Validated robotic laparoscopic surgical training in a virtual
advertisement

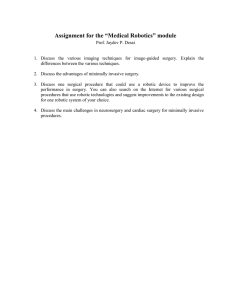
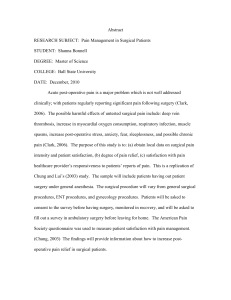
Surg Endosc DOI 10.1007/s00464-008-9894-z Validated robotic laparoscopic surgical training in a virtual-reality environment Dimitrios Katsavelis Æ Ka-Chun Siu Æ Bernadette Brown-Clerk Æ Irene H. Lee Æ Yong Kwon Lee Æ Dmitry Oleynikov Æ Nick Stergiou Received: 21 April 2007 / Accepted: 25 February 2008 Ó Springer Science+Business Media, LLC 2008 Abstract Background A robotic virtual-reality (VR) simulator has been developed to improve robot-assisted training for laparoscopic surgery and to enhance surgical performance in laparoscopic skills. The simulated VR training environment provides an effective approach to evaluate and improve surgical performance. This study presents our findings of the VR training environment for robotic laparoscopy. Methods Eight volunteers performed two inanimate tasks in both the VR and the actual training environment. The tasks were bimanual carrying (BC) and needle passing (NP). For the BC task, the volunteers simultaneously transferred two plastic pieces in opposite directions five times consecutively. The same volunteers passed a surgical needle through six pairs of holes in the NP task. Both tasks require significant bimanual coordination that mimics actual laparoscopic skills. Data analysis included time to task completion, speed and distance traveled of the instrument tip, as well as range of motion of the subject’s wrist and elbow of the right arm. Electromyography of the right wrist flexor and extensor were also analyzed. Paired t-tests and Pearson’s r were used to explore the differences and correlations between the two environments. A1 A2 A3 A4 A5 D. Katsavelis K.-C. Siu B. Brown-Clerk I. H. Lee N. Stergiou (&) HPER Biomechanics Lab, University of Nebraska at Omaha, Omaha, NE 68182-0216, USA e-mail: nstergiou@mail.unomaha.edu A6 A7 A8 A9 D. Katsavelis K.-C. Siu I. H. Lee Y. K. Lee D. Oleynikov N. Stergiou Department of Surgery, University of Nebraska Medical Center, Omaha, NE, USA Results There were no significant differences between the actual and the simulated VR environment with respect to the BC task, while there were significant differences in almost all dependent parameters for the NP task. Moderate to high correlations for most dependent parameters were revealed for both tasks. Conclusions Our data shows that the VR environment adequately simulated the BC task. The significant differences found for the NP task may be attributed to an oversimplification in the VR environment. However, they do point to the need for improvements in the complexity of our VR simulation. Further research work is needed to develop effective and reliable VR environments for robotic laparoscopic training. Keywords da Vinci surgical system Electromyography Kinematics Electrogoniometry Training It is well established that the reduced invasiveness of laparoscopic surgery results in superior patient outcomes as measured by a less painful recovery and an earlier return to a healthy status as compared with traditional open surgery [1]. However, laparoscopic surgery has also presented some disadvantages such as poor visualization, difficultness in wrist manipulation, and prolonged abnormal standing posture. Thus, robot-assisted laparoscopy has been developed to address these problems [2]. Recent studies comparing robot-assisted with conventional laparoscopy have shown improved surgical dexterity [3] and decreased training time for surgical residents [4–6]. However, despite the dramatic increase in the use of robotassisted surgery [7, 8], such technology has not been widely adopted into the educational curriculum of current 123 Surg Endosc training programs in general surgery [9]. A survey on residents’ preference, in a comparative study between the robotic and conventional techniques, showed that they would pursue a fellowship in robotic surgical training if it was available to them, while experienced surgeons appeared to be reluctant [10]. The relatively high cost of robot-assisted surgery, the absence of well-constructed training routines, and the lack of expert technical proficiency may be some of the reasons for the severely limited robotic surgical educational programs. Recently, an increasing number of studies have evaluate the surgeons’ performance in either inanimate [6, 11, 12] or animate [13, 14] models by using primarily qualitative measurements. Even though these studies lack direct applicability to clinical settings [13], their convenience and low cost make inanimate models essential during the initial stages of robotic training programs. Virtual reality (VR)—a form of inanimate model training—is considered an attractive, inexpensive, and user-friendly mean of motor learning [15, 16]. VR environments have been widely used to mimic general and specific surgical tasks, or even entire surgical procedures [16, 17]. However, there is not enough evidence to support whether these environments can actually mimic a surgeon’s performance in terms of kinematic and physiological parameters. Therefore, the purpose of the present study was to evaluate a proposed VR environment for robot-assisted surgery. We compared the VR environment with an actual training environment using two inanimate tasks that required significant bimanual coordination. These inanimate tasks have been used by others [12] in an effort to develop a training module for robotic laparoscopy. We hypothesized that kinematic and physiological measurements acquired while performing the inanimate tasks in the VR environment will not differ from those of the actual environment. Tasks The following two inanimate robotic surgical tasks were performed in this study: 1. 2. Bimanual carrying (BC), a pick-and-place task: picking up six 15 9 2 mm rubber pieces from a 30-mm metal cap with the right and left instruments, respectively, and carrying them to the opposite caps simultaneously (Fig. 1). Needle passing (NP), a ‘translational’ task: passing a 26-mm surgical needle through six pairs of holes made on the surface of a latex tube (Fig. 2). Our robotic VR simulator was constructed using the simulation software Webots (Cyberbotics Ltd., Lausanne, Switzerland) based on the specification provided by the dVSS company, Intuitive Surgical, Inc. The da Vinci instruments and training task platform were modeled as 3D objects using SolidWorks (SolidWorks Corp., Concord, MA, USA; Fig. 3). The simulation was overlaid on the screen inside the surgeon console of the dVSS, and driven by the kinematic data from the dVSS robot through Methods Subjects Eight volunteers including six medical students and two medical research fellows (four men and four women) with basic surgical knowledge and with no prior experience on the da Vinci surgical system (dVSS; Intuitive Surgical, Inc., Sunnyvale, CA, USA) were recruited to participate in this study. The mean (±standard deviation, SD) age of the participants was 28.8 (±6.2) years. All participants were right-handed. Informed consent was obtained from each subject prior to participation and was in accordance with the Institutional Review Board of the University of Nebraska Medical Center. 123 Fig. 1 The bimanual carrying (BC) task in (a) the actual and (b) the virtual environment Surg Endosc Fig. 3 The VR simulator (left) was constructed using the simulation software Webots (Cyberbotics Ltd., Lausanne, Switzerland). The da Vinci instruments and training task platform were modeled as 3D objects using SolidWorks (SolidWorks Corp., Concord, MA, USA). This simulation was driven by the kinematic data from the robotic operating console through LabVIEW (National Instruments, Austin, TX, USA) Measurements Fig. 2 The needle passing (NP) task in (a) the actual and (b) the virtual environment LabVIEW (National Instruments, Austin, TX, USA). All subjects were instructed to sit at the dVSS console while performing the training task in both actual and virtual environments. Experimental design All the participants were asked to perform both the BC and NP tasks in the actual and VR environment in one visit. At the beginning of the test, the participants received a verbal explanation about the use of the dVSS and testing procedures from the investigators. The participants familiarized themselves with the system, but not with the tasks, for 5 min. During this familiarization period, the participants were allowed to ask questions and receive further verbal explanation and suggestions from the investigators. After the familiarization, each participant performed five trials of each task for each environment. The order of the presentation of the tasks and the environments was randomized. Temporal and spatial variables with respect to the position and angular movement of the surgical instruments were measured for all tested conditions. The variables were acquired from the force transducers built into the system. They were extracted at a frequency of 11 Hz by the dVSS application programmer’s interface. These data sets were then processed using MATLAB 6.5 (The MathWorks Inc., MA, USA) to obtain linear kinematics with respect to the movement of the surgical instrument tips. Physiological measurements directly from the participants were acquired with electrogoniometers (Biometrics, Gwent, UK) that were placed at the wrist and elbow joints