Part B: Surgical Safety Checklist
“How-To” Implementation Guide
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Surgical Safety
Checklist “How-To”
Implementation Guide
This section sets out a step-by-step
approach hospitals can use to implement
the Surgical Safety Checklist in their
operating rooms. Hospitals are
encouraged to use this approach because
it focuses on improving compliance via
improved teamwork, communications,
and use of evidence-based practices.
For more information about the
background, evidence, and rationale
for surgical safety checklists, refer to the
Part A: Primer in this toolkit.
02
Table of Contents
This pull-out guide describes the “What you need to do” to implement a surgical safety checklist
program within your hospital.
Setting the Stage
Outlines important steps to engage all hospital leaders and stakeholders to introduce a checklist program.
The importance of preparing and encouraging all clinicians to “own” the checklist - including using local
evidence to create a case for use of the checklist.
1. Build Ownership and Buy-in......................................................................................................................05
2. Assess Current Practices and Risk of Complications from Surgery......................................................... 08
Getting Started
Steps to assist the checklist program leader with formation of pilot teams, raising awareness and launching a
checklist program, modification of the CPSI checklist, recommendations to consider when running through
the checklist, and overcoming common barriers to program implementation.
3. Form the Pilot Team(s).............................................................................................................................. 1 1
4. Public Reporting and the Surgical Safety Checklist................................................................................. 1 4
5. The CPSI Checklist and Detailed Explanation of Checklist Items.......................................................... 1 5
6. Consider Customizing the Checklist (includes modifications and compliance to public reporting)............ 29
7. Run the Checklist........................................................................................................................................32
8. Overcoming Barriers to Using the Checklist............................................................................................34
Moving to Full Implementation
Provides strategies to spread the checklist across your organization, including sharing successes, full scale roll
out, and sustainability ideas.
9. Spread the Checklist Across the Organization/ Share the Checklist’s Success...................................... 36
10. Sustain the New Practices...........................................................................................................................38
11. Address the Evidence-Based Practices Contained in the Checklist......................................................... 40
12. Identify Additional Opportunities for Quality Improvement.................................................................. 4 7
Checklists are designed to help team members exchange information, reduce communication failures, and
improve safety by:
•
•
•
Providing structured memory prompts to ensure that team members do not omit critical steps or established
safety practices.1,2,3
Identifying opportunities to share information about a patient that may not be known by all members of the team.4,5
Improving team building and communications between professionals and thereby increasing the team’s
ability to act as a “safety net” for the patient.6,7
03
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
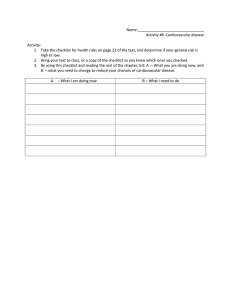
The steps involved in implementing the Surgical Safety Checklist include:
Setting the Stage
Getting Started
Moving to Full
Implementation
1. Build Ownership and Buy-in
2. Assess Current Practices and Risk
of Complications from Surgery
3. Form the Pilot Team(s)
4. Public Reporting and the Surgical Safety Checklist
5. The CPSI Checklist
6. Consider Customizing the Checklist
(includes modification compliance to public reporting)
7. Run the Checklist
8.Barriers to Using the Checklist
9.Spread the Checklist Across the
Organization
10. Sustain the New Practices
11. Address Evidence Based Practice Contained in the Checklist
12.Identify Additional Opportunities for Quality Improvement
As the diagram illustrates, some of the steps occur in sequence while others
should happen simultaneously. For example, identifying opportunities for
improvement in evidence based practices and developing new processes to
meet them can occur while test teams are being formed and the checklist is
being customized and run.
04
Setting the Stage
1. Build Ownership and Buy-In
While ultimate and final
accountability for the
checklist program resides
with the CEO and the
Board of Directors, the
direct responsibility for
actual delivery of the
program lies with the
Peri-operative Services
Advisory Committee.
To achieve the goals of the Safe Surgery Saves Lives Initiative and the Surgical
Safety Checklist, all members of the OR team must be fully engaged and
“own” the checklist. Ownership and buy-in requires the formal support and
endorsement of administrative and clinical/physician leaders.
Clinician support is critical. Any significant change to the design, process,
practice, or delivery of medical or surgical care can be challenging to
implement without strong engagement and acceptance.8
Establishing Clinician Ownership:
•
•
•
•
•
Physicians need to be involved at the outset in any decisions making that
concerns the delivery of care to patients, since they carry a powerful sense
of personal responsibility for the quality of care that they provide, as well as
the outcomes of their care*.
Reinforce that the checklist is a patient safety initiative, and that much of
the value in the tool pertains to common sense (i.e., every patient case is
discussed by the team, and all necessary preparations are made to ensure
patients receive any and all interventions that will lead to the best
possible outcome).
Encourage clinicians to mentor and influence their peer group.
Reinforce the systems perspective of patient safety and focus on the team*.
Consider harnessing the “logical negative” of those clinicians who historically
have been the most vocal or critical about changes and new programs. Seek
their active participation and keep an open mind to discover any previously
unreported problems with implementing new changes*. This will help produce
a realistic change plan well suited to the needs of individual organizations.
* Reinertsen JL, Gosfield AG, Rupp W, Whittington JW. Engaging Physicians in a
Shared Quality Agenda. IHI Innovation Series white paper. Cambridge, Massachusetts:
Institutive for Healthcare Improvement; 2007. (Available at www.IHI.org)
05
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
To obtain optimal buy-in, adoption and spread of the checklist among
clinical staff, consider the following:
1.
Identify senior leadership lead(s). Ensure that senior administrative
(e.g., corporate and clinical) leadership actively supports this initiative
and considers it a patient safety priority. Clinical staff will be more
likely to “buy in” when they believe their physician leaders are serious
about improving the quality of care of their patients.
The Role of Senior Leadership:
•
•
•
•
•
•
•
•
06
Support the use of the checklist as a communications tool to facilitate
teamwork and communication, not as another piece of documentation to
be completed for the chart.
Support the time and effort teams will need to implement the
checklist program.
Encourage pilot teams to test, modify and adapt the checklist to setting
and type of surgery (and not by individual preference).
Be visible and address concerns as teams pilot the checklist. People will
be more apt to adopt a tool if their concerns are addressed and they
receive positive feedback on how they are doing.
Encourage teams to collect proof that the checklist is working to
improve patient safety.
Support a highly visible, ongoing tracking record of the uptake and
implementation of the checklist across the organization. This may take the
form of a weekly (or daily) chart of accomplishments posted in a prominent
location in the OR.
