Florida Blue - Miscellaneous Drug
advertisement

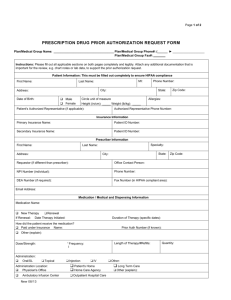
FLORIDA BLUE MISCELLANEOUS DRUG PRIOR AUTHORIZATION FORM ONLY the prescriber may complete this form. This form is for prospective, concurrent, and retrospective reviews. PLEASE NOTE: Incomplete forms will be returned for additional information. To ensure you are submitting this form correctly, you can complete and submit it directly to us online at www.covermymeds.com For formulary information, please visit the Florida Blue website at http://www.floridablue.com PATIENT INFORMATION Patient First Name: Patient Last Name: Patient Street Address: City, State MI: ZIP DOB (mm/dd/yyyy): AGE: Patient Phone: INSURANCE INFORMATION Patient ID Number: Group Number: PHYSICIAN/CLINIC INFORMATION Prescriber First Name: Prescriber Last Name: NPI: Specialty: Clinic Name: Contact Name: Phone: Secure Fax: Clinic Street Address: City, State ZIP MEDICAL INFORMATION. PLEASE ATTACH ADDITIONAL INFORMATION AS NEEDED. Patient Diagnosis with ICD-9 Code: ICD-10 Code: Medication and Strength Requested: Dosing Schedule: Quantity per Month: Is the patient currently treated with the requested medication?.............................................................................. ☐ Yes ☐ No If yes: When was treatment with the requested medication started? ______________________________ Please list all reasons for selecting the requested medication over alternatives (e.g., contraindications, allergies, history of adverse drug reactions to alternatives.) __________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________ Please list all medications the patient has previously tried and failed for treatment of this diagnosis. (Please specify if the patient has tried brand-name, generic, or over-the-counter products.) __________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________ Please list any other medications the patient will use in combination with the requested medication for treatment of this diagnosis. __________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________________ Please fax or mail this form to: Prime Therapeutics LLC Medical Drug Review Department 1305 Corporate Center Drive Eagan, Minnesota 55121 TOLL FREE FAX: 855.729.7216 PHONE: 866.260.0452 Misc_FL_CS_PAQL_MDRQ_AR0315 CONFIDENTIALITY NOTICE: This communication is intended only for the use of the individual entity to which it is addressed, and may contain information that is privileged or confidential. If the reader of this message is not the intended recipient, you are hereby notified that any dissemination, distribution or copying of this communication is strictly prohibited. If you have received this communication in error, please notify the sender immediately by telephone at 800.858.0723, and return the original message to Prime Therapeutics via U.S. Mail. Thank you for your cooperation. © PRIME THERAPEUTICS LLC Florida Blue and Florida Blue HMO Prescription Drug Benefits are administered by Prime Therapeutics, our pharmacy benefit manager (PBM). Patient First Name: Patient Last Name: MI: DOB (mm/dd/yyyy): Prescription Section Will you, acting as the patient’s agent, or will your patient be using Prime Therapeutics Specialty Pharmacy to process this prescription and fill the order?.................................................................................................................. ☐ Yes ☐ No If yes: Please use the section below to complete the prescription: If no: Please refer back to the Florida Blue website for additional information and the correct forms to submit for appropriate review (http://www.bcbsfl.com/DocumentLibrary/Providers/Content/Rx_PriorAuthorization.pdf). Medication Name, Form, Strength, Dose: __________________________________________________________________ Directions: __________________________________________________________________________________________ Frequency: Quantity: _________________________ Refills: NR 1 2 3 4 5 _____ ☐ Check this box if you would like the associated supplies dispensed along with injectable medications. PRESCRIBER SIGNATURE: Prescriber signature is required to validate prescriptions. _________________________________________________ ☐ Dispense as written Date Please fax or mail this form to: Prime Therapeutics LLC Medical Drug Review Department 1305 Corporate Center Drive Eagan, Minnesota 55121 TOLL FREE FAX: 855.729.7216 PHONE: 866.260.0452 Misc_FL_CS_PAQL_MDRQ_AR0315 ___________________________________________ ☐ Substitution permitted Date CONFIDENTIALITY NOTICE: This communication is intended only for the use of the individual entity to which it is addressed, and may contain information that is privileged or confidential. If the reader of this message is not the intended recipient, you are hereby notified that any dissemination, distribution or copying of this communication is strictly prohibited. If you have received this communication in error, please notify the sender immediately by telephone at 866.469.5660, and return the original message to Prime Therapeutics via U.S. Mail. Thank you for your cooperation. © PRIME THERAPEUTICS LLC Florida Blue and Florida Blue HMO Prescription Drug Benefits are administered by Prime Therapeutics, our pharmacy benefit manager (PBM).