Print this article - Dentistry 3000
advertisement

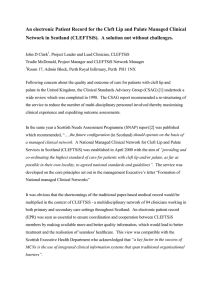
Vol 1, No 1 (2013) ISSN 2167‐8677 (online) DOI 10.5195/d3000.2013.11 Non‐syndromic oral clefts and risk of cancer: a systematic review Daniela Araújo Veloso Popoff1, Mateus Prates Coelho2, Daniella Reis Barbosa Martelli1, Rajiv Saini3, Ricardo Della Cole a4, Hercílio Martelli‐ Júnior1 1 Department of Den stry, State University of Montes Claros, Montes Claros, Minas Gerais, Brazil. Department of Medicine, State University of Montes Claros, Montes Claros, Minas Gerais, Brazil. 3 Department of Periodontology and Oral Implantology, Rural Dental College, Ahmednagar, Maharashtra, India. 4 Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas, Piracicaba, São Paulo, Brazil. 2 Abstract Objec ve: To discuss the risk of cancer among rela ves of individuals with cle lip and pal‐ ate (CL/P), as well as the risk of CL/P among rela ves of individuals with cancer, since stud‐ ies currently published have suggested an increased risk of cancer among rela ves of indi‐ viduals with cle s. Methods: A systema c literature review was carried out in accordance with the Cochrane Collabora on Group protocol, including literature search strategy, selec on of papers through the inclusion and exclusion criteria, data extrac on and quality assessment. Pub‐ Med, Scopus and ISI ‐ Web of Science databases were systema cally searched using the fol‐ lowing search strings: “cle lip and palate” AND “cancer,” “oral cle s” AND “cancer” and “orofacial cle s” AND “cancer.” Results: From 653 studies accessed, eight comprised the final sample: six inves ga ng CL/P index cases and their family history of cancer and two inves ga ng individuals with cancer and their family history for CL/P. The sample sizes were not homogeneous. Oral cle s, the type of cancer and the degree of kinship family were not categorized in all studies. Leuke‐ mia, breast cancer and colon cancer were the most cited types, even as first‐ and second‐ degree rela ves. Conclusion: An increased risk of cancer among rela ves of individuals with cle s could not be en rely confirmed. However, studies with this specific purpose suggest that first‐ and second‐degrees rela ves of individuals with cle have some types of cancer more o en than unexposed families, highligh ng that future studies should expand their samples to in‐ ves gate possible common molecular mechanisms that allow rela ng oral cle s and can‐ cer. Cita on: Popoff DAV, Coelho MP, Martelli DRB, Saini R, Cole a RD, and Martelli‐Junior H. (2013) Non‐ syndromic oral cle s and risk of cancer: a systema c review. Den stry 3000 1:a002 doi: 10.5195/d3000.2013.11 Received: June 24, 2013 Accepted: August 12, 2013 Published: August 23, 2013 Copyright: ©2013 Popoff et al. This is an open‐access ar cle licensed under a Crea ve Commons A ribu on 3.0 United States License. Email: danielavelloso@yahoo.com.br Introduc on Orofacial malformations are the most common form of congenital anomalies in the world [1]. Among the orofacial alterations, the most prevalent is the cleft lip with or withoutcleftpalate(CL/P)[2-5],whichmay occur more commonly in an isolated and non-syndromicformasaspeci icphenotype or, more rarely, composing several associations or syndromes [6,7]. Embryologically, clefts result from primary fusion defects of the craniofacial processes that form the primary and secondary palate in the irst intrauterinetrimester[8]. The incidence of CL/P varies according to geographical location, racial and ethnic http://dentistry3000.pitt.edu groups,environmentalexposures,andsocioeconomic status, affecting approximately 1/700 live births with wide variability across geographic origin. Generally, Asian andAmerindianpopulationshavethehighestreportedbirthprevalencerates,oftenas high as 1/500, European-derived populationshaveintermediateprevalenceratesat about 1/1000, and African-derived populations have the lowest prevalence rates at about1/2500[5,9,10]. AccordingtoVieira(2008)[7],thelastdecadewascrucialtoelucidateissuesconcerning the etiology of CL/P when compared to other defects observed at birth. As this is a multifactorial trait, environmental risk factors such as smoking, alcohol,parental age, medications, birth order, interpregnancy interval, and folic acid de iciency are listed asmodi iers,andriskfactoridenti icationis the irststeptobetterunderstandingandto preventsuchcraniofacialchanges[7,11,12]. However, current knowledge about the causes of CL/P points particularly towards genetic risk factors, and the study of the pathogenesis of CL/P has provided ample opportunities to identify candidate genes for this disorder and even link them to the occurrenceofcancerinrelativesofindividuals born with CL/P, or even in these individuals themselves when at an adult age, supporting the hypothesis that common geneticfactorsmaybepresentinbothconditions[13].Althoughothergenesthathave This work is licensed under a Creative Commons Attribution 3.0 United States License. This site is published by the University Library System, University of Pittsburgh as part of its