echocardiography in dogs treated with doxorubicin. J Toxicol Sci 1996;21:1-10 87. Herman EH, Rerrans VJ, Young RSK, Hamlin RL. Pretreatment with ICRF-187 allows a marked increase in the total cumulative dose of doxorubicin tolerated by Beagle dogs. Drugs Exp Clin Res 1988;14(9):563-70 88. Desbuards N, Antier D, Apfeldorfer CS, et al. Dexfenfluramine discontinuous treatment does not worsen hypoxia-induced pulmonary vascular remodeling but activates RhoA/ROCK pathway: consequences on pulmonary hypertension. Eur J Pharmacol (submitted for publication) 89. Droogmans S, Franken PR, Garbar C, et al. In vivo model of drug-induced valvular heart disease in rats: pergolide-induced valvular heart disease demonstrated with echocardiography and correlation with pathology. Eur Heart J 2007;28:2156-62 90. Balazs T, Bloom S. Cardiotoxicity of adrenergic bronchodilator and vasodilating anti-hypertensive drugs. In: Van Stee EW, editor, Cardiovascular Toxicology. Raven Press; New York, USA: 1982. p. 199-220 A review of the cardiovascular toxicity of vasodilators. Kerut EK, Valina CM, Luka T, et al. Technique and imaging for transthoracic echocardiography of the laboratory pig. Echocardiography 2004;21:439-42 Description of the establishment of EC in pigs. 80. Raher MJ, Thibault H, Poh KK, et al. In vivo characterization of murine myocardial perfusion with myocardial contrast echocardiography: validation and application in nitric oxide synthase 3-deficient mice. Circulation 2007;116:1250-7 Gan L, Wikström J, Bergström G, Wandt B. Non-invasive imaging of coronary arteries in living mice using high-resolution echocardiography. Scand Cardiovasc J 2004;38:121-6 Fei HW, Wang XF, Xie MX, He YL. Tissue Doppler echocardiography to evaluate myocardial contraction improvement by autologous bone marrow stromal cell transplantation in adriamycin-induced cardiomyopathy rabbit model. 8th TESI Annual Meeting; 2005 Shangai, China. Tissue Eng 2006;12(4):1106 Sandor GS, Puterman M, Rogers P, et al. Early prediction of antracycline cardiomyopathy using standard M-mode and digitized echocardiography. Am J Pediatric Hematol Oncol 1992;14:151-7 Hanton G, Baneux PJR. Echocardiography in laboratory dogs: a method of refinement for the assessment of cardiovascular toxicology. Example of minoxidil and quinidine. In: Balls M, van Zeller AM, Halder ME, editors, Progress in the Reduction, Refinement and Replacement of Animal Experimentation. Amsterdam, The Netherlands: Elsevier; 2000. p. 1175-86 A review of the ethical value of EC in animal experimentation. Dahan M, Siohan P, Viron B, et al. Relationship between left ventricular Expert Opin. Drug Metab. Toxicol. (2008) 4(6) • 91. Detweiler DK. Spontaneous and arterial disease in the dog: pathology and pathogenesis. Toxicol Pathol 1989;17:94-108 92. Mesfin GM, Piper RC, DuCharme DW, et al. Pathogenesis of cardiovascular alterations in dogs treated with minoxidil. Toxicol Pathol 1989;17:164-81 A key article on the mechanism of development of cardiac toxicity produced by vasodilators. • 93. Hanton G, Lodola A. Echocardiography, a non-invasive method for the investigation of heart morphology and function in laboratory dogs: 2. Effects of minoxidil 695 Echocardiography, a non-invasive method for the assessment of cardiac function and morphology in preclinical drug toxicology and safety pharmacology • 94. • Expert Opin. Drug Metab. Toxicol. Downloaded from informahealthcare.com by University of Alberta on 05/10/10 For personal use only. 95. 96. • and quinidine on the left ventricle function. Lab Anim 1998;32:183-90 An example of the use of EC in preclinical evaluation of drug toxicity. 97. Hanton G, Gautier M, Bonnet P. Using M-mode and Doppler echocardiography to investigate the cardiotoxicity of minoxidil in Beagle dogs. Arch Toxicol 2004;78:40-8 An example of the use of EC in preclinical evaluation of drug toxicity. •• Hanton G, Le Net J-L, Abott D. Cardiovascular toxicity of UK-61,260, a PDE III inhibitor, in dogs. 21st meeting of the American College of Toxicology, San Diego, USA (2000). Proc Int J Toxicol 2000;19:28 Hanton G, Gautier M, Herbet A, Bonnet P. Effect of milrinone on echocardiographic parameters after single dose in Beagle dogs and relationship with drug-induced cardiotoxicity. Toxicol Lett 2005;155:307-17 An example of the use of EC in preclinical evaluation of drug toxicity. 696 View publication stats 98. 99. Dogterom P, Zbinden G, Reznik GK. Cardiotoxicity of vasodilators and positive inotropic/vasodilating drugs in dogs: an overview. Crit Rev Toxicol 1992;22:203-41 A review of the cardiovascular toxicity of vasodilators. 102. Roth DM, Swaney JS, Dalton ND, et al. Impact of anesthesia on cardiac function during echocardiography in mice. Am J Physiol Heart Circul Physiol 2002;282:H2134-40 Hanton G, Sobry C, Dagues N, et al. Cardiovascular toxicity of minoxidil in the marmoset (Submitted). Toxcol Lett Affiliation Mason SJ, Weiss JL, Weisfeld ML, et al. Exercise echocardiography: detection of wall motion abnormalities during ischemia. Circulation 1979;59:50-9 100. Fitzgerald LW, Burn TC, Brown BS, et al. Possible role of valvular serotonin 5HT2B receptors in the cardiopathy associated with fenfluramine. Mol Pharmacol 2000;57:75-81 101. Dukes-McEwan J, French AT, Corcoran BM. Doppler echocardiography in the dog: measurement variability and reproducibility. Vet Radiol Ultrasound 2002;43:144-52 Expert Opin. Drug Metab. Toxicol. (2008) 4(6) Gilles Hanton†1 DVM DABT, Véronique Eder2 MD PhD, Gael Rochefort2 PhD, Pierre Bonnet2 MD PhD & Jean-Marc Hyvelin2 PhD †Author for correspondence 1Associate Research Fellow Pfizer Global Research and Development, Department of Toxicology and Comparative Medicine, Z.I. Pocé sur Cisse, BP 159, F-37401 Amboise Cedex, France Tel: +33 2 47 23 77 27; Fax: +33 2 47 23 79 39; E-mail: gilles.hanton@yahoo.fr 2University François Rabelais, LABPART, EA3852, Faculty of Medicine, IFR 135, Boulevard Tonnellé, Tours, France