of the right arm and were used to obtain the subjects’ flexion and extension range of motion while performing the two tasks in the two environments. The muscular activation of two muscles was also monitored from the participants’ right forearm. These muscles were the flexor carpi radialis (FCR) and the extensor digitorum (ED), both of which are superficial and can be monitored by a Delsys surface electromyography (EMG) system (Delsys Inc., Boston, MA, USA). Although many other types of movements (e.g., flexion and extension of the thumb, index and middle fingers, forearm pronation and supination) and thus many other muscles are involved, it has been suggested [18, 19] that the contribution of these two muscles in the BC and NP tasks are considerably higher than all others. Consequently, measurement of the EMG activities performed by these muscles was important for the purpose of this study. 123 Surg Endosc Fig. 4 EMG analysis of the FCR: (a) graphical representation of the raw EMG signal, (b) rectification of the EMG signal, (c) root mean square of the normalized EMG signal, and (d) frequency spectrum analysis by using fast Fourier transformation Surface electrodes were placed over the bellies of these muscles, as described by Basmajian and Deluca [20]. The EMG data were collected and extracted at 1,000 Hz through a LabVIEW-based data acquisition board. These data sets were processed using MATLAB to obtain normalized EMG outputs (Fig. 4). Data analysis For each trial, task completion time (T) was calculated. Total traveling distance (D) and speed (S) with respect to the robot surgical instrument tips were calculated for each trial from the linear kinematics. In addition, wrist flexion/ extension range of motion (WROM) and elbow flexion/ extension range of motion (EROM) were calculated as the relative angle between the subject’s forearm and hand, and between upper arm and forearm, respectively. The EMG signals were then analyzed according to Narazaki et al. [18] and Judkins et al. [19]. The muscular activation volume (EMGv) is the integration of the normalized EMG output of the entire task, whereas the muscular activation rate (EMGr) is the average value of this task and it can be calculated by dividing EMGv by completion time. The median frequency (EMGfm) is the frequency response of each muscle. 123 Statistical analysis The mean values for the dependent variables of T, D, S, EMGv, EMGr, EMGfm, WROM, and EROM were compared between the actual and VR environments for both the BC and NP tasks with dependent t-tests (p = 0.05) using SPSS (version 12.0, SPSS Inc, IL, USA). Pearson’s correlation r was also used to identify correlations of the dependent variables between the actual and the VR condition. Results Significant differences were found for T (p = 0.003), D (p \ 0.001), WROM (p = 0.002), and EROM (p = 0.002) for the NP task, with the VR environment always producing lower values than the actual environment (Fig. 5). The only parameter that was not found to be significantly different was speed (p = 0.072). On the other hand, no significant differences were found between the actual and VR environment for the BC task (Fig. 6). Interestingly, Pearson’s r revealed similar correlations in the range of motion in both tasks, with EROM to display the highest value (r = 0.79 for BC; r = 0.78 for NP) and the WROM the lowest value (r = 0.21 for BC; r = 0.20 for NP). Surg Endosc Fig. 5 Comparison of the time to task completion, distance and speed of the instrument tip during the task, wrist and elbow range of motion between actual and VR environment in the NP task. All parameters except speed displayed significantly greater values for the actual environment (*p \ 0.05) Fig. 6 Comparison of the time to task completion, distance and speed of the instrument tip during the task, wrist and elbow range of motion between actual and VR environment for the BC task. There were no significant differences (p C 0.05) For the EMG, dependent t-tests between the actual and VR environments revealed that there were no significant differences for the BC task, but there were significant differences (p \ 0.05) for the NP task in most parameters, with the actual environment always producing higher values (Figs. 7 and 8). Specifically in the NP task, EMGr for both FCR (p = 0.003) and ED (p = 0.023) were significantly different. EMGv was also found to be significantly different for both muscle groups (p = 0.001 for FCR and p = 0.007 for ED). Pearson’s correlations between the two environments revealed r values from 0.41 to 0.93 for the NP task and from 0.17 to 0.91 for the BC task (Table 1). Discussion The purpose of the present study was to evaluate a proposed VR