Celebrate the work of champions and spread the news throughout the
organization via newsletters, banners, emails, notice boards, or lunch and
learn sessions. Make this an ongoing success story for your hospital.
Remember that clinicians are driven to change practice by local evidence
of improvements due to their change in practice. Measuring success will
help spread adoption of the checklist throughout the organization.
Champions are usually
highly-respected clinicians
who are not necessarily the
administrative leaders in
an organization. If they are
not in leadership roles, it is
important that they have the
full endorsement of senior
leadership. They have gained
respect from their colleagues
and are often early adopters
of emerging evidence-based
practice. They generally have
good social skills and may be
able to counteract other staff
resistance.*
* Reinertsen JL, Gosfield AG,
Rupp W, Whittington JW.
Engaging Physicians in a Shared
Quality Agenda. IHI Innovation
Series white paper. Cambridge,
Massachusetts: Institutive for
Healthcare Improvement; 2007.
(Available at www.IHI.org)
2. Formally engage the Perioperative Advisory Committee (or equivalent) to
formally endorse the checklist program in practice as well as principle.
3. Appoint a program lead or co-leads. These individuals will help coordinate
implementation of the checklist and provide instant feedback as teams
become more familiar with it.
4.
Engage other stakeholders in the process. Consider leaders in Patient Safety,
Quality, Risk Management, Pharmacy, Central Processing Department,
Information Technology, Decision Support, Blood Bank, Infection
Prevention and Control, Medicine, and others.
5.
Read this toolkit in its entirety. Ensure the checklist lead(s) and the
hospital’s Perioperative Services Advisory Committee read this toolkit. Encourage them to also read other resources such as the CPSI’s Implementation Kit for the Surgical Safety Checklist 9, and the WHO Guidelines for Safe Surgery 2009.10
6.
Establish physician, anesthesiologist, and nurse champion teams for every
surgical service if possible. Identify champions in various clinical
groups, such as professional practice leaders, team leaders, OR
educators, and clinical nurse specialists.
7.
Communicate and inform OR teams and other services in the organization
about what you are doing. The key messages located in appendix 11 - A40 may help with messaging. It is essential that consistent internal
messages and memos are shared with all internal stakeholders and
consistently come from the list below:
Senior
Administrators
CEO
Board of Directors
VP of Clinical Services
VP of Patient Services
Clinical Chiefs
Director/Manager
Chief of Surgery
Surgical Division Chiefs
Chief of Anesthesia
Chief Nursing Officer
Director of Peri-operative Services
Director of Surgery
OR Manager
Director of Risk Management
Director of Quality and Patient Safety
Perioperative Services Advisory Committee
Medical Advisory Committee
07
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
2.Assess Current Practices and Risk of
Complications from Surgery
To obtain ownership, buy-in, and a passion for change, it is highly
recommended to collect and share some local hospital data about risk of
complications from surgery in your hospital. This can be consolidated and
presented back to leadership and clinical teams, and will help to create a
platform for launch and implementation of the surgical safety checklist.
While collecting the evidence, it is important to ascertain the “current state”
of the operating room - including policies, processes, practices, safety and
teamwork cultures, and communication patterns. Statistics around adverse
events and rates of certain preventable complications (such as VTE) are also
useful. Approach your clinicians and identify how a surgical safety checklist
could improve issues and outcomes.
Appendix 5 - A27 of this toolkit includes a self-assessment audit tool that
hospitals may find helpful to assess their current OR practices.
To evaluate programs and assess for current practice and risk, consider
the following:
1.
Work with the hospital’s patient safety, quality, or risk lead. They may have
access and knowledge of information and quantitative data necessary to
prioritize some areas for improvement within the checklist program.
2. Determine the hospital’s “current state”. Assess processes and practices
in the operating room.
•
•
08
Use the Surgical Safety Checklist Self-Assessment Audit Tool
(see appendix 5 - A27). It includes questions about culture,
communications and teamwork, processes and practices around
select evidence based practices contained in the checklist.
Compare results with those reported in the OHA’s June 2009 survey
(see appendix 5 - A29) for benchmarking purposes. Identify gaps in
processes or evidence-based interventions.
•
3.
Determine the impact of culture, communication, and teamwork in the
OR. Teams that practice good communication and teamwork are more
likely to provide safe care.11 Consider completing a culture and
teamwork survey, such as the Safety Attitudes Questionnaire (for ORs).
Note: there is a cost to use the questionnaire. For an article about the
original SAQ questionnaire, see http://www.biomedcentral.com/
content/pdf/1472-6963-6-44.pdf.12
Create a gap analysis chart. This will help determine current state of
practice for each item or phase of the checklist, and define a program’s
strengths or areas for improvement. Add additional items or practices
that would constitute full wide-spread compliance with the intervention
(e.g., SSI, VTE).
Example of a Gap Analysis Chart
(using the Surgical Safety Checklist)
Checklist
item/phase
Full
compliance
Anesthesia
safety check
completed
prior to every
surgery
√
Site, side and
level marked
SSI:
Antibiotic
prophylaxis for
major general
surgery
Partial
compliance
No
compliance
Rating
Comment
strength
√
Improvement
needed
Practice varies
by surgeon/
anesthesiologist.
Need to
develop policy/
guidelines for
marking.
√
Improvement
needed
Timing is
late when
administered
on patient unit
09
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
4. Collect key quantitative information if available
•
•
•
•
10
Analyze reported incidents using your patient information or event
tracking system (either electronic or paper-based) and claims
information. Analyze the “easier to find” incidents which may relate to
surgical error (such as wrong site, wrong side, wrong patient, wrong
procedure, or unintended retained foreign objects). Look at data from
the past five years to get an idea of an organization’s rates and trends.
Determine the more “difficult to capture” incidents, such as mislabeled
specimens, medication errors, unsuitable or delayed equipment or
supplies. Keep in mind that the number of reported errors will be
directly proportional to the type of safety and reporting culture
at a hospital.
Determine the number of cases (or rates) of both VTE and SSIs. These
two preventable complications from surgery can be difficult to track
and may require the involvement of decision support and infection
control practitioners to extract and examine the data. It is essential to
capture both in-hospital and post-discharge events - using readmission
rates and/or imaging results – because a high proportion of
post-operative VTE and SSI occur after the initial surgical admission.
Consider doing a more thorough search of data related to surgical
complications. Some of the items in the box can be used as a list
of search terms for a clinical audit. For other potential complications
related to surgery, see the indicators listed in the Institute for
Healthcare Improvement’s Surgical Trigger Toolkit,13 including
change in procedure, transfer to higher level of care, and re-intubation
in the Post-Anesthesia Care Unit.