D‐Scribe Digital Publishing Program and is cosponsored by the University of Pittsburgh Press. Non‐syndromic oral cle s and risk of cancer: a systema c review Vol 1, No 1 (2013) DOI 10.5195/d3000.2013.11 notbeenexploredyetcanbeinvolvedinthe both conditions, three genes are suspected to underlie such associations: FGF - ibroblast signaling pathway, CDH1 - epithelial cadherin and AXIN2 - AXIS inhibition protein2[14].Colorectalandbreastcancerare themostassociatedwithmutationsofthese genes [2].Thus, given the growing number of studies published currently suggesting a common etiology for CL/P and cancer and increased risk of cancer among relatives of cleft individuals [2,5,13-18], the current study aimed to discuss the issue through a systematic literature review in order to provideadditionalevidenceofthesegenetic risks, which will aid in the development of strategies that target more aggressive screening programs and preventive chemicaltreatments. Methods The present review was carried out in accordance with the Cochrane Collaboration Groupprotocolforsystematicreviews[19], includingaliteraturesearchstrategy,selection of papers through the inclusion and exclusioncriteria,dataextraction,andquality assessment. Meta-analysis was not possiblesince selectedstudiesdidnotobserve the same variables, methods, participants, and outcomes, which prevented comparisons. Literaturesearchstrategy Our review was performed in February 2013inordertoobtainliteratureregarding cleftlipand/orpalateandfamilyhistoryof cancer. PubMed, Scopus, and ISI - Web of Science databases were systematically searched using two basic approaches: the search strings “cleft lip and palate” AND “cancer,” “oral clefts” AND “cancer,” and “orofacial clefts” AND “cancer” for studies publisheduptothattime. Selectionofpapersthroughtheinclusionand exclusioncriteria Theselectionofpapersisdiagrammatically explained in Figure 1. Of the 653 studies originally found through the literature search strategy, 235 studies were excluded (in non-English language, with no full text available, and non-cross-sectional, prevalence, cohort, or case-control design), remainingwith418papers.Additionalstudies were found through the references of the potentialstudiesretrieved.Then,allstudies involvingoralclefts(associatedornotwith craniofacial syndromes or any anomalies) and cancer were selected. Afterwards, only studies presenting information regarding http://dentistry3000.pitt.edu Figure 1: Flowchart of the studies included and excluded risk of cancer in relatives of individuals born with non-syndromic oral clefts were included in the present study, as well as articles regarding the frequency of nonsyndromic oral clefts among relatives of individualsdiagnosedwithcancer. The following speci ic inclusion criteria were used to identify relevant articles: (1) Index cases with non-syndromic cleft lip and/or palate, whose relatives were investigated for any type of cancer; (2) Index cases with any type of cancer, whose relatives were investigated for non-syndromic cleftlipand/orpalate;(3)Indexcasescompared to healthy controls for risk assessment; (4) The degree of relationship between index cases and investigated family members is investigated in the study. All studies that included individuals with cleft lip and/or palate associated with other abnormalities, having syndromic causes or regarding Mendelian traits were excluded. Thus,eightstudieswereselected.(Figure1) Dataextraction Titleandabstractscreeningwasperformed by two reviewers (DAVP and HMJ) who workedindependentlytoidentifypotentiallyrelevantpapersforwhichfulltextpublications were retrieved. If, however, there wasanydiscrepancyofopinion,thereviewers reexamined the paper together and arrived at a joint inal decision. A standardized form was used to extract information, suchasauthorandyearofpublicationofthe paper, origin of participants, study design, sample size,typeoforalclefts,typeofcancer, degree of kinship of family members andtheassociationbetweennon-syndromic oralcleftsandcancer. Qualityassessment STROBE methodology (Strengthening the Reporting of Observational Studies in Epidemiology) [20], considered the guideline for an appropriate assessment of observational studies, was used to perform the quality assessment of the studies selected. Thespeci icSTROBEitemsconsideredwere inclusionandexclusioncriteria,assessment of exposure and outcome, statistical methods, confounders, bias, and report limitation. Results The initial database search identified 653 citationspublishedbetween1980and2013. After screening, 235 studies were excluded (72innon-Englishlanguage,93withnofull text available, and 70 which type of study was other than those listed in the methodology),remainingwith418papers. A second screening was performed on the remaining papers and other studies were excluded, this time for the following reasons:51articlesinduplicity(foundinmore thanoneofthedatabases)and351articles that did not report non-syndromic cleft lip and/or palate and risk of cancer. In addition, ive papers listed in the references of theselectedoneswereincluded,resultingin 21papersforthe inalscreening. 