environment for robot-assisted surgery. We developed a dVSS robotic VR training simulator and compared the performance of two actual inanimate surgical tasks (NP and BC) between dVSS and VR simulator. Our results showed no significant differences for the BC task in all parameters between the actual and the VR environment, with moderate correlations for spatiotemporal parameters and high correlations for most EMG parameters. For the NP task, our results showed significant differences in most parameters with moderate correlations for spatiotemporal 123 Surg Endosc Fig. 7 Comparison of selected EMG parameters between actual and VR environment for the NP task. All parameters besides EMGfm displayed significantly greater values during the actual environment (*p \ 0.05) Fig. 8 Comparison of selected EMG parameters between actual and VR environment for the BC task. There were no significant differences (p C 0.05) Table 1 Pearson’s correlation r values for selected EMG parameters from the FCR and ED muscle groups between actual and VR environments in both BC and NP tasks Task EMGr EMGv RMGfm FCR ED FCR ED FCR ED BC 0.83 0.27 0.91 0.18 0.17 0.57 NP 0.93 0.53 0.86 0.46 0.87 0.41 parameters and high correlations for most EMG parameters. The noticeable differences in almost all parameters for the NP task imply that the VR environment did not sufficiently simulate the actual environment. Values during the VR environment appeared to be consistently lower. 123 A possible explanation for this behavior is the lack of the physical interaction feature of the simulated objects in the VR environment. Needle passing was simulated as a simultaneous overlap of two touch sensors attached to a cylindrical tube. Grasping the needle using the instrument tips and gravitational forces were not available. Therefore, the absence of physical interaction might have resulted in different motions of the telemanipulators, reduced muscle activation, and thus different motion of the instrument tips. The only parameters that did not yield significant differences were the median frequency of the FCR and ED muscle groups. Frequency analysis of the electromyographic signals from these muscles has proven to be an effective method of measuring muscle fatigue. Specifically, increased muscle fatigue is associated with a decreased median frequency of the power spectrum [20, 21]. Given Surg Endosc the short time to completion in both tasks as well as the small number of repetitions, it was expected that EMGfm would not yield significant differences. However, based on the reduced activation of the EMGr during NP on the VR environment, more repetitions of this task will probably elicit different results in terms of EMGfm. On the other hand, the VR environment for the BC task appeared to elicit similar behavior with the actual environment in both the FCR and ED muscle groups. The moderate to high correlations for most of the parameters and the lack of significant differences between the actual and VR environment imply that BC was simulated effectively. A number of studies have investigated the feasibility and validity of performance assessments with virtual-reality simulators. The main drawback in this procedure is the fact that the validity of performance assessment is limited by the reliability of such measurements [22]. Most of these studies did not make a direct comparison between the actual and virtual environment, but rather based the comparison on simple parameters, such as time to completion, to evaluate the effectiveness of such environments [22–24]. The strength of the present study is the direct comparison between the actual and VR environment, as well as the variety of measured parameters. A possible limitation of the present study is the high inter-subject variability due to the inexperience of the participants. As mentioned above, the average of five trials was used for data analysis. The differences in response among trials, especially from first to last, may distort the actual performance of the participants. However, participant selection was based on the fact that the proposed form of training is designed for the initial steps of a potential robotic surgical training program. The replication of the present study with more trained participants may increase the power and validity of the current findings. In conclusion, our study showed that the VR environment adequately simulated the BC task. The significant differences found for the NP task may be attributed to an oversimplification in the VR environment. Thus, they do point to the need for improvements in the complexity of our VR simulation. Along with the improvement of the NP task, by incorporating more physical