Easier to Find Incidents
(search terms):
Wrong site
Wrong side
Wrong patient
Wrong procedure
Foreign body in patient
Procedure not ordered
Consent missing or inadequate
Count incomplete or not
performed
Count incorrect
Surgical site infection
Deep vein thrombosis (DVT)
Pulmonary embolism (PE)
Other Search Terms:
Procedure not completed
Procedure cancelled or
not performed)
Break in sterile technique
Unanticipated insertion of
arterial or central venous
line during surgery
Unplanned return to OR
Unplanned intubation
5.
Rank probability and impact of the risk. This will help you determine
the areas of greatest priority for targeted quality improvement. For
more information on how to rank probability and impact of risk,
see appendix 10 - A39.
6.
Summarize and present this data to senior administration, the Perioperative
Services Advisory Committee, and OR teams. The numbers and trends of surgical complications may help build buy-in for using the checklist.
Consider telling a story about a previous preventable adverse event that occurred in the hospital, as well as any examples of when a potential
event was averted (i.e., a “good catch”). However, if a case is under review, consult with legal councel before sharing any facts with staff.
Getting Started
3. Form the Pilot Team(s)
1.
Start with the enthusiastic. In any new initiative, it is much easier to start
with the willing. Find people passionate about patient safety who are
willing to assist in laying the groundwork for implementing the checklist
in the OR. Try to include clinical champions from all professions
(surgery, anesthesiology, and nursing) as well as those in administrative
roles. Work with teams who already have high compliance to the
present “time out”.
2.
Assemble materials and raise awareness. Use information from the Part
A: Primer of the Surgical Safety Checklist Implementation Toolkit to present
evidence that the Surgical Safety Checklist is an effective way to build
teamwork and improve patient safety. Provide copies of the checklist
and various articles referenced in appendix 4 - A26. Tell staff that the
checklist is a tool that can improve process, and communication and
is not intended to be a documentation form. Explain that the
checklist is only an extension of the surgical pause or “time out” that
they are already doing.
11
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
3.
Choose a forum to introduce the Surgical Safety Checklist. It is important to
have a well planned communications strategy. Communication about
this program must reach all the stakeholders who will be affected by this
new process. Having a key champion present the same information at
all venues to all disciplines will ensure consistency in messaging.
•
•
•
12
Provide several different venues and opportunities for OR personnel
to attend and learn about the checklist and decide on a venue that will
be well received but that is also practical for the OR team.
Hold “lunch and learns” if teams are already keen to get started, or
dedicate a week of early morning coffee and muffin sessions whereby
staff could visit a “safe surgery information booth.”
For maximum exposure, use a large multi-disciplinary forum, such as
Grand Rounds, to share information about the initiative.
The goal is to ensure that everyone involved understands that the
checklist is the new expected standard of care. It’s important to
reinforce that all items in the checklist will contribute to improved
patient safety through better teamwork and communication.
4.
Invite a local guest speaker. Take advantage of clinician champions who
have already started using the checklist in their hospital. Invite local
and/or well respected guest speaker(s) who have used the checklist and
have them share their success stories.
5.
Form a “test team” and pilot the checklist. Once you have enough people
who are on board with this initiative, form the initial testing team to
provide feedback and modifications to the checklist, and decide where,
how and who should be testing it.
The core team(s) will need to trial the modified checklist and ensure
that it fits with the setting and types of surgeries it will be used for.
Start small in one OR suite or with one case per day. Have a week of
“practice runs” before committing to using the checklist for every
patient. Ensure all test team members have ample time to try the
checklist, provide input on what process is best to run the checklist, and
suggest any additional modifications that may be needed. Work out any
potential problems and make adjustments to your checklist before you
“go live”. Once the core team(s) is satisfied that the checklist can work
for one service or division, it will be well positioned for use throughout
the entire division.
6. Determine the best format for the checklist.
1. An oversized laminated checklist.
• Posted on the back of the operating theatre door and then
taken down and led by the designated checklist coordinator.
This ensures the checklist remains a conversation and not a
written tick box exercise.
• If you use this option, you will need separate documentation that
indicates the checklist was completed.
2. A paper form that resides on the patient’s chart.
• Read and marked by the individual who leads the conversation.
• Note that this option could lead to mindless box ticking, in which
case the inherent value of the conversation is lost. The upside is the
real time documentation that each item is discussed.
13
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
4. Public Reporting and the Surgical Safety Checklist
14
Compliance to the Surgical Safety
Checklist and Public Reporting
For the purposes of public reporting to the Ontario government, the case
definition is the percentage of surgeries in which a three-phased checklist
based on the CPSI checklist was performed.
The most basic reporting requirements of the surgical safety checklist will
entail a simple check of “yes” or “no” to a field prompt in the present Surgical
Efficiencies Target Program (SETp) ministry wait times electronic reporting
Operating Room Benchmark Collaborative (ORBC) system. It will replace
the “surgical pause – yes or no” prompt that is presently in place. Hospitals that
are not wait times funded, will have to collect data (either as an electronic
record or in a paper-based method), and report it through the Government of
Ontario’s Web-Enabled Reporting (WERS) system.
To check “yes” implies the OR team complies with completing a three-phased
surgical safety checklist for each individual surgical procedure and there was
no collapsing of the phases of the checklist (from three phases to two).
Compliance assumes the briefing was carried out while the patient was still
awake, and every phase had representation from the entire surgical team.
To ensure the best possible quality data, hospitals are encouraged to take steps
to ensure reliability of their process so that the data they submit is accurate
(see appendix 10 - A39).
Compliance with the checklist process includes principles of interprofessional
teamwork and communication with all relevant interventions for a surgical
procedure being discussed, as appropriate. This also includes taking steps to
address the evidence based practices that are contained in the checklist.
5. The CPSI Checklist and Detailed Explanation
of Checklist items
The CPSI Surgical Safety Checklist is a one-page list of 26 important patient
safety processes/items that surgical teams should discuss at three critical
points in surgery with all team members present:
1)
2)
3)
The preoperative evaluation of the conscious patient prior to induction
of anesthesia or “Briefing”.
The time out immediately prior to incision or “Time Out”.
The preparations for appropriate postoperative care prior to the patient
leaving the operating room or “Debriefing”.
The Briefing and Time Out phases of the checklist should be viewed as an
extended surgical pause during which team members verbally confirm the
identity of the patient, the operative site, and the procedure to be performed.
Also in these phases, team members should ensure that evidence-based
interventions are provided (e.g., prophylaxis against infection).