2 Non‐syndromic oral cle s and risk of cancer: a systema c review Vol 1, No 1 (2013) DOI 10.5195/d3000.2013.11 Table 1: Main characteris cs of the eight selected papers. First author, year [reference] Country of study Study design Jindal, 2012 India Case‐control Taioli, 2010 United States Case‐control Turkey Case‐control United States Case‐control Denmark Case‐control Latvia Cross‐ sectional Yildirim, 2012 Menezes , 2009 Zhu, 2002 Vieira, 2012 Exposure Individuals diagnosed with cancer Cancer survivors Cleft individuals Cleft individuals Cleft individuals Cleft individuals Sample size (case/population) Cleft Classification Type of cancer Statistical test Kinship with index cases Outcome 142 (85/57) CL/P Leukemia X2 and Fischer exact First‐degree Increased risk 338 (168/170) All Unspecified First/second‐ degree Increased risk 319 (158/161) All Unspecified First‐degree Increased risk 168 (75/93) Unspecified Unspecified Not reported Increased risk 41206 (45/41161) Unspecified Unspecified Odds Ratio First Degree Increased risk 89 Unspecified Unspecified Risk Ratio First/second/ third‐degree Logistic regression Logistic regression X2 and Fischer exact Dietz, 2012 Denmark Retrospec‐ tive cohort Cleft individuals 1809 All Breast Cancer Cox regression First‐degree Steinwachs, 2000 United States Cross‐ sectional Cleft individuals 196 CL/P and CL Unspecified Odds Ratio First/second‐ degree The full text of these papers was read and 13werethereafterexcludedfornotreportingriskofcancerinrelativesofindividuals with non-syndromic cleft lip and/or palate, aswellasfornotreportingthefrequencyof non-syndromic cleft lip and/or palate in relativesofindividualsdiagnosedwithcancer.Thus,eightpaperswereselectedforthe systematicreview. The characteristics of the eight selected papersarepresentedinTable1.Threeused a case-control design, two used a crosssectional/prevalence design and one was a retrospectivecohortstudy.Thosereporting frequencyofnon-syndromiccleftlipand/or palate in relatives of individuals diagnosed withcanceralsousedacase-controldesign. Table 2: Most cited types of cancer among rela ves of cle individuals and cancer index cases. First author, year [reference] Most commonly found types of cancer Leukemia* Jindal, 2012 Taioli, 2010 Breast, colon‐rectal, melanoma, tes cular Unspecified Yildirim, 2012 Menezes, 2009 Zhu, 2002 Types of cancer with increased risk at index cases rela ves Leukemia Tes cular, melanoma, colon‐ rectal Unspecified Unspecified Unspecified Breast, melanoma of skin, tes s, cervix uteri, brain and nervous system Lymphoma, Leukemia Unspecified Vieira, 2012 Breast* Dietz, 2012 Steinwachs, 2000 Breast, lung, leukemia, colon, uterine. *The study specifically searched for this type of cancer only. http://dentistry3000.pitt.edu Unspecified Breast None found Increased risk No association when all non‐ syndromic CL/P were analyzed together No increased risk Thesamplesizesandthepopulationinvestigated varied considerably amongst the studies, not being homogeneous. From those investigating risk of cancer in relatives of individuals with non-syndromic cleftlipand/orpalate,twowereconducted intheUnitedStates,twoinDenmark,onein Turkey, and one in Latvia. Regarding those reporting frequency of non-syndromic cleft lip and/or palate in relatives of individuals diagnosed with cancer, one was conducted intheUnitedStatesandoneinIndia(Table 1). Mostofstudiesinvestigatedalltypesoforal clefts. Type of cancer and the degree were not categorized in all studies of kinship in thefamily.Despitethis,leukemia,testicular cancer,melanoma,colon-rectalcancer,lymphoma, and breast cancer were the most citedtypesofcancer(Table2)inboth irst- andsecond-degreerelatives(Table1). The relationship between oral clefts and cancer within the studies was tested using chi-squareandFisher’sExacttests[14,18], Logistic regression [2, 17], Odds ratio [15, 21], Risk ratio [13], and Cox regression [5] (Table1). Alleightstudiesweresubmittedto quality assessment using STROBE guidelines. Inclusion and exclusion criteria were describedinallofthem(Table3).Theoutcomes of two studies provide suggestive evidence that families with individuals diagnosed with some types of cancer report familyhistoryofcleftlipand/orpalate more frequently than families without cases 3 Non‐syndromic oral cle s and risk of cancer: a systema c review Vol 1, No 1 (2013) DOI 10.5195/d3000.2013.11 Table 3: Inclusion and exclusion criteria among the eight selected papers. First year author, Inclusion Criteria Exclusion Criteria All subjects were children being cared for at the General Hospital of Chandigarh, India. Cases were identified from the Pediatric Leukemia Clinic and controls were identified randomly from the Allergy/Immunology clinic. Children with lymphoma were excluded from the case group and the ones with positive history for cancer, from the control group. [reference] Jindal, 2012 Taioli, 2010 Case group was composed of patients who were treated for cancer in the past, who were considered in remission for at least six months, and who were scheduled