interaction and the presence of a simulated needle, we are currently developing more complex and advanced training tasks for robotic surgery. These tasks will be evaluated in order to meet the specific physical and mechanical needs of the inanimate tasks. Further research is needed to develop effective and reliable VR trainers for robotic surgery and identify the training procedures needed to optimize learning and transfer these skills into the operating room. Acknowledgements This work was supported by NIH (K25HD047194), NIDRR (H133G040118), and the Nebraska Research Initiative. References 1. Satava RM, Bowersox JC, Mack M, Krummel TM (2001) Robotic surgery: state of the art and future trends. Contemp Surg 57:489–499 2. Robinson TN, Stiegmann GV (2004) Minimally invasive surgery. Endoscopy 36:48–51 3. Moorthy K, Munz Y, Dosis A, Hernandez J, Martin S, Bello F, Rockall T, Darzi A (2004) Dexterity enhancement with robotic surgery. Surg Endosc 18:790–795 4. Chang L, Satava RM, Pellegrini CA, Sinanan MN (2003) Robotic surgery: identifying the learning curve through objective measurement of skill. Surg Endosc 17:1744–1748 5. De Ugarte DA, Etzioni DA, Gracia C, Atkinson JB (2003) Roboticsurgery an resident training. Surg Endosc 17:960–963 6. Hernandez JD, Bann SD, Munz Y, Moorthy K, Datta V, Martin S, Dosis A, Bello F, Darzi A, Rockall T (2004) Qualitative and quantitative analysis of the learning curve of a simulated surgical task on the da Vinci system. Surg Endosc 18:372–378 7. Gutt CN, Oniu T, Mehrabi A, Kashfi A, Schemmer P, Buchler MW (2004) Robot-assisted abdominal surgery. Br J Surg 91:1390 – 1397 8. Hanly EJ, Marohn MR, Bachman SL, Talamini MA, Hacker SO, Howard RS, Schenkman NS (2004) Multiservice laparoscopic surgical training using the da Vinci surgical system. Am J Surg 187:309–315 9. Donias HW, Karamanoukian RL, Glick PL, Bergsland J, Karamanoukian HL (2002) Survey of resident training in robotic surgery. Am Surg 68:177–181 10. Guru KA, Kuvshinoff BW, Pavlov-Shapiro S, Bienko MB, Aftab MN, Brady WE, Mohler JL (2007) Impact of robotics and laparoscopy on surgical skills: a comparative study. J Am Coll Surg 204:96–101 11. Moorthy K, Munz Y, Dosis A, Hernandez J, Martin S, Bello F, Rockall T, Darzi A (2004) Dexterity enhancement with robotic surgery. Surg Endosc 18:790–795 12. Sarle R, Tewari A, Shrivastava A, Peabody J, Menon M (2004) Surgical robotics and laparoscopic training drills. J Endourol 18:63–67 13. Mehrabi A, Yetimoglu CL, Nickkholgh A, Kashfi A, Kienle P, Konstantinides L, Ahmadi MR, Fonouni H, Schemmer P, Friess H, Gebhard MM, Buchler MW, Schmidt J, Gutt CN (2006) Development and evaluation of a training module for the clinical introduction of the da Vinci robotic system in visceral and vascular surgery. Surg Endosc 20:1376–1382 14. Hanly EJ, Zand J, Bachman SL, Marohn MR, Talamini MA (2005) Value of SAGES Learning Center in introducing new technology. Surg Endosc 19:477–483 15. Dohi T (2004) The overview of robot surgery. Nippon Rinsho 62:824–830 16. Weiss H, Ortmaier T, Maass H, Hirzinger G, Kuehnapfel U (2003) A virtual-reality-based haptic surgical training system. Comput Aided Surg 8:269–272 17. Kypson A, Nifong LW, Chitwood Jr WR (2004) Robot-assisted surgery: training and re-training surgeons. Int J Med Robot 1:70–76 18. Narazaki K, Oleynikov D, Stergiou N (2006) Robotic surgery training and performance: identifying objective variables for quantifying the extent of proficiency. Surg Endosc 20:96–103 19. Judkins T, Oleynikov D, Narazaki K, Stergiou N (2006) Robotic surgery and training: electromyographic correlates of robotic laparoscopic training. Surg Endosc 20:824–829 123 Surg Endosc 20. Basmajian JV, De Luca CJ (1985) Muscles alive, their functions revealed by electromyography. Williams & Wilkins, Baltimore, MD 21. Bonato P, Roy SH, Knaflitz M, Luca CJD (2001) Time-frequency parameters of the surface myoelectric signal for assessing muscle fatigue during cyclic dynamic contractions. IEEE Trans Biomed Eng 48:745–753 22. Rosenthal R, Gantert WA, Scheidegger D, Oertli D (2006) Can skills assessment on a virtual reality trainer predict a surgical trainee’s talent in laparoscopic surgery? Surg Endosc 20:1286–1290 123 23. Grantcharov TP, Bardram L, Funch-Jensen P, Rosenberg J (2003) Learning curves and impact of previous operative experience on performance on a virtual reality simulator to test laparoscopic surgical skills. Am J Surg 185:146–149 24. Lehmann KS, Ritz JP, Maass H, Cakmak HK, Kuehnapfel UG, Germer CT, Bretthauer G, Buhr HJ (2005) A prospective randomized study to test the transfer of basic psychomotor skills from virtual reality to physical reality in a comparable training setting. Ann Surg 241:442–449