The Debriefing section of the checklist is a key opportunity to discuss future
ideas for quality improvement and learning. The final question -- “Could
anything have been done to make this case safer or more efficient?” -- will
allow every member of the team to provide their thoughts and plans to
address these issues. These kinds of conversations may not otherwise
occur once the team has left the operating room. Used in this manner, the
Surgical Safety Checklist should take no more than one minute per section.
The following checklist and explanation of checklist items has been
reprinted with the permission of the Canadian Patient Safety Institute,
as presented in their Detailed Explanation of the Surgical Safety Checklist
Items manual (www.safesurgerysaveslives.ca).
15
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
16
17
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
18
19
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
20
21
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
22
23
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
24
25
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
26
27
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
28
The Surgical Safety
Checklist is available
in an electronic Word
format, making it easily
customizable. For example,
hospitals can add their
logos and add or remove
items within a section as
required by each unique
surgical setting.
It is important to not
remove safety items
from the checklist simply
because they cannot
accomplished*. Some items
on the checklist, such as
antibiotic prophylaxis and
medications, may require
OR teams to make process
changes to the delivery
of care.
*Implementation Kit For the
Surgical Safety Checklist;
Canadian Patient Safety
Institute, May 2009. www.
patientsafetyinstitute.ca
6. Consider Customizing the Checklist
The CPSI Surgical Safety Checklist is the provincial standard. It aligns with
other Canadian initiatives such as SSI prevention and VTE prophylaxis,
supported by Safer Healthcare Now! However, the full Surgical Safety
Checklist may not be appropriate for all surgeries.
If customizing the checklist, hospitals should proceed with caution and
consider the following:
1.
The Perioperative Services Advisory Committee should work with the pilot team during the customization process and approves any modifications.
2.
Changes should be driven by best practices for improved patient safety.
Modifications to the checklist should be driven by surgery type rather than by individual preference. For example, the items to verify patient, site, side, procedure, and allergies are highly relevant for both minor procedures and major operations. However, the items on blood loss and VTE prophylaxis are not relevant for cataract surgery.
For additional information regarding the rationale for the 19 essential
items on the original WHO checklist, see the detailed Guidelines for
Safe Surgery manual on WHO’s website.14
3.
How to handle interventions on the checklist that are only in a
developmental stage. Even if your hospital has not yet fully implemented
SSI or VTE prevention, keep these items on the checklist. Make a
definitive plan to implement these practices, and ask teams to address
them when running the checklist by stating something to the effect of:
“We can’t do this today, but we are in the process of implementing VTE
as a standard part of patient care, and we will do this as soon as we can.”
4.
OR teams and other professionals need to be included in modification processes.
Encourage OR teams to discuss and test modifications to the checklist
and provide feedback and recommendations to the Perioperative
Services Advisory Committee. There may also be other clinical
specialties that can provide valuable input such as pharmacy, perfusionists, blood bank, respiratory therapists, and medicine.
29
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
5.
What will work best to promote teamwork and a patient safety culture? Some
hospitals have opted to separate items within the phases of the checklist
by role (e.g., nursing, anesthesiology, surgery) to ensure all disciplines
have an opportunity to speak. See examples of these types
of communication modifications in appendix 1.
6.
Limit the number of checklists used within the organization. Some hospitals
may decide to use one comprehensive checklist for all surgeries, with
minor surgery teams agreeing to review relevant information only,
stating “not applicable” to items that are not pertinent to that type of
surgery. Other hospitals may choose to have several checklists, for
example a shorter “high-volume” checklist for minor surgeries and
a longer “standard” version. Some exceptions may apply for certain
specialties, such as cataract surgery and caesarean section. Multi-site
hospitals using separate site checklists could cause confusion and/or
frustration for team members travelling and working between sites.
7.
Resist the temptation to add many new items to the checklist or to combine it
with other checklists. One long checklist could become cumbersome for
your teams. Always keep in mind that the checklist is a communication
improvement tool and not a documentation form.
For more guidance related to checklist modifications see appendix 9, the CPSI has available a “Human Factors Guidelines for Redesigning the
Checklist” and the WHO has created a “Surgical Safety Checklist Adaptation Guide”. Additional examples of modified checklists are also available in appendix 1 of this toolkit.
8. Pilot test the customized checklist for functionality. Initial piloting should be
done in only a few operating rooms or services.
•
•
30
Give ample time for test teams to try modifications to the checklist
before the Perioperative Services Advisory Committee makes
final decisions.
A quality improvement methodology approach -- including Plan Do
Study Act (PDSA) cycles - may work well for some teams
(see appendix 10 - A39).
•
•
•
•
•
•
Invite those who have tested the modified checklist to a quick meeting
at the end of the week or, for immediate feedback, write down what
worked well and what didn’t in a log book outside the pilot OR.
This may allow the more quiet members of the team to share their
opinions freely.
Prompt teams with questions such as how many minutes it took to run
the checklist or how the role of Checklist Coordinator is going.
The core team can take this information, plan next steps and test the
appropriate changes the following week.
Keep the same questions to see if there are any positive changes.
Teams may take several months and make 10 or more modifications to
the checklist as improvement cycles continue. This is common.
Once final modifications are made to the checklist, it can be formally
rolled out to the rest of the organization.
For examples of high volume and standard checklists, see appendix 1.
Customizing for Pediatric Populations
Populations such as pediatric patients may present unique challenges that may
not currently permit a full Briefing phase to be completed before the induction
of anesthesia, distinct from the pre-incision Time Out phase. Nevertheless, as a
patient safety initiative, the goal remains to prevent incorrect Briefing elements
from occurring prior to the induction of anesthesia, especially if they would have
precluded or altered the plan for proceeding with the anesthetic.
In addition, some checklist elements may not be as applicable on a routine basis in
the pediatric population (e.g., VTE prophylaxis), while other elements not on the
CPSI checklist template (e.g., Sickle Cell Disease testing) may need to be added.
31
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Customization of the Checklist and Public Reporting
To ensure compliance with public reporting, adhere to three distinct phases
when modifying and carrying out the Surgical Safety Checklist. For the purposes
of public reporting to the Ministry of Health and Long-Term Care, this indicator will
only be reported as one check (overall as “yes or no” compliance), but includes:
•
•
•
Briefing (before induction of anesthesia)
Time out (after induction, before initial incision)
Debriefing (during or after closure)
Do not collapse the checklist into two phases. Collapsing the checklist involves
removing an entire phase or combining Briefing and Timeout into one phase.
A representative from each professional discipline is expected to be present at
each phase: this participation is essential to ensure interdisciplinary teamwork,
communication and optimal patient safety.
Print these steps and
include them on the
back of a laminated copy
of the checklist.
32
7. Run the Checklist
Here are the steps to running the checklist.
1.