for an appointment for a routine checkup. Control group was composed by healthy people from the general population who were 18 years of age or older. Not reported. Yildirim, 2012 All subjects were patients at the Department of Pedodontics clinic, Istanbul University, Tur‐ key. Case group was composed of individuals born with any type of CL/P and controls were individuals unrelated to them. Case group members’ first‐degree relatives were evaluated, also. Case and control siblings were excluded. Menezes, 2009 All subjects were from white ancestry families from Pittsburgh. Cases were recruited from a registry maintained by the Cleft‐Craniofacial Center, Children’s Hospital of Pittsburgh of UPMC. Not reported. Zhu, 2002 Subjects were identified from the Denmark’s Central Population Registry by their kinship with patients diagnosed with cancer and registered at the Cancer Registry. They also ought to have been born between 1977 and 1995 in Denmark to mothers with a Danish citizenship. Patients whose parents had other children be‐ fore 1977, who were diagnosed with patent ductus arteriosus, undescended testis and hip dislocation. Vieira, 2012 Subjects were picked from the Riga Cleft Lip and Palate Centre Registry from the time period of 1980‐2009. Not reported. Dietz, 2012 Subjects were individuals with non‐syndromic CL/P registered at the Danish Facial Cleft Regis‐ ter. Individuals born after 1975 were excluded. Steinwachs, 2000 Subjects ought to have been diagnosed with cleft lip with or without cleft palate and have no known syndromal cause for the cleft. Not reported. ofcancer[2,18].Fromstudiesinvestigating cancer in relatives of individuals with oral clefts, only two suggest that the irst- and second-degree relatives of the individuals with clefts are not at an increased risk for cancer[5,21].Allstudiesde inedtheexposure variables (Table 1). Although all studieshaddescribedpotentialbias/limitations, only three properly reported identi ication of bias/limitations (Table 1). Although all studies had described potential bias/limitations,onlythreeproperlyreported identi icationofbias/limitations(Table4). DISCUSSION This systematic review assessed available studies suggesting a common etiology for non-syndromic oral clefts and cancer and increased risk of cancer among relatives of cleftindividuals,aswellasincreasedriskof non-syndromic oral clefts among relatives ofindividualsdiagnosedwithcancer,thereby providing additional evidence of these genetic risks, which could aid in the development of strategies that target more ag- http://dentistry3000.pitt.edu gressivescreeningprogramsandpreventive chemicaltreatments. Our original intention was to integrate the results of included studies through a metaanalysis, however, given the differences in variables, methods, participants and outcomesamongthestudies,themostsuitable and responsible was to address the issue throughasystematicreview. We demonstrated that there is a large amount of literature distinguishing nonsyndromic cleft lip and palate from those cases of clefts associated with other abnormalities, syndromes, or Mendelian traits. Our indings also demonstrated that the studiespublishedagreethatnon-syndromic oralcleftsareoneofthemostcommonhumanmalformations,withanaverageprevalence of 1 per 700 or 1,000 live births [ 2,4,5,7,16,17,21-26],aswellasthatitsincidencevariesaccordingtogender:2:1being theratioofmalestofemalesforcleftlipand palate and 1:2 the approximate ratio of male to female for isolated cleft palate [1,10,16,26,27]. Other common information between the studies is the fact that unilateral clefts are more common than bilateral clefts, and of the unilateral cases of non-syndromic cleft lip and palate, left-sided cleft lips occur morefrequentlythanright-sidedcleftlips[ 4,5,,21,23,28,29]. Many studies have also demonstratedthatgeneticfactorsmayplay a role in the cause of non-syndromic oral clefts in addition to certain environmental and/orstochasticfactors,meaningthatthis malformation is a multifactorial trait [2,21,22,26,30,31]. Similarly, studies have shown that cleft lip, with or without cleft palate, is entirely different from isolated cleftpalateinbothembryologicalandpathogeneticstandpoints[32,33]. Likewise, many of the studies report relationships between non-syndromic oral clefts and cancer or childhood cancer [14,18,25,34-41]. Nonetheless, the studies thatpresentedinformationregardingriskof cancer in relatives of individuals born with non-syndromic oral clefts or regarding the frequency of non-syndromic oral clefts 4 Non‐syndromic oral cle s and risk of cancer: a systema c review Vol 1, No 1 (2013) DOI 10.5195/d3000.2013.11 among relatives of individuals diagnosed with cancer, besides being scarce, vary greatly in their characteristics and designs, precluding a meta-analysis of the results found. Inthecurrentsystematicreview,bothstudiesassessingtheprevalenceofCL/Pinfamily members of cancer patients had a casecontrol design and suggest that this malformation is more frequent in families of cancer survivors in comparison with families of a population-based sample of controls.InthestudyofTaiolietal.(2010)[2], the results were not statistically signi icant andtheauthorsrelateittothesamplesize ofthestudyandtotherarityofCL/Poccurrence. In the second study, relating CL/P and childhood cancer, none of the children from the unaffected group had a positive family history of cleft lip and palate, while ive children with leukemia had a positive historyoforalclefts[18]. In these studies, the population investigated,ortheirparentsorguardians,answered standardized questionnaires with demographic information about the respondents and their family history of CL/P. It was a consensus between the authors that information on number of second-degree relativesislackingforboth,whichcouldexplain their indings for the irst-degree relatives, since the more distant the relative is, less informationisknownabouthim. In the study investigating adult individuals who survived cancer, the most frequent types of cancer were melanoma, testicular, breast, colon-rectal, and lymphoma. The authors state, however, that one limitation ofthestudywastoincludecancersurvivors insteadofnewlydiagnosedcancerpatients, whichcouldexcludehighlyfatalcancers[2]. Despite the different characteristics of the populations investigated in the studies of Taioli et al. (2010) and Jindal and Vieira (2012) [2,18], both suggest that shared genetic factors may explain an association betweenoralcleftsandcancer.Thus,investigating the relationship between malformations and malignancies becomes important as it is speculated that they might havecommoncauses.Endorsingthatpossibility, Chalothorn et al. (2008) and Kü chler et al. (2013) [42,43] have previously proposed an association between tooth agenesisandcancer.Insomecases,toothagenesis and oral cleft may share the same genetic background. This review also accessed studies [5,1315,17,21] regarding risk of cancer in relatives of individuals born with non- syndromic oral clefts. From the six studies found, three also had a case-control design and more cancer cases were reported amongrelativesofcleftindividualsthanby controls [14,15,17]. The most prevalent typesofcancerhavenotbeenplainlyidentiiedinallstudies,whichwasalimitationof thestudiesdeclaredbytheauthors.However, in those which it was possible, a clear predominanceofcoloncancerandleukemia cases was noticed, as well as some reports of breast cancer, lymphoma and brain cancer [14,15]. The most affected relatives werespeci iedonlyinthestudyofZhuetal., (2002) [15], which exclusively investigated parents.Afurtherlimitationthatwasfound is the fact that the speci ic data regarding theageofonsetofcancerwasnotaccessed, which makes it impossible to determine if family members of individuals with cleft developed cancer at earlier ages than the generalpopulation. A higher prevalence of cancer in family membersofindividualsbornwithCL/Pwas presented in a cross-sectional study with a Latvian population, too [13]. The risk was calculated by dividing the prevalence of cancerinthetargetgroupbytheprevalence ofcancerinthatpopulation.Itwasdemonstratedthatthisriskisthreetimeshigherin Table 4: Poten al bias/limita ons and the author’s efforts to iden fy them among the eight selected papers. First author, year [reference] Jindal, 2012 Taioli, 2010 Yildirim, 2012 Menezes, 2009 Zhu, 2002 Vieira, 2012 Dietz, 2012 Steinwachs, 2000 Bias/limitations Information concerning illnesses on relatives more distant than the first‐degree may not be so reliable. Since it researched cancer survivors and not patients diagnosed with cancer per se, the most fatal forms of cancer tend to have their association with CL/P not reported accurately. Also, an association between the type of cancer and CL/P becomes impossible to be made in this case because of characteristic survivor‐ ships in each type. As information regarding specific types of cancers was not available for all indi‐ viduals, an analysis by cancer types could not be done. Also, the specific data regarding the age of onset of cancer was not accessed, which made it impossible to determine if family members of cleft individuals developed cancer at earlier ages than the general population. The cancer types reported may not all have been related to the same causes. Also, as there was no access to data that specified the age of cancer develop‐ ment in those individuals’ family members, it was no possible to determine if family members of cleft individuals developed cancer at earlier ages than the general population. There may have been some confusion from the teratogenic effects of cancer treatment in parents who had cancer previous to the child’s birth. The outcome of previous births also could induce some bias as well as maternal age at birth and sex of the child. Lastly, the lack of data on stillbirths may have biased results if fetal mortality differs between parents who will develop cancer and parents who won’t. The population studied was composed mostly by individuals in their first years of life, and because of that, the prevalence of pediatric or earlier onset types of cancer was relatively increased when compared