Who should be present? All members and/or representatives of the
surgical team (surgeon or resident, anesthesiology, nursing) should be
present for every phase. Although getting everyone together just before
induction can be challenging, it is important, for optimal patient safety,
that all members involved in the patient’s surgery have access to the
right information at the right time.
2.
Who takes responsibility for running the checklist? The entire team is
ultimately responsible for ensuring the checklist is completed.
However, some organizations may assign this responsibility to a
“Checklist Coordinator,” such as the surgeon, circulating or scrub
nurse, or anesthesiologist.
3. Where and when to run the checklist? Run the checklist in the OR, or in
the holding area. The Briefing should be done before induction, while
the patient is awake, either with or without the patient in the room.
The checklist should not
be read to merely “go
through the motions”.
If experiencing regular
difficulties from specific
team members, seek
to resolve the situation
by consulting with the
Perioperative Services
Advisory Committee and
senior leadership.
4.
How will the patient react? The decision to run the checklist in front of
the patient is up to each hospital. Many patients welcome and
appreciate this approach, especially if it is explained ahead of time
(i.e., either in the surgeon’s office, pre-op clinic, or in a pre-admission
package). Some OR teams may be concerned that patients will become
alarmed by discussions of blood loss. Patients should already have
been advised about surgical risks as part of their consent to the
procedure. However, if clinicians do not wish to do the Briefing in
front of patients, or patients do not wish to hear, the team should make
appropriate alternative arrangements.
5.
How to run through the checklist? There are several alternatives. One is to
designate a “Checklist Coordinator”. Any profession can take this role.
The coordinator leads the checklist by posing each item either
as a question to the others (if an intervention has been done) or as
a confirmation with details (if that item is applicable to their expertise).
Someone on the team should confirm that each item or task has been
completed and that there are no concerns. If there is no answer from
either another team member or the Checklist Coordinator, the team
should not continue with the next item until the necessary information
is exchanged. Each team member will have discipline-specific
information that should be shared.
Another alternative is to discuss items by relevant role. Each profession
is responsible for speaking to the items related to their knowledge of
the patient/procedure. Or, one profession could ask another profession
the questions that pertain to their role (e.g., anesthesiology asks items
related to nursing).
6.
Can work continue at the same time as running through the checklist? To fully realize its patient safety potential, the checklist should be regarded as an “extended surgical pause” or “extended time out”. It is strongly recommended that
the team stop all individual task work during the “Briefing” and “Time Out” sections of the checklist. The entire team should fully concentrate and
actively participate.
33
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
7. Ensure the team goes through all three phases. Completing the Debriefing
phase will be a new process, and will have its own challenges. Some
staff may have to leave to attend other duties, so the Debriefing may
be discussed just prior to or while the case is closing. It presents the
best time to discuss post-operative plans, and quality improvement
plans for future cases.
Think of ways to improve surgical team communication:
•
•
Try to break up the checklist by profession, and have each profession be
responsible for going through their most relevant section.
Or, have each profession be responsible for asking the other profession a
selection of questions on the checklist (for example, nursing asks
anesthesiology about all anesthesia relevant interventions).
8. Overcoming Barriers to Using the Checklist
Resistance or barriers may arise when implementing the Surgical Safety
Checklist. Here are some common ones and ways to overcome them:
The checklist involves a change in practice. Teams may need to change processes
and practices to meet some of the evidence-based interventions in the
checklist. This will require education and support and may involve the
forming of separate working groups and the appointing of champions to
help lead the changes (see appendix 7 and 8 for evidence based practice,
and appendix 10 - A39). Respect and collaboration of all disciplines is key to
process and practice change.
34
The checklist involves a change in culture. Surgical, anesthesia, nursing, and OR
teams all have different cultures and hierarchies. Each profession must take
part in the initiative for it to succeed. This may require a comprehensive
effort on the part of the organization to help change the culture of the
OR. The active participation of senior administration can help. Encourage
administrators to meet with staff, listen to problems, and work with them
to overcome barriers. Encourage open communication by having senior
leadership perform OR walk-arounds. To build teams, frontline workers
need to feel supported by senior leadership and have opportunities to
communicate directly with them. Nurses and other team members also need
to be empowered to speak up and stop the running of the checklist if it is not
followed in an appropriate manner.
There will be a new flow in the OR. Some team members may worry that the process
will slow the flow through the OR. Initially the flow may be slower, as teams get
used to the checklist. But, with time and experience, teams will find that it takes
very little time (approximately one minute for each phase). Skeptical clinicians
will be more likely to “buy in” if they see the checklist can save them time.
Ask test teams to document any time savings (e.g., fewer work-arounds to get
equipment and supplies) in written logs.
Gathering the entire team for a Briefing is a change in routine. There will be some
clinicians who may have to change their regular routines in order to attend the
Briefing before patient induction. Reinforce that the goal of the Briefing is to
improve team communication and patient safety, and highlight the benefits of
having the entire team present with the patient still awake during the Briefing.
The Briefing phase ensures all professions confirm adequate preparations for
surgery have been made so that optimal patient safety can be achieved.
The checklist is seen as an add-on task rather than an integral part of patient safety.
Some members of the team may become antagonistic if they see the Checklist
Coordinator as a “policing role” in the OR (rather than someone working
within the team to improve patient safety). It is important to allow time to adapt
to the “new normal”. If problems with the same individuals persist over time,
it is important to have a strategy in place to address them. It may be easier to
address the small number of resisters after the wider implementation of the
Surgical Safety Checklist when the majority of clinicians are accepting and
supportive of the initiative.
35
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Moving to Full Implementation
9. Spread the Checklist Across the Organization/
Share the Checklist’s Success
To help create buy-in and readiness for using the Surgical Safety Checklist
throughout the hospital, it is important to share information about the pilot
tests with all OR teams.
1.
Collect and share positive preliminary data. Collect early evidence that
OR staff can easily see. Keep a log of “good catches” and post it in a
common area. Write down success stories of saved time, improved
flow, or improved teamwork to help raise awareness and improve
team camaraderie.
2. Post the question: “Would you want the Surgical Safety Checklist done for you if
you were having surgery?” Let teams write their answer below.
3. Ask patients pre- or post-operatively if they feel safer knowing the checklist is
being used. Share their answers with the teams.
Posters and bulletin boards
work well to spread the
news and make other staff
in the OR aware that the
checklist is being rolled out.
36
4. Spread the news and celebrate successes. Share the good work and
successes of the teams who are testing and running the checklist.
•
•
•
•
Encourage staff to speak out and to collaborate with their colleagues.
They should be encouraged to plant the seeds of success and share
their positive experiences.
Celebrate the fact that many teams may become more sensitive to
picking up potential sources of error and work proactively to become
tighter “safety nets” for the patients.