with the other types. The same is true for their relatives, as they are most likely also relatively young. A left and right truncation in this study was observed, as no information can be gotten neither previous nor post the period studied. There is known lack of accuracy in information provided by patient reports about their family members. http://dentistry3000.pitt.edu Identification of bias/limitations Not reported. Not reported. Not reported. Proposes new research with increased sample size to replicate findings and test the association between genetic variants and specific types of cancer. It only used parents whose cancer diagnostic came up after the birth of their indexed children. Also, the children analyzed were only firstborns and the age of the mother at birth and the child’s sex were reported. Not reported. Not reported. Proposes new and larger studies with sufficient power to study only first‐degree relatives. 5 Non‐syndromic oral cle s and risk of cancer: a systema c review Vol 1, No 1 (2013) DOI 10.5195/d3000.2013.11 irst- and second-degree relatives and decreases to 1.5 times in third-degree relatives.Similartomostavailablestudieswith thesameproposal,thetypesofcancerwere not consistently reported and, because of that,thisstudydidnotdiscriminatebycancertypes. As well as in the studies addressing prevalence of CL/P in family members of cancer patients, indingsfromfour[13-15,17]ofsix studiesregardingriskofcancerinrelatives ofindividualsbornwithnon-syndromicoral clefts provide additional support for a commonetiologybetweenCL/Pandcancer, suggestingthatthesefamilieshaveahigher genetic load for CL/P, which also impacts theircancerrisk. On the other hand, two other studies regarding risk of cancer in relatives of individuals with clefts could not conclude the same [5,21]. The irst one, performed by Steinwachsetal.,(2000)[21]wasemphatic in denying an increased risk for cancer in the irst- and second-degree relatives of individual affected with non-syndromic CL/P. The population investigated was composed of Caucasians, Hispanics, African Americans, and Asian individuals. The cancerdatawereanalyzedinaggregatebytype ofcancer,bydegreeofrelationtotheindex case, and by ethnicity. As a result, neither irst-degree relatives nor second-degree relatives of the index cases had a signi icantlyincreasedriskforcancer.Noparticularethnicgroupdemonstratedanexcessively increased risk for cancer. Not even the most commonly reported cancers (lymphoproliferative cancers, female cancers, andlungcancer)wereincreasedasawhole orin irst-degreerelativesonly. In the same way, in a recent retrospective cohort study [5] testing whether mothers and sisters of individuals born with CL/P haveanincreasedriskforbreastcancer,the authors were not able to con irm a general increaseinthisriskforbreastcanceramong the study population. However, some associations were revealed when cleft subtype was analyzed, and having a child with isolated cleft palate was associated with an increased risk of breast cancer for the mother,whichmaybebiologicallyplausible due to the evidence that the different cleft typeshavedifferentgeneticorigins[44,45]. Thus, the hypothesis that parental cancer and congenital malformations in offspring may be correlated could not be entirely con irmedbythepresentsystematicreview. Despiteitbeingknownthatpossiblemechanisms at the basis of an association between CL/P and cancer are shared genetic factors, once polymorphisms in genes involvedincell–celladhesionandcellmotility http://dentistry3000.pitt.edu are associated with both cancer and CL/P [16,18], studies in this direction are very scarceandofthoseexistingandmostinvestigatedallsubtypesoforalclefts,whichsets alimitationto indoutsuchcorrelation. There is agreement among almost every reviewed author [2, 14,17,18] that the investigatedpopulationsintheirstudiesneed to be expanded in order to avoid any random indings in multiple testing or the potential impact of Type I error. It is also in agreement that future studies should explorethepossibilitythatthereisapreferentialoccurrenceofspeci ictypesofcancerin families with individuals born with CL/P andtestthehypothesisthatcommongeneticandepigeneticmechanismsareplayinga role in both conditions [14,17]. Through thisinformation,futurestudiesmaybebetter able to identify the causes of nonsyndromicorofacialcleftsandultimatelyto predict its occurrence and to facilitate genetic counseling of affected families [21]. AnotherissueraisedbyDietzetal.(2012)is the fact that having a cleft leads to social marginalization and changes in lifestyle could predispose not only the individual, but also their family for cancer, which seems plausible from a standpoint of relationship between stress and cancer, as discussedintheliterature. Conflict of interest: There are no conflicts ofinteresttoreport. References 1. The evolu on of human gene c studies of cle lip and cle palate. Marazita L M. Annu Rev Genomics Hum Genet. 2012;13:263‐83. Epub 2012 Jun 6. PMID:22703175 [PubMed ‐ indexed for MEDLINE] 28. PMID: 22037380 [PubMed ‐ indexed for MEDLINE] . 