Ask teams to submit articles, stories and anecdotes about their pilot
testing experience and print them in your internal messaging system,
OR newsletters, or corporate newsletter.
Include thank you notes from senior administration and other leaders
to make people feel that their efforts are being noticed.
Full-Scale Rollout
Once the new process has been tested and shown to make improvements, it
should be more widely accepted, and changes can be implemented across
the hospital, developing a “new norm”. Once the Perioperative Services
Advisory Committee is satisfied that a checklist can be rolled out to the
broader organization, the following strategies may be helpful to increase
widespread use:
1.
Introduce the checklist into a new service or OR every week (depending upon
the size of the organization).
2.
Make sure that all staff receive written communication and notice of the launch
date and upcoming roll out schedule. Include endorsement letters from the
Perioperative Services Advisory Committee, senior administration, and physician champions. Make all the materials that were provided to test teams, such as FAQs, evidence, and articles available to everyone.
3. Build in sufficient time to allow staff to attend scheduled education sessions, and
include discussion of the checklist in morning huddles.
4.
Consider creating a policy
for the Surgical Safety
Checklist once the tool
and process for completion
has been trialled, revised
and agreed upon. This
policy can then be used for
teaching and to assist in
the standardization in
the Surgical Safety
Checklist process.
Provide day-to-day leadership support to help teams learn about and implement
the Surgical Safety Checklist process. The constant physical presence of
OR educators, mentoring clinicians from all professional disciplines,
and leads and co-leads of the checklist program is important to prevent
early frustration and resistance to the program.
5. Continue to congratulate and celebrate success of those participating, and
share these messages across the hospital.
6.
Engage late adopters. As much as possible, clinicians should be encouraged to
influence their peers. Consider posting data comparing the rates of
compliance in different teams. This may help sway clinicians who may not
want to be seen to practice differently from their colleagues. However, some
people may continue to resist the use of the checklist, even after the broad
rollout of the initiative across the organization. As a last resort, it may be
necessary to inform these individuals that the current practice is no longer
an option, especially given the requirement for public reporting of
compliance with the Surgical Safety Checklist. Plan who will deliver this
message; it is advised that this be handled at the senior administrative level.
37
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
10. Sustain the New Practices
It will take time for the Surgical Safety Checklist to take hold and spread
throughout hospital ORs. It will also take ongoing effort to sustain its
momentum. Over time, teams may lose some of the initial enthusiasm of
running the checklist. As time pressures and demands increase, teams may
start rushing through in a “tick and flick” manner. Ongoing monitoring
and support of this process – including occasional direct audits -- is essential
to ensure proper adherence. Monthly or quarterly compliance reports are
useful to monitor sustainability (see appendix 10 - A39 for more information
on monitoring).
Follow these steps to maintain the use of the checklist, sustain the new
practices, and meet reporting requirements:
38
1.
Continue to support surgical teams. Provide education and support as
required to help teams use the checklist and implement best
practices effectively.
2.
Audit practice. Periodic random sampling “snapshot” audits are a good
way to ensure the process is working as intended. Collecting data
on overall use of the checklist and possibly compliance with individual
components or phases may help direct sustainability efforts, and focus
on areas for continued improvement.
When developing audit tools, consider examining current process for
quality checks of data submitted to the Government of Ontario
(e.g., SETp surgical pause indicator, or SSI on-time antibiotic prophylaxis).
If a method to audit processes is in place, it may be helpful to revisit and use
previous lessons learned to audit for the Surgical Safety Checklist. Consider
in the audit, different operating room teams, surgical divisions, times of day,
and OR suites; consider having an OR educator, OR manager, or trained
student observing processes; or randomly interview professionals who have
just completed surgery.
3.
Communicate improvement data and keep teams motivated. Share
information about reductions in surgical complications, “good
catches” that were caught by teams, improvements in patient safety,
patient satisfaction, teamwork, communication, and staff satisfaction to
show how well the new process is working. It is ideal to show the data
over time in an annotated run chart. Continue informing everyone
affected by the change in practice about the progress being made, and
focus on the overall aim15 to improve patient safety.
4.
Document results and ensure data quality: Ensure there is appropriate
documentation identifying whether the checklist was actually done.
How to document is best left to individual hospitals, however a clear
policy and process should be established. For Wait Times-funded,
Surgical Efficiencies Targets Program (SETp) hospitals, the absolute
minimal documentation entails the entry of checklist completion into
the ORBC system. However, for quality purposes, it is recommended
that there be another documentation process for the patient’s record.
Some facilities have decided that compliance should be dictated or
written into the surgeons operating room note (as part of
ensuring ownership).
Other hospitals have built a check for the checklist as a mandatory field of
their electronic system (i.e., Meditech or PICIS) as one check (completed or
not completed) or as three checks (one for Briefing, Time out, and
Debriefing). Other hospitals are choosing to physically mark the checklist
directly as phases are completed in surgery with the paper copy included
the patient chart.
5. Assign accountability for documentation of surgical checklist completion by
profession or role (e.g., surgeon, anesthesiologist, circulating nurse).
6.
Consider documenting compliance to each phase separately to remind clinicians that they need to complete each phase and to target future
quality improvement efforts. For example, if the Debriefing phase is seen to have the lowest compliance, a targeted effort can be made to improve compliance to this phase.
39
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
7.
Some hospitals have moved ahead to request an “incident report” if the checklist
or any phase has been omitted, which is another way to capture data about
compliance in the OR.
11. Address the Evidence-Based Practices
Contained in the Checklist
A significant amount of research supports evidence based practices for the
prevention of the following surgical complications: VTE, wrong site surgery,
medication errors, and surgical site infections. Elements of the surgical
safety checklist support prevention of these complications and are located
on the CPSI checklist and are considered to be integral to hospitals’ efforts
in providing safe, quality patient care. The OHA and the Government of
Ontario strongly recommend that hospitals integrate these practices into
their surgical checklist program and utilize practice guidelines available
from Safer Healthcare Now! More information and references are located in
appendix 7 and 8 of this toolkit.
40
Compliance with the VTE prophylaxis component of the Safe
Surgery Checklist involves the following principles:
VTE Prevention*
Despite compelling evidence that thromboprophylaxis reduces the
morbidity and mortality from VTE after surgery, consistent adherence
to optimal practice remains low. In a national survey sent to all Canadian
hospitals, 94% of hospitals reported that they routinely provided
thromboprophylaxis to hip replacement patients, but only 33%
reported routinely providing thromboprophylaxis to patients
undergoing major general surgery. (See pages 34 and 35 of Part A: Primer)
Preventative Actions*
A proactive VTE prevention strategy means using evidence-based
guidelines to assess patients and/or patient groups for risk of VTE and
to consistently deliver an appropriate anticoagulant and/or mechanical
method of thromboprophylaxis to all patients with sufficient risk.