6. Prevalence of nonsyndromic oral cle s in a reference hospital in the state of Minas Gerais, Brazil, between 2000‐2005. Martelli‐Junior H, Porto LCVP, Barbosa DR, Bonan PRF, Freitas AB, Cole a RD. Braz Oral Res. 2007 Oct‐ Dec;21(4):314‐7. PMID:18060257 [PubMed ‐ indexed for MEDLINE] 7. Unraveling human cle lip and palate research. Vieira AR. J Dent Res. 2008 Feb;87(2):119‐25. PMID:18218836 [PubMed ‐ indexed for MED‐ LINE] 8. The current understanding of cle lip malfor‐ ma ons. Wan a N, Re nger G. Facial Plast Surg. 2002 Aug;18(3):147‐53. PMID:12152133 [PubMed ‐ indexed for MEDLINE] 9. The complex gene cs of cle lip and palate. Cobourne MT. Eur J Orthod. 2004 Feb;26(1):7‐ 16. PMID:14994877 [PubMed ‐ indexed for MEDLINE] 10. Cle lip and palate: synthesizing gene c and environmental influences. Dixon M, ML, Beaty TH,Murray JC. Nat Rev Genet. 2011 March; 12(3): 167–178. PMID:21331089 [PubMed ‐ indexed for MEDLINE] 11. Zeiger JS, Beaty TH (2002) Gene–environment interac on and risk to oral cle s. In: Wyszynski DF editors. Cle lip and palate: from origin to treatment. New York: Oxford University Press; pp. 283–289. 12. Frequency of congenital craniofacial malfor‐ ma ons in a Brazilian Reference Center. Para‐ naiba LMR, Miranda RT, Ribeiro LA, Barros LM, Martelli‐Júnior H. Rev Bras Epidemi‐ ol. 2011;14:151‐160. 13. Risk of cancer in rela ves of children born with isolated cle lip and palate. Vieira AR, Khaliq S, Lace B. Am J Med Genet A. 2012 Jun;158A(6):1503‐4. Epub 2012 May 14. PMID:22585460 [PubMed ‐ indexed for MED‐ LINE] 14. AXIS inhibi on protein 2, orofacial cle s and a family history of cancer. Menezes R, Marazita ML, Goldstein McHenry T, Cooper ME, Bardi K, Brandon C, Letra A, Mar n RA, Vieira AR. J Am Dent Assoc. 2009 Jan;140(1):80‐4. PMID:19119171 [PubMed ‐ indexed for MED‐ LINE] 2. Cle Lip and Palate in Family Members of Can‐ cer Survivors. Taioli E, Ragin C, Robertson L, Linkov F, Thuman LE, Vieira AR. Cancer In‐ vest. 2010 Nov;28(9):958‐62. PMID:20569073 [PubMed ‐ indexed for MEDLINE] 3. Iden fying determinants of quality of life of children with cancer and childhood cancer sur‐ vivors: a systema c review. Klassen AF, Antho‐ ny SJ, Khan A, Sung L, Klaassen R. Support Care Cancer. 2011 Sep;19(9):1275‐87. Epub 2011 May 25. PMID:21611865 [PubMed ‐ indexed for MEDLINE] 15. Do parents of children with congenital malfor‐ 4. Parental age as a risk for non‐syndromic oral cle s: a meta‐analysis. Herkrath APCQ, Her‐ krath FJ, Rebelo MAB, Ve ore MV. J Dent. 2012 Jan;40(1):3‐14.Epub 2011 Oct 13. PMID:22019990 [PubMed ‐ indexed for MED‐ LINE] 5. Risk of breast cancer in females with cle lip and palate. Dietz A, Pedersen DA, Jacobsen R, Wehby GL, Murray JC, Christensen K. Ann Epi‐ demiol. 2012 Jan;22(1):37‐42. Epub 2011 Oct in families with hereditary diffuse gastric can‐ cer. Frebourg T, Oliveira C, Hochain P, Karam R, Manouvrier S, Graziadio C, Vekemans M, Hartmann A, Baert‐Desurmont S, Alexandre C, Lejeune Dumoulin S,Marroni C, Mar n C, Castedo S, Love M, Winston J, Machado JC, A é T, Jabs EW, Cai J, Pellerin P, Triboulet JP, Sco e M, Le Pessot F, Hedouin A, Carneiro F, Blayau M, Seruca R. J Med Genet. 2006 Feb;43(2):138‐42. Epub 2005 Apr 14. ma ons have a higher cancer risk? A na on‐ wide study in Denmark. Zhu JL, Basso O, Hasle H, Winther JF, Olsen JH, Olsen J. Br J Can‐ cer. 2002 Aug 27;87(5):524‐8. PMID:12189550 [PubMed ‐ indexed for MEDLINE] 16. Cle lip/palate and CDH1/E‐cadherin muta on 6 Non‐syndromic oral cle s and risk of cancer: a systema c review Vol 1, No 1 (2013) DOI 10.5195/d3000.2013.11 17. Defining predictors of cle lip and palate risk. Yildirim, Seymen F, Deeley K, Cooper ME, Vieira AR. J Dent Res. 2012 Jun;91(6):556‐61. Epub 2012 Apr 10. PMID:22496123 [PubMed ‐ in‐ dexed for MEDLINE] 18. Family history of cle lip and palate in subjects diagnosed with leukemia. Jindal A, Vieira AR. Am J Med Genet A. 2012 Mar;158A(3):678‐ 9.Epub 2012 Feb 2. PMID:22302642 [PubMed ‐ indexed for MEDLINE] 19. Alderson P, Green S, Higgins JPT, editors. Cochrane Reviewers’ Handbook 4.2.2 [updated March 2004]. In: The Cochrane Library, Issue 1, 2004. Chichester, UK: John Wiley & Sons, Ltd. 20. The strengthening the repor ng of observa‐ onal studies in epidemiology (STROBE) state‐ ment: guidelines for repor ng observa onal studies. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzche PC, Vanderbroucke JP. BMJ. 2007 Oct 20;335(7624):806‐8. PMID:17947786 [PubMed ‐ indexed for MEDLINE] 21. Nonsyndromic cle lip and palate is not associ‐ ated with cancer or other birth defects. Stein‐ wachs EF, Amos C, Johnston D, Mulliken J, Stal S, Hecht JT Am J Med Genet. 2000 Jan 3;90(1):17‐24 PMID:10602112 [PubMed ‐ in‐ dexed for MEDLINE] 22. Major hematological diseases associated with cle lip and palate. Lin CH, Lo LJ, Wang ML, Chen YR, Noordhoff MS. Cle Palate Craniofac J. 2000 Sep;37(5):512‐5. PMID:11034036 [PubMed ‐ indexed for MEDLINE] 23. Mossey P, Li le J (2002) Epidemiology of oral cle s: an interna onal perspec ve. In: Wyszyn‐ ski DF, editors. Cle lip and palate: from origin to treatment. New York: Oxford University Press.pp 127‐158. 24. Maternal use of an bio cs and the risk of oro‐ facial cle s: a na onwide cohort study. Møl‐ gaard‐Nielsen, Hviid A. Pharmacoepidemiol Drug Saf. 2012 Mar;21(3):246‐53. Epub 2011 Nov 28. PMID: 22125260 [PubMed ‐ indexed for MEDLINE] 25. Cancer risk in persons with oral cle ‐ a popu‐ PMID:3308178 [PubMed ‐ indexed for MED‐ LINE] 29. The gene cs of isolated orofacial cle s: from genotypes to subphenotypes. Jugessur A, Farlie PG, Kilpatrick N. Oral Dis. 2009 Oct;15(7):437‐ 53. Epub 2009 Jul 2. PMID:19583827 [PubMed ‐ indexed for MEDLINE] 30. Hereditary cle lip/palate and Will Tumor: A rare associa on. Yu CC, Wong FH, Lo LJ, Chen YR. Cle Palate Craniofac J. 2002 May;39(3):376‐9. PMID:12019017 [PubMed ‐ indexed for MEDLINE] 31. Gene/environment causes of cle lip and/or palate. Murray JC. Clin Genet. 2002 Apr;61(4):248‐56. PMID:12030886 [PubMed ‐ indexed for MEDLINE] 32. Cle lip (+/‐ cle palate) in Danish twins, 1970‐ 1990. Christensen K, Fogh‐Andersen P. Am J Med Genet. 1993 Nov 1;47(6):910‐6. PMID:8279491 [PubMed ‐ indexed for MED‐ LINE] 33. Analysis of family incidence of cle lip and/or palate. Kot M, Kruk‐Jeromini J. Med Sci Monit. 2007 May;13 (5):CR231‐4. PMID:17476195 [PubMed ‐ indexed for MED‐ LINE] 34. A popula on‐based study of cancer incidence in twins and in children with congenital malfor‐ ma ons or low birth weight, Norway, 1967‐ 1980. Windham GC, Bjerkedal T, Langmark F. Am J Epidemiol. 1985 Jan;121(1):49‐56. PMID:3155484 [PubMed ‐ indexed for MED‐ LINE] 35. Increased prevalence of minor anomalies in childhood malignancy. Mehes K, Signer E, Pluss HJ, Müller HJ, Stalder G. Eur J Pediatr. 1985 Sep;144(3):243‐54. PMID:4054163 [PubMed ‐ indexed for MEDLINE] 26. Nevoid basal cell carcionoma syndrome with 38. Risk of childhood cancer for infants with birth three year study. Oliver‐Padilla G, Mar nez‐ González V. Cle Palate J. 1986 Jan;23(1):48‐57. PMID:3455903 [PubMed ‐ indexed for MED‐ LINE] 28. Incidence of cle lip, cle palate, and cle lip and palate among races: a review. Vanderas AP. Cle Palate J. 1987 Jul;24(3):216‐25. an cancer: a case‐controlled study. Chalothorn LA, Beeman CS, Ebersole JL, Kluemper GT, Hicks EP, Kryscio RJ, DeSimone CP, Modesi SC. J Am Dent Assoc. 2008 Feb;139(2):163‐9. PMID:18245684 [PubMed ‐ indexed for MED‐ LINE] 43. Tooth agenesis associa on with self‐ reported family history of cancer. Küchler EC, Lips A, Tannure PN, Ho B, Costa MC, Granjeiro JM, Vieira AR. J Dent Res. 2013 Feb;92(2):149‐55. Epub 2012 Nov 20. PMID:23169889 [PubMed ‐ indexed for MED‐ LINE] 44. Disrup on of an AP‐2alpha binding site in an IRF6 enhancer is associated with cle lip. Rahimov F, Marazita M, Visel A, Cooper M, Hitchler M, Rubini M, Domann FE, Govil M, Christensen K, Bille C, Melbye M, Jugessur A, Lie RT, Wilcox AJ,Fitzpatrick DR, Green ED, Mossey PA, Li le J, Steegers‐Theunissen RP, Pennacchio LA, Schu e BC, Murray JC. Nat Genet. 2008 Nov;40(11):1341‐7. Epub 2008 Oct 5. PMID:18836445 [PubMed ‐ indexed for MEDLINE]. 45. A cohort study of recurrence pa erns among more than 54,000 rela ves of oral cle cases in Denmark: Support for the mul factorial threshold model of inheritance. Grosen D, Chevrier C, Sky he A, Bille C, Mølsted K, Sivertsen A, Murray JC, Christensen K. J Med Genet. 2010 Mar;47(3):162‐8.Epub 2009 Sep 14. PMID:19752161 [PubMed ‐ indexed for MEDLINE] childhood lymphoblas c leukemia. Mehes K, Kajtar P, Sandor G, Scheel‐Walter M, Niethammer D. Am J Med Genet. 1998 Jan 6;75(1):22‐7. PMID:9450852 [PubMed ‐ indexed for MEDLINE] 37. Maternal and perinatal risk factors for child‐ 27. Cle lip and palate in Puerto Rico: A Thirty‐ 42. Hypodon a as a risk marker for epithelial ovari‐ 36. Excess of mild errors of morphogenesis in la on‐based study of 8,093 cases. Bille C, Winther JF, Bautz A, Murray JC, Olsen J, Chris‐ tensen K. Am J Epidemiol. 2005 Jun 1;161(11):1047‐55. PMID:15901625 [PubMed ‐ indexed for MEDLINE] cle lip and palate associated with the novel PTCH gene muta ons. Sasaki R, Saito K, Watanabe Y, Yoshinaga T, Fujii K, Agawa K, Miyashita T, Ando T, Akizuki T. J Hum Genet. 2009 Jul;54(7):398‐402. Epub 2009 Jun 12. PMID: 19521425 [PubMed ‐ indexed for MEDLINE] Roesler MA, Linabery AM, Hilden JA, Davies SM, Ross JA. Pediatr Blood Cancer. 2010 Jul;55(1):95‐9. PMID:20486175 [PubMed ‐ in‐ dexed for MEDLINE] hood leukemia. Zack M, Adami HO, Ericson A. Cancer Res. 1991 Jul 15;51(14):3696‐701. PMID: 2065325 [PubMed ‐ indexed for MED‐ LINE] defects, part I: a record‐linkage study, Atlanta, Georgia, 1968‐1988. Mili F, Khoury MJ, Flanders WD, Greenberg RS. Am J Epidemiol. 1993 Mar 15;137(6):629‐38. PMID:8470664 [PubMed ‐ indexed for MEDLINE] 39. Congenital malforma ons and childhood can‐ cer. Nishi M, Miyake H, Takeda T, Hatae Y. Med Pediatr Oncol. 2000;34:250–254. 40. Increased prevalence of minor anomalies in children with hematologic malignancies. Roga‐ novic J, Radojcic‐Badovinac A, Ahel V. Med Pe‐ diatr Oncol. 2002 Feb;38(2):128‐30. PMID:11813182 [PubMed ‐ indexed for MED‐ LINE]. 41. Infant leukemia and congenital abnormali es: a children’s oncology group study. Johnson KJ, http://dentistry3000.pitt.edu 7