This best practice involves selecting an appropriate prophylaxis
option, at the optimal dose, starting at the optimal time, and
continuing for an appropriate duration of time.
•
•
Assess all patients for their risk of VTE. In some surgical patients or
patient groups, the VTE risk is too low to warrant the routine use of
thromboprophylaxis. However, in all surgical patients, the need for
thromboprophylaxis (or not) should be an active decision. Most
inpatients undergoing major surgery warrant thromboprophylaxis.
Assessment of VTE risk can be done at the group level (for
example, all colorectal surgery patients or all hip arthroplasty
patients have sufficient thromboembolic risk to warrant
thromboprophylaxis, but most patients undergoing an
uncomplicated inguinal hernia repair do not) or thromboembolic
risk can be made at the individual patient level. See appendix 7 - A31
for recommended prophylaxis options for various patient groups.
41
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Continued...
•
•
Consider patient risk of bleeding. Patients with active bleeding or
those at high risk of bleeding should either not receive
anticoagulant-based thromboprophylaxis or have it be delayed
until the bleeding risk decreases. For patients who warrant
thromboprophylaxis based on their VTE risk but in whom
anticoagulant prophylaxis is contraindicated because of bleeding
risk, a non-pharmacologic, mechanical method of prophylaxis
should be used.
Address the need for thromboprophylaxis both in advance
of surgery and post-operatively. In some cases, it is appropriate
to commence thromboprophylaxis before surgery while, in
other cases, VTE prophylaxis may be commenced
postoperatively. Non-pharmacologic, mechanical methods of
prophylaxis should generally start before surgery.
Useful Strategies:
• Develop a facility-wide guidelines, and or/policy to provide
routine prophylaxis to all “at risk” surgical patient groups.
• Develop and routinely use pre-printed orders and/or
postoperative order sets that embed evidence-based, best
practices of surgical patient care.
*See appendix 2 - A15, 3, 4, and 7 - A32 for resources to help you update your hospital’s VTE
approach, including examples of VTE Guidelines, order sets, and reference lists.
42
Compliance with the site marking step of the Safe Surgery
Checklist involves the following principles:
Site Marking to Avoid Wrong Site Surgery*
In any invasive procedure, using multiple steps to verbally confirm
patient identity, consent, procedure, and surgical site are good
measures to prevent wrong site/wrong person surgery (see pages 31
and 32 of the Part A: Primer). Most teams review these items
consistently with patients, however, according to an OHA survey,
the practice of site marking for surgical procedures with bilaterality
varies among hospitals (see appendix 5 - A29).
Preventative Actions
For procedures involving bilaterality:
•
•
•
•
Mark the surgical site in an unambiguous way to clearly identify
the location of the procedure for all team members.
Use a standard format to mark sites, such as the initials of the
surgeon – with or without a line to indicate the proposed incision.
For midline approaches to procedures involving bilateral
organs, indicate the surgical side with the site mark.
Actively include the patient in the site marking process if possible.
Have a defined alternative process for:
•
•
•
•
•
Exploratory and diagnostic procedures.
Mucosal surfaces, the perineum, teeth.
Interventional procedures with no predetermined
insertional site.
Patients who refuse site marking, premature infants.
Procedures involving a midline approach to midline organs
(heart, c-sections) are exempt from site marking.
*See appendix 2 - A13 and 4 for resources to help you update your hospital’s site marking
approach, including an policy example, and a reference list.
43
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Compliance with the medications step of the Safe Surgery
Checklist involves the following principles:
Medication Safety*
The OR is a unique environment where high-alert medications are
frequently used and most procedures take place in a sterile field,
requiring medications to be removed from their original packaging.
According to the Canadian Adverse Events Study**, medication and
fluid-related events are the second leading cause of harm in
hospitalized patients (see pages 32 and 33 of Part A: Primer).
Preventative Actions
To reduce the risk of medication errors:
•
•
•
•
•
•
•
•
•
Conduct an anesthesia safety check.
Confirm patient identity.
Check for allergies.
Administer antibiotics within the specified time frame.
Monitor anticoagulant status and plan to prevent VTE.
Monitor for glycemic control.
Monitor status of beta blocker therapy.
All medications and solutions removed from their original packaging
and placed onto the sterile field must be clearly labelled.
High-alert medications intended for topical application such as
epinephrine 1 mg/mL and those intended for injection by the
surgeon (e.g., topical anesthetic with epinephrine 0.01 mg/ mL used
for infiltration) requires careful review and attention, with specific
mention before certain procedures, such as ear, nose, throat surgeries.
*See appendix 4 and 8 for more information about medications safety and epinephrine, the ISMP
Canada Operating Room Medication Safety Checklist®, and a reference list.
** Baker R, Norton P, Flintoft V et al. The Canadian Adverse Events Study: the incidence
of adverse events among hospital patients in Canada. Canadian Medical Assoc Journal
2004;170(11):1678-86 :http://www.cmaj.ca/cgi/reprint/170/11/1678
44
Compliance with the SSI Prevention for the Safe Surgery
Checklist involves the following principles:
SSI Prevention*
A proactive SSI prevention strategy means using evidence-based
guidelines to assess patients and/or patient groups at risk of SSI and
consistently delivering the appropriate type, dose, mode of delivery, and
timing of antibiotic to achieve optimal antimicrobial prophylaxis (see
pages 33 and 34 of Part A: Primer).
The Surgical Safety Checklist contains many interventions designed
to prevent SSIs:
•
•
•
The Briefing section includes: antibiotic prophylaxis-double dose
as well as monitoring for glycemic control and normothermia and
warming device prompts.
The Time Out section includes “antibiotic prophylaxis: repeat dose”.
Note: Other interventions not included in the checklist, such as
proper hair removal, maintenance of postoperative normothermia,
glucose control for certain patient populations, and discontinuation
of antibiotics 24 hours post operatively, are also extremely
important measures to keep SSI rates as low as possible.
Preventative Actions:
• Screen all surgical patients individually for their risk of
developing an SSI before surgery and risk associated with
the surgery based on their innate risk factors (such as obesity,
concomitant infection, colonization, and smoking) as outlined
in the evidence (Guidelines for Prevention of Surgical Site Infection,
Mungram, 1999) as well as against the level of SSI risk that is
associated with the type of surgery planned (prosthetic
implants, colorectal surgery, etc.) (The Medical Letter, 2004).
• Choose specific treatments to reduce risk (e.g., double dosing,
normothermia) based on evidence-based guidelines.
• Ensure type, dosing and mode of delivery of antimicrobial
prophylaxis is appropriate for patient and operative risk factors
(type and length of surgery).
45
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Continued...
Timing of the antibiotic is essential:
• The overall goal should be to maintain adequate serum and tissue levels of the antibiotic throughout surgery which implies re-dosing certain antibiotics if the surgery exceeds three hours or if the blood loss exceeds 1500 cc.
• Encourage pharmacy, anesthesiology, nursing, and surgeons
to work together to ensure delivery of medication within
recommended time frames of 60 minutes prior to surgery for
regular antibiotics (or 120 minutes for vancomycin).
Useful Strategies:
• Develop facility-wide guidelines and/or policies to provide
routine prophylaxis to all “at risk” surgical patient groups.
• Develop and routinely use pre-printed orders and/or
postoperative order sets that embed evidence-based, best
practices of surgical patient care.
*See appendix 2 - A14, 3, 4, 7 - A33 for resources to help hospitals update their SSI approach,
including examples of policies, order sets, and process ideas from hospitals that have made
significant progress in minimizing SSIs in surgical patients, and a reference list.
46
12.Identify Additional Opportunities for Quality Improvement
Completing a hospital self-assessment and/or spreading the use of the
Surgical Safety Checklist throughout a hospital, may uncover some gaps
or inconsistencies in practices or processes that could be flagged for
concurrent or future quality improvement projects as part of the checklist
program. For example, site verification procedures may vary between
different services. A standardized site marking protocol may help prevent
wrong site anesthesia block or wrong site surgery. Or, perhaps “on time”
antibiotic administration has been identified as a challenge. It is important
to remember that quality improvement is a constant work in progress.
See appendix 10 - A39 for a more detailed explanation of the quality
improvement process.
47
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Endnotes
48
1
White S., Lingard L, Espin S., Baker R. et al. Paradoxical effects of
interprofessional briefings on OR team performance. Cogn Tech Work
(2008) 10:287-294
2
Lingard L., Whyte S.,Espin S.,Baker R., Orser B., Doran D., Towards
safer interprofessional communication: Constructing a model of
“utility” from preoperative team briefings. Journal of Interprofessional
Care (2006) 20(5):471-483.
3
Lingard L, Regehr G., Orser B. et al. Evaluation of a Preoperative
Checklist and Team Briefing Among Surgeons, Nurses, and
Anesthesiologists to Reduce Failures in Communication. Arch. Surg.
2008;143(1):12-17
4
Lingard L., Whyte S.,Espin S.,Baker R., Orser B., Doran D., Towards
safer interprofessional communication: Constructing a model of
“utility” from preoperative team briefings. Journal of Interprofessional
Care (2006) 20(5):471-483.
5
White S., Lingard L, Espin S., Baker R. et al. Paradoxical effects of
interprofessional briefings on OR team performance. Cogn Tech Work
(2008) 10:287-294
6
Lingard L,, Espin S., Rubin B. et al. Getting teams to talk: development
and pilot implementation of a checklist to promote interprofessional
communication in the OR. Qual Saf Health Care.2005;14:340-346
7
Espin S., Lingard L., Baker R.,Regehr G.,Persistence of unsafe practice
in everyday work: an exploration of organizational and psychological
factors constraining safety in the operating room. Qual Saf Health Care
2006;15:165-170
8
Reinertsen JL, Gosfield AG, Rupp W, Whittington JW. Engaging
Physicians in a Shared Quality Agenda. IHI Innovation Series white
paper. Cambridge, Massachusetts: Institutive for Healthcare
Improvement; 2007. (Available at www.IHI.org)
9
Canadian Patient Safety Institute, Surgical Safety Checklist How to
Guide. Retrieved from www.safesurgerysaveslives.ca
10 WHO Guidelines for Safe Surgery 2009, World Alliance for Patient
Safety, World Health Organization, Retrieved from
http://www.who.int/patientsafety/safesurgery
11 Mazzoco K., Pettiti DB., et al.: Surgical team behaviours and patient
outcomes; Am J Surg.2009:197: 678-685
12
Sexton J, Helmrieich R, Neilands T.et al. The Safety Attitudes
Questionnaire: psychometric properties, benchmarking data, and
emerging research. BMC Health Services Research 2006, 6:44.
Retrieved from http://www.biomedcentral.com/content/pdf/14726963-6-44.pdf)
13 IHI Surgical Trigger Tool. Available at http://www.ihi.org/IHI/Topics/
PatientSafety/SafetyGeneral/Tools/SurgicalTriggerTool.htm
14 WHO Guidelines for Safe Surgery 2009, World Alliance for Patient
Safety, World Health Organization, Retrieved from
http://www.who.int/patientsafety/safesurgery
15 The Improvement Guide: A Practical Approach to Enhancing
Organizational Performance. Gerald Langley, Kevin Nolan, Thomas Nolan,
Clifford Norman, Llyod Provost. Jossey-Bass Pub., San Francisco, 1996.
49
Part B: Surgical Safety Checklist “How-To” Implementation Guide
Surgical Safety Checklist
Implementation Guide
Disclaimer
This toolkit has been prepared by the Ontario Hospital Association (OHA)
and the Government of Ontario to help hospitals implement the Surgical
Safety Checklist and improve patient safety.
The materials in this toolkit are for general information purposes only and
should be adapted to the circumstances of each hospital that uses them. The
toolkit reflects the interpretations and recommendations regarded as valid when
it was published. This toolkit is not intended as professional advice or opinion
and users are encouraged to seek their own professional advice and opinion
in the development of their institution’s program and specific plans. The
toolkit is intended to serve as a planning guide to assist hospitals in developing
and updating a Surgical Safety Checklist program. The OHA will not be held
responsible or liable for any harm, damage or other losses resulting from
reliance of the use or misuse of the general information contained in this toolkit.
Copyright © 2010 by Ontario Hospital Association and Government of Ontario, all rights reserved.
This toolkit is published for OHA members. All rights reserved. No part of this publication may
be reproduced stored in a retrieval system, or transmitted in any form by any means, electronic
mechanical, photocopying, recording, or otherwise, except for the personal use of OHA members,
without prior written permission of the Ontario Hospital Association.
For more information about the Surgical Safety
Checklist Implementation Guide, please contact
Dominique Taylor,
Consultant, Patient Safety and
Clinical Best Practice, at
dtaylor@oha.com or (416) 205-1372
50
200 Front Street West, Ste. 2800
Toronto, ON M5V 3L1
Tel 416 205 1300
Fax 416 205 